
Abstract
Parental daily care and adequate stimuli are extremely important for development and safety of premature babies at home. This study aimed to analyze safe home care for babies born under 32 weeks from parents’ perspectives, with a view to a longitudinal promotion of baby development. A qualitative study, based on philosophical hermeneutic approach proposed by Hans-Georg Gadamer, in which dialogue as a principle provides understanding and fusion of experiences and knowledge. Semi-structured interviews were conducted with 18 parents of premature babies under 1 year of age. Thematic analysis proposed by Braun and Clarke was applied using an inductive approach. Elements related to safe care were identified: home arrival, safe home care: preserving baby health and development, support for safe home care, and development of parental care to promote baby safety. These elements can provide a basis for safe home care that needs to be reinforced longitudinally to increase particularities of baby protection, avoid accidents and illnesses, and improve appropriate developmental stimuli and positive parenting.
Introduction
Births before 37 weeks of gestational age (GA) are the leading cause of death in children under 5 years old (Liu et al., 2016; Unicef, 2018; WHO, 2018). Brazil estimated prevalence of premature births in 11.5%, making it a challenge for health services, maternal and child survival, and health assistance organizations (Leal et al., 2016).
Understanding growth and development of premature babies is important for protecting their daily routines, expanding parental confidence, and avoiding neurodevelopmental adversities (Guralnick, 2012; Jarjour, 2015; Vance et al., 2020). In Brazil, comprehensive childcare is recommended in the guidelines advocated by National Policy for Integral Child Care (Ministry of Health of Brazil, 2018). However, there are gaps in its applicability, generating child, and family vulnerabilities, especially in premature babies (Silva et al., 2020; Viera et al., 2016).
Regarding premature baby care at home, scientific research has highlighted the safe sleep (Naugler and Di Carlo, 2018; Dowling et al., 2018), safe sound exposure (Krueger et al., 2012), success of breastfeeding (Breivold et al., 2019), and secure attachment (Gabler et al., 2014; Posada et al., 2016). Studies also emphasize the importance of professional parental support, especially after hospital discharge (Aydon et al., 2018; Silva et al., 2020; Viera et al., 2016).
Parental confidence is an important factor in promoting health and development of babies with health complexities, and it is relevant to understand how parents deal with their own abilities (Vance et al., 2020). Fragile family contexts can increase child cognitive, social, and learning developmental problems, especially when bonds are impaired by hospitalization (Argall et al., 2021) and prematurity (Pineda et al., 2018). High-risk babies have complex care needs and can benefit from regular follow-up services (Patel et al., 2017).
It is important to examine how mothers and fathers present their perspectives for daily safe care that promotes development of premature babies at home, especially those born with a GA of less than 32 weeks in a Brazilian locality. This study aimed to analyze safe home care for babies born under 32 weeks from parents’ perspectives, with a view to a longitudinal promotion of baby development.
Method
A qualitative study based on philosophical hermeneutic approach proposed by Hans-Georg Gadamer, in which an intersubjective understanding of dialogue as a principle provides a fusion of experiences and knowledge (Gadamer, 2014).
In this study, dialogue with parents allowed an exchange of knowledge and experiences, to emphasize babies’ safe care at home. Interpretative and integral processes are needed to strengthen health care, deepening the meaning of living and falling ill for families and favoring intersubjective aspects of daily life mediated by dialogue (Ayres, 2007).
Consolidated criteria for reporting qualitative studies (COREQ) were used to qualify the study, containing 32 criteria verifications (Tong et al., 2007).
Research was carried out in a Brazilian city, specifically and only in a health institution that performs outpatient and multidisciplinary follow-up for premature babies that have been discharged from a neonatal intensive care unit (NICU) before the age of two. The researcher had no previous connections with the service or participants. The health institution and the Research Ethics Committee of Ribeirao Preto School of Nursing—University of São Paulo approved the research project (registered number: 73412617.0.0000.5393/2017).
Follow-up service nurses indicated to researcher details of all eligible babies and corresponding dates of follow-up, so their parents could be interviewed. A number of participants were not demarcated, a priori, understanding that the realm of interest in this study is not the subjects themselves, but their experiences, knowledge, and practices (Gadamer, 2014). Interviews were conducted with all subjects that fit inclusion criteria. Data saturation was not used, as all eligible babies were included before saturation process took place.
Data collection lasts from January to March 2018 on days of follow-up scheduling for premature babies born between 01 January 2017 and 31 December 2017. Inclusion criteria were mothers and/or fathers above 18 years of age with babies born at a GA under 32 weeks. Babies under one were focused, considering the structuring character of early years and their repercussions in subsequent years (World Health Organization, 2018). Exclusion criteria were twin and primary caregivers who did not play parental role at the time of interview and parents with psychiatric disorders whose diagnosis was reported by the health team.
A single one-off interview was carried out for each participant. Parents received an introduction about the name and origin of the researcher, emphasizing the independence of the investigation from the health institution, confidentiality, research objectives, and invitation to participate (Marconi and Lakatos, 2008). Written consent was obtained from all participants via an informed consent form. Pseudonyms (names of flowers) were included, preserving their identity, in accordance with the government guidelines of Resolution 466/2012 (Ministry of Health of Brazil, 2012). Participant’s identity was kept confidential during data transcription and results description.
Interviews were conducted in a private location provided by the health institution and consisted of two stages. Initially, the participants answered a structured questionnaire about baby’s history, based on “analytical matrix of the child’s vulnerability to adverse situations in their development.” The conceptual bases of “essential needs of the child” and “health vulnerabilities,” used to build the analytical matrix, constitute a theoretical foundation for understanding premature baby’s safety and dimensions to promote their development (Silva et al., 2013).
Participants were interviewed face to face following a semi-structured script built by authors to identify aspects of home care and stimulating practices for premature babies in home context. The guiding questions were: “Please tell me what your baby’s main needs are? What is your understanding of home safety for your baby?” Interviews were audio recorded, transcribed, and organized into individual digital files by the first author.
Transcripts were analyzed according to inductive thematic analysis method, as follows: familiarization with data, generation of initial codes, search for themes, review of themes, definition, and denomination of themes, and report (Braun and Clarke, 2006).
The first conducted interview served as a “pilot,” aiming to learn the applicability of data collection. No questions needed to be changed and the “pilot” interview was also included in the results.
Interviews contents referred to parents’ memories, so there were occasional cases of emotional discomfort when remembering moments of baby’s birth and hospitalization. The researcher maintained a warm attitude toward the interviewees, respecting their feelings. All cases had positive emotional results from recalled memories, reporting that this was due to the baby’s recovery.
Findings
Thirty babies with a GA < 32 weeks were referred to follow-up service in the period and 15 were excluded for the reasons: twins or triplets; mother had mental health problems; baby accompanied by an aunt; lived in another municipality; failed to attend on successive occasions. Fifteen babies (eight girls and seven boys) participated in the follow-up and fulfilled research criteria.
Eighteen parents of 15 premature babies participated in the study. Among these, both parents attended three interviews; one was conducted only with the father and 11 only with the mother. Interviews lasted for 45–60 min. All babies lived with their father and mother, with one exception, who was cared for by her father because mother died during baby birth. Regarding family’s socioeconomic data 09 parents had primary education, 08 high school, and 01 had higher education. Among the interviewees, 04 worked outside the home, one of them delegated care to grandmother, 03 mothers were away from work, and 02 mentioned that they would resign after the period of leave to take care of the baby.
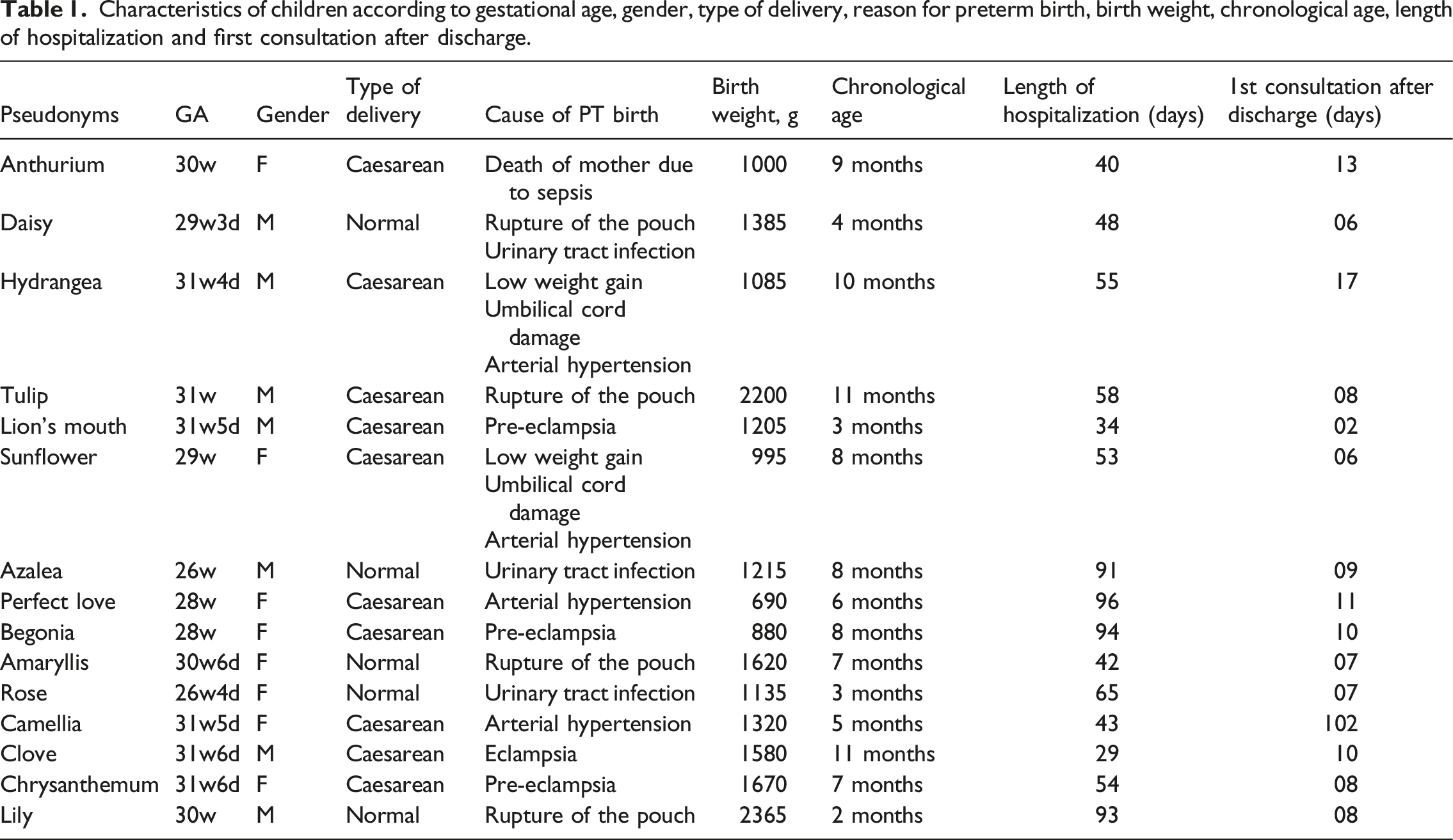
Characteristics of children according to gestational age, gender, type of delivery, reason for preterm birth, birth weight, chronological age, length of hospitalization and first consultation after discharge.
Qualitative results were organized to show aspects relating to safe care of premature babies in the home context. From thematic analysis, a matrix of results (Supplementary Material) was constructed as a synthesis to represent the development of results with codes, initial subthemes, and refined themes from interview analysis. Results are presented in four thematic units: home arrival, safe home care: preserving baby health and development, support for safe home care, and development of parental care to promote baby safety.
Home arrival
Prolonged hospitalization of premature babies causes baby–parent separation, influencing care actions and perceptions at home after hospital discharge. “During that whole period [of hospitalization] I couldn’t take care of him as a mother. Even in the nursery, I spent so little time with him there” (Azalea, mother, eight-month-old baby). “At home, we get so nervous with the care practice because there [at the NICU], the nurses took care of him. Everyone was around him. Then [at home], you are afraid that something wrong could happen” (Amaryllis, mother, seven-month-old baby).
The fact that baby was born prematurely, along with the need for prior hospitalization, conveys an idea of fragility, causing parental uncertainty about baby care. “Because I was afraid he could choke, I did not even sleep at night. I was afraid the milk would come back up because he was very tiny [...]. I was afraid he’d stopped breathing because he had apnea in the NICU […] and he needs so much attention” (Daisy, mother, four-month-old baby).
The establishment of strict hygiene rules at home is common, for example, when picking up the baby and receiving visitors, to prevent the baby from getting sick. There are also attempts to reproduce practices performed in the hospital, which seem to provide more security to baby. “We always clean our hands with alcohol, and I do not let her get cold, and she is a baby who can’t have much contact with people because she is more fragile. So, we have to set rules and I continued the same rules as the hospital” (Perfecto Love, mother, six-month-old baby). “The visitors [at home] always have to wash their hands because he’s premature and he can get an infection faster with any bacteria, you know?” (Lily, mother, two-month-old baby).
Over time, the reproduction of hospital routines at home becomes stressful and parents begin to rethink and construct alternative home care routines. “Trying to follow the nursery routine at home was stressful. Initially, I had to wake her every three hours to breastfeed, to change diapers, because that was the nursery routine. [...]. I can leave her sleeping and, at the time she wakes up and feels hungry, she’ll cry, and I will go there” (Azalea, mother, eight-month-old baby).
The perception of a premature baby’s fragility may be indicative of parental insecurity. Caregivers understand they should be aware of the baby all the time, and concerns focus on the fear that baby will choke on regurgitation or have respiratory distress.
For some parents, hospitalization is the period in which mothers can learn to care for the baby with the hospital staff and gain confidence, strengthening security in home care in relation to initial vulnerable situations. “It was easy to get home, especially because I spent all my time there at the hospital. So I learned a lot and I came home felling to capable to care of my baby. Because he is premature and this time he spends in hospital is also important for us to feel capable” (Clove, mother, 10-month-old baby).
The nursing team provided parents information about care, focusing on bathing, feeding and how to act in case of common accidents at home, so that going home was based on good practices. Such information does not mention stimuli for baby development. “I had no problem getting home, because I learned everything when she was hospitalized. Taking care of her, bathing, those things I had already learned everything. Then I didn’t have any difficulties. It was easy.” (Sunflower, mother, 8-month-old baby) “It was in the maternity hospital that they taught me how to choke the child.” (Begonia, mother, 8-month-old baby)
Safe home care: preserving baby health and development
The interviewees emphasized premature baby safety, focusing on special care at home, mainly on cleaning, dust elimination, concern regarding protecting baby from infections and respiratory allergies, and avoiding accidents.
Parents often show a proactive attitude and reorganize household routines to provide better care and prevent accidents (electrical shocks, burns, drowning, and falls). There are reports about some stages of baby development that require safe precautions. “He’s more fragile and can catch allergies. So, everything has to be clean, hygienic, and in its right place” (Sunflower, mother, eight-month-old baby). “A safe house is where there is little risk for the baby, like the kind of socket plug with no bare wires, and we can’t leave a lot of sharp things near them” (Rose, mother, three-month-old baby). “A safe house is where there is nothing to hurt him [...] when he begins crawling” (Clove, mother, 10-month-old baby).
Reports show that there is recognition that the relationship between parents and baby, permeated with affection, has potential to promote safe care and enable parents to identify baby’s needs. “The baby must feel welcome and loved at home. Parents must stay close and be very careful with them. And that’s where they feel better” (Rose, mother, three-month-old baby). “I think he is safe when we are close to him and taking good care of him. I think this is safety” (Daisy, mother, four-month-old baby).
Support for safe home care
Support for care at home was reported, highlighting extended family support and Internet access to minimize the vulnerability of premature babies and promote safe care.
The need for information to exercise home care and trust in the NICU team, connecting to health professionals by telephone and the Internet, are also reported as a source of support. “I left the hospital and I was able to give medicine. By the time it was six o’clock when I had to administer the medicine, I had already forgotten how. Then, I called the nurse to see if she could explain to me what to do” (Anthurium, father, nine-month-old baby). “I forgot how to act in an emergency with her. Therefore, I searched the Internet to see what to do with a choking baby. When she choked, I used to hit her on the back, as I had seen on YouTube, and she would be okay” (Amaryllis, mother, seven-month-old baby). “We have always been doing exercises with the legs and with the arms as we had seen on YouTube. Then we do the same” (Lion´s Mouth, mother, three-month-old baby).
Information in online videos about home care for premature babies is linked to the need to visualize actions that can be taken and stimulate their development, which gives parents security and confidence.
Children’s videos configure interaction tools between parents and baby, enabling the observation of the baby’s positive reactions to the sound of the videos and interaction with the caregiver’s dancing body movements. “Now I put the ‘lottie dottie chicken’ [music and cartoons] on YouTube, on television, and he’s all happy to see the chicken and to hear the song. Then I sing and dance with him” (Azalea, mother, eight-month-old baby).
Internet access enables communication and social support from relatives and friends through virtual social networks. Photos, reports about baby’s health condition, and the externalization of the lived experience make it possible to follow the evolution of premature babies’ clinical situation. “I published his photos on Facebook so my friends and my relatives could see. They said: ‘Wow, this is really a miracle, because this boy does not seem like a premature baby.’ Then, I said, ‘But he was premature.’ I even gave a testimonial on Facebook, I told our story and everything about how he was born, how complicated it was” (Azalea, mother, eight-month-old baby).
The participation of close family members helps build trust, facilitating baby care at home. Grandmothers were reported as a source of support, as they had already experienced motherhood. “My mother and my mother-in-law, who are older and have already had children, can help me” (Lily, mother, two-month-old baby). “I listen to advice from her grandmother, her aunt. [...]. The family members gave a lot of advice and helped to distract me at times. I would not have made it” (Anthurium, father, nine-month-old baby).
Specialized follow-up clinics provide resolution of doubts, new information and support, as a secure source of continuity with home care. The importance of support from the primary health care team was also reported due to geographic proximity in emergencies and practices of home visits. “I alternate. I bring him every night. I have an appointment here at the beginning of the month and an appointment there [at the Public Family Health Service] in the middle of the month” (Azalea, mother, eight-month-old baby). “But the primary health care service is closer, it’s easier, and I already know the team” (Clove, mother, 10-month-old baby).
Parents may feel prepared for care and supported, even so, they have fears and moments of apprehension of any damage to baby health and need the effective support of health professionals.
Development of parental care to promote baby safety
Changes in parental perceptions are noted, understanding babies’ manifestations and seeking to identify baby needs, especially in the type of crying. “Through his gestures and his crying, I try to understand what he wants” (Daisy, mother, four-month-old baby). “I know his type of crying in the morning, his crying from hunger, when he feels some pain, when he is angry. I know his various types of crying” (Azalea, mother, eight-month-old baby).
There are situations in which parents feel that they need to be present and taking care of the baby, which alerts us to possible circumstances of overprotection. Parents report the desire to go beyond baby needs when caring at home, in an attempt to compensate for their initial difficulties. “You end up overprotecting the child to make up for everything she’s been through” (Daisy, father, four-month-old baby). “The care and the child become special because everyone saw that my son is a miracle. Everyone saw him being born at 26 weeks and spending 90 days in the NICU” (Azalea, mother, eight-month-old baby).
The path taken in the baby’s first year of life helps parents to recognize personal transformation and maturity, with a re-significance of parental role. “We learn slowly. At first, we think we will not make it, we think we will go crazy. Then, later, we can do it” (Anthurium, father, nine-month-old baby).
The time elapsed parallel to baby’s development gives rise to feelings of gratification and overcoming. “Nowadays, everyone says that I took good care of him, because he is a very healthy child. So, I believe it is difficult, but as is well known, when a mother gives birth, she has the gift of becoming a mother” (Azalea, mother, eight-month-old baby).
Parents' overcoming movement is related to their identification that the baby is doing well. Thus, parental roles are recognized as developing in accordance with baby development.
Results suggest two transition periods for preterm baby home care: First, due to the transition of care between hospital discharge and the first reorganizations of care actions at home and another moment is characterized by a certain ambiguity between identification of signs of overcoming the prematurity initial clinical condition and baby overprotection. Both moments of transition are extremely relevant to contemplate safe care and adequate protection for growth and development and good parenting practices.
Discussion
Results show that prematurity of babies under 32 weeks of GA triggers the perception of fragility that influences the parental care offered. Transition periods are structural, substantiating more adequate and safe care and also providing parents with confidence and good daily practices.
In the profile of parental caregivers of premature babies, maternal education is a key marker of socioeconomic status and is associated with later neurocognitive outcomes, especially extreme preterm babies (Joseph et al., 2018). In Brazil, socio-demographic factors associated with spontaneous preterm birth were adolescent pregnancy, low total years of schooling, and inadequate prenatal care (Leal et al., 2016). Spontaneous premature births associated with socially disadvantaged population groups reaffirm the importance of reducing social and health inequalities (Leal et al., 2016).
Results bring elements about parents’ efforts to preserve early baby health and development, linking to their experiences during premature hospitalization. There is a marked appreciation of hospital practices, suggesting that it influences parental confidence to provide babies safe care at home. Results also highlight the search for information in online videos about care and development of premature babies, showing the need to visualize actions to stimulate babies’ development and autonomy.
Parental experiences express tension of any harm to premature baby, in constant alert and sharp surveillance to neutralize the initial difficulties. Such circumstances show parents need to be supported in safe care routines that allow for progress in stimulating adequate baby development, suppressing uncertainties, fears, and overprotection.
Going home from hospital is a stressful time for premature babies’ parents. This moment is characterized by loss of the neonatal team support and perception of preterm fragility, mediated trial and error in parenting skills to perform care (Aydon et al., 2018; Boykova, 2016; Custódio et al., 2016; Franck et al., 2017). Also, parents have overprotective attitudes and are inconstant concerned about their baby’s well-being at home (Granero-Molina et al., 2019). Consistent support during hospitalization and post-discharge can affect the level of maternal confidence in caring for a premature baby (Lee et al., 2019; Premji et al., 2018).
Transition between hospitalization and home requires continuity of care, active and reliable relationships, connection between primary care services, specialized outpatient clinics and home, avoiding poor care delivery, family discomfort, gaps in the search for resources, and adversities to babies’ health and development (Patel et al., 2017). This process requires high quality and scientific evidence-based resources that are readily accessible, easy to understand, reliable, and parent-centered (Alderdice et al., 2018).
Maternal confidence of Canadian premature babies decreases after the first 2 months of discharge, related to baby care demands, memories of the hospital period, type of interaction with nurses in primary health care, and social and emotional support (Premji et al., 2018). Parental knowledge about prematurity is fundamental, and nurses are a source of care information (Matos et al., 2020).
Extended family support was configured as an opening to help parents. Supporting family relationships are relevant and gaps in family support can negatively weaken bonds, consequently to baby’s health and development (Mulcahy and Savage, 2016).
Internet access was also used as a source of support in home care reported by parents, through their own research. Smartphones are accessible and practical to be used by caregivers during childcare (Garfield et al., 2016), allowing quick access to virtual information. Good parenting practices are important to deal with daily routines, but it is necessary to seek correct and pertinent information that favors facing and relieving stress in baby development monitoring (Msall, 2019).
Brazilian initiatives with digital educational materials were carried out with families of premature babies, with encouragement and information that facilitates daily care (Dagostini et al., 2020; Ferecini et al., 2012; Nieto et al., 2016; Pinto et al., 2018). Information and care support needs for British parents were also reinforced for post-discharge preterm infants (Alderdice et al., 2018).
Home visits to premature babies’ families are important strategies in primary health care to improve care outcomes, provide rich opportunities to identify, intervene, and filling gaps, optimizing social and health services resources (Patel et al., 2017; Silva et al., 2020). In Brazil, the Standard for Humanized Care for Low-Weight Newborns with Kangaroo Method is a government policy covering follow-up from birth (1st stage), achieving clinical stability (2nd stage) to discharge (3rd stage) and is related with the public health network (Ministry of Health of Brazil, 2007; Ministry of Health of Brazil, 2013). The third stage of the Brazilian Kangaroo Method includes continuity of care for premature babies at home, recognizing the importance of bond with hospital staff and health professionals accessible to the family after hospital discharge.
Family-centered home visits by nurses are identified as a beneficial strategy developing a positive therapeutic relationship with parents and intensifying attention to their baby needs (Lam et al., 2017). Brazilian studies with families of premature babies found gaps in the transition between neonatal units and home (Silva et al., 2020; Viera et al., 2016), with few longitudinal baby care actions. Safe care offered at home encompasses physical protection, prevention of accidents and diseases, and promotion of premature baby development, involving caregivers and their interaction permeated with affection, through which they identify needs and promote baby safety (Silva et al., 2020; Viera et al., 2016).
There are parental reports that show overprotective attitudes. Maternal overprotection has already been found in home care for babies born under 32 weeks, signaled by excessive concern and constant search for baby well-being (Granero-Molina et al., 2019). It is important to consider that babies’ development requires responsive care and opportunities for learning from the first years of life, combined with nurturing care (Black et al., 2017; WHO, 2018). Thus, overprotection requires a careful look related to its effects on full development.
Effective mutual interaction between parents and baby is essential, connected by affect and multidirectional flow, enabling the emission, reception, and processing of information in verbal, nonverbal, tactile, kinesthetic, and olfactory sensory channels (Sparrow, 2013).
Safe care for premature babies at home is permeated by different parental experiences, sometimes more vulnerable and sometimes stronger. Unsafe home environment for a premature baby implies an increase in circumstances of vulnerability, due to prematurity and the process of growth and development, or due to the position of uncertainty and reconfiguration of parenthood.
Health professionals and institutional programs and services need to contribute to reducing vulnerabilities and strengthening safe home care. It is essential to expand the specific care that involves the peculiarities of full babies’ protection and promote adequate stimuli for their full and longitudinal development.
Study limitations
Study limitations refer to parental perspectives, with a predominance of maternal reports, which may hide additional aspects of childcare at home. In addition, there were no cases of babies who needed to use life support technologies at home, such as breathing apparatus or tube feeding, as occurs with premature babies in the studied age group, with implications for safe care at home and parental trust.
A single interview was conducted with each participant and did not include an analysis of context of home care. Observation techniques to assess attendance during the interview were not used. Therefore, this study only addresses parental perspectives.
Another methodological limitation refers to the same person who performed data collection and analysis of results, which could weaken the analysis of the safe childcare at home. On the other hand, research based on philosophical hermeneutics, with dialogue as a principle that provides understanding and fusion of experiences and knowledge, strengthens the analysis of results.
Implications for health care and nursing
The study has implications for health care and nursing, contributing to the understanding of the daily care of preterm infants, in order to highlight longitudinal care in primary health care.
Interventions that emphasize dialogue between health professionals and parents and proximity to the home environment allow knowing different parental contexts, favoring gradual learning of safe care skills, promoting physical, emotional, and social bonds as early as possible, sharing innovative knowledge, avoiding false information, guide appropriate stimuli for full baby development, and dignify parenting skills. In particular, nurses carrying out educational activities and being attentive to mistakes and inadequate information provided on the Internet can ensure the clarification of doubts, avoid uncertainties, generate new information, and promote adequate support for essential care.
In terms of scientific research, this study provides elements for the theme of home safety linked to the promotion of safe development in early childhood. It also identifies actions that are vital for nursing care in the care transition and contributes to discussing positive parenting.
Conclusion
Aspects are presented about home arrival, safe home care: preserving baby health and development, support for safe home care, and development of parental care to promote safety, bringing together components linked to safe childcare and parenting. This set of aspects constitutes an interface between parental demands in concrete experiences and needs to offer policy health attention in moments of care transition.
Results expand the comprehensive care of premature babies at home, relevant to the fusion of horizons between health professionals and parents. Intersubjective comprehensive care on routine home care is relevant through the path of dialogue. Thus, there is value in experiences and knowledge and a fruitful way to ensure the longitudinally of parental care and baby integral and safe development.
The object of the study outlined is complex and should be expanded with other research, in the community and in home visits, exploring health professionals’ perspectives, intersectoral care network, and the challenges of adversity in early childhood.
Supplemental Material
sj-zip-1-chc-10.1177_13674935221089450 – Supplemental Material for Safe care for premature babies at home: Parenting and stimulating development
Supplemental Material, sj-zip-1-chc-10.1177_13674935221089450 for Safe care for premature babies at home: Parenting and stimulating development by Letícia Pancieri, Rosane M M Silva, Monika Wernet, Luciana M M Fonseca, Shaffa Hameed and Debora F Mello in Journal of Child Health Care
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was support for research from the National Council for Scientific and Technological Development of Brazil.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.