
Abstract
Public, policy, and media discourses increasingly frame loneliness as a “modern epidemic,” raising concerns that this complex emotional and social experience is being medicalized. However, empirical attempts to trace the extent and mechanisms of this process remain limited. Adopting a social constructionist perspective, this article operationally defines medicalization as the process of “making an experience medical” and analyzes 23,182 loneliness-related publications in the Web of Science (1980–2024) to map disciplinary locations, citation impact, and temporal growth patterns. Findings show that while psychology maintains a substantial presence, suggesting a prominence of emotional framings, there is marked growth in psychiatry, public health, and neurosciences. This trend may indicate that loneliness is being increasingly incorporated into mental health and neurobiological domains. Drawing on traditional medicalization theories, the article proposes a four-phase trajectory model as a provisional framework for further discussion. Within this framework, psychologization potentially facilitates an individualization that may serve as a basis for biomedical intervention. Furthermore, public health may play an ambivalent role: while retaining its social-reformist orientation, it could potentially accelerate medicalization by reframing loneliness as a “risk factor.” Looking forward, it remains to be seen whether frameworks viewing deficits in the quality and quantity of social relationships as health risks will emerge, potentially extending medicalization to domains beyond the individual as risk and surveillance technology advances. Despite its macro-level scope, this study provides empirical insights for the theoretical development of medicalization by exploring how everyday experience aligns with biomedical domains.
Introduction
Definition and approaches to loneliness: Universalism and constructionism
In recent years, loneliness has become a social and policy issue in many countries (Goldman et al., 2024). Its prevalence is considered problematic in many high-income nations (Surkalim et al., 2022). In January 2018, the UK government appointed the world’s first “Minister for Loneliness,” and Japan followed in February 2021, drawing widespread attention. In implementing loneliness-related policies, the UK government cited Perlman and Peplau (1981) and defined loneliness as “a subjective, unwelcome feeling of lack or loss of companionship. It happens when we have a mismatch between the quantity and quality of social relationships that we have, and those that we want” (UK Department for Digital, Culture, Media and Sport, 2018).
However, loneliness is also an everyday term, making it difficult to capture with a single definition. It is generally understood to include at least two distinct dimensions: emotional loneliness, resulting from the absence of intimate relationships, and social loneliness, arising from a lack of broader social networks (Weiss, 1974). Even when focusing solely on loneliness as an emotional experience, two major approaches can be identified. Universalist perspectives are found primarily in medicine, neuroscience, and psychology, and social constructionist perspectives are associated mainly with history, sociology, and cultural anthropology (Plamper, 2015). Universalist perspectives are exemplified by Ekman’s (1992) theory of “basic emotions,” which assumes that certain emotional states are universal across time and culture. This assumption implies that loneliness can be standardized and treated as a measurable, comparable psychological state. In psychology, the UCLA Loneliness Scale is one of the most widely used instruments for measuring the concept. It measures the intensity of loneliness, which is conceptualized as a unidimensional construct and defined as a subjective and unpleasant emotional experience that arises from a perceived discrepancy between desired and actual social relationships (Russell et al., 1980). A more reductionist view would treat loneliness as a neurophysiological response, identifying the brain regions activated when loneliness is induced through particular stimuli using medical imaging.
This paper used a social constructionist perspective, an approach that views loneliness as a social, cultural, and relational concept that transcends individual psychology and cognition (Ozawa-de Silva and Parsons, 2020). Rather than a simple stimulus–response reaction in the brain, loneliness is seen as a multifaceted and relational phenomenon that cannot be measured as a standard concept or using just one tool (Nambisan et al., 2024; Ozawa-de Silva and Parsons, 2020). Scholarship on the language of distress—which examines culturally-embedded bodily expressions of emotional suffering—is closely related to this perspective on human experience. Cultural-historical accounts of emotional states, such as histories of melancholy (e.g. Schmidt, 2007) and nostalgia (Arnold-Forster, 2024), also offer relevant insights. Alberti (2019) explored loneliness by looking at historical views of emotions. She argued that loneliness is a complex experience involving physiological sensations, and therefore more appropriately conceptualized as a cluster of emotions than a singular affective state. She noted, “Loneliness is not ahistorical or universal. Nor is it a single emotion. It is an individual and social cluster, composed of a wide variety of responses that include fear, anger, resentment, and sorrow” (Alberti, 2019: 223).
The Oxford English Dictionary states that the English words loneliness and lonely appeared in print at least as early as the late 16th century, initially referring to the physical state of being alone or to remote, uninhabited places. Over time, a distinction emerged between the physical condition of being alone and the internal feelings of sadness or estrangement that might be associated with it. In the late 18th century, against the backdrop of urbanization following the Industrial Revolution, the term loneliness acquired the subjective and negative connotations it carries today (Alberti, 2018).
Loneliness as a health risk: Public health concern or “medicalization”?
Loneliness is now increasingly recognized as a clear health risk as well as a social problem. Some have even described it as a “modern epidemic” (Murthy, 2020; The Lancet, 2023). Meta-analyses by Holt-Lunstad and colleagues are often cited as evidence of the health risks associated with loneliness and social disconnection (Holt-Lunstad et al., 2010, 2015). These studies quantified the “health risk” of loneliness and social disconnection by showing that people with poor social relationships have a 50% higher risk of premature death (Holt-Lunstad et al., 2010). This result was reinforced by a subsequent analysis (Holt-Lunstad et al., 2015) and was widely reported by domestic and international media outlets, often with headlines such as “loneliness is more dangerous than obesity” or “equivalent to smoking 15 cigarettes a day.” Since then, simplified expressions such as “having few friends leads to early death” have spread through popular media. Loneliness has increasingly been portrayed as the root cause of nearly all adverse health outcomes (Park et al., 2020), leading to it being treated as a public health “epidemic” rather than an individual concern (Murthy, 2020).
In 2018, a discussion began in the Correspondence section of the medical journal The Lancet, triggered by a letter from American neuroscientists (Cacioppo and Cacioppo, 2018: 426), which stated: Imagine a condition that makes a person irritable, depressed, and self-centred, and is associated with a 26% increase in the risk of premature mortality. Imagine too that in industrialised countries around a third of people are affected by this condition, with one person in 12 affected severely, and that these proportions are increasing. Income, education, sex, and ethnicity are not protective, and the condition is contagious. The effects of the condition are not attributable to some peculiarity of the character of a subset of individuals, they are a result of the condition affecting ordinary people. Such a condition exists—loneliness.
After citing the meta-analysis mentioned above, they concluded by emphasizing the mission of medicine and public health: Loneliness is a public health problem that can be largely solved in our lifetime but doing so will require the full engagement and support of the medical community. The physical health and mental health of a growing number of afflicted individuals and their families and friends are at stake.
A rebuttal letter followed from British anthropologists (McLennan and Ulijaszek, 2018: 1480), stating: Loneliness was recently described in The Lancet as a public health problem that needs to be solved by the medical community (Feb 3, p. 426). We believe that the medicalisation of loneliness in this way is damaging, especially at a time when the issue is making its way into public understanding.
They stated that the real health risk factor was “social disconnection” and that loneliness was a unifying issue. They then argued: Medicalisation of loneliness will discourage the collaboration needed, and medicine probably has no effective instruments with which to single-handedly address the absence of human connection.
This brief correspondence did not explicitly define “medicalization,” but the authors’ clear concern was that if a social issue was framed as a public health problem, the response to that problem would be dominated by medical solutions. Public health, in its original conception, encompassed both social reform-oriented approaches and biomedical approaches. However, in recent years, the field has shown a tendency toward medicalization, with growing reliance on technological and biomedical solutions and an increasing individualization of health problems (Nunes, 2025). In 2023, the World Health Organization established a Commission on Social Connection, marking the formal recognition of loneliness as a global public health issue. Treating subjective feelings of loneliness as a health risk and using emotive public health messaging such as “loneliness causes early death” may itself be understood as part of the social construction of risk (Lupton, 2013).
This paper shares these concerns. Building on them, I examine the extent to which the complex emotion and experience of loneliness is being framed within a medicalized context, particularly in terms of the individualization and biomedicalization of health, and, if so, in which domains and to what extent. My aim was to explore current academic trends in a neutral manner and then to engage critically with the issue.
Definition of medicalization and the medicalization of emotion
What conditions must be met to claim that a given phenomenon has been “medicalized”? There are several representative definitions of medicalization. The term is commonly used in everyday contexts, but the most influential scholarly definition was offered by Conrad and Schneider (1992): “Medicalization consists of defining a problem in medical terms, using medical language to describe it, adopting a medical framework to understand it, or using medical intervention to ‘treat’ it” (p. 211).
Medicalization theory originated with early critical discussions of medicine and science by Zola (1972). He examined how medicine and medical professionals expanded their jurisdiction as a means of exercising social control over various forms of “deviance,” defined as problematic behaviors and social issues. Later research, particularly that of Conrad (2007), developed the concept into a more neutral analytical framework that describes the social processes through which medical categories are constructed. In recent decades, scholars have pointed out that a wide range of human problems are being redefined as conditions requiring medical treatment (Crawford, 1980).
Many theoretical works have discussed medicalization, but conceptual definitions of medicalization vary considerably across empirical research. In 31 of 50 papers examined in a review (van Dijk et al., 2020), the term was not explicitly defined. Many studies drew on Conrad and Schneider’s (1992) definition, but still fell into at least 10 distinct categories that could be organized by whether they used a macro or micro perspective, and a value-neutral or more critical view. There was no clear association between research topics and definitions, leading Van Dijk and colleagues to conclude that definitions of medicalization are context-dependent. There is therefore no established guideline indicating which definition of medicalization should be adopted when discussing loneliness, whether as an individual emotion or as a social phenomenon.
Few studies have examined the medicalization of loneliness. Loneliness can be linked to several dimensions of medicalization. These include the medicalization of emotions (e.g. the medical delineation between ordinary sadness and clinical depression, or normal anxiety and social anxiety disorder; Horwitz and Wakefield, 2007); the medicalization of daily life, given that loneliness is an experience that anyone may encounter (e.g. childbirth or menopause; Lock, 2004); and biomedicalization, identifying and controlling biological causal mechanisms (Clarke et al., 2003). However, only a few papers have engaged critically with the issue and provided explicit definitions of medicalization (Klinenberg and Leigh, 2024). Alberti (2019), for instance, argued that excessive anxiety surrounding loneliness is almost a moral panic. She cited media reports about neuroscientists developing a “loneliness drug” as evidence for growing concerns about medicalization (p. 276). Indeed, efforts to explore bioscientific treatments are already underway. Neuroscientific approaches are particularly prominent, including research on neurotransmitters that may mitigate the negative effects of loneliness (Cacioppo and Cacioppo, 2015; Entis, 2019). Some studies have also reported on medical interventions to alleviate loneliness, such as intranasal sprays designed to increase oxytocin levels in the brain (Entis, 2019; Shamai-Leshem et al., 2025).
There is an abundance of anecdotal accounts, editorials, and popular press articles discussing the “medicalization of loneliness.” However, to my knowledge, there are no academic studies that focus specifically on the medicalization of loneliness. More broadly, discussions of medicalization grounded in empirical data remain limited even outside the context of loneliness, and it has been pointed out that neither researchers nor governments collect quantitative data (Conrad, 2007; Conrad et al., 2010).
This paper therefore explores whether loneliness has been “medicalized” using bibliometric data patterns and a clear operational definition. I used the Web of Science (WoS) database of academic literature to examine (1) the current distribution of fields and topics in loneliness-related literature, (2) temporal trends in fields and topics, and (3) growth patterns across disciplines and thematic areas. I operationally defined “medicalization” as “making an experience medical.” This definition was chosen because loneliness is fundamentally an individual “experience,” and therefore requires a micro-level focus (van Dijk et al., 2020). This definition was also considered the most value-neutral among those used in previous studies, because it has been argued that the term medicalization should ideally be used in a non-normative manner (Williams et al., 2008).
Methods
I examined the extent of medicalization by analyzing temporal changes in the academic literature on loneliness. This methodological approach was inspired by the works of Conrad (2007), who used similar strategies (e.g. tracking changes in the number of disorders listed in each edition of the Diagnostic and Statistical Manual of Mental Disorders, analyzing the expansion of total page count, or assessing increases in medical expenditure).
Study scope and data extraction
I collected data from WoS, a citation database that contains literature from a variety of academic fields. It is the world’s largest publisher-independent database, and is operated by Clarivate. The search strategy was based on a Topic search for “loneliness” in WoS, initially restricted to English-language articles and review articles published between 1 January 1980 and 31 December 2024 (database access date: 12 August 2025). The study period was set because Citation Topics are available from 1980 onward.
This initial search yielded 24,044 records but included some records also indexed under document types other than articles or reviews. The results were therefore manually filtered to retain only articles and reviews. The final dataset contained 23,182 documents.
To identify the academic fields and topics in which loneliness-related literature is published, I used three classification schemes provided by WoS: Research Areas (RA) and the Meso- and Micro-level Citation Topics. The analyses used InCites, a data analysis tool integrated with WoS. InCites enables detailed investigation of research trends across fields, such as the number of publications, citation counts, and citation patterns within specific research areas. Year-by-year data on research topics cannot be obtained directly from the WoS core system, and InCites was therefore used for this analysis.
In the core WoS platform, the Research Area classification consists of 5 major categories and 254 subcategories (as of August 2025). Each document is assigned to one or more research areas based on the subject categories of the journals in which it is published (https://incites.zendesk.com/hc/en-gb/articles/22586272202513-Web-of-Science-Research-Areas).The InCites category corresponding to the WoS Research Area is listed under “Web of Science,” but the classification is more granular than in the core WoS database. For example, WoS may classify a journal under the broad category of Psychology, but InCites subdivides it into more specific fields such as Psychology, Multidisciplinary or Psychology, Clinical.
The Citation Topics classification is a proprietary WoS taxonomy introduced in December 2020. Using citation relationships at the level of individual papers, the system generates clusters of publications that share similar research themes. This makes it possible to capture dynamic developments in research topics that cannot be fully represented by journal-based classifications such as Research Areas. Using a citation clustering algorithm, each document published from 1980 onward is automatically labeled. When classification updates occur, the revised taxonomy is retroactively applied. In other words, as new publications appear, they are added to existing topic clusters, and new clusters may also emerge, allowing the system to reflect current research trends more accurately. The latest version of the classification includes 3 hierarchical levels, with 10 broad “macro” clusters, 326 intermediate “meso” clusters, and 2478 fine-grained “micro” clusters (https://incites.zendesk.com/hc/en-gb/articles/22514077746961-Citation-Topics?utm). In this study, I examined the meso- and micro-level classifications or topics.
Analysis
I used the number of publications and citation counts for each field for the simple tabulation of Research Areas and Citation Topics. To adjust for differences in field size, I calculated the Average Citations per Paper. To analyze temporal changes in Research Areas and Citation Topics, I used two indicators: the slope (per year) obtained from a linear regression line, and the relative growth ratio (RGR). These indicators were selected because they can be calculated even when the appearance of a field or topic varies across the 1980–2024 period, when the initial value is zero or extremely small, or when certain years contain no publications.
The slope (per year) was derived from a linear regression analysis in which publication year was treated as the independent variable and the number of publications as the dependent variable. The slope coefficient represents the average annual linear change increase in the number of publications and can be calculated even when the dataset includes years with zero publications.
Relative growth ratio (RGR) was calculated to measure the relative growth since the first year in which publications appeared. Specifically, RGR was obtained by dividing the number of publications in the final year by that in the first year with a nonzero publication count, thereby indicating the relative magnitude of growth within each research field.
Findings
Areas and topics of loneliness-related papers
There were 23,182 loneliness-related publications from 1980 to 2024, tabulated by Research Area and meso- and micro-level Citation Topics. The top 30 fields were extracted (Table 1). I calculated the proportion of loneliness-related papers within all publications assigned to each Research Area. The most common fields were Psychiatry (10.91%), Public, Environmental & Occupational Health (8.72%), and Psychology, Multidisciplinary (7.41%). When lower-level subcategories were aggregated, it was clear that the overwhelming proportion of loneliness-related articles were published in psychology and related disciplines. Neurosciences (1.66%) and Clinical Neurology (1.65%) also ranked among the top fields.
Top 30 research areas and topics of loneliness articles from 1980 to 2024 (by article count).
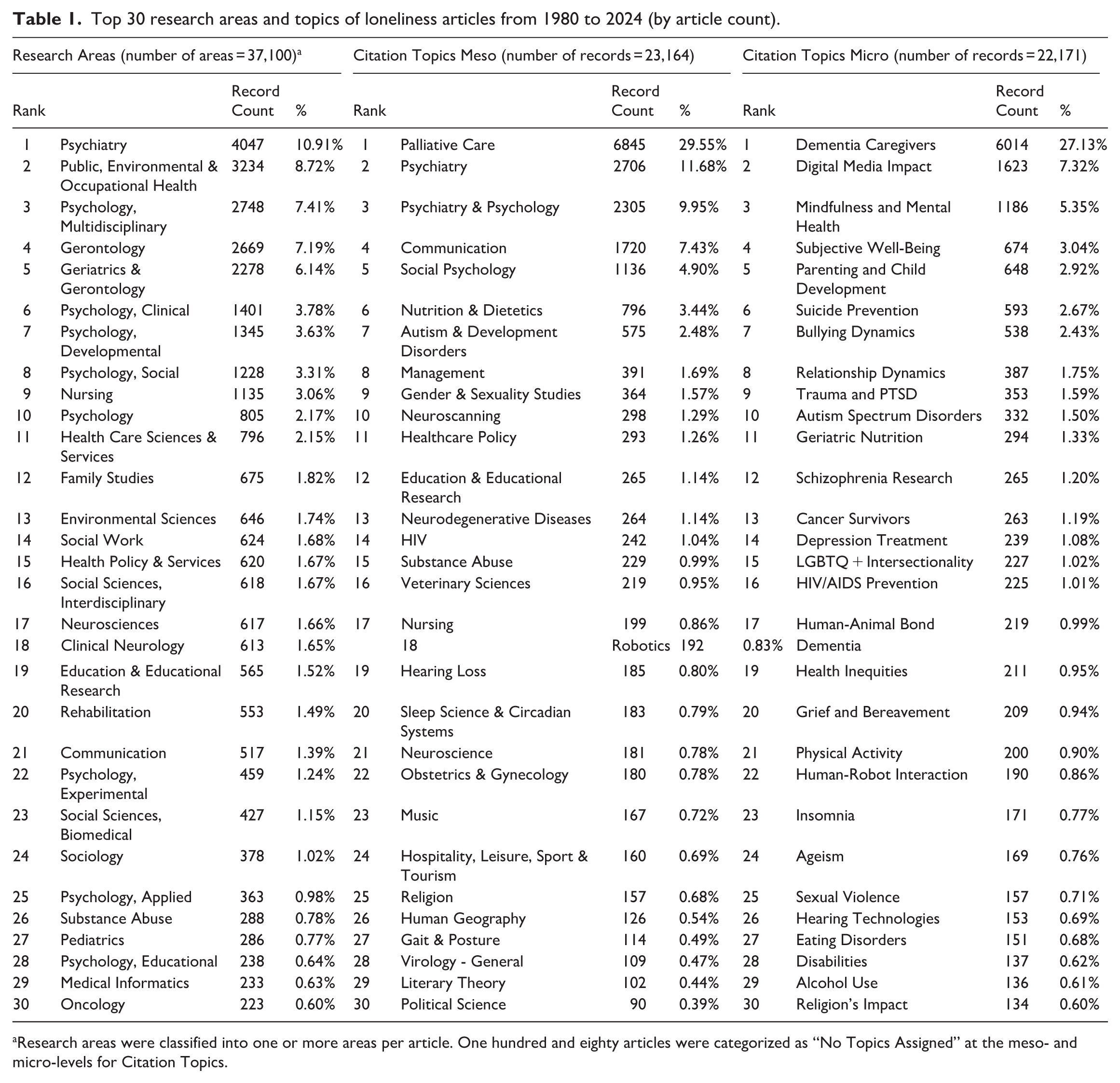
Research areas were classified into one or more areas per article. One hundred and eighty articles were categorized as “No Topics Assigned” at the meso- and micro-levels for Citation Topics.
The most common categories in both meso- and micro-categories of Citation Topics related to older adults (e.g. Palliative Care: 29.55%, Dementia Caregivers: 27.13%). At the meso-level, numerous studies were found in areas such as Neuroscanning (1.29%) and Neurodegenerative Diseases (1.14%) as well as psychiatry and psychology. At the micro-level, topics were more widely dispersed: in addition to Mindfulness and Mental Health (5.35%), several highly ranked issues concerned young people, including education, social welfare, and minority-related themes (parenting, bullying, suicide, LGBTQ+). Technology-related issues (digital media impact, human–robot interaction) were also common.
To examine the influence of each field while adjusting for differences in publication volume, the top 30 fields in Table 1 were re-ranked by Average Citations per Paper (Table 2). Within Research Areas, the fields with the most citations were psychology-related, indicating substantial citation influence. Psychiatry (rank 13th) and Public, Environmental & Occupational Health (23rd) had the largest publication counts, but Neurosciences (11th) showed higher average citations per paper, with Clinical Neurology (16th) also ranking near the top. At the meso-level, Neuroscience topics (4th) received particularly high citation counts relative to the number of publications. At the micro-level, citations were more widely dispersed, given the finer topic classification.
Top 30 research areas and topics (by average citations).
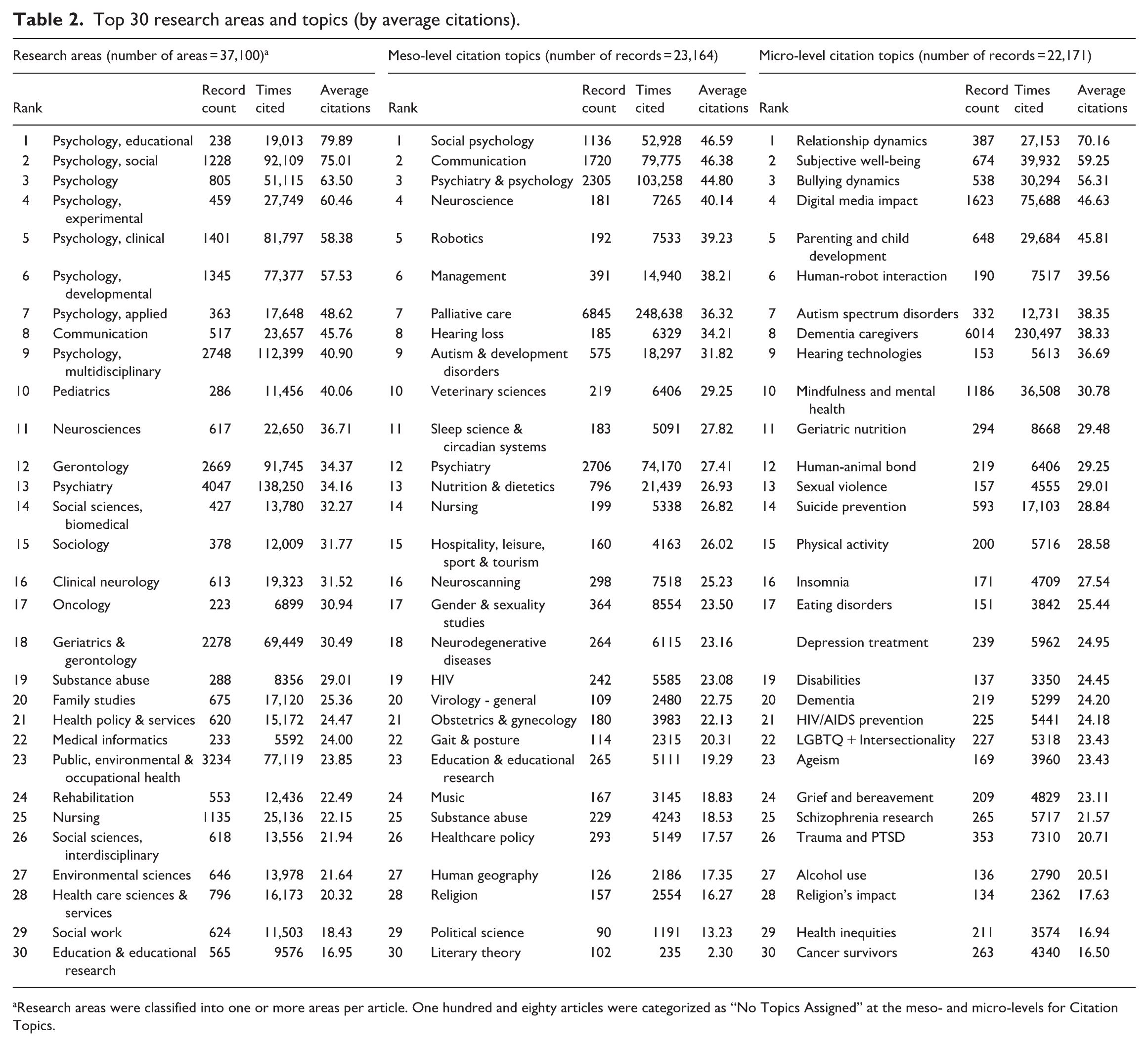
Research areas were classified into one or more areas per article. One hundred and eighty articles were categorized as “No Topics Assigned” at the meso- and micro-levels for Citation Topics.
Trends and growth patterns in research areas and topics
There was a proportional increase in the percentage of the total number of articles published annually across all research areas. The increase in the 2000s, particularly around 2018, was rapid, with 95.3% of all articles being published after 2000 and 65.2% after 2020.
Focusing on the top 20 research areas, Figure 1 shows changes in the proportion of loneliness-related publications relative to all publications in each field between 1980 and 2024. The sharp rise in Psychiatry and Public Health is striking. Both fields experienced explosive growth following the onset of the COVID-19 pandemic around 2020, although the increase had already accelerated in the late 2010s, particularly around 2018. Turning to Neurosciences and Clinical Neurology, both fields show a steady upward trend over the longer term, but a pronounced increase became evident only around 2020.
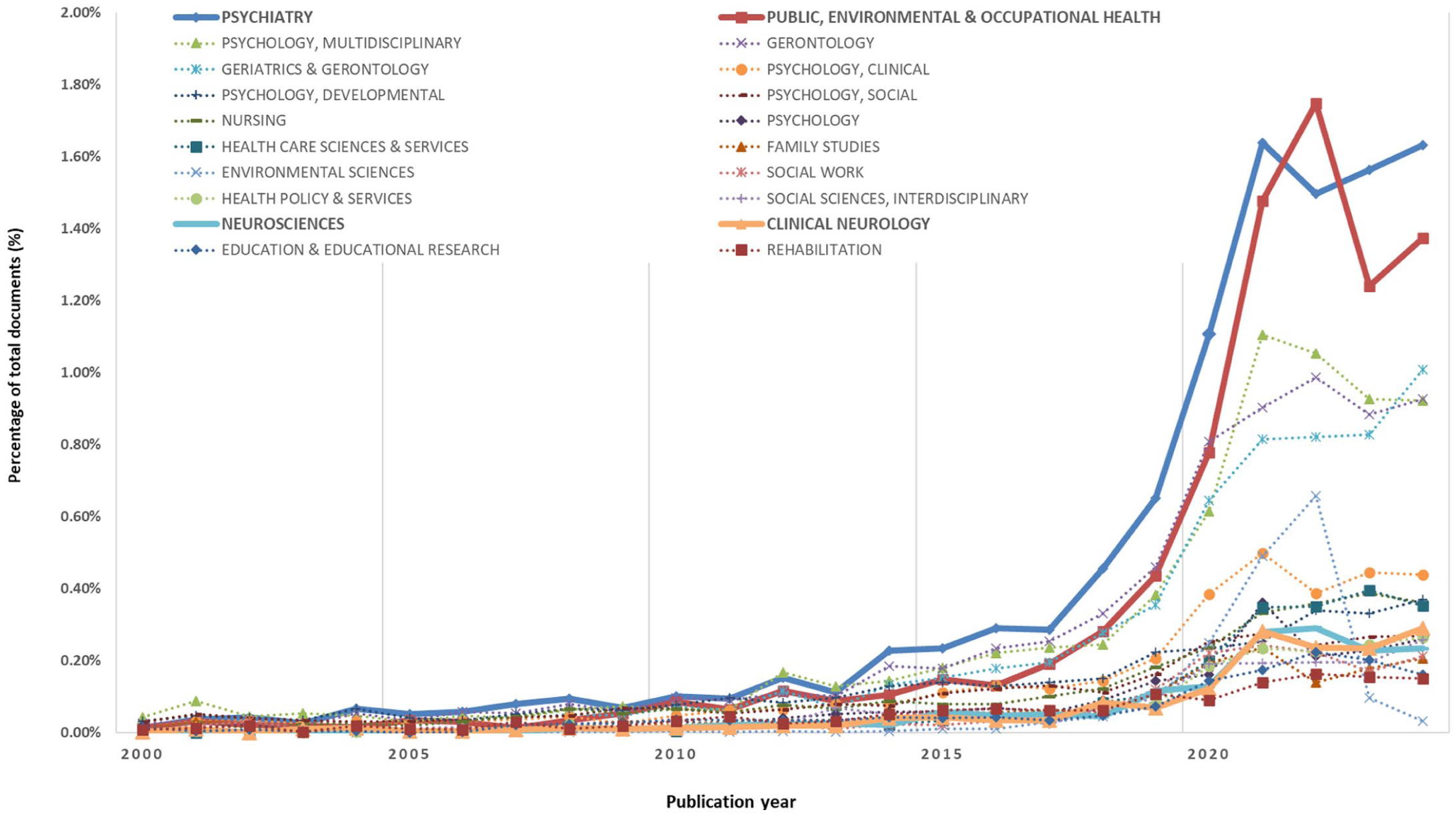
Top 20 research areas showing changes in the proportion of loneliness-related publications relative to all publications in each field (1980–2024).
Next, to examine temporal changes in research areas and topics in greater detail, I calculated the slope (per year) and the relative growth ratio. The slope shows which research areas had the largest absolute increases in publication counts, and the relative growth ratio indicates the relative magnitude of growth from the first year with a nonzero publication count to the final year. To identify areas with high relative growth, I selected the top 20 research areas and topics ranked by relative growth ratio and examined their growth patterns using scatterplots (Figure 2).
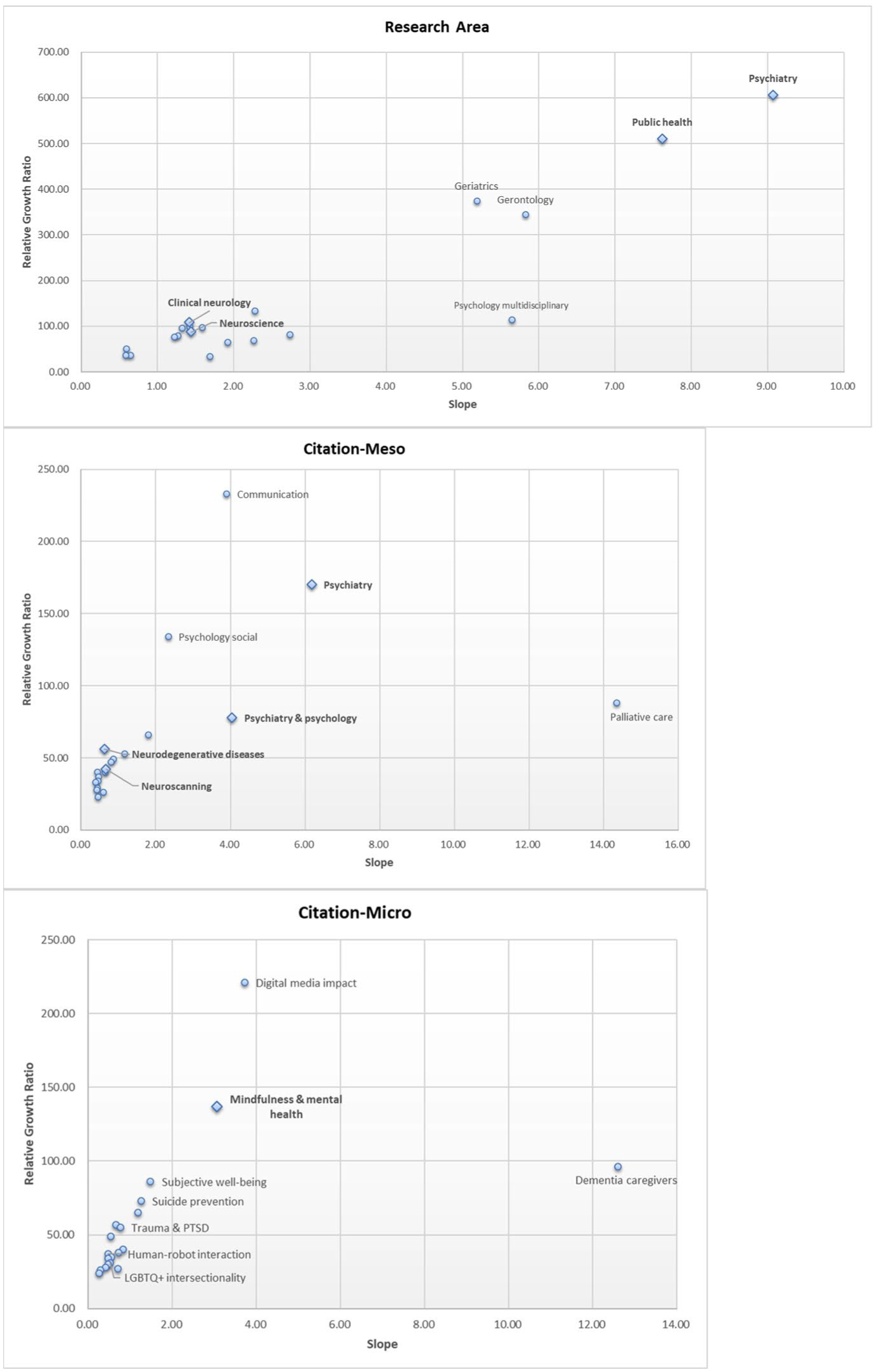
Growth patterns by slope and relative growth ratio for the top 20 research areas and citation topics (ranked by relative growth ratio).
Overall, the scatterplots for research areas and meso- and micro-level citation topics all showed an upward-sloping relationship. Research areas with large annual increases in publication counts also tended to show high relative growth ratios. Research areas and topics plotted in the upper-right quadrant (high slope, high RGR) were considered to be “hot” research areas or topics, because they are expanding in both absolute numbers and extent of growth. These can be interpreted as well-established research areas experiencing substantial growth; Psychiatry and Public Health were particularly prominent.
The upper-left quadrant (low slope, high RGR) represents emerging research areas or topics. The accumulation of publications is still small, but these areas are showing high relative growth ratios. Examples include the meso-level topics Communication and Psychology (Social), and the micro topics Digital Media Impact and Mindfulness and Mental Health.
The lower-right quadrant (high slope, low RGR) represents large, mature research areas or topics. The relative increase in this quadrant is weaker than in emerging fields, but these topics are central, stable domains of scholarly activity. Representative examples include the meso-level topic Palliative Care and the micro-level topic Dementia Caregivers.
The relative growth ratios of neuro-related, bio-related, and mental health-related fields—the primary interest of this study—all indicate substantial growth. Clinical Neurology (108.00; 7th) and Neurosciences (87.00; 11th) were among the research areas with the highest relative growth ratios. Among the meso-topics, Psychiatry (170.00; 2nd), Psychiatry & Psychology (77.67; 5th), Neurodegenerative Diseases (56.00; 7th), and Neuroscanning (42.00; 11th) showed substantial growth. Mindfulness & Mental Health (137.00; 2nd) showed particularly substantial growth among the micro-topics. Overall, neuro- and mental health-related areas and topics were among the domains with the highest relative growth ratios.
Discussion
Changes in topics and trends in the literature on loneliness
The descriptive overview of the entire study period revealed a clear dominance of psychology-related research areas in the field of loneliness (Table 1). While publication norms and primary modes of dissemination (e.g. books, journal articles) vary across disciplines, psychology accounted for the largest number of articles throughout the period and also had substantial influence when measured by average citations per paper (Table 2). This finding suggests that, of the two dimensions of loneliness, emotional and social (Weiss, 1974), the emotional dimension has been the primary focus of scholarly investigation. This quantitative dominance of psychology does not necessarily contradict the medicalization thesis; rather, it may indicate a “psychologization” of loneliness that provides the conceptual infrastructure for subsequent biomedical interventions. However, the influence of neuroscience was also evident. Despite a larger overall volume of publications in public health and psychiatry, Neurosciences had higher average citations per paper, and Clinical Neurology also ranked near the top in citations per paper (Table 2). Taken together, these results suggest that neuroscientific fields exert a strong influence relative to their smaller publication volume.
I then analyzed temporal trends to examine the “-zation” aspect of medicalization, meaning its dynamic expansion over time (Figure 1). The research areas with the strongest or most substantial growth were those most closely aligned with biomedical and clinical framings, particularly Psychiatry, Public Health, Clinical Neurology, and Neurosciences (as shown in Figure 2). Mindfulness & Mental Health also emerged as a topical cluster with a high relative growth ratio. Research in public health, a field situated at the interdisciplinary intersection of medicine and society, showed a particularly marked increase from the mid-2010s (Figure 1). This period coincides with the publication of the meta-analyses by Holt-Lunstad et al. (2010, 2015) and Marmot’s final European report on social determinants and the health divide (Marmot and UCL Institute of Health Equity, 2014). It can therefore be interpreted as a time when the significance of public health as a nexus between medicine and society was being re-examined.
Taken together, my findings highlight patterns consistent with the view that loneliness is being medicalized, when medicalization is defined as “Making an experience medical” (van Dijk et al., 2020). This interpretation is supported by both the dominance of “medical” fields (particularly the biosciences and mental health-related areas and topics), and the dynamic, temporal expansion in the literature.
Possible types and directions of medicalization of loneliness
This section interprets the findings presented in the previous section in light of representative theories of medicalization. Specifically, it considers the four types of medicalization proposed by Conrad (2007: (1) extension, (2) expansion, (3) enhancement, and (4) continuity, to explore the potential direction of the medicalization of loneliness.
Extension is a type of medicalization in which the jurisdiction of medicine extends beyond its conventional boundaries into new domains such as everyday experiences. For loneliness, the rapid increase in research in the fields of public health and psychiatry (Figure 1) suggests both that this everyday experience is being socialized as a problem and that it is being perceived as a health risk. Furthermore, given the surge in topics such as “Mindfulness & Mental Health,” it may be reasonable to regard loneliness as becoming incorporated into this broader trend of extension within the “mental health” domain.
Typical examples of redefining “normal” emotions as medical conditions and targeting them for intervention are shyness and worry, which have been transformed into social anxiety disorder (SAD) and generalized anxiety disorder (GAD), respectively (Starkstein, 2018). This shift also reflects cultural norms that pathologize social anxiety (Scott, 2006); in societies valuing assertiveness, shyness is more readily framed as a medical problem (Starkstein, 2018). The same applies to loneliness. The meaning of being alone that is accepted in Euro-American contexts may not be shared in other cultures (Ozawa-de Silva and Parsons, 2020). Although not discernible solely from the bibliometric data analyzed in this study, it is possible that the degree to which loneliness is problematized and defined, as well as the progression of its medicalization, vary across different regional and cultural contexts.
Expansion is the broadening of the definition or scope of an existing disease category. In this process, diagnostic criteria are relaxed or modified so that more people or situations fit the diagnosis. In this study, the psychiatry research area showed substantial increases in both publication volume and growth, suggesting that loneliness is becoming more closely linked to psychiatric frameworks. This may reflect a more general trend in which thresholds for pathology in psychiatry are broadened, allowing mild or ambiguous emotional states to be incorporated into existing diagnoses.
A comparable case would be the series of developments culminating in the introduction of Prolonged Grief Disorder as a distinct diagnosis, which has been criticized as part of a broader psychiatric expansion of diagnostic boundaries around grief and bereavement (Gurley-Green et al., 2025). Following the introduction of the diagnosis, research has begun to investigate biological markers and to explore pharmacological approaches (e.g. the use of naltrexone), indicating a shift toward medical intervention. Similarly, loneliness is frequently discussed in relation to depression within psychiatric research (Homma, 2025). If it follows a trajectory similar to that of normal grief, it seems likely that loneliness will increasingly be subsumed into existing psychiatric categories.
Enhancement is the use of medical interventions to augment human functioning rather than treat disease. Practices like shifting “normal” bodily traits toward socially desirable norms have become increasingly feasible because of advances in genetics and biotechnology. A relevant example in loneliness has been termed neuro/cognitive enhancement (Farah et al., 2004). This includes the use of pharmaceuticals that were originally intended to treat disease by healthy individuals to adjust mood or cognitive performance (Erler and Forlini, 2020). If loneliness were seen as an undesirable emotion, and medical or technological interventions were used to generate a more positive effect at the level of individual practice, this would constitute affective enhancement (Erler and Forlini, 2020). From a macro perspective, it could also be described as a form of pharmaceuticalization, defined as “the translation or transformation of human conditions, capabilities and capacities into opportunities for pharmaceutical intervention” (Williams et al., 2011).
Results also show evidence of strong influence and substantial growth in studies on loneliness in both Neurosciences and Clinical Neurology (Table 2, Figure 2). Neuroscientific approaches include neuroimaging to identify associations between loneliness and amyloid-β accumulation (Donovan et al., 2016). Brain-stimulation methods have also been investigated to reduce loneliness (Zheng et al., 2025), and neurotransmitter-based research has examined dopamine, oxytocin, serotonin, and related neurochemicals, including exploratory pharmaceutical approaches not yet clinically available (Cacioppo and Cacioppo, 2015; Carney, 2020; Entis, 2019; Shamai-Leshem et al., 2025). Although the present study draws exclusively on macro-level bibliometric data, even a brief consideration of several concrete examples from the research areas in which growth is observed further illustrates that loneliness is increasingly subject to pharmaceuticalization and biomedicalization (Clarke et al., 2003).
Finally, continuity refers to the possibility that phenomena may be first de-medicalized, and then re-medicalized at a later date; that is, it indicates that both medicalizing and de-medicalizing forces coexist and that medicalization is not a fixed, one-directional process (e.g. homosexuality). Loneliness appears to be a case in which medicalization is only just beginning. This study found a sharp increase in loneliness-related research, particularly in psychiatry and public health, from the late 2010s (Figure 1). This suggests that the prominent emergence of the medicalization of loneliness is a phenomenon confined approximately to the past decade.
In contrast to loneliness, some emotions have followed trajectories that look more like de-medicalization (e.g. nostalgia; Arnold-Forster, 2024). Examining how related emotions have been named and reinterpreted over time offers a useful point of comparison. On the other hand, public health has been criticized for tendencies toward medicalization (Nunes, 2025), but it is also a field with a mission that is fundamentally oriented toward social reform. The observed increase in loneliness research within public health may therefore be interpreted as reflecting a complex mixture of medicalizing and de-medicalizing forces. While public health retains a fundamental orientation toward social reform, its recent emphasis on individual health metrics and risk-factor framing may, in practice, serve as a vehicle for medicalization by situating social isolation within a clinical jurisdiction. The situation in which loneliness is simultaneously problematized as a social issue and criticized as being medicalized is therefore itself an intriguing case when viewed through the lens of medicalization theory.
The progression and drivers of the medicalization of loneliness
It is worth considering the current stage of the medicalization process of loneliness, and the forces that may be driving it forward. In the case of loneliness, the expansion of traditional medical jurisdictions alone is insufficient for a comprehensive analysis. Instead, it is useful to adopt a perspective focusing on interactive processes—specifically the reconstitution and optimization of health, bodies, and subjectivities—as proposed by Clarke et al. (2003) in their concept of “biomedicalization.” This concept encompasses five key interactive processes: (1) the political economic reconstitution of the vast sector of biomedicine; (2) the focus on health itself and the elaboration of risk and surveillance biomedicines; (3) the increasingly technological and scientific nature of biomedicine; (4) transformations in how biomedical knowledges are produced, distributed, and consumed, and in medical information management; and (5) transformations of bodies to include new properties and the production of new individual and collective technoscientific identities. This perspective is particularly relevant because loneliness currently navigates a complex space between subjective experience and quantifiable health risk, facilitated by emerging technoscientific conditions.
To further the discussion on how loneliness is being medicalized, I suggest a possible trajectory of this process as a provisional framework. Informed by the interactive process model of Clarke et al. (2003), this trajectory is intended not as a definitive empirical proof, but as a conceptual lens to interpret the academic trends identified in this study. Based on the patterns observed, the medicalization of loneliness may be viewed through the following four-phase trajectory.
First, regarding the problematization of emotion, which constitutes the pre-medicalization stage, the case of loneliness can be interpreted as having entered this phase. The sustained dominance of psychology throughout the study period (Table 1), which could be partly conceptualized as “psychologization” (De Vos, 2011), indicates a concentrated focus on the emotional dimension of loneliness. This is also consistent with the broader process of “emotionalization” (Cabanas and Illouz, 2019), where subjective states are critically noted to be repositioned as collective goals and indicators of personal worth, alongside the rise of “positive psychology” in the early 2000s. Within this landscape, loneliness has functioned as a conceptual “hook” (Alberti, 2019) for diverse social concerns, framing it as an undesirable condition, or a form of “deviance,” that necessitates individual intervention. If intertwined with neoliberal notions of self-responsibility, it risks being reduced to discourses of mindset or attitude (Fullagar and O’Brien, 2013). Medicalization may advance by transforming latent dissatisfaction, or problems that should be addressed socially, into a demand for self-regulation and by creating markets for intervention. A similar pattern is seen in the application of antidepressants for the SAD or GAD, where pharmaceutical marketing has been identified as a key driver (Conrad, 2007). Similarly, consumer desires stimulated by media representations may influence the medicalization of loneliness.
Second, the phase of framing as a health risk and recasting as a public health issue could be reflected in the marked growth of the public health literature observed since the mid-2010s (Figure 1). In this stage, loneliness is not yet defined as a disease but is constructed as a significant risk because of its negative effects on health outcomes. The 2010s acceleration aligns with the widespread dissemination of meta-analytic findings equating loneliness and related forms of social disconnection to a mortality risk (Holt-Lunstad et al., 2010), often described in public discourse as equivalent to “smoking 15 cigarettes per day.” This process has effectively made the issue visible and quantifiable, potentially allowing public health discourse to serve as an “engine” of medicalization by translating a social experience into a manageable health metric.
Third, in the phase of the pursuit of biomedical solutions, the strong influence of psychiatry and the growing presence of neuro-related research areas and topics (Figure 2) suggest that biomedicalization is already underway. Clarke et al. (2003) highlighted a shift in focus from illness to health, with an emphasis on risk and “surveillance biomedicines” as a condition of biomedicalization. This study did not examine the content of individual papers. However, the growing prevalence of technologies beyond conventional medical domains (e.g. smartphones, wearable devices, and health-monitoring apps) indicates potential for recording, self-monitoring, and intervening in loneliness as an emotional state (Jafarlou et al., 2024). There are as yet no established clinical technologies that detect loneliness using data on vital signs, but there are apps prompting users to engage in social behaviors (Bruehlman-Senecal et al., 2020). If these trends continue, domains beyond the individual, such as the quality and quantity of human relationships, may increasingly become managed and medicalized. The emerging framing of relational deficits as health risks could be seen as an extension of the general trend of inflation of the concept of risk in the medical literature (Skolbekken, 1995).
Lastly, concerning the potential emergence of diagnostic categories and legitimation of associated medical interventions, loneliness does not currently correspond to a formal diagnostic label. However, the trajectory indicated by current academic trends, along with the precedents of similar medical conditions, suggests that the possibility remains. As loneliness becomes increasingly intertwined with psychiatric frameworks, the groundwork for its eventual legitimation as a diagnostic entity, or its potential to be subsumed under an existing disorder, cannot be ruled out.
Throughout this study, medicalization has been operationally defined as “making experience medical” (van Dijk et al., 2020). However, the fundamental question remains: where does the “medical” begin and end? The very act of posing this question implies a preexisting assumption regarding the legitimate jurisdiction of medicine. If we interpret medicalization as the social expansion of the classic “sick role,” the criteria would be whether an individual is labeled as “sick” by experts and placed under medical jurisdiction. Yet, loneliness is not currently a matter for medical diagnosis; consequently, it does not involve the right to be exempted from normal social roles or the obligation to follow a physician’s orders. Furthermore, since loneliness itself is not inherently a case of high deviance (unlike some mental disorders, such as ADHD), individuals do not necessarily gain the “benefit” of exemption by being labeled as sick.
Nevertheless, the results of this study suggest that loneliness is being framed as a risk factor on the grounds of its negative impact on various health outcomes, leading to a search for biomedical causes and interventions. In other words, this suggests a situation where individuals gain no exemption as “patients,” yet the individual responsibility, which is inherent in medicalization, is increasingly emphasized. As noted in the context of preventive medicine, the shift toward earlier intervention points promotes the idea that the spread of information about avoidable risks reinforces the notion that one can be responsible for being ill (Verweij, 1999).
Loneliness may cause health risks, but it is also a consequence of a fraying society. In a context where health is defined as encompassing well-being and quality of life and not just as the absence of disease, solutions limited to neuroscience, pharmaceuticals, or technological management risk obscuring the social and structural origins of loneliness (Cabanas and Illouz, 2019). The coupling of such technological solutions with neoliberal values risks reinforcing the view that managing “health risks” like loneliness is an individual responsibility, thereby obscuring its social origins.
While medicalization theory originally carried strong implications of social critique, the theory itself must reflexively evolve as the society it critiques undergoes transformation. The examination of loneliness as a new case study will contribute to this reflexive development.
Implications for further research
This study only examined research areas and topics at a macro level and did not analyze the detailed content of individual publications. Furthermore, while bibliometric trends may indicate a potential for medicalization within academic discourse, they do not conclusively demonstrate the process of medicalization. It is therefore not possible to determine how loneliness is being framed in specific terms in each article or experienced as lived reality. Future research should incorporate discourse analysis and detailed text mining to identify how loneliness is linguistically and conceptually reconstructed within different disciplines. The dominant fields for studying and defining emotions vary across countries and regions: social psychology predominates in North America, whereas humanities disciplines play a more central role in the UK and Australia (Olson et al., 2017), and comparative analyses that consider regional variation would also be valuable.
Despite these limitations, this study provides empirical insight into the process by which loneliness is becoming medicalized. It therefore contributes to the advancement of medicalization theory, particularly regarding the medicalization of emotions. Future developments will depend on whether the emotional dimension of loneliness—an experience that is inherently complex, multifaceted, and embodied—becomes formalized as a diagnostic category, and whether any such redefinition achieves widespread acceptance.
Footnotes
Acknowledgements
Funding
The author disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by JSPS KAKENHI [Grant Number 22K01880].
Declaration of conflicting interests
The author declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.