
Abstract
Early marriage (i.e., at less than 18 years of age) is a significant global problem threatening the well-being of women. This cross-sectional study evaluated early marriage and the mental health of Roma women in Adana, Turkey. Data were collected between March 2019 and September 2019 using the Descriptive Characteristics Form and the Brief Symptom Inventory. We interviewed 272 married Roma women over 18 years of age, of whom 59.6% (n = 162) had married before the age of 18 years; of these, 14.2% had done so before the age of 15. Significant positive correlations were found between the duration of the marriage and measures of interpersonal sensitivity, somatization, depression, anxiety, phobia, paranoid ideation, psychoticism, and the Global Severity Index in the women who had married early. Among women who married after 18, the duration of marriage had a significant positive relationship with somatization and phobic anxiety. Early marriage and a longer duration of marriage were associated with more symptoms of psychological distress.
Introduction
Early marriage is defined as an official or traditional marriage in which one of the partners is younger than 18 years of age (United Nations Children's Fund [UNICEF], 2021). The legal age of marriage is 16–18 years in many countries. However, it has been suggested by UNICEF that the legal age of marriage should be at least 18 (UNICEF, 2022). Traditional marriages without official sanction before the age of 18 are common worldwide (Arthur et al., 2018; World Health Organization [WHO], 2016). Globally, 21% of women are married before the age of 18. In more than one-third of these marriages, the age of marriage of the woman is less than 15 years (UNICEF, 2012, 2014a, 2014b). For men worldwide, 4.5% marry when they are below the age of 18 (Gaston et al., 2019; United Nations Population Fund [UNFPA], 2012). Although early marriages involve both genders, young women are at a greater risk than young men of sexual, physical, and psychological violence and related outcomes (UNICEF, 2012; WHO, 2016). In recent years, policymakers around the word have made efforts to reduce the frequency of early marriages (Council of Europe, 2015a; UNICEF, 2021). However, despite such attempts, early marriage remains a significant public health concern in many countries. Early marriage is particularly prevalent in some cultures and countries, including those in central Europe, eastern Europe, Asia, and Africa (Gaston et al., 2019; UNICEF, 2012; WHO, 2016). Roma people, who have a large population in Romania, Italy, Ireland, Poland, Bulgaria, Greece, Serbia, Moldova, and Turkey, are distinct cultural minorities in which early marriages frequently occur (Council of Europe, 2015a). The prevalence of early marriage in the Roma population is about twice that of the general population in these countries (Council of Europe, 2015a, 2015b; Sedlecky & Rašević, 2015).
In Turkey, rates of early marriages among Roma girls are well above the Turkish average. Almost half of Roma girls under 18 are married, and 13.6% of those younger than 15 are married (Tanrıverdi et al., 2012; Taylan, 2016; Turkey Ministry of Family and Social Policies General Directorate of Family and Community Services [TMFSPG], 2020). The average age of marriage for a Roma girl in Turkey is between 13 and 17 years (Özkan, 2006). It is further estimated that between 25%–30% of Roma women aged 15–19 years in Romania are married (Council of Europe, 2015a, 2015b).
Cultural and socioeconomic factors may explain the phenomenon of early marriage in Roma communities. Community pressure and traditional values influence parents to accept early marriage for their children (Sedlecky & Rašević, 2015). Values and rituals, as well as power relations, are clearly defined in the Roma culture (Casey, 2014; Sedlecky & Rašević, 2015). In many Roma families, grandparents and parents are the highest authority, and their decisions are rarely opposed. Parents’ views define the boundary between childhood and adulthood. The acceptance of a teenage girl into the Roma social environment is carried out through the assimilation of sexual roles and the culture of marital and family relationships. Marriage, and later motherhood, confer status on Roma women. The emphasis on building a family early, and other traditions related to sexuality, leads many Roma women to consider early marriage to be a normal part of their life course. This practice ensures they have respect and relevance within their communities and allows Roma girls to consider early marriage as normative. In general, Roma men also tend to marry younger than the general population, and therefore the age difference between spouses is usually small. The notion of the normality of early marriage in Roma communities is somewhat controversial. While some Roma boys and girls support the practice, others may be critical of it (Afanasieva et al., 2020; Stojanovski et al., 2017). Roma parents, girls and boys are all navigating the spaces between the demands of modern society and the requirements of traditions and values. Community pressure and traditional values lead parents to accept early marriage for their children (Afanasieva et al., 2020; Bosnjak & Acton, 2013; Sedlecky & Rašević, 2015; Stojanovski et al., 2017).
The situation for Roma women in Adana, Turkey, is quite similar to that of Roma women in other parts of the world. The Roma people in Turkey are poor in terms of social, economic, political, and civil welfare, and lack decision-making power to influence matters concerning them. They are also more likely to lack access to the opportunities afforded by high income, education, employment, and safe and stable housing (Adana Valiliği, 2019; Aktepe & Atay, 2017; Balkız & Göktepe, 2014; Casey, 2014; Çelik & Yüce Tar, 2015; Danka, 2008; Sedlecky & Rašević, 2015; Tanrıverdi et al., 2012; Voicu & Popescu, 2009). In conditions of exclusion, poverty and marginality, the Roma values and traditions about family generate a situation in which marriage may be the only viable strategy for survival from a very early age. The social structure of Roma society is based on strict gender roles in which Roma women are expected to marry, have children, and care for their husbands and children. Structural inequities for Roma can be further worsened by gender-related inequalities in this population (Casey, 2014; Sedlecky & Rašević, 2015; Tanrıverdi et al., 2012; Voicu & Popescu, 2009). Early marriages cause or exacerbate many difficulties for Roma women. Given these circumstances, Roma women are one of the groups most adversely affected by early marriage, compared to other communities in Turkey and worldwide (Council of Europe, 2015a; Gamella, 2018; Martin & Gamella, 2005; Tanrıverdi et al., 2012). Gender-based violence and early marriage faced by Roma women are viewed by some Roma people as normal cultural characteristics of the Roma community and not as problems in themselves. However, these issues are pervasive and threaten the status and well-being of young women. The tradition of early marriage in particular makes Roma women vulnerable to morbidity and mortality risk factors. A Roma girl is expected to fulfill her gendered role as a mother and a wife (Afanasieva et al., 2020; Bosnjak & Acton, 2013). Adolescent Roma girls who have not yet reached physical and psychosocial maturity are expected to marry, establish a family, and have children. As a result, they end their formal education, become mothers, assume full responsibility for the management of their homes, and start working out of the home in addition to having children earlier than is optimal for their development (Aktepe & Atay, 2017; Council of Europe, 2015a; Gamella, 2018; Tanrıverdi et al., 2012). Increased risk for partner violence and its consequences for women's health are other aspects of early marriage faced by these young women (Hotchkiss et al., 2016; McFarlane et al., 2016; Nasrullah et al., 2014; WHO, 2013).
Roma women are at a higher risk of mental illness than non-Roma women (Foldes & Covaci, 2012). A study conducted in Serbia found that Roma women were more unhappy and dissatisfied with their lives than non-Roma women (Cvjetkovic et al., 2017). According to another study conducted in Romania and Bulgaria, Roma women have more mental health problems than non-Roma (Le Cook et al., 2019). A similar study in Portugal revealed that Roma women experience anxiety, depression, and suicidal ideation, and attempt suicide many times more often than the population average (Pereira et al., 2016).
These mental health disparities may be related to the lack of opportunities to set and achieve goals in their lives and the sense of not belonging to society and family, which are strongly associated with symptoms such as low self-esteem and depression during the transitional stages from childhood to adolescence and from adolescence to young adulthood. In addition, the multiple risk factors such as physical and sexual violence, poverty, and adolescent pregnancy that these women are exposed to from adolescence may worsen over time and lead to psychological stress and depression (Le Cook et al., 2019). In addition to all these social and economic factors, early marriages and their consequences harm the psychosocial health of Roma women (Hajduchová & Urban, 2014; Medas, 2020; Robinson et al., 2022; Vorvolakos et al., 2012).
Improving the mental health of Roma women requires a systematic approach, policy reform, research studies, and evidence-based interventions. Studies should therefore be performed to determine the causes, prevalence, and consequences of mental health issues and the support needs of Roma women who marry before the age of 18 (Le Cook et al., 2019; Svanemyr et al., 2015).
Many studies have been conducted to evaluate the physical and mental health of Roma women and find that they have elevated rates of physical health problems, including obesity, hypertension, diabetes, and coronary artery disease, as well as mental health problems such as major depression, anxiety disorder, and substance abuse (Carrasco-Garrido et al., 2010; Coea & Cvorovic, 2017; Cook et al., 2013; Kotrotsiou et al., 2014; McGorrian et al., 2013; Van Cleemput, 2018). However, few studies have focused on the long-term effects of early marriage on women's mental health, and none to date have addressed this issue among Roma women in Turkey (Le Strat et al., 2011; McFarlane et al., 2016).
The United Nations Convention on the Rights of the Child recommends the protection of the civil, political, economic, social, and cultural rights of every child, regardless of race, religion, or ability (UNICEF, 2021). It further states that every child has the right to survival, protection, and education. Therefore, it is essential to reveal how early marriages affect the mental state of Roma women to plan and implement interventions that can prevent the harmful effects of this practice on public health and economy, and to detect, treat, and encourage women in early marriages to receive appropriate health care. This understanding can also contribute significantly to preventing early marriages (Le Strat et al., 2011; McFarlane et al., 2016; Shives, 2008). Accordingly, this study was conducted to evaluate the relationship between early marriage and the mental state of Roma women in Adana, Turkey.
Methods
Study design and setting
This study used a cross-sectional population survey to examine the prevalence of early marriage and its correlates with mental state among Roma women in Adana, Turkey. The study was carried out in a part of Yüreğir, a small town in Adana, between March and September 2019. Adana is the fifth most populous city in Turkey and is considered the junction of migration in the country. Yüreğir has a high proportion of people with low socioeconomic status and is notable for high levels of migration into the region. Many different ethnic groups, including Roma people, live in Yüreğir, although their interactions are limited.
Participants
About 900 Roma people, including adults and older people, live in Yüreğir (Adana Valiliği, 2019), and the study population was estimated as .5 × 900 = 450 Roma women. The sample size of the study was calculated on the basis of the known universe approach. To represent this population, a power calculation suggested minimum sample size was 269 based on a 95% confidence interval (α = .05), a standard error of 5% (d = .05) and incidence of Roma women of p = .5 and q = .5 (Cochran, 1977). A list of married Roma women was obtained by interviewing the headman of the Roma neighborhood and the head of the Adana Roma Association. Roma women who were married, aged over 18 years old, and had sufficient communication abilities were included in the study. Simple random sampling was performed using a random numbers table, and 272 Roma women were contacted. The participants spoke Turkish well. No data exclusion occurred in our analysis.
Data collection
The study data were collected via face-to-face interviews by the author of the study. Accompanied by the head of the Adana Roma Association, the author met with the participants and shared information about the study process. The survey questions were read aloud as the participants were either illiterate or had low levels of education. The interviews were held in a separate room in the women's homes. Other family members waited in another room. Each interview lasted 15–20 min. The participants were not given any incentives.
The data were gathered using the Descriptive Characteristics Form and the Brief Symptom Inventory (BSI). The Descriptive Characteristics Form was created by the researcher based on the relevant literature. The form was composed of 13 questions about the women's sociodemographic characteristics (age, marital status, marriage age, mother's marriage age, duration of the marriage, employment, social security status, educational status, having children, number of children) and health (chronic disease, name of chronic disease, smoking) (Coea & Cvorovic, 2017; Kotrotsiou et al., 2014; Van Cleemput, 2018).
The BSI is the short form of the Symptom Checklist-90-Revised (SCL-90-R). It was developed by Derogatis (1992) and adapted to Turkish culture by Şahin and Durak (1994). The BSI is a 53-item, 5-point self-report Likert scale that is used to screen various psychological symptoms. Higher scores on the scale indicate a higher frequency of symptoms. Derogatis (1992) reported that Cronbach's alpha for the BSI's nine subscales ranged from .71 to .85. Şahin and Durak (1994) reported that the Cronbach's alpha of the subscales of the Turkish version of the scale ranged from .63 to .86, while the Cronbach's alpha calculated for the total score of the scale was .93–.96.
The BSI consists of nine symptom dimensions, namely, somatization, obsession-compulsion, interpersonal sensitivity, depression, anxiety, hostility, phobic anxiety, paranoid ideation, and psychoticism, and three global indices of distress: The Global Severity Index, the Positive Symptom Distress Index, and the Positive Symptom Total. These global indices measure the current or past levels of symptomatology, symptom intensity, and the number of reported symptoms, respectively (Derogatis, 1992; Şahin & Durak, 1994).
Statistical analysis
The data were analyzed using SPSS 21. The Shapiro–Wilk test was used to check the normality of the continuous variables. The data relating to the age of the participants, their mother's age at marriage, the duration of their marriage, and the BSI were normally distributed. Student's t-test was used to compare the women who married before the age of 18 and those who married after the age of 18 and the mean scores of the BSI between the women with chronic diseases and those without chronic diseases. The data on the number of children did not have a normal distribution, so the Mann–Whitney U test was employed to compare the data. A chi-square test was used to compare the categorical variables of the women who married before 18 and those who married after the age of 18. Fisher's exact test was used when the proportion of cells with expected values less than five was greater than 20%. The Pearson correlation coefficient was calculated to examine the linear relationship between the scores for the BSI, age at marriage, and duration of the marriage. Finally, multiple linear regression analysis with backward elimination was applied to analyze the effects of chronic diseases, age at marriage, and duration of marriage on the results of the BSI. The reliability of the BSI was expressed as Cronbach's alpha. The statistical significance was set at p < .05.
Ethical considerations
The study was conducted in accordance with the principles of the Declaration of Helsinki. Ethical approval was obtained from the Cukurova University Ethical Board of Clinical Research (number 79/51, dated July 6, 2018), and written permission was obtained from the city governor. Participation in the study was voluntary, and oral and written informed consent was obtained from the women after being given relevant information about the study, including aspects relating to confidentiality, privacy, and the right to withdraw from the study.
Results
Sociodemographic characteristics of the study participants
The study was conducted with 272 Roma women, of whom 59.6% (n = 162) had married before the age of 18 years, and 40.4% (n = 110) had married after the age of 18 years. The mean age of the women was 37.64 ± 13.62 years and ranged from 18 to 67 years. Of the Roma women in early marriages, 14.2% (n = 22) had married before the age of 15 years, and 85.8% (n = 140) had married when they were between 15 and 17 years of age.
Table 1 shows the sociodemographic characteristics and health knowledge of the participants. The majority of women in the study had a perception of low socioeconomic level; 37.9% of the participants did not receive any education, 40.7% of the women, who have not completed secondary school education, dropped out due to financial reasons. There was no significant difference in terms of education, employment, and socioeconomic status between women who married before and after the age of 18 (p > .05) (Table 1). However, significant differences were found between the women who married before and after the age of 18 in terms of their mean age, mother's age at marriage, and duration of marriage (p < .05) (see Table 1 for results).
Descriptive characteristics of participants according to age at marriage.
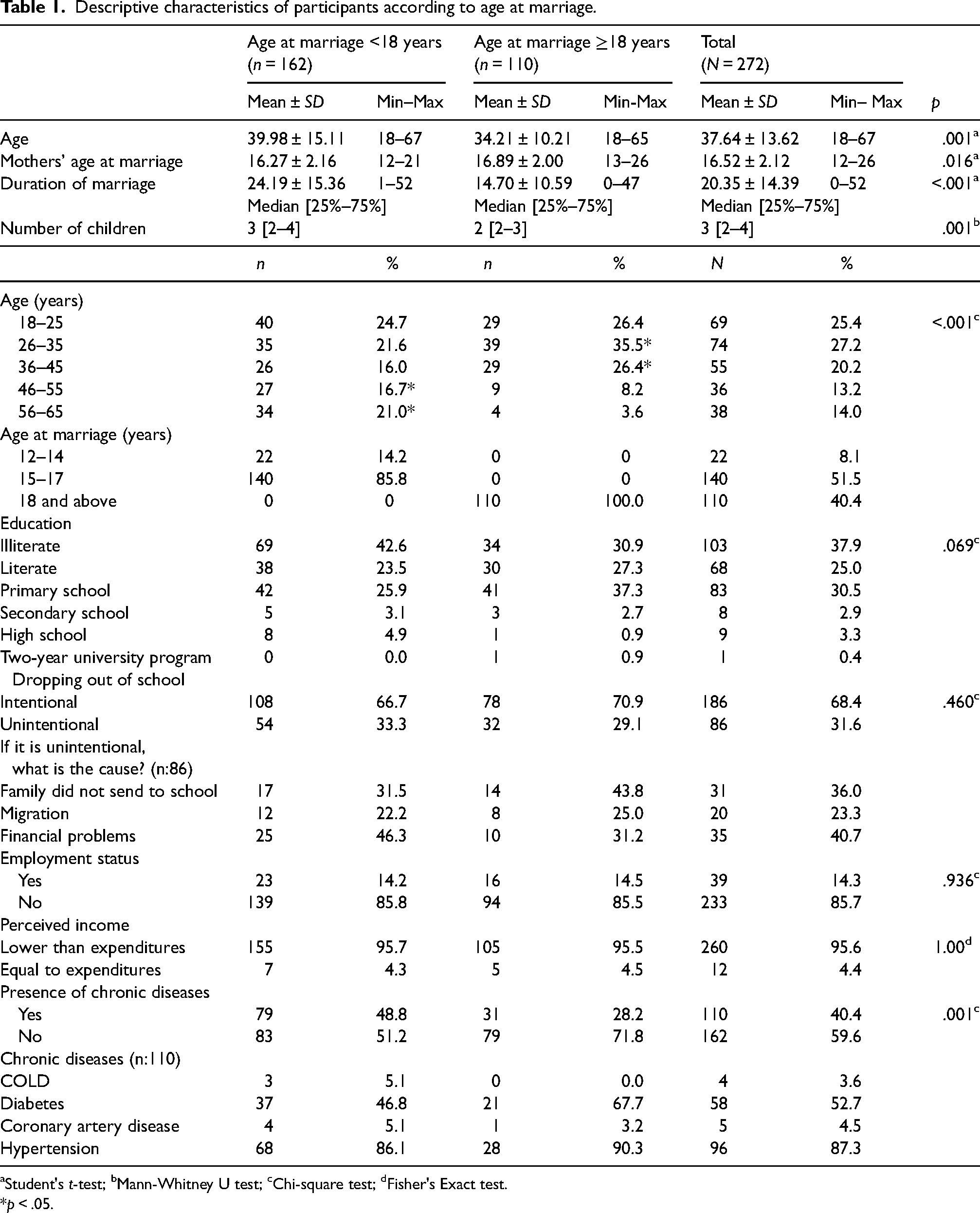
Student's t-test; bMann-Whitney U test; cChi-square test; dFisher's Exact test.
*p < .05.
The women with early marriages had a significantly higher number of children: Median = 3, range age at marriage <18 years; Median = 2, range age at marriage >18 years (p = .001). The mean age also differed significantly between the women who married before the age of 18 years old (M = 39.98, SD = 15.1) and those who married after 18 years old (M = 34.21, SD = 10.21) (p < .001). The presence of chronic diseases was significantly different between the women who married before and after 18 years old (p = .001). In fact, 48.8% (n = 79) of the former group and 28.8% (n = 31) of the latter group had a chronic disease (Table 1).
Mental health outcomes
Cronbach alpha coefficients were calculated for the reliability of the BSI and BSI subscales. As shown in Table 2, the subscales of interpersonal sensitivity and psychoticism had low reliability (.40 ≤ α < .60) but the subscales for obsession-compulsion, depression, anxiety, hostility, phobic anxiety, and paranoid ideation had relatively high reliability (.80 ≤ α < l.00). In addition, the subscale somatization was very reliable (.60 ≤ α < .80).
Roma women's scores and reliability for the subscales of the Brief Symptom Inventory.
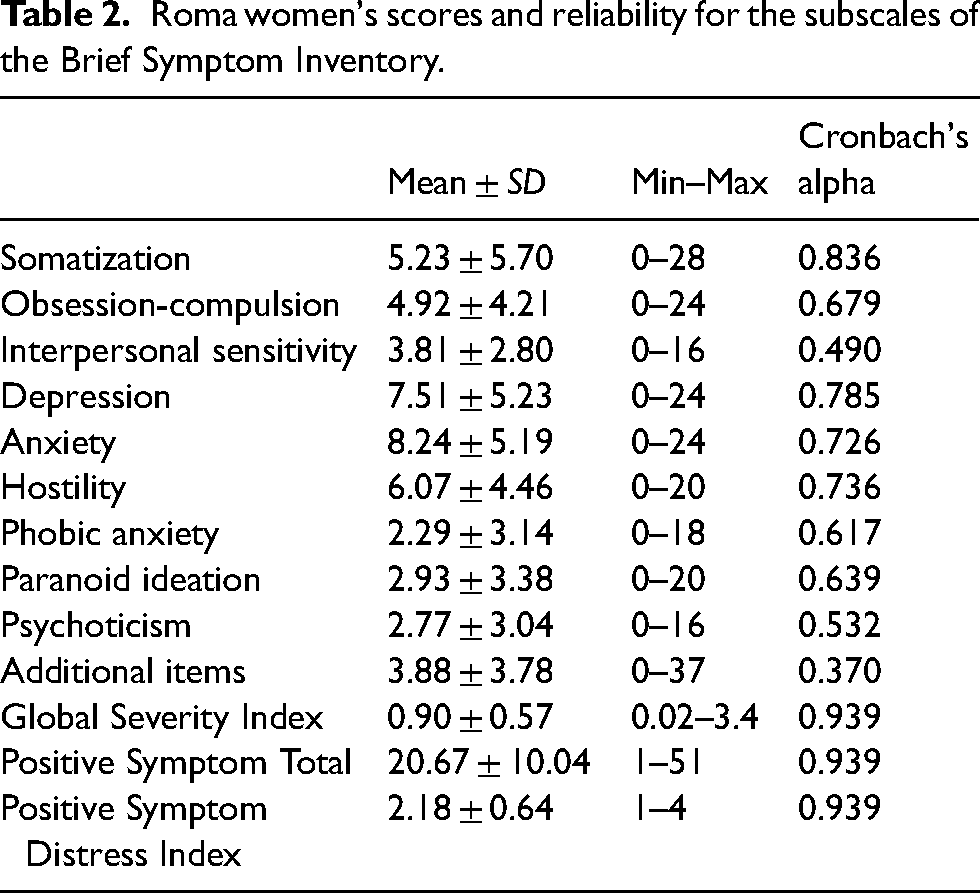
Table 3 shows the correlations between the mean scores of the Roma women who married before and after the age of 18 for the BSI subscales, the duration of marriage, and their mother's age at marriage. A significant positive association was found between duration of the marriage and the subscales of interpersonal sensitivity, somatization, depression, anxiety, phobic anxiety, paranoid ideation, psychoticism, and the Global Severity Index in the women who married before the age of 18. Among the women who married after the age of 18, duration of marriage had a significant positive association with the subscales somatization (r = .258) and phobic anxiety (r = .191; p < .001; Table 3). Further, duration of marriage among the Roma women had a significant positive association with all the subscales of the BSI except hostility (Table 3).
Bivariate correlations between Brief Symptom Inventory scores and age at marriage, mothers’ age at marriage and duration of marriage among Roma women.
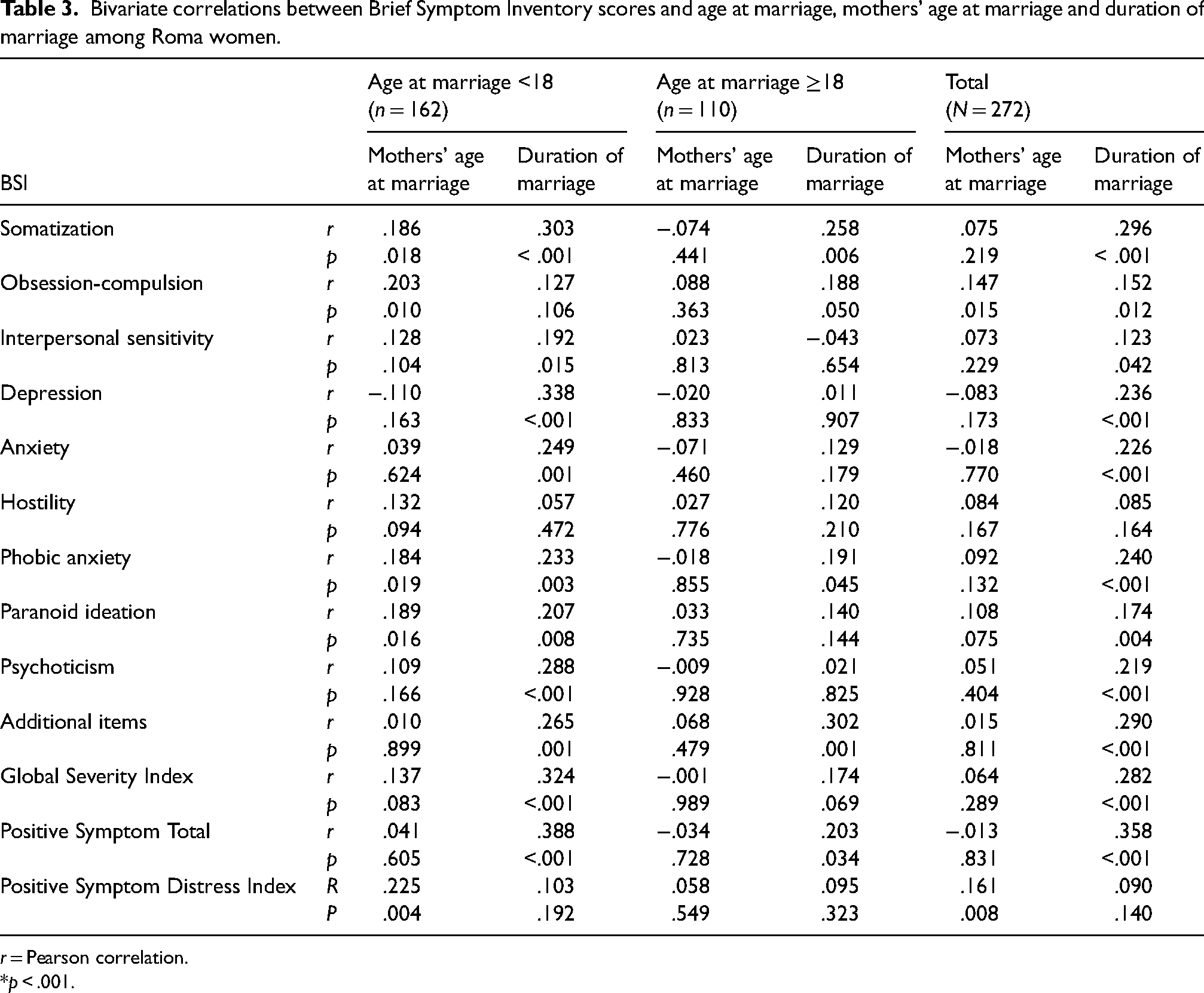
r = Pearson correlation.
*p < .001.
Table 4 presents the results of the multiple linear regression examining the effects of the risk factors (age at marriage, mother's age at marriage, duration of marriage, and the number of children) on the scores for the BSI among the Roma women. Significant predictors of the BSI among the study participants were duration of marriage and somatization, R2 = .09, F(4, 267) = 7.56, p = .000, depression, R2 = .06, F(4, 267) = 4.92, p = .001, psychoticism, R2 = .07, F(4, 267) = 5.90, p = .000, the Global Severity Index, R2 = .08, F(4, 267) = 6.93, p = .000, and the Positive Symptom Total, R2 = .12, F(4, 267) = 10.51, p = .000 (Table 4).
Multiple linear regression models of effects of risk factors on Brief Symptom Inventory scores of Roma women (N = 272).
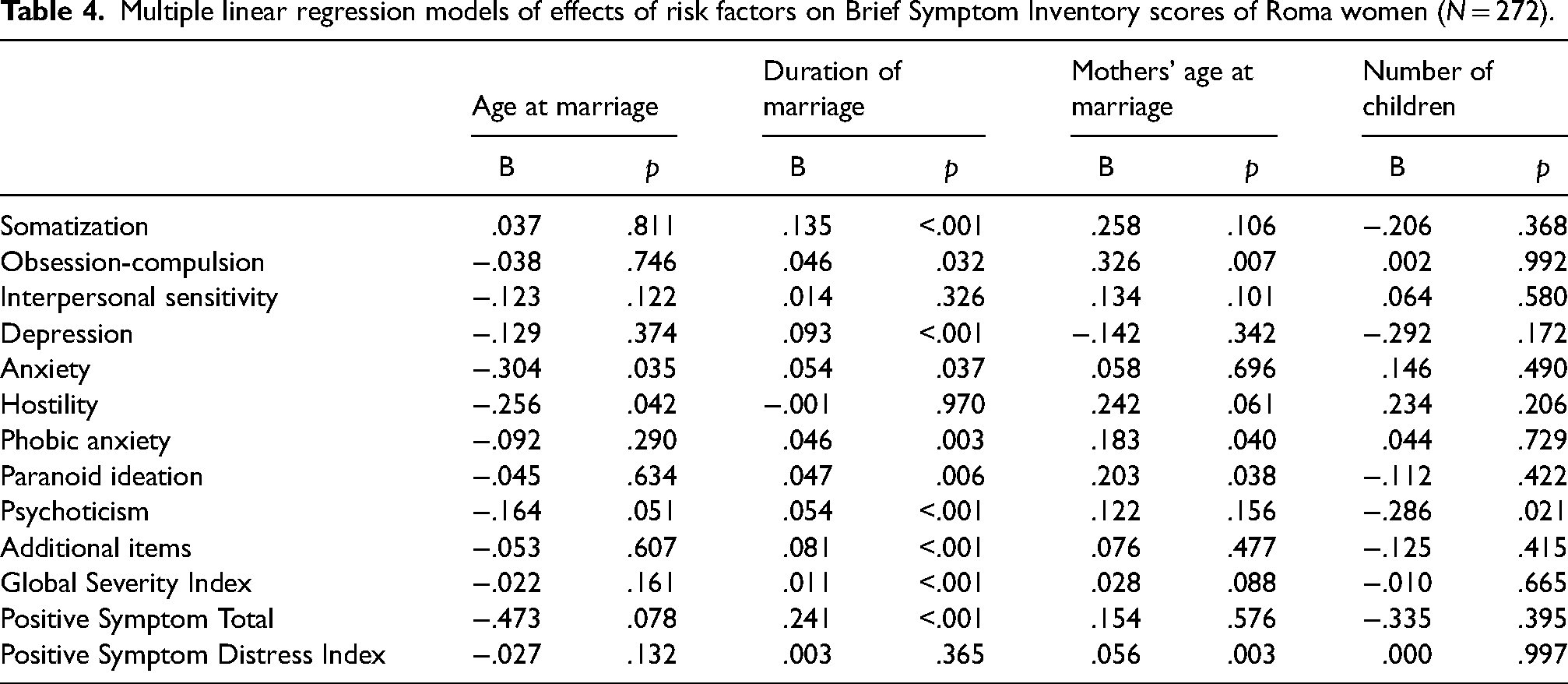
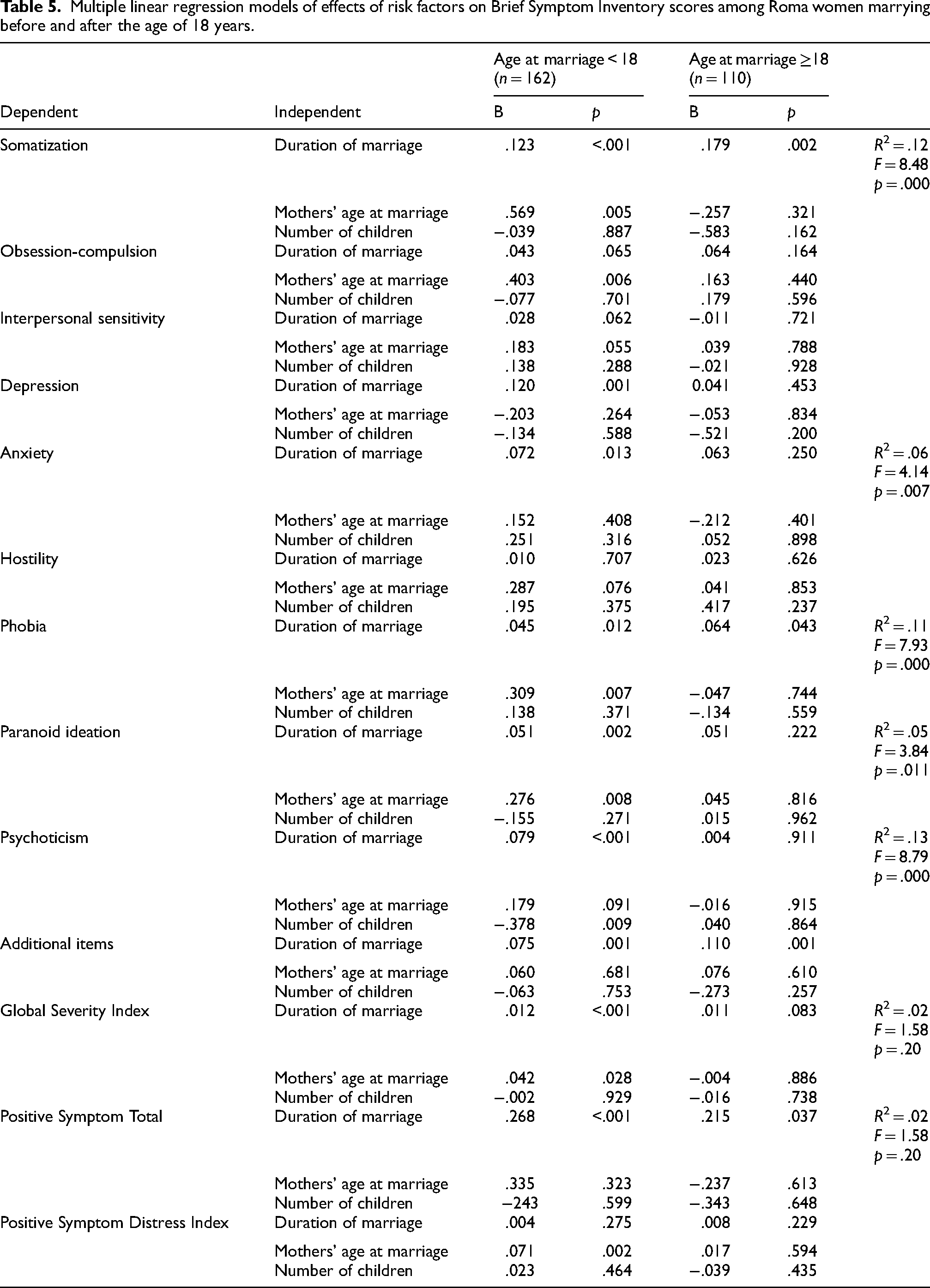
Table 5 summarizes the results of separate multiple linear regression analyses with the effects of the mother's age at marriage, duration of marriage, and number of children on the BSI scores in the women who married before and after 18 years of age (Table 5). Among the women who married before the age of 18, longer duration of marriage had a significant positive correlation with somatization, R2 = .12, F(3, 158) = 8.48, p = .000, depression, R2 = .10, F(3, 158) = 7.25, p = .000, anxiety, R2 = .06, F(3, 158) = 4.14, p = .007, phobia, R2 = .11, F(3, 158) = 7.93, p = .000, paranoid ideation, R2 = .05, F(3, 158) = 3.84, p = .011, and psychoticism, R2 = .13, F(3, 158) = 8.79, p = .000 (Table 5). In addition, a significant relationship was found between the duration of the marriage and the Global Severity Index and Positive Symptom Total. Among the women who married after the age of 18, a longer duration of marriage had an effect on somatization, R2 = .02, F(3, 106) = 1.58, p = .200 (Table 5).
Multiple linear regression models of effects of risk factors on Brief Symptom Inventory scores among Roma women marrying before and after the age of 18 years.
Discussion
The present study contributes to the growing literature on the mental health effects of early marriage in adult Roma women. More than half of the participants in this study were married early. Among these women, 14.2% married when they were 12–14 years old, and 85.8% married when they were 15–17 years of age (see Table 1 for demographic information). In Turkey, estimates of the prevalence of early marriage among Roma women vary between 30% and 50% (Tanrıverdi et al., 2012; Taylan, 2016).
As the duration of marriage increased, the levels of interpersonal sensitivity, somatization, depression, anxiety, phobia, paranoid thoughts, psychoticism, and scores on the Global Severity Index increased among the Roma women in the early marriage group in this study (Table 3). On the other hand, considerably less psychopathological symptomatology was found in the group that married after 18 years old. The results of the multiple regression analysis supported these findings (Table 5).
In a study undertaken to evaluate the relationship between mental health and age among Roma people in Greece, aside from hostility, women had significantly higher levels of psychological symptoms as measured by the Symptom Checklist-90-Revised (SCL-90-R), and these symptoms had a positive correlation with age (Kotrotsiou et al., 2014). Vorvolakos et al. (2012) compared sociodemographic and clinical features of Roma people with psychological disorders with those of non-Roma people with psychological disorders. They reported that most of the Roma group was female and had married early (mean age of marriage = 16.71 years). The researchers added that the Roma group had more symptoms of major depression, somatization, anxiety, hostility, and phobia than the other group (Vorvolakos et al., 2012). In their study in the United States, Le Strat et al. (2011) found that women who married in their childhood had higher rates of psychiatric and mood disorders rates than those who married in adulthood. Researchers also noted that a higher number of older women in the study had married early (Le Strat et al., 2011).
Marriage can have either positive or negative effects on mental health. It has been suggested that, compared to young adults who have married at a relatively early age, people who marry in early adulthood (20–29 years of age) are more satisfied with their lives and these marriages can be beneficial for their mental health in many respects (Uecker, 2012). Early marriage is a significant stressor that leads women to have difficulties in adolescence and can increase later exposure to other stressors (Alexandridis, 2016; Efevbera et al., 2017; Nour, 2009; Raj, 2010). In the present study, symptoms of psychological distress among Roma women in the early marriage group correlated with the duration of marriage. Longitudinal studies could confirm this and identify the factors that contribute to long-term impacts on mental health.
Limitations
This study examined only one population and the results may have limited generalizability. A similar ethnic group known as “Cono,” who do not consider themselves Roma and live in a different part of Adana, were not included in the study. Additionally, Roma girls younger than 18 years who were married at the time of the data collection were excluded from participating in the study for legal reasons. The study was cross-sectional so causal relationships cannot be confirmed. Lastly, this study was quantitative and did not ascertain potential aspects of the marital trajectory that could influence mental health outcomes. Marriage is a common and traditional practice for Roma women in Roma culture; it makes the conditions of life for Roma women even more challenging due to the difficulties and responsibilities that women face before completing their development in adolescence. A mixed-methods study could be conducted to gather more information about the lived experiences of this population, which is not studied frequently. Additional information could be obtained by interviewing both partners, women and men, in future studies.
Conclusion
This article reports the results of a study of a sample of 272 Roma women in Adana, Turkey. The findings may be specific to this setting but highlight the need for health professionals to protect and promote the mental health of Roma women. Almost two-thirds of women (59.6%) (n = 162) had married before the age of 18 years; of these, 14.2% (n = 22) married before the age of 15. Duration of marriage and age at marriage were significantly associated with higher levels of psychological symptoms in the women who married early. Women who married early reported more psychological symptoms on subscales of interpersonal sensitivity, somatization, depression, anxiety, phobia, paranoid thoughts, psychoticism. Future studies with larger sample sizes that include Roma women in other regions can shed light on the effects of early marriage on the mental state of Roma women.
Compliance with ethical standards
The study was conducted in accordance with the principles of the Declaration of Helsinki. Ethical approval was obtained from the University Ethical Board of Clinical Research and written permission was taken from the city governor. Participation in the study was voluntary and oral and written informed consent were obtained after the women included in the study were given information about the study, confidentiality, privacy, and their right to drop out of the study.
Footnotes
Declaration of conflicting interests
The author declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author received no financial support for the research, authorship, and/or publication of this article.