
Abstract
Autism is increasingly seen as a social identity, as well as a clinical diagnosis. Evidence suggests that autistic adults who have stronger autism social identification have better psychological well-being. Autism is a condition which impacts on social interactions, and so one’s sense of autism identification may be particularly important for reducing social anxiety, which is common in autistic adolescents. We aimed to investigate how the subcomponents of autism identification relate to social anxiety in autistic young people. We hypothesised that autistic young people who had a higher satisfaction with their autism identity, and more solidarity with other autistic people, would have better psychological well-being and lower social anxiety. 121 autistic young people between the ages of 15–22 completed questionnaires measuring self-reported autism traits, social anxiety, psychological well-being, and different components of autism social identification. We conducted regression analyses controlling for age, gender, and autism traits. We found that higher autism satisfaction was associated with higher psychological well-being and lower social anxiety. Young people with higher autism solidarity had higher psychological well-being, but there was no significant relationship between solidarity and social anxiety. We conclude that it is important to support autistic young people to develop autism social identification.
Lay abstract
Autism is a diagnosis given to individuals by professionals but is also increasingly seen as an identity which an individual can choose for themselves. We wanted to explore how having autism as an identity affects autistic young people. There is evidence that autistic adults have better psychological well-being when they feel more solidarity with other autistic people and feel positively about being autistic. We know that autistic teenagers often feel anxious in social situations. Having a positive autism identity might help alleviate social anxiety associated with being autistic. We wanted to find out if autistic young people who felt more solidarity with other autistic people, and had more positive feelings about autism, had better psychological well-being and less social anxiety. We asked 121 autistic people aged 15–22 years to complete some questionnaires. These questionnaires asked about the young person’s autism traits, social anxiety, and psychological well-being. The questionnaires also asked how satisfied they felt to be autistic (satisfaction) and how much solidarity they felt with the autism community (solidarity). We found that autistic young people who had higher autism satisfaction had better psychological well-being and lower social anxiety. Young people who felt more solidarity with other autistic people had higher psychological well-being. There was no association between autism solidarity and social anxiety. We conclude that is important to support autistic young people to develop positive feelings about autism and to feel solidarity with other autistic people.
Keywords
Autism spectrum disorder is a diagnosis which has been defined by Psychiatrists, Psychologists and other health professionals and researchers in the Diagnostic and Statistical Manual of Mental Disorders (5th ed.; DSM-5; American Psychiatric Association, 2013). Not only is autism a diagnosis, but it is increasingly viewed as an identity which the autistic individual may see as central to their sense of self, or may distance themselves from (e. g., Botha & Frost, 2020; Cooper et al., 2021; Perry et al., 2021). This viewpoint of autism as an identity has emerged alongside increasing self-advocacy in the autistic community (e.g. Rosqvist et al., 2015) and awareness of the strengths and talents of autistic people (Kenny et al., 2016), with a cultural shift away from a medically defined and deficit-focused model of autism. This conceptualisation of autism as an identity as well as a diagnosis is exemplified by the increase in individuals who self-identify as autistic but who have not received a formal diagnosis of autism from a health professional (Lewis, 2017). While it is important to acknowledge autism as an identity and the strengths focus which can come along with this, autistic individuals also face multiple challenges, so it is important to acknowledge that an autism identity may not be solely strengths focused, with perceptions of a disability identity being prominent for many autistic people (Den Houting, 2019). Therefore, acknowledging autism as a social identity should not obscure the experiences of autistic people who perceive autism as a disability. Indeed, other researchers have proposed the importance of a social identity approach within disability studies more broadly (Dirth & Branscombe, 2018).
Autistic young people face the opportunity and challenge of making sense of their autism diagnosis and navigating their identity as an autistic person (Huws & Jones, 2008). In typical development, adolescence is considered a critical period for the development of an individual’s identity, or sense of self (Erikson, 1968). Adolescents must navigate their own personal identity, for example, their choices in relationships, education and work, and in their beliefs and values (Marcia et al., 1993). They must also navigate their social identities, as outlined by social identity theory (Tajfel & Turner, 1979). Social identity theory suggests that individuals have a drive to form social groups, to favour members of their group over others, identify with in-group members, and to derive self-worth from memberships in these groups (Rubin & Hewstone, 1998). Adolescents therefore must navigate their memberships within social groups.
Social identity theory posits that individuals can derive a sense of self-esteem and well-being from belonging to social groups (Rubin & Hewstone, 1998). However, belonging to a social group which is stigmatised may have negative implications for well-being. Autistic people experience high levels of discrimination, or autism minority stress (Botha & Frost, 2020). This discrimination presents challenges to the self-esteem and well-being of autistic young people, and autistic people are significantly more likely to experience mental health problems compared to the typically developing population (Lai et al., 2019). Moreover, social exclusion and feelings of loneliness may also contribute to high rates of mental health need in this group. Indeed, loneliness has been shown to mediate the relationship between social contact and mental health needs in young autistic adults (Schiltz et al., 2021).
Social anxiety disorder is characterised by marked distress in social situations with negative perceptions about one’s own social performance, fears of negative evaluation by others and avoidance of social interactions. Social anxiety is commonly reported by young people, with a recent international study highlighting at least 36% of young people meet criteria (Jefferies and Ungar, 2020). Autistic young people are no different in this respect, and rates of social anxiety disorder reported in the literature for this group range between 29% and 57% (e.g. Bellini, 2004; Kuusikko et al., 2008; Simonoff et al., 2008). Studies have considered potential overlap between social anxiety symptoms and core characteristics of autism at the measurement and construct level. Such studies have reported a reliable distinction between the cognitive processes associated with social anxiety such as fear of negative evaluation by others and core autism traits such as social skills difference (Lei & Russell, 2021; White et al., 2012). There is a strong association between negative self-perceptions and distressing anxiety in social situations for autistic young people. Furthermore, the double empathy problem (Milton, 2012), whereby autistic and non-autistic people struggle to understand each other’s perspectives, may accentuate the cognitive processes inherent in social anxiety for autistic people. The findings of greater success in autistic peer to peer information transfer (Crompton, Ropar, et al., 2020) and higher autistic peer to peer rapport (Crompton, Sharp, et al., 2020) provide some indirect support for this.
The cognitive behavioural model of social anxiety posits negative self-beliefs, high standards for performance and catastrophic beliefs about failure underpin the development of social anxiety in an individual (Clark and Wells, 1995). Autistic young people are often subject to peer victimisation (Weiss & Fardella, 2018) which may increase their vulnerability to these cognitive processes. Individual formulation-driven interventions within a cognitive behavioural framework are at the heart of evidence-based interventions for social anxiety, which focus on an individual’s negative self-beliefs and in situ attentional processes. However, negative beliefs about oneself as an individual may stem from one’s perception of a group social identity, and be influenced by experiences of stigma and prejudice which are internalised (Han et al., 2021). Such negative beliefs about a social identity may require consideration within treatment for social anxiety if they underpin distress and related social impairment.
Identity management strategies may be used to mitigate the negative mental health impacts of stigma and discrimination associated with being autistic (Crabtree et al., 2010). One such strategy is leaving the group, however for autistic young people this is not possible, as autism is a lifelong neurodevelopmental condition. Instead, some individuals choose not to disclose their diagnosis or attempt to hide their autism characteristics in order to be perceived by others as neurotypical (Hull et al., 2017; Macleod et al., 2013; Pearson & Rose, 2021), and indeed concealment of autism identity has been found to be related to internalised stigma associated with autism (Botha & Frost, 2020).
Another identity management strategy is to focus on the strengths of autism to derive a sense of psychological well-being (or collective self-esteem, Luhtanen & Crocker, 1992) from the autism identity (Kapp et al., 2013). Research across a range of social groups that face discrimination has demonstrated the positive role of social identification and collective self-esteem in mental health (Jetten et al., 2012). There is evidence that social identity processes may be important for autistic adults. For example,K.Cooper et al. (2017) found that there was a positive association between autism social identification and personal self-esteem and psychological well-being, which was mediated by collective self-esteem, or how positively individuals viewed their autism identity. Furthermore, self-acceptance of autism identity as well as perceived acceptance from friends and family has been shown to be linked to well-being in autistic adults (Cage et al., 2018), and autism personal identity has been found to be positively associated with psychological well-being (Corden et al., 2021). There is also qualitative evidence that autistic people experience benefits and increased feelings of connectedness when communicating with other autistic people (Crompton, Sharp, et al., 2020; Milton & Sims, 2016). These findings are at odds with research demonstrating that social identity processes may be less salient in autistic people compared to the typically developing population (Skorich et al., 2016, 2017). The most plausible explanation for these divergent findings is that while autistic people may often be less inclined to self-categorise as belonging to certain groups and to form themselves into social groups, these processes do still occur in autistic people. Moreover, there is evidence that these processes can have a positive effect on well-being, but perhaps require more scaffolding and support than in the general population.
Social identification is often divided into a number of components (Leach et al., 2008), some of which may impact on mental health more than others, depending on the particular identity and mental health problem being investigated. The above research findings indicate that there may be a particular role of autism solidarity and collective self-esteem (autism satisfaction) in contributing to better mental health in autistic individuals. The other components of social identification have not been shown to be individually associated with mental health in autistic people, and so we do not make specific hypotheses about these. Autism social identification may have a particular role in social anxiety, as well as psychological well-being more broadly, because it is a condition characterised by a focus on the self as a social object. An individual’s perception of their autism identity could well contribute positively or negatively to their evaluation of their own social performance, their perception of their autism traits and any associated psychological distress, such as anxiety in social situations. These processes may be particularly important during adolescence, given that this is a time of identity formation (Erikson, 1968), in the face of high levels of victimisation and high rates of social anxiety for autistic young people.
In this study, we aimed to investigate the cross-sectional relationships between positive feelings about one’s autism identity (autism satisfaction) and feeling more solidarity with other autistic people (autism solidarity), with social anxiety and psychological well-being, when controlling for age, gender, and self-reported autism traits in autistic young people. We hypothesized the following:
Autism solidarity will be associated with lower social anxiety.
Autism satisfaction will be associated with lower social anxiety.
Autism solidarity will be associated with higher psychological well-being.
Autism satisfaction will be associated with higher psychological well-being.
Method
Participants
Participants (n = 121) were young people between the ages of 15 and 22 years with a clinical diagnosis of an autism spectrum disorder. All participants had a diagnosis of autism from a healthcare professional which they shared with the research team. Participants were invited to take part in this research when invited to attend a summer school based in a UK university. The summer school was aimed at students aged 16 years and above who were completing compulsory education and who were considering attending higher education at a university, with the aim of improving success and well-being at University for autistic students. Taking part in the research was not a mandatory part of summer school attendance. Some individuals who completed measures later decided against attending, and two young people who attended the summer school opted to not complete the questionnaires. Of those who completed measures, there were two participants with some incomplete data.
The average age of participants was 17.6 years (SD = 1.10). Participants reported their gender and 36 (30%) of the young people were female, 82 (68%) were male and 3 (3%) had another gender identity. Participants reported their ethnicity, and 109 (90%) participants were Caucasian, 4 (3%) were mixed race, 4 (3%) were Asian, 1 (1%) was African and 1 (1%) was Caribbean, with two participants not disclosing their ethnicity.
Ethics
Ethical approval was gained for this study from the Department of Psychology Ethics Committee. Participants and their parents or carers were provided with information sheets about the study and given the opportunity to ask questions about these. Participants and their parents then gave fully informed consent by signing a consent form. Participants were aware of their right to withdraw and to not complete the questionnaires.
Procedure
Participants were attendees at a university autism summer school between 2016 and 2019. Attendees were able to refer themselves to attend the summer school by contacting the summer school organisers, and places were allocated to all eligible young people until capacity was reached. Young people and their parents signed consent forms to complete questionnaires to be used for research purposes, as well as to tailor the summer school to individual students’ needs. Before attending the summer school, while at home, young people were invited to complete a set of questionnaires. These were completed either on paper or online through a Qualtrics online survey. Participants completed a number of measures for other studies alongside the measures included in this article (see Lei et al., 2020). Participants were shown a debrief form after completing these questionnaires. Students were also asked to complete further questionnaires during and after the summer school, but these questionnaires are not included in this study.
Measures
Self-report autism traits
Autistic traits were measured using the social responsiveness scale – short, a self-report measure of autistic traits including differences in social communication and interaction and restricted, repetitive behaviours (SRS-S; Constantino & Gruber, 2005; Kanne et al., 2009). This eleven-item scale measures the individual’s perceived social difficulties and adherence to routines and specific interests, with items such as ‘I avoid eye contact with other people’. Items are scored on a Likert-type scale from 0 ‘not true’ to 3 ‘almost always true’. This scale had good internal consistency (α = 0.80).
Autism identification
Autism identification was measured using a multidimensional scale of social identification developed by Leach et al. (2008), adapted for autistic people ( K.Cooper et al., 2017). This 14-item scale (α = 0.84) has good reliability and construct validity. Items were scored from 1 ‘Strongly disagree’ to 7 ‘Strongly agree’. Component scores are summed and then divided by the number of items, so the score for each subscale ranges between 1 (low autism identification) to 7 (high autism identification). The scale has two dimensions, the first being self-investment, which has three components. The first component is solidarity (α = 0.88), which refers to the extent to someone feels a connection to other autistic people, and has three items, one being ‘I feel a social bond with autistic people’. 1 The second component is satisfaction (α = 0.86), which refers to how positively the individual feels about their autism identity. It has four items, an example being ‘I am glad to be autistic’. The third component is centrality (α = 0.79), which is about the importance the individual places on their autism identity. This component is made up of three items, for example, ‘Being autistic is an important part of how I see myself’.
The second dimension of the autism identification scale is self-definition, which has two components. The first is individual self-stereotyping (α = 0.86), which measures how similar the individual feels to other autistic people, and has two items, for example, ‘I have a lot in common with the average autistic person’. The second component is in-group homogeneity (α = 0.81), which measures whether the individuals thinks that autistic people are similar to one another using two items, for example, ‘Autistic people have a lot in common with each other’.
Social anxiety
We used the social anxiety scale for adolescents (La Greca & Lopez, 1998), a 22-item measure of social anxiety in young people which has three subscales made up of 18 items. The three subscales are fear of negative evaluation; social avoidance and distress in new situations; social avoidance and distress in general. The scale had good internal consistency (α = 0.90). Items include ‘I get nervous when I meet new people’. Items are scored on a Likert-type scale from 1 ‘not at all’ to 5 ‘all the time’, with higher scores indicating higher levels of social anxiety.
Psychological well-being
We used the Warwick-Edinburgh Mental Well-being Scale (WEMWEBS; Tennant et al., 2007) to measure psychological well-being in this group. This 14-item scale has not been validated for use with autistic people but had good internal reliability in this study (α = 0.86). Items include ‘I’ve been feeling confident’. Items are scored on a Likert-type scale from 1 ‘none of the time’ to 5 ‘all the time’.
Community involvement statement
The research question and methods were developed by non-autistic researchers and clinicians who work with autistic young people and adults. Data collection ran over several years, and we removed one measure (of collective self-esteem) following feedback from previous autistic participants.
Analytic strategy
To test the hypotheses 1 and 2, that feeling more solidarity with other autistic people (solidarity) and having a more positive feelings about one’s autism identity (satisfaction) would be negatively related to social anxiety, we ran a regression analysis with social anxiety as the dependent variable. To test hypotheses 3 and 4, that autism solidarity and autism satisfaction would be positively associated with psychological well-being, we ran a second regression analysis with psychological well-being as the dependent variable. To determine which variables we should control for, we conducted initial descriptive analyses and partial correlations between the study variables, finding that both autism traits and gender were significantly associated with key study variables. Moreover, previous research has indicated an influence of age on autism social identification ( R.Cooper et al., 2021), so age was also entered as a control variable. For both regression analyses, in step 1 we entered the control variables age, gender and autism traits. In step 2, we added each subcomponent of the autism identification measure: autism solidarity; satisfaction; centrality; self-stereotyping; and in-group homogeneity. We analysed the data using IBM SPSS Statistics 26 and ran initial checks to ensure that the assumptions of hierarchical regression analysis were met. 2
Results
In our preliminary analysis, we looked at the correlations between all key study variables and autism traits, controlling for age and gender (see Table 1). Participants who reported that they had more autism traits had poorer psychological well-being r(115) = –0.43, p < 0.001 and higher social anxiety r(115) = 0.57, p < 0.001, and so we controlled for autism traits in the regression analyses. Those who reported more autism traits also reported that their autism identity was more central r(115) = 0.34, p < 0.001 and felt more solidarity with other autistic people r(115) = 0.26, p = 0.005. There were no significant relationships between self-reported autism traits and autism satisfaction, autism self-stereotyping, or autism homogeneity.
Descriptive statistics and partial correlations controlling for age and gender (N = 121).
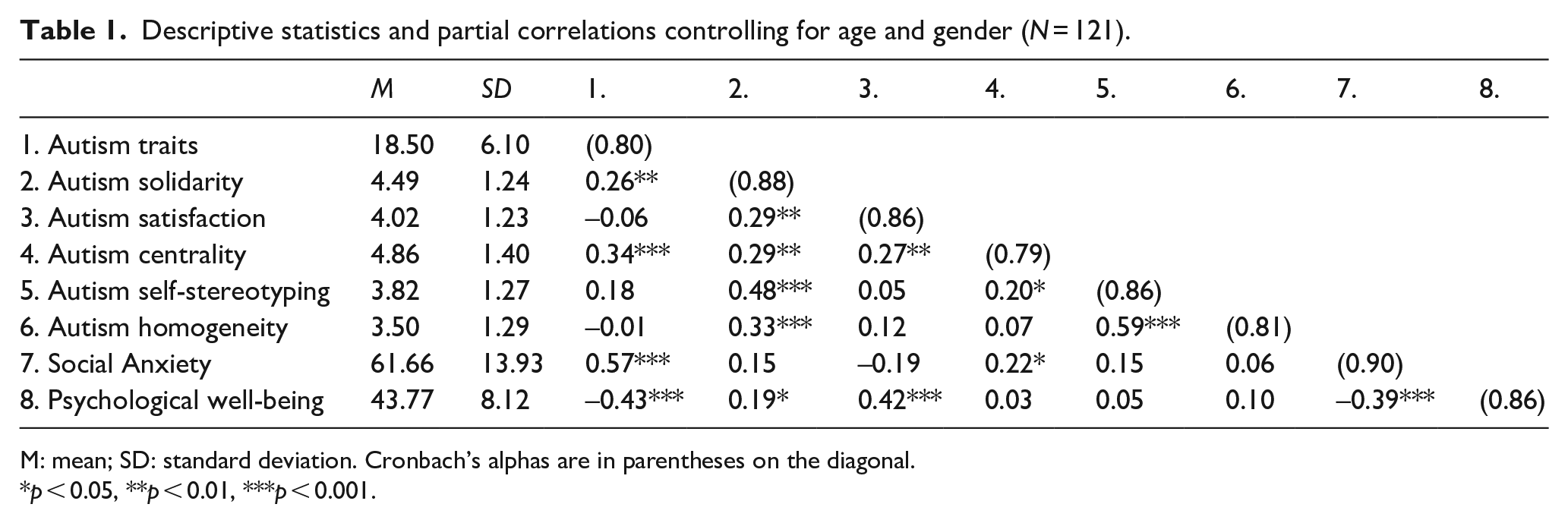
M: mean; SD: standard deviation. Cronbach’s alphas are in parentheses on the diagonal.
*p < 0.05, **p < 0.01, ***p < 0.001.
We found support for our hypothesis that autism satisfaction would be associated with lower social anxiety, but did not find support that autism solidarity would be associated with social anxiety. In the first regression analysis predicting social anxiety, step 1 was significant F(3, 115) = 18.62, p < 0.001, R2 = 0.33. In step 1, higher self-reported autism traits were associated with higher social anxiety β = 0.57, p < 0.001. Step 2 was also significant F(8, 110) = 7.87, p < 0.001, R2 = 0.36, R2ch. = 0.04, Fch. (5, 110) = 1.28, p = 0.28. In step 2, alongside autism traits, only autism satisfaction was a significant predictor, with higher autism satisfaction associated with lower social anxiety β = –0.20, p = 0.023. Autism solidarity was not a significant predictor of social anxiety.
We found full support for our hypotheses that autism solidarity and autism satisfaction would be positively associated with higher psychological well-being. In the second regression analysis predicting psychological well-being, step 1 was significant F(3, 116) = 8.96, p < 0.001, R2 = 0.19. Higher autism traits were associated with lower psychological well-being β = –0.44, p < 0.001. Step 2 was also significant F(8, 111) = 8.53, p < 0.001, R2 = 0.38, R2ch = 0.19, Fch.(5, 111) = 6.90, p < 0.001. Autism solidarity was a significant predictor, with higher autism solidarity associated with higher psychological well-being β = 0.21, p = 0.031. Autism satisfaction was also a significant predictor, with higher autism satisfaction associated with higher psychological well-being β = 0.33, p < 0.001 (Table 2).
Regression analysis predicting total social anxiety score and well-being score.
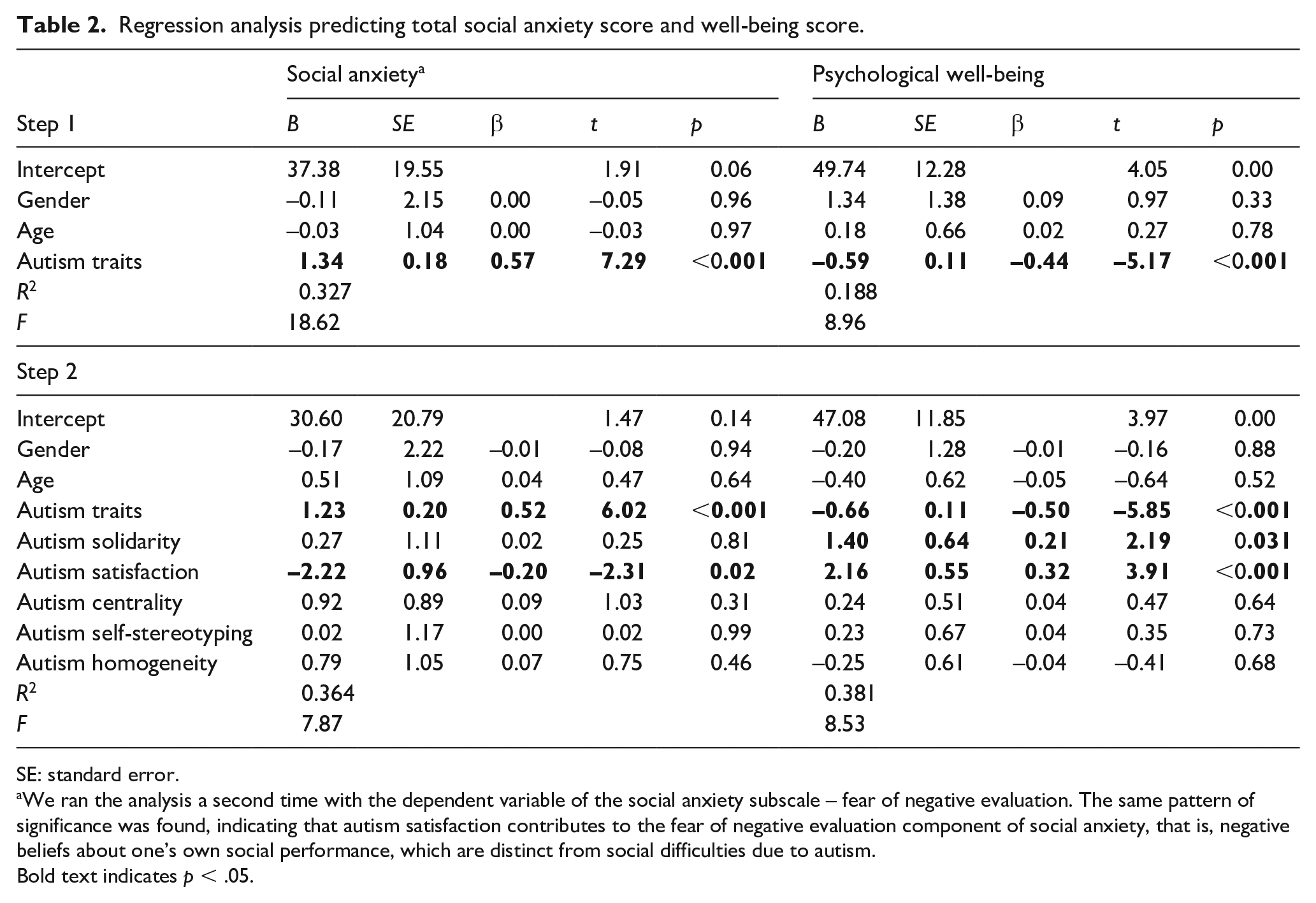
SE: standard error.
We ran the analysis a second time with the dependent variable of the social anxiety subscale – fear of negative evaluation. The same pattern of significance was found, indicating that autism satisfaction contributes to the fear of negative evaluation component of social anxiety, that is, negative beliefs about one’s own social performance, which are distinct from social difficulties due to autism.
Bold text indicates p < .05.
Discussion
Summary of findings
In this research, we tested the hypothesis that autistic young people who had a positive sense of their autism identity and felt solidarity with other autistic people would have better psychological well-being and lower social anxiety. In line with our hypotheses, we found that higher autism satisfaction predicted higher psychological well-being and lower social anxiety. Higher autism solidarity predicted better psychological well-being but was not a predictor of social anxiety. It should be noted that social identity variables did not significantly improve the model predicting social anxiety, with autism traits the most significant predictor. This suggests that social identity processes are relevant in autistic young people as well as adults, in that positive feelings about one’s autism identity and autism solidarity are particularly related to better psychological well-being.
Autism satisfaction and mental health
Our results support previous findings in autistic adults that collective self-esteem (having positive associations with one’s autism social identity) is associated with better mental health (K.Cooper et al., 2017; R.Cooper et al., 2021), and other findings that autism acceptance is associated with better mental health (Cage et al., 2018). This fits with the wider social identity research which finds that social identification and collective self-esteem are associated with improved psychological well-being (Jetten et al., 2012). This is an important finding because autistic young people often experience bullying and victimisation (Weiss & Fardella, 2018), which is more likely for autistic young people with higher autism traits (Zablotsky et al., 2014). It is therefore plausible that children and young people on the spectrum would internalise negative beliefs about autism and feel that they have to adapt to fit into school environments (Williams et al., 2019). Moreover, developing a sense of pride in their autism identity may be more challenging in youth than for adults who may be in environments where they are less likely to face daily harassment and stigmatisation. Our research indicates that having a positive sense of one’s autism identity in adolescence and young adulthood is still associated with better mental health, despite the additional challenges that autistic young people face in making sense of their identities. Due to the cross-sectional nature of our study, it is not possible to ascertain the direction of these relationships, and indeed they may be reciprocal, with young people with higher levels of psychological well-being able to identify more positives about their autism identity, and this positive sense of self contributing to better mental health. The direction of these relationships should be investigated in future research. It is also worth noting that there were much stronger and more consistent associations with autism satisfaction and psychological well-being than with social anxiety (due to differences in findings between the correlation and regression analysis). It is likely that the relationships between autism traits, autism identification and social anxiety are more complex than with well-being due to the interrelations between social difficulties, fear of negative evaluation and feelings about one’s autism identity, a condition which has a pervasive impact on one’s social experiences.
Autism solidarity and mental health
Autism solidarity was related to psychological well-being, but not to social anxiety. This aligns with previous qualitative findings that feelings of connection to the autistic community are associated with well-being (Crompton, Hallett, et al., 2020), and with wider social identity research indicating that social connections are supportive of psychological and physical health (Jetten et al., 2012). However, it seems that different processes are involved in social anxiety, as autism solidarity was not related to social anxiety. It is notable that those who rated themselves as having more autism traits on the SRS-S, also rated themselves as having higher solidarity with the autistic community. The SRS-S autism traits measure, like all self-report measures, might be better conceptualised as a measure of the individual’s beliefs about the extent of their autism-related differences rather than an objective measure of autism traits. Individuals who rated themselves as having more autism traits may have felt more solidarity with the autistic community, but this feeling of connection with the autistic community may not alleviate fear of negative evaluation from non-autistic young people. Indeed, it was notable that the autism social identification components predicted more of the variance in psychological well-being than in social anxiety. Therefore, autism social identification may be more impactful on well-being than on social anxiety, and this speaks to the complex relationships between the autism diagnostic traits, sense of self and social anxiety.
Autism centrality and social anxiety
Interestingly, in the initial correlation analysis, participants who saw autism as more central to their identities also had higher social anxiety and rated themselves as having higher autism traits. These relationships may be reciprocal, that is, having fear of negative evaluation in social situations may make one more focused on the social challenges that come with autism, which may make autism a more central part of their identity. It is also possible that there is construct overlap in that the centrality component of the autism identification measure and the autism traits measure, with both scales picking up the extent to which an individual feels their autism impacts them. These findings provide preliminary data suggesting that young people who distance themselves from their autism identity (e.g. Macleod et al., 2013) may be less likely to experience social anxiety, although this may come at the expense of developing a positive sense of autism identity. For some autistic people, their features of autism could impact on their ability to distance themselves from their autism identity. For example, individuals with more significant social communication difficulties may struggle to ‘pass’ as non-autistic due to their social differences being evident to others. Moreover, identity management strategies may have different impacts on psychological well-being and social anxiety, due to the complexity of social anxiety in individuals with an identity that contributes to difficulties navigating the social world. Future research should carefully measure fear of negative evaluation from autistic people and the non-autistic population, in order to unpack the complex relationships between self-perceived autism traits, the components of autism social identification, and social anxiety. Furthermore, longitudinal studies will be important to disentangle the causal directions between these factors, which will be important in the development of interventions to support well-being in autistic young people.
Clinical implications and conclusion
Promoting a balanced sense of autism identity, including positive elements as well as acknowledging challenges, will be supportive of well-being in autistic young people. Clinicians providing autism diagnosis should be aware of the language that they use when providing a diagnosis (Brown et al., 2021) and provide an account of the profile of strengths, as well as challenges, that come with being autistic. Post-diagnostic support which helps young people to make sense of their autism diagnosis, and ways to harness their strengths and adapt to challenges will help ensure that autistic young people have the knowledge and tools to navigate their identities into adulthood (Crane et al., 2021; Gordon et al., 2015). A systematic review and meta-analysis of social-identity building interventions in a wide range of participant groups found that such interventions had positive impacts on quality of life, physical health and psychological well-being (Steffens et al., 2021). Online settings may also provide a space for autistic young people to come together and develop a sense of community and positive autism identity (Brownlow & O’Dell, 2006). Social prescribing, and particularly social support from other autistic people, may have promise in improving psychological well-being and reducing social anxiety in autistic young people, particularly when individualised (Charlton et al., 2021; Pavlopoulou, 2021). Moreover, stigma reduction interventions in educational settings for non-autistic adolescents and young adults may help in reducing stigma associated with the features of autism and increasing acceptance of difference in young people. Furthermore, wider public awareness of the neurodiversity movement and more connections with and awareness of autistic individuals in the wider community are likely to reduce stigma across the board (Brosnan & Mills, 2016; Cremin et al., 2021), rather than placing the onus on autistic people to develop a sense of autism satisfaction in the face of discrimination from wider society.
Our findings shed light on how autism social identity processes might have a different relationship to social anxiety specifically, as compared to broader psychological well-being. Social anxiety interventions for autistic young people should pay attention to how autistic people think about social interactions with autistic versus non-autistic young people, and consider others’ neurodevelopmental conditions in behavioural experiments, where relevant to the formulation.
In conclusion, our research indicates that having autism satisfaction is associated with better mental health in autistic young adults. Complicated relationships between self-perceived autism traits, autism social identification components, and social anxiety, warrant future research and consideration in clinical work with this population.
Footnotes
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: K.C. was funded by a National Institute for Health Research (NIHR) Clinical Doctoral Research Fellowship for this research project (ICA-CDRF-2018-04-ST2-047).