
Abstract
There is considerable variation in the presentation of mental health problems across cultural contexts. Most screening and assessment tools do not capture local idioms and culturally specific presentations of distress, thus introducing measurement error and overlooking meaningful variation in mental health. Before applying screening and assessment tools in a particular context, a qualitative exploration of locally salient idioms and expression of distress can help assess whether existing measures are appropriate in a specific context as well as what adaptations may improve their construct validity. We aimed to employ a mixed-methods approach to describe and measure cultural concepts of distress among female Congolese survivors of intimate partner violence in Nyarugusu refugee camp, Tanzania. This sequential study used data from 55 qualitative (free-listing and in-depth) interviews followed by 311 quantitative interviews that included assessments of symptoms of common mental disorder to explore whether the symptom constellations were consistent across these methodologies. Results from thematic analysis of qualitative data and exploratory factor analysis of quantitative data converged on three concepts of distress: huzuni (deep sadness), msongo wa mawazo (stress, too many thoughts), and hofu (fear). The psychometric properties of these constructs were comparable to those of the three original common mental disorders measured by the quantitative symptom assessment tools—anxiety, depression, and post-traumatic stress disorder—adding weight to the appropriateness of using these tools in this specific setting. This mixed-methods approach presents an innovative additional method for assessing the local “cultural fit” of globally used tools for measuring mental health in cross-cultural research.
Introduction
Whether psychiatric diagnoses are universal conditions that are present across cultures and contexts has been a long-standing debate in the fields of cultural psychiatry and global mental health (Canino & Alegria, 2008; Kleinman, 1977; Singer, 1975; Stein et al., 2013). Systematic reviews have consistently found evidence supporting the validity of questionnaires that assess common mental disorders across cultures (Baxter et al., 2013; Canino & Alegria, 2008; Gutierrez-Rojas et al., 2020). However, it remains unclear whether observed variation in the epidemiology of these disorders is due to differences in prevalence, the distribution of risk and protective factors, or to measurement error caused by applying assessment tools and diagnostic criteria for psychiatric disorders that are not valid in the study population and context (Kirmayer & Swartz, 2014; Kleinman, 1977). Literature on cultural concepts of distress, including idioms of distress and culture-bound syndromes, shows considerable variation in expressions of distress across populations and cultures (Haroz et al., 2017; Kohrt et al., 2014; Rees & Silove, 2011; Rees et al., 2009; Ventevogel et al., 2013). These findings do not definitively indicate whether this variation reflects unique expressions of universal disorders or distinct mental health problems. Regardless, it is important that diagnostic interviews and screening tools for research and programming engage appropriately with culturally specific presentations of distress (de Jong & van Ommeren, 2002). It is essential that the used instruments have face validity within the target population, which can be accomplished by using culturally relevant terms and concepts (Bolton & Bass, 2014).
There are different ways to incorporate cultural diversity in assessment of mental health issues. One way is to select an existing assessment tool, often based on “universal” International Classification of Diseases (ICD) or Diagnostic and Statistical Manual of Mental Disorders (DSM) criteria, and adapt it linguistically and culturally. The other way is to develop an entirely new instrument, bottom up, to capture locally salient signs and symptoms. Global psychiatric epidemiology studies have typically employed the first approach with variable degrees of adaptation and validation (Betancourt et al., 2012; Ertl et al., 2010; Kaaya et al., 2002; Scholte et al., 2011; van Ommeren et al., 1999; Ventevogel et al., 2014). Measures that have been developed or adapted to incorporate locally salient experiences have displayed incremental validity in their ability to predict related constructs, such as functional impairment, as compared to measures based on universal diagnoses that have not been culturally adapted (Jayawickreme et al., 2012; Rasmussen et al., 2014). Studies in Mozambique and Nepal have employed vignette-based assessments, which have been developed using western diagnostic criteria as a foundation, while using locally developed descriptions of cultural concepts of distress to identify cases of mental disorder in community-based research (Jordans et al., 2020; Patel et al., 2007). An alternative approach is to generate culturally specific assessment methods “from scratch” using ethnographic methods and take local experience as the starting point to build a contextually relevant instrument (Betancourt et al., 2009; Bolton & Tang, 2004; Chhim, 2012; Miller et al., 2006; Patel et al., 1997; Rasmussen et al., 2011). Such locally developed instruments can markedly differ from supposedly “universal” instruments in the sense that local categories and concepts may cut through professional nosological categories of mental disorders (Miller et al., 2006), but in other cases map quite closely. For example, in post-genocide Rwanda, rapid ethnographic research by Bolton and colleagues (2003) found that the local concept of agahinda gakabije closely resembled the symptoms of the DSM-defined depression, which prompted them to use a universal screening instrument for depression, with some cultural adaptations including integrating locally developed assessments of functional impairment (Bolton, 2003; Bolton & Tang, 2002), a process that has been replicated in other contexts (Betancourt et al., 2009; Bolton et al., 2004).
Using locally salient terms, concepts, and examples may improve identification of individuals with mental health problems, and integration of such terms in care provision may make mental health services more relevant to their experiences of distress, thereby improving engagement and retention in care. Integrating cultural concepts of distress into existing screening and assessment tools enhances face validity while also facilitating cross-study comparison and harmonization of data. Few studies have examined the consistency of item-level performance or the construct validity across cultures and contexts (Haroz et al., 2016).
This study aims to characterize cultural concepts of distress using a mixed-methods design employing complementary universalist and localized perspectives among survivors of intimate partner violence (IPV) in a protracted humanitarian context. IPV and other forms of gender-based violence are strong risk factors for common mental health problems globally (Ellsberg & Emmelin, 2014; Ellsberg et al., 2008; Rees et al., 2011; Shield & Rehm, 2015; Trevillion et al., 2012). Available data show a high burden of IPV and mental health problems in humanitarian settings. In line with these global findings, a strong correlation between experiences of IPV and worse mental health outcomes has also been found among Congolese refugee women (Familiar et al., 2021; Morof et al., 2014; Sipsma et al., 2015). This study uses data collected from Congolese survivors of IPV living in Nyarugusu Refugee Camp, Tanzania—a population and humanitarian context with high documented burden of IPV and associated mental health problems (Greene et al., 2016; Johnson et al., 2010; Lugova et al., 2020; Norman & Niehuus, 2015; Schmitt et al., 2021; Tankink et al., 2010). In this study, we compared the psychometric properties of common mental disorder constructs defined a priori (anxiety, depression, post-traumatic stress disorder) to locally defined constructs identified through an analysis of common presentations of distress.
Methods
We conducted a sequential mixed-methods study that integrated findings from a formative qualitative research study conducted in late 2015 with quantitative baseline data collected as part of a cluster randomized trial conducted in early 2017 (Creswell, 2013; NIH Office of Behavioral and Social Sciences, 2018).
Participants and procedures
This study was conducted in Nyarugusu, a protracted refugee camp setting located in Kigoma region in western Tanzania. Nyarugusu was established in 1996 to accommodate the influx of Congolese fleeing conflict in the eastern region of the Democratic Republic of the Congo (DRC). At the time the study started in 2015 there were approximately 65,000 Congolese and 2,500 Burundian persons residing in Nyarugusu as refugees. In mid-2015 approximately 85,000 additional people from Burundi sought protection in Nyarugusu, followed by continued arrivals from Burundi and the DRC, resulting in a population size of more than 150,000 people by 2018 (UNHCR, 2018). Tanzania continues to host a large population of Congolese and Burundian refugees (253,040 in June 2021), most of whom reside in camps (UNHCR, 2021).
Participants in the current study were recruited as part of a larger intervention development and feasibility trial aimed at reducing psychological distress and IPV among Congolese women who are refugees living in Nyarugusu. A critical aspect of the intervention development research that was conducted in preparation for the feasibility trial was to select and evaluate the performance of mental health outcome measures using a mixed-methods formative research process. The details of the intervention development process and cluster feasibility trial are provided elsewhere, but are summarized below (Greene et al., 2019, 2021; Tol et al., 2017). This study employed a mixed-methods, sequential exploratory design to investigate the construct validity of assessment tools for common mental disorders among female Congolese survivors of IPV. Together, these study phases included a qualitative research component to identify and describe the common symptoms of psychological distress among survivors of IPV. In the qualitative phase we recruited 55 local refugee workers affiliated with non-governmental organizations delivering mental health and/or gender-based violence programs in Nyarugusu to participate in free-listing interviews (n = 40) or in-depth key informant interviews (n = 15). Adults who are refugees and had experience working with humanitarian agencies on gender or health programs in Nyarugusu were invited by members of our research team and implementing partner to participate in free-listing interviews. People from the refugee community who were considered by UNHCR and its implementing partners to be knowledgeable in gender-based violence and mental health-related problems affecting women in the community were invited to participate in key informant interviews. All interviews were conducted in Kiswahili by trained female research assistants from the refugee community. The objective of these qualitative interviews was to identify and characterize common psychological problems affecting survivors of IPV in their community.
Following the qualitative research phase, we conducted quantitative assessments of psychological distress among 311 Congolese survivors of IPV who were enrolled in the feasibility trial. Congolese women were recruited from community-based women's groups to participate in the feasibility trial. Eligible women were adult Congolese people who were refugees living in Nyarugusu who had experienced past-year IPV and reported elevated levels of psychological distress. Quantitative assessments were also administered in Kiswahili by trained research assistants from the refugee community.
All procedures were reviewed and approved by the institutional review boards at the Johns Hopkins Bloomberg School of Public Health (IRB0007219), the Muhimbili University of Health and Allied Sciences (2014-10-27/AEC/Vol.X/56), and the Tanzania National Institute for Medical Research (NIMR/HQ/R.8a/Vol.IX/2016).
Measures
The free-listing interview guides asked respondents (1) to describe the most common problems faced by women who experience IPV in Nyarugusu, (2) which three of these reported mental health and psychosocial problems were most important and why, and (3) how women deal with the three most important problems. The in-depth interview guide asked separate key informants to describe the three most important problems identified in the free-listing interviews in terms of their symptoms, affected groups, causes, and appropriate responses or treatments in Nyarugusu. Qualitative interview guides are available as Supplemental Files 1 and 2.
Quantitative measures of psychological distress were selected to reflect the symptoms described in the qualitative interviews. These measures, which have been commonly used to measure common mental disorder symptoms in global mental health research, included the Hopkins Symptom Checklist, a 25-item measure assessing anxiety and depressive symptoms (Derogatis et al., 1974), and the Harvard Trauma Questionnaire, a 16-item measure assessing post-traumatic stress symptoms (Mollica et al., 1992). In a pilot treatment cohort study, we found evidence of good internal consistency, inter-rater reliability, test-retest reliability, and construct validity of the Swahili versions of these symptom scales within their original diagnostic domains – anxiety, depression, and post-traumatic stress disorder (Greene et al., 2019).
Data analysis
The importance of problems reported in the free-listing interviews was quantitatively ascertained using Smith‘s salience index of the three mental health and psychosocial items prioritized across the 40 interviews (Borgatti, 1999). We characterized the three most important mental health and psychosocial problems affecting survivors of IPV using thematic analysis of the key informant in-depth interview data. Two members of the research team independently read all key informant interview transcripts and generated codes within the interview domains: mental health symptoms, affected groups, causes of mental health problems, and appropriate interventions to address those problems. Any discrepancies in coding were reviewed and discussed with a third member of the research team.
We conducted an exploratory factor analysis of all items included in the Hopkins Symptom Checklist and Harvard Trauma Questionnaire collected at baseline from the 311 survivors of IPV who were enrolled in the cluster randomized feasibility study. There was no item-level missingness in these mental health outcomes at baseline. Given the ordinal nature of the response options, we used the polychoric correlation matrix to examine the covariance among the symptoms of psychological distress included in these assessment tools. Factors were extracted using information from the Eigenvalues, scree plot, and the proportion of variance explained by each factor. Items were retained on the factor on which the rotated factor loading was largest. In this analysis, we did not eliminate items with low loadings or cross-loading. We compared the internal consistency of the original subscales and those that emerged from the exploratory factor analysis. We examined the sensitivity to change of the original and emergent latent subscales by comparing the standardized mean difference from baseline to nine weeks in the sample using a structural equation model. Data on 36 participants (11.6%) of the sample were missing at the nine-week follow-up. Lastly, to explore the external construct validity we estimated the association between baseline characteristics that we would expect to be associated with psychological distress, including functional impairment, frequency of IPV, relationship quality, coping, social support (emotional, instrumental, financial), and history of potentially traumatic events. All quantitative analyses used a significance level of p < 0.05 and were conducted in Stata, Version 14 (StataCorp, 2015).
In this sequential mixed-methods study, we used our qualitative data to explore mental health experiences and constructs from the participant perspective. These data were applied during the design phase to inform the inclusion of quantitative items. We used triangulation to integrate these data in our analysis (Miles & Huberman, 1994). The factors that emerged from the exploratory factor analysis (quantitative) were compared to the descriptions of priority mental health problems from the formative research (qualitative). We explored similarities in the constellation of symptoms across these quantitative and qualitative constructs to evaluate the construct validity of the local concepts of distress explored in this analysis.
Results
Characteristics of sample
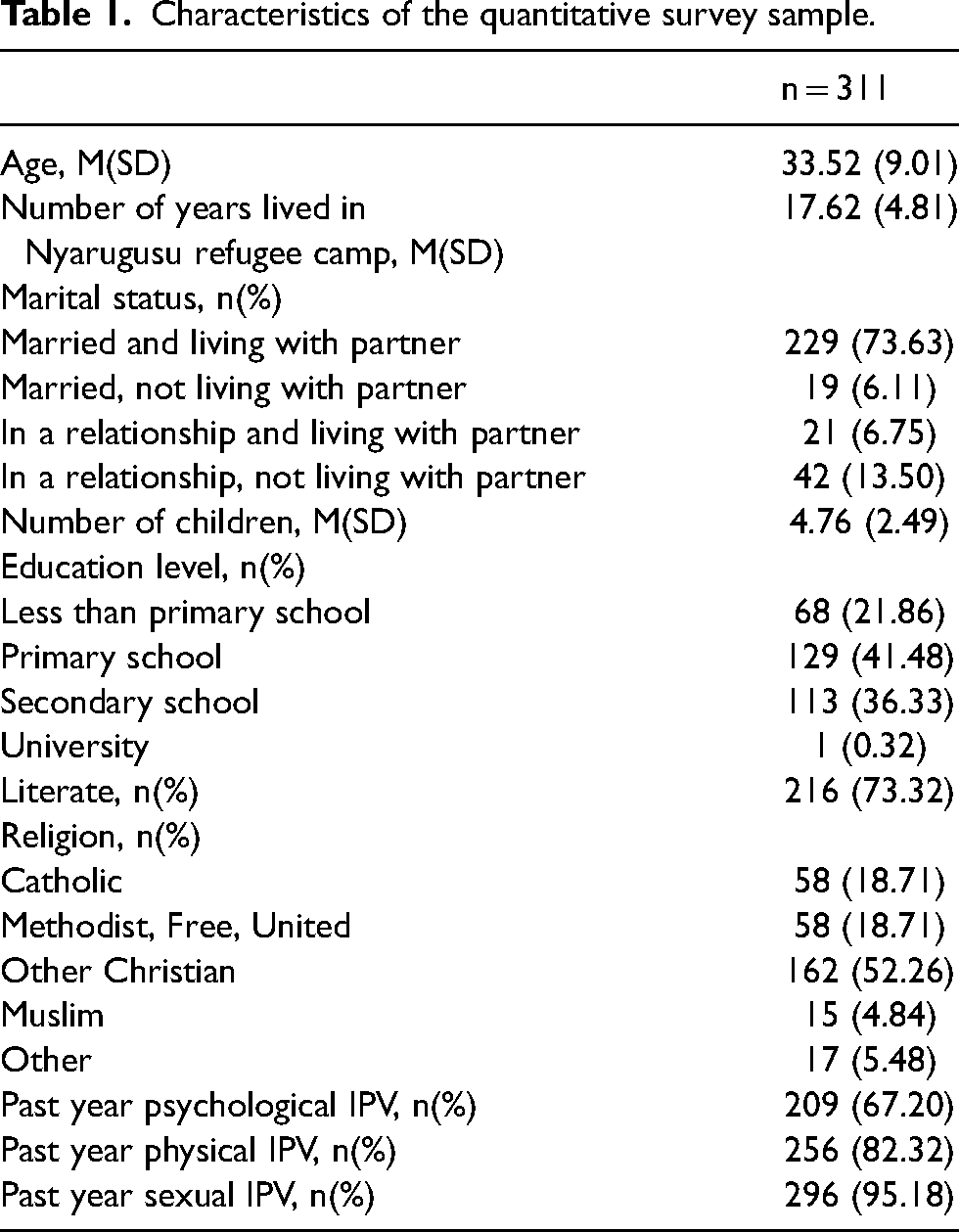
Fifty-five Congolese adults from the refugee community with experience or knowledge regarding mental health problems and IPV in their community completed free-listing (n = 40) or key informant in-depth interviews (n = 15). Participants included male and female adult Congolese workers from the refugee community who were selected because of their familiarity with the way Congolese women express distress given that they engage with IPV survivors in their work as health or protection worker and/or were themselves women from the refugee community. The 311 Congolese women who completed the quantitative survey and were enrolled in the study were 33.5 years of age (SD = 9.0), had lived in Nyarugusu refugee camp for 17.6 years (SD = 4.8), and had 4.8 children (SD = 2.5) on average. Most of them were married and living with their partner (73.6%), literate (73.3%), and Christian (89.7%). Twenty-two percent had less than a primary school education. All participants reported elevated distress and past-year IPV in order to be eligible for the study. The most common form of past-year IPV was sexual violence (95.2%), followed by physical (82.3%) and psychological violence (67.2%) (Table 1).
Qualitative descriptions of local concepts of distress affecting survivors of IPV in Nyarugusu refugee camp
In the qualitative free-listing interviews, adults from the refugee community who had worked with humanitarian agencies in Nyarugusu reported that the three most salient problems affecting women who experience IPV were: 1) msongo wa mawazo: stress or too many thoughts, which was characterized by silence, preferring to be alone, unhappiness, lack of self-care, loneliness, sleeplessness, headache, and heart pain; 2) huzuni: deep sadness, which was characterized by crying, silence, aggressiveness, being upset, looking down / head bent to the side, poor appetite, anger, and losing hope; and 3) hofu: fear, which was characterized by preferring to be alone, worry, being easily shocked, trembling, feeling unsettled, avoiding eye contact with others, and avoiding or being afraid of one‘s husband and other people. Additional details of these three locally salient mental health problems, including vulnerable groups, perceived causes, and acceptable treatment approaches, are described elsewhere (Greene et al., 2019).
Quantitative assessment of psychological distress among survivors of IPV in Nyarugusu refugee camp
Exploratory factor analysis of items assessing symptoms of depression, anxiety, and post-traumatic stress revealed two plausible factor solutions. The first, a single-factor solution, revealed that a single underlying factor describing psychological distress explained 22% of the variance in psychological distress symptoms (Table 2; Eigenvalues reported in Supplemental File 3). Most of the symptom items loaded strongly on the single factor, with the exception of the following items: in the past two weeks how often have you felt the problem of / been bothered by 1) faintness, dizziness, or weakness; 2) trouble sleeping; 3) inability to remember parts of the most traumatic or hurtful events; and 4) avoiding thoughts or feelings associated with the traumatic or hurtful experience. These items displayed very low factor loadings (<0.3) and high uniqueness (>0.9).
Exploratory factor analysis of mental health symptoms at baseline.
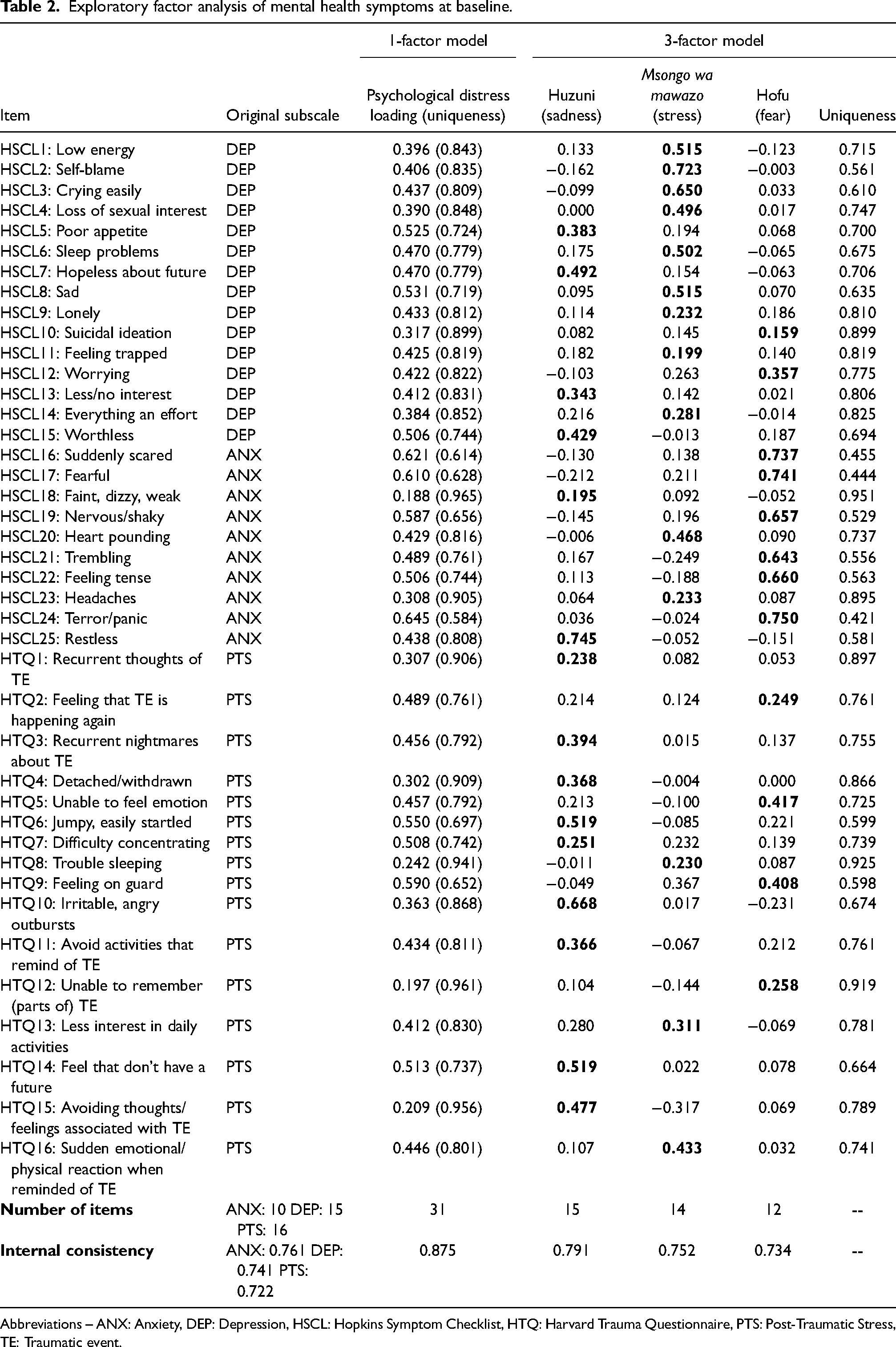
Abbreviations – ANX: Anxiety, DEP: Depression, HSCL: Hopkins Symptom Checklist, HTQ: Harvard Trauma Questionnaire, PTS: Post-Traumatic Stress, TE: Traumatic event.
Second, we identified a three-factor solution where each of the three extracted factors explained at least 5% of the variance and displayed eigenvalues greater than two (see Supplemental File 3). Cumulatively, these three factors explained 33.3% of the total variance in mental health symptoms.
Integrating the qualitative and quantitative descriptions of psychological distress
Review of the items included in these three factors revealed consistency with the three priority mental health problems affecting survivors of IPV that were reported through free-listing and key informant interviews during the formative phase of the study (Greene et al., 2019; Tol et al., 2017). As shown in Table 2, the first factor is similar to msongo wa mawazo (stress, too many thoughts). Items from the HSCL-25 and HTQ that loaded on this factor included self-blame, crying, low energy, sleep problems, sadness, loss of sexual interest, loneliness, heart pounding, headaches, feeling trapped, feeling that everything is an effort, less interest in daily activities, and reactivity. Items that loaded most strongly on the second factor, which resembled huzuni (deep sadness), included feeling restless, jumpy or easily startled, irritable or angry, hopeless, avoidance, social withdrawal, recurrent thoughts and nightmares related to a traumatic event, worthlessness, anhedonia, poor appetite, feeling faint/dizzy/weak, and difficulty concentrating. Lastly, the third factor resembled hofu (fear) and included items from the HSCL-25 and HTQ describing feeling suddenly scared, fearful, nervous/shaky, trembling, worried, tense, terror/panic, and that the traumatic event is happening again.
Some items displayed low loadings across factors and/or notable cross-loading: loneliness, suicidal ideation, difficulty concentrating, feeling the traumatic event will happen again, and feeling trapped. We identified a few discrepancies between the qualitative and quantitative findings, including that crying was the most commonly reported symptom of huzuni by key informants but loaded more strongly on the msongo wa mawazo factor in exploratory factor analyses. Social withdrawal and avoidance were features of all three local concepts of distress, primarily msongo wa mawazo and hofu; however, in the exploratory factor analysis symptoms of social withdrawal and avoidance loaded most strongly on huzuni.
Psychometric performance of local concepts of distress as compared to common mental disorders
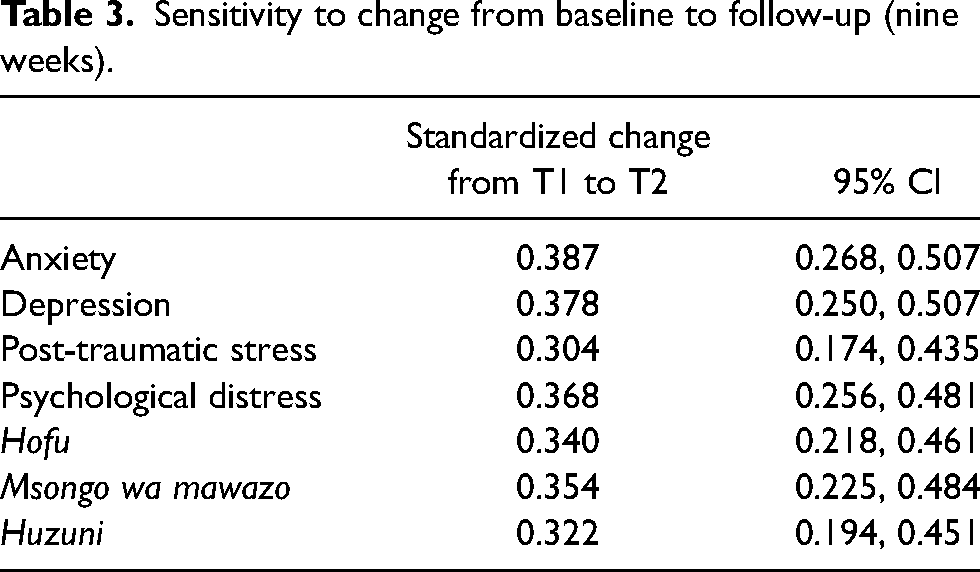
The emergent factors produced subscales of comparable sizes to the original diagnostic subscales and ranged from 12 to 15 items. The internal consistency was also comparable between the factors reflecting local concepts of distress (msongo wa mawazo: α = 0.752; huzuni: α = 0.791; hofu: α = 0.734) and common mental disorders (anxiety: α = 0.761; depression: α = 0.741; post-traumatic stress: α = 0.722). When examining sensitivity to change across these constructs from baseline to nine weeks post-baseline, we found similar standardized mean differences among the local concepts of distress and common mental disorders ranging from 0.304 for post-traumatic stress disorder (95% CI: 0.174, 0.435) to 0.387 for anxiety (95% CI: 0.268, 0.507; Table 3).
Sensitivity to change from baseline to follow-up (nine weeks).
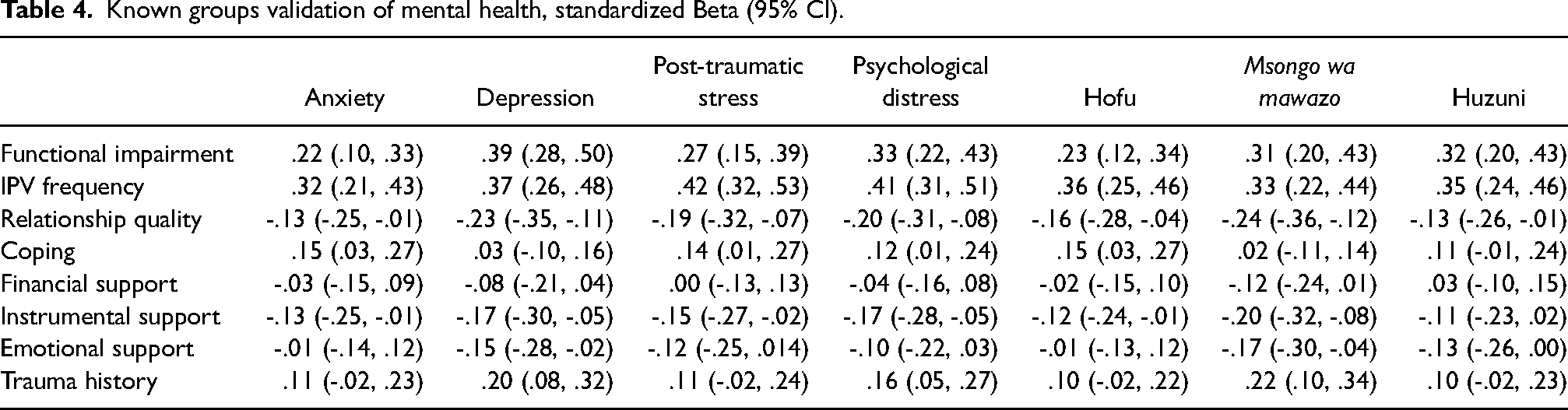
To examine whether factors we would expect to be associated with psychological distress were more strongly associated with common mental disorder constructs or local concepts of distress, we estimated their correlation with functional impairment, IPV frequency, relationship quality, coping, social support (financial, instrumental, emotional), and trauma history (Table 4). There was a significant linear association between all psychological distress constructs and greater functional impairment, more frequent experiences of IPV, and worse relationship quality. Higher levels of functional impairment were most strongly associated with depressive symptoms. More frequent IPV was most strongly associated with symptoms of post-traumatic stress disorder. Better relationship quality, more social support (financial, instrumental, emotional), and lower levels of trauma history were most strongly associated with lower levels of msongo wa mawazo (stress, too many thoughts). Coping, history of potentially traumatic events, and social support were inconsistently associated with symptoms of common mental disorder and local concepts of distress. Msongo wa mawazo was most strongly associated with less social support in all forms (emotional, instrumental, financial). We found that higher levels of coping were most strongly associated with higher symptoms of anxiety and hofu (fear).
Known groups validation of mental health, standardized Beta (95% CI).
Discussion
In this mixed-methods examination of mental health among female survivors of IPV in Nyarugusu refugee camp, we identified convergence between qualitative descriptions of psychological distress and the internal construct validity of quantitative psychological symptom screening tools. In this sample, cultural concepts of distress included huzuni (deep sadness), msongo wa mawazo (stress, too many thoughts), and hofu (fear). These cultural concepts of distress that emerged through qualitative interviews and exploratory factor analyses resembled those described in previous literature. For example, the idiom of “thinking too much” has been described in numerous countries in sub-Saharan Africa and other world regions as, similar to msongo wa mawazo, having a head full of intrusive thoughts, social withdrawal, sleep problems, headache, and heart palpitations (Kaiser et al., 2015). “Thinking too much” also displays some similarities to huzuni, both of which presented with symptoms of irritability, rumination and recurrent thoughts, anhedonia, and poor appetite (Kaiser et al., 2015). Researchers have suggested that “thinking too much” may be an indicator of depression risk and presents with overlapping symptomatology but is not synonymous with depression (Adaku et al., 2016; Patel et al., 1995; Ventevogel et al., 2013). Furthermore, similar to huzuni, the idiom of hozun has previously been described among people who were refugees in Darfur as an idiom of distress that included hopelessness, poor appetite, crying, recurrent and intrusive thoughts or nightmares, and irritability (Rasmussen et al., 2011). Cultural concepts similar to hofu have not been previously identified in the literature. However, in this sample, hofu resembled somatic presentations of anxiety and the hyperarousal presentation of stress-related mental health problems (Tay et al., 2015).
Despite the similarities observed among the cultural concepts of distress identified in this study and previous research, local conceptualizations of mental health problems may evolve over time and be context dependent and thus should not be considered fixed, static constructs (Ventevogel et al., 2013). This is particularly true in a protracted emergency setting where exposure to potentially traumatic events, such as IPV, may vary throughout displacement and, along with it, the culturally understood experience of distress (Rees & Silove, 2011). Previous idioms of distress described in eastern DRC and among Congolese people who are refugees in Tanzania show some variation to those described in this study, which provides further evidence of the dynamic nature of cultural concepts of distress and the importance of considering variation in distress across cultures and context (Mann, 2012; Tankink et al., 2010). Furthermore, there were symptoms of cultural concepts of distress identified in this study that deviated from the exploratory factor. These symptoms—crying, social withdrawal, and avoidance—cross-loaded on multiple factors and may reflect signs and symptoms that are common across dimensions of distress.
In this sample, we compared the psychometric properties of common mental disorder and local distress constructs. In general, we found adequate and comparable performance of these constructs, suggesting, from the perspective of reliability and internal construct validity, that both measurement approaches are acceptable. We also found evidence of adequate external validity, whereby higher levels of common mental disorder symptoms and local concepts of distress were associated with higher levels of IPV and potentially traumatic events and lower levels of social support and functioning. The sensitivity to change over a nine-week interval was comparable across the local concepts of distress as compared to anxiety, depression, and post-traumatic stress symptoms.
Surprisingly, we found greater coping was associated with greater symptoms of anxiety, post-traumatic stress disorder, hofu (fear), and general distress. One potential explanation is that participants with anxiety and stress-related mental health problems were more likely to utilize these coping strategies to alleviate symptoms of distress. It is also possible that anxiety, fear, and PTSD are common among women exposed to IPV and so too is the strength and resilience that helps them to survive this ongoing source of threat. Overall, the correlations among trauma, social support, functioning, and symptoms of distress support the relevance of both common mental disorders and local concepts of distress to the experiences of Congolese women in Nyarugusu refugee camp, thus supporting their validity. However, the observed differences in the strengths of these associations suggest possible differences in the causes and consequences of these presentations that should be explored in future research.
Findings from this research must be considered along with the following limitations. First, this study represents an analysis of data from across several phases of an intervention study for which the primary goal was not to examine cultural concepts of distress. However, a central aspect of our formative work and intervention development stage was to identify and evaluate the psychometric performance of our study outcome measures. We did not develop measurement tools to capture huzuni, hofu, and msongo wa mawazo a priori. Furthermore, we did not add items for symptoms described into the qualitative interviews that were not already present in symptom-screening tools beyond terminology that was introduced through translations and adaptations of the primary common mental disorder outcome measures. Future research could extend the mixed-methods approach described in this study by examining the influence of additional culturally specific items on the psychometric performance of these measures. Second, this study does not cover the full spectrum of mental disorders and omits cultural concepts of severe mental and substance use disorders. The scope of this study was defined during our formative research phase when we identified that symptoms consistent with common mental disorders most closely reflected the priority mental health problems affecting survivors of IPV in this study setting. Third, this study was conducted in a sample of female Congolese survivors of IPV in a refugee camp setting. Given the dynamic nature of cultural concepts of distress and the influence of context, the specific concepts and findings reported in this study may not be generalizable to other populations and settings. In addition to contextual generalizability, future research exploring the gendered aspects of distress that may shape experiences and symptoms of distress would strengthen our understanding of cultural concepts of distress across population groups. Despite these limitations, this study presents an approach to integrating qualitative and quantitative methods to explore cultural concepts of distress and their measurement that may be applied in other contexts.
Conclusions
We identified consistencies in cultural concepts of distress as compared to previous literature and extended these methods to describe a mixed-methods approach to facilitate cross-cultural comparability and relevance of instruments in global mental health research. The convergent qualitative and quantitative findings revealed considerable overlap in local concepts of distress and common symptom measurement tools. Integrating the qualitative and quantitative methodologies as described in this analysis presents an approach for examining the local construct validity of mental health assessment tools in cross-cultural research.
Characteristics of the quantitative survey sample.
Footnotes
Authorship contributions
WAT & SLL designed the parent study from which the data for this manuscript were collected. MCG and WAT drafted the manuscript. All authors contributed to drafting and revision of the final manuscript.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the Elrha (grant number 9923).