
Abstract
There has been a growing focus on the importance of understanding strengths in children with neurodevelopmental conditions and how such knowledge can support clinical practices. However, limited research has explored systematic reports of strengths from caregivers of children with neurodevelopmental conditions, most commonly autism. In this study, we explored caregiver-identified strengths in children attending their first neurodevelopmental assessment. Caregivers of 686 children attending a tertiary assessment service answered a survey question about their children’s strengths. Content analysis identified 61 unique categories of strengths, which were grouped into six themes: cognitive and intellectual, social and interpersonal, hobbies and passions, character and personality, physical, and behavioural. The most frequently reported specific strengths were kind caring, and compassionate, social and friendly, loving and affectionate, music singing and dancing, and good memory recall. The breadth of positive strengths identified here may reflect the larger population sampled or the diversity of presentations in this cohort. We then present a caregiver checklist, the Child Autism and Neurodevelopment Strengths (CANS) Checklist, that was developed with community representatives, to inform assessment and feedback of child strengths. We discuss what is required to use this knowledge to inform strengths-based practices that can support clinical practice and inform on child development and family well-being.
Lay Abstract
There has been a growing focus on the importance of understanding strengths in children with neurodevelopmental conditions, but there is little research exploring caregiver-reported strengths at the time of diagnostic assessment. In this study, we explored caregiver-identified strengths in 686 children who were attending a neurodevelopmental assessment. Content analysis identified 61 unique categories of strengths, which we grouped into six main themes. These six themes were cognitive and intellectual, social and interpersonal, hobbies and passions, character and personality, physical, and behavioural. The most common strengths identified by caregivers were ‘kind, caring, and compassionate’, ‘social and friendly’, ‘loving and affectionate’, ‘music, singing, and dancing’, and ‘good memory recall’. Based on these strengths, we present a checklist that was developed with community representatives, to make sure a strengths-based framework can be used during the diagnostic process. We discuss how we can use this knowledge to develop strengths-based practices that can support clinical practice and inform on child development and family well-being.
Approximately one in 10 Australian children are diagnosed with a neurodevelopmental condition (NDC), including attention-deficit/hyperactivity disorder, autism spectrum disorder (hereafter, autism), intellectual developmental disorder, specific learning disorders, and tic disorders (Arabiat et al., 2018; Boulton et al., 2021; Thapar & Rutter, 2015). NDCs have been characterised by lifelong difficulties in social, communication, motor, and behavioural skills, across multiple contexts (American Psychiatric Association (APA), 2022). Many studies focus on identifying areas of need including poorer outcomes in interpersonal communication (Kanfiszer et al., 2017); cognitive and executive function (Carter et al., 2015; Climie & Mastoras, 2015; Demetriou et al., 2018; Kuriyan et al., 2013; Taneja-Johansson, 2021), processing speed and reasoning (Velikonja et al., 2019); daily living skills (Kanne et al., 2011); and mental health, including anxiety, depression, and sleep disorders (Boulton, Guastella, et al., 2023; Brookman-Frazee et al., 2018; Burnham Riosa et al., 2017; Cohen et al., 2014; Hollocks et al., 2019).
While it is important to identify needs and concerns so that appropriate supports can be put in place, there is growing recognition that a strengths-based approach may also have an important role in clinical care. Past research shows that caregivers of children on the autism spectrum report that deficit-focused diagnostic narratives leave them feeling discouraged, and unsure of how to access interventions and support (Crane et al., 2018; Lebeer et al., 2012; Potter, 2017; Sabapathy et al., 2017). As a result, recent diagnostic and assessment guidelines for neurodevelopmental conditions have emphasised the need to integrate strengths-based approaches to clinical assessments and diagnostic narratives (Boulton, Hodge, Levu, et al., 2023; Braun et al., 2017; Dinishak, 2016; Fitzpatrick et al., 2024; Munro et al., 2023; Rutherford et al., 2021; Whitehouse et al., 2018).
The importance and value of taking a strengths-based approach to assessment for NDCs, which identifies character strengths and abilities, and how these support better long-term outcomes across domains, is well recognised (Climie & Mastoras, 2015; McCrimmon & Montgomery, 2014; Niemiec et al., 2017; Seligman & Csikszentmihalyi, 2000). Recognising and celebrating strengths can enhance well-being, quality of life, and positive self-image for people with NDCs, by increasing self-efficacy, self-determination, and hope (Bal et al., 2022; Burnham Riosa et al., 2017; Climie & Mastoras, 2015; Niemiec et al., 2017; Wehmeyer & Shogren, 2014). This was highlighted by recent research which found that people on the autism spectrum who reported using their strengths often had better quality of life, well-being and mental health than those who reported using their strengths less frequently (Taylor et al., 2023). For children and young people with NDCs, including autism and ADHD, a strengths-based approach to the diagnostic narrative is also associated with higher caregiver, teacher, and clinician satisfaction, hope, and optimism (Abbott et al., 2013; Climie & Mastoras, 2015; Hennel et al., 2016; Lebeer et al., 2012; Mulligan et al., 2012; Nickerson & Fishman, 2013). Furthermore, when children with emotional or behavioural challenges are assessed using strengths-based measures by a strengths-focused practitioner, they are more likely to experience positive functioning outcomes and fewer missed appointments (Cox, 2006). Despite this, in a recent study, we evaluated written reports provided to caregivers following an autism assessment in a diagnostic assessment service and found that only 9.4% included activity and character-related strengths (Munro et al., 2023). This may be partially attributed to a lack of clinical guidance and structure about how strengths can be integrated into the clinical reporting process, as well as to a deficit-focused funding system, whereby increased funding supports may be provided when clinical reports emphasise deficits.
There are many advantages to identifying and building on strengths in children with NDCs that stand to benefit children and caregivers alike. For instance, while the challenges of caring for a child with an NDC have been reported, many caregivers also report positive experiences of caring for a child with an NDC. These include caregiver benefits, such as personal growth and greater appreciation for their child (García-López et al., 2016; Meleady et al., 2020; Potter, 2016); family benefits, such as strengthening spousal bonds (DePape & Lindsay, 2015; Ekas et al., 2015; Schlebusch & Dada, 2018); and societal benefits, such as increasing community awareness of diversity and different capabilities (DePape & Lindsay, 2015; King et al., 2012). Increased focus on positive parenting experiences could reduce caregivers’ levels of stress, anxiety, and depression (Ekas et al., 2016; García-López et al., 2016; Kayfitz et al., 2010; Lovell et al., 2016; Manning et al., 2011) as well as increase positive affect (Lickenbrock et al., 2011; McGrew & Keyes, 2014).
A handful of studies have explored the strengths caregivers identify in children and adolescents with NDCs, most commonly autism (Carter et al., 2015; Colavita et al., 2014; Cost et al., 2021; Potter, 2016; Sabapathy et al., 2017; Warren et al., 2021). Caregivers may identify numerous strengths in children with NDCs, including interpersonal abilities, such as social skills (Carter et al., 2015; Carter et al., 2014; Potter, 2016); personality traits, such as honesty and humour (Cost et al., 2021); intellectual abilities, such as abstract thinking and memory (Sabapathy et al., 2017; Warren et al., 2021); and hobbies and skills (Carter et al., 2015; Colavita et al., 2014) Caregivers may also report strengths within the caregiver-child relationship, including affection, emotional bonds, and shared interests (Potter, 2016). Similar traits have likewise been acknowledged in young adults with autism and/or intellectual developmental disorder by their siblings (Carter et al., 2020). To date however, research has largely not moved beyond identification of strengths, meaning that there are a lack of frameworks guiding how caregiver-identified strengths can be integrated into the assessment process to inform feedback sessions and personalise intervention and support strategies following an assessment and diagnosis.
Of the existing studies, only two to date have considered caregiver-identified strengths in younger children following an autism diagnosis. Extracting information from clinical notes, Sabapathy et al. (2017) found 98 US-based caregivers reported an average of 4.25 strengths in their children with autism, including academic and recreational skills, a good memory, intelligence, and being loving and affectionate. Reviewing responses to an open-ended question from 153 Canadian caregivers of children with autism across three time-points, Cost et al. (2021) reported that caregivers listed their preschool children’s top four strengths as love, happiness, kindness, and humour. However, no research to date has investigated caregiver-identified strengths in children with neurodevelopmental concerns at the time of their first diagnostic assessment. This means that clinicians may not be able to provide recommendations and feedback within a strengths-based framework. Identifying strengths in children with NDCs at the time of first assessment would facilitate a strengths-based approach to assessment, feedback and intervention planning, and would enable clinicians to tailor recommendations for interventions and supports in the context of the child’s strengths. The aim of this study was to understand caregiver-identified strengths for children attending a child neurodevelopment assessment service, with the most frequent assessment being for autism. We then present the Child Autism and Neurodevelopment Strengths (CANS) checklist based on these caregiver-identified strengths, which may have utility in clinical services for use in the assessment process. This evaluation and checklist be used to contribute to an integrated strengths-based approach for the diagnostic narrative that meets caregivers’, clinicians’, and children’s needs.
Methods
Participants and setting
Participants were caregivers of 686 children who attended the Child Development Unit (CDU) at The Children’s Hospital Sydney, Australia, between 2020 and 2022. Participants consented to the Sydney Child Neurodevelopment Research Registry (Boulton, Hodge, Jewell, et al., 2023), a partnership with the Clinic for Autism and Neurodevelopmental Research at the University of Sydney. The study was approved by the Sydney Children’s Hospital Network Human Research Ethics Committee (reference: LNR/17/SCHN/293).
The CDU is part of the publicly funded Sydney Children’s Hospital Network, which provides tertiary level developmental and diagnostic assessment services to children aged 0–16 years of age with complex developmental conditions. The average age at diagnostic assessment for children attending this service is 6.56 years (Boulton, Hodge, Jewell, et al., 2023). Children who are referred by a paediatrician, and who live within defined geographical regions or have ongoing complex medical needs cared for at the hospital, are eligible for assessment. Given these criteria, a large proportion of referrals are children from vulnerable backgrounds (low socioeconomic status, culturally and linguistically diverse). Children are referred for assessment of neurodevelopmental difficulties including autism, developmental disorder, global developmental delay, speech/language delays and other difficulties with adaptive and/or cognitive functioning. On average, about 70% of children receive an autism related diagnosis and over 50% receive more than one diagnosis. To provide an accurate representation of the service, we have reported data for all presenting children. We also note that diagnostic and assessment services such as this service are often the only option within the public health assessment system for autism diagnoses in Australia, which is reflected by most presenting children receiving an autism diagnosis. All families participated in this study using opt-out consent procedures. Families were provided with information about the registry study at the time of assessment and were provided with the opportunity to opt-out of their data being used in the research registry. In total, 21 families (3% of the cohort) opted out.
Measures
The Parent Carer Questionnaire (PCQ) is a six-page questionnaire, developed by the CDU to collect clinically relevant information on children and families before their appointment. Completed by the primary caregiver of the child being assessed, it collects information on demographics, family history, and child developmental history. For this study, responses to the question in the PCQ ‘What do you think are your child’s strongest points (what does he or she do best)?’ were extracted, as well as sociodemographic characteristics for children (age at assessment, gender) and caregivers (level of education, culturally and linguistically diverse status). Specific data pertaining to socioeconomic status was not reported.
Procedure
Approximately 1 month prior to their assessment at the CDU, caregivers were sent the PCQ. Questionnaires were sent electronically via the Research Enterprise Data Capture platform, an online data collection system endorsed by the University of Sydney (Harris et al., 2019; Harris et al., 2009). Families received an email reminder to complete the protocol 1 week prior to their appointment, and those who did not do so before their appointment completed it on the day of assessment as per the process described elsewhere (Patel et al., 2021).
Data analysis
Qualitative content analysis
This study used qualitative methods to identify categories and themes from caregiver-identified strengths. Responses to the question in the PCQ ‘What do you think are your child’s strongest points (what does he or she do best)?’ were uploaded into NVivo-12 (QSR International Pty Ltd, 2020). Responses varied from a few words to several sentences. All responses were coded, except for two words that were ambiguous and could not be clarified.
An independent data analysis process was undertaken from the open text responses to the question ‘What do you think are your child’s strongest points (what does he or she do best)?’, using qualitative content analysis, as informed by Kleinheksel et al. (2020) and Vaismoradi et al. (2016). A combined inductive and deductive approach was used to analyse the content of responses and ensure identified categories, and their overarching themes, were meaningful to the research questions. The process was as follows: one author (L.H) familiarised themselves with the content prior to analysis, noting initial trends. Next, NVivo was used to capture and derive an initial set of codes from the responses. These codes were aggregated in NVivo, after which categories of strengths were identified and refined based on these codes. Categories were reviewed extensively for similarity and duplication of meaning, and multiple categories were collapsed and merged as appropriate. Themes were then generated based on a synthesis of these categories. Finally, themes were reviewed and determined valid if their content was meaningfully cohesive and captured distinct parts of the overall data set. They were then named to be concise, informative, and memorable. A codebook containing definition for themes and categories, along with exemplar responses, is provided in Supplementary Information. One researcher examined this study’s data set in its entirety. A second researcher independently reviewed 20% of the coded responses, categories and themes to explore interpretations and reach consensus among themes.
We also examined whether children who went on to receive a diagnosis of autism showed differences in caregiver-identified strengths compared to children who did not receive a diagnosis of autism. To do so, chi-square tests were used to compare the frequency of themes between children who received an autism diagnosis and children who did not receive an autism diagnosis.
Development and modification of the Child Autism and Neurodevelopment Strengths (CANS) Checklist
Following content analysis and identification of categories and themes, we collated the categories and themes into a checklist, the CANS Checklist. Our goal was to develop a checklist that could be completed by caregivers at the time of diagnostic assessment and reviewed by clinicians as part of the diagnostic assessment and observation. The checklist can then be used to inform the clinical feedback session, with clinicians personalising recommendations and intervention strategies based on the caregiver-identified strengths noted in the checklist. This would provide a framework for how caregiver-identified strengths can be integrated into the assessment process. We consulted community representatives and clinicians to seek feedback on this checklist, namely, its structure, proposed items, and the way it could be integrated within clinical assessments. A group of 12 community representatives and clinicians were involved in feedback and consultation. Feedback was received via email and through group discussions. There were multiple opportunities for discussion and feedback from community representatives and clinicians. Discussions continued until consensus was reached. The checklist was modified following these consultation and feedback sessions with key stakeholders.
Community involvement
The Brain and Mind Centre Neurodevelopment Community Research Advisory Committee were involved in overseeing and providing feedback on this study. This committee consists of people with neurodevelopmental conditions and their caregivers. Members of the Research Advisory Committee provide suggestions and feedback throughout the research process, from conceptualisation through to dissemination, and are reimbursed for their time and expertise. As described above, community representatives and clinicians provided feedback on the CANS Checklist as part of this study.
Results
Demographics
Demographics for 686 children and their caregivers are presented in Table 1. Children were 6.5 years old on average (SD = 3.56; range = 1.17–17.58 years) at the time of assessment. Most children were male, and more than half had at least one caregiver with a culturally and linguistically diverse background. In total, 70% of children (n = 445) received an autism diagnosis following assessment.
Participant demographics.

Cultural and linguistic diversity was indicated when at least one caregiver had a culturally and linguistically diverse background. Cultural background data was missing for 6 caregivers. Education level data was missing for 11 mothers and 44 fathers. Diagnosis data was unavailable for 54 children. Information on caregiver who completed the questionnaires was missing for 24 respondents. ‘Other’ caregiver respondents included foster carer or case worker (n = 10) or another family member (n = 10).
Caregiver-identified strengths
Caregiver-identified strengths were coded into six themes: cognitive and intellectual, social and interpersonal, hobbies and passions, character and personality, physical, and behavioural. Each theme had between 6 and 12 categories, resulting in a total of 61 identified categories of strengths. On average, caregivers identified 2.8 strengths in their child (SD = 2.02, range = 0–18). Figure 1 displays the categories and themes identified following our content analysis.
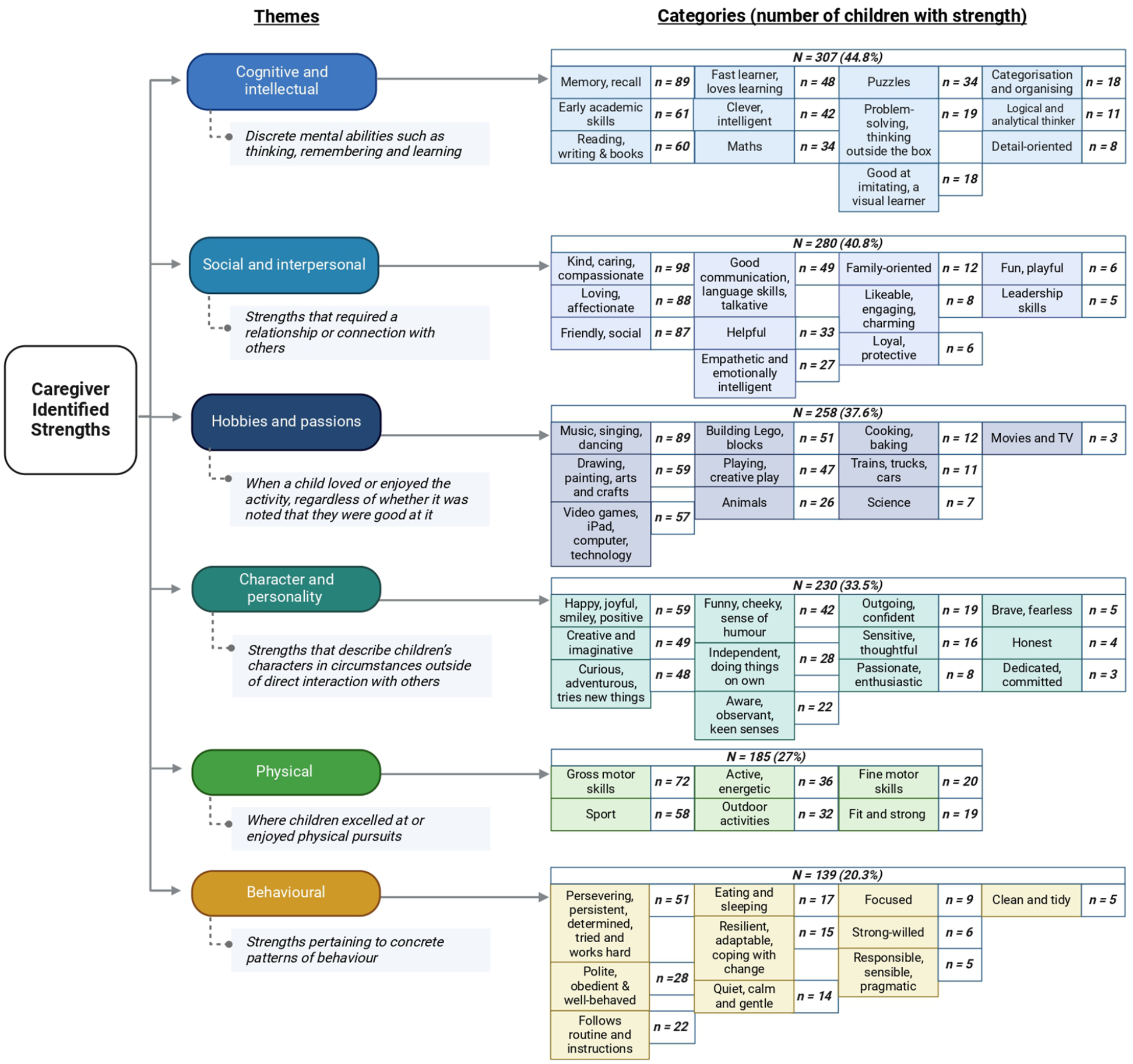
Themes and categories identified in qualitative analysis.
Cognitive and intellectual strengths
The most frequently identified theme covered ‘Cognitive and intellectual’ strengths, which include discrete mental abilities such as thinking, remembering, and learning. In total, 12 categories were identified in the cognitive and intellectual theme, which were identified 433 times in 307 children (44.8% of the total children in the study). The most-identified cognitive and intellectual strengths were ‘memory, recall’ (identified 89 times across 89 children), ‘Early academic skills’ (identified 85 times across 61 children), and ‘Reading, writing and books’ (identified 67 times across 60 children). Some caregivers described their child’s memory as ‘amazing’, ‘incredible’, ‘exceptional’, and ‘photographic’. Other categories included being a ‘fast learner’ (identified 48 times across 48 children), ‘clever’ or ‘smart’ (identified 42 times across 42 children), or good at maths (identified 34 times across 34 children). Some caregivers highlighted their child’s broad-reaching cognitive abilities, for example they are ‘Very academically focussed and gifted’. Others were more specific in the skills they described, noting: ‘His strong points are his numbers, alphabets, colo[u]rs and his attitude to adapt and learn’.
Social and interpersonal strengths
The second most frequently identified theme, ‘social and interpersonal’, included strengths that required a relationship or connection with others. Caregivers described 11 unique social and interpersonal categories of strengths, which were identified 411 times in 280 children (40.8%). The most identified was ‘kind, caring, and compassionate’. This was also the most frequently identified category across the data set, appearing 115 times across 98 children. Caregivers described their children as having a ‘very caring nature’ and ‘kind heart’. One described this strength in their son: ‘He is such a loving and caring person with a genuine and gentle soul. He cares more for others than himself’. Other social and interpersonal strengths included being loving and affectionate (identified 92 times across 88 children), friendly and social (identified 88 times across 87 children), and having good communication and language skills (identified 50 times across 49 children). Some caregivers noted their children liked cuddles, having fun, and helping around the house. Another described their daughter as ‘Such a happy and friendly girl who people genuinely love being around’.
Hobbies and passions
Hobbies and passions were categorised when caregivers identified that a child enjoyed the activity, regardless of whether it was noted they were good at it. In some instances, caregivers described their child’s passion for a pastime, for example, ‘Loves art and great at painting and drawing. Loves making things (craft activities) for hours on end’. Other caregivers listed single activities, such as cars, baking, or music. Activities were included in ‘hobbies and passions’ if they could not be more accurately included under other categories and themes. For example, a love of sport was included under ‘physical’ strengths and a love of reading in ‘cognitive and intellectual’. Overall, caregivers described 10 unique categories for hobbies and passions, which were identified 341 times in 258 children (37.6%). The most frequently identified was ‘music, singing, and dancing’ (identified 92 times across 89 children), followed by ‘drawing, painting, arts, and craft’ (identified 60 times across 59 children), and ‘video games and technology’ (identified 57 times across 57 children). There was also a clear passion for Lego (identified 51 times), with one caregiver noting ‘She loves building and will play with Lego for hours’.
Character and personality strengths
Caregivers identified 12 unique personality strengths that can be said to describe their children’s characters in circumstances outside of direct interaction with others, including being outgoing, independent, honest, and having a great sense of humour. Character and personality strengths were identified 303 times across 230 children (33.5%), with the most common categories being ‘happy, joyful, smiley and positive’ (identified 61 times across 59 children), ‘creative and imaginative’ (identified 52 times across 49 children), and ‘curious, adventurous, tries new things’ (identified 51 times across 48 children). Some caregivers described their children’s ‘bubbly, friendly, positive & happy personality’ and ‘joy for the world . . ’. Others noted their child is ‘curious and always wants to explore new things’ or that they are ‘very independent and determined’.
Physical strengths
Caregivers frequently listed areas where they felt their children excelled at or enjoyed physical activities, including gross and fine motor skills, as well as sport and more general outdoor activities. Six unique categories were identified, with strengths appearing 220 times across 185 children (27.0%). Caregivers most frequently described strengths in gross motor skills (identified 72 times across 72 children), including throwing, jumping, climbing, and running. One caregiver noted their child had good balance and ‘could ride a bike without training wheels from 2 years old’. Other common physical strengths included a love of sport (identified 58 times across 58 children) and being active and energetic (identified 36 times across 36 children), with one caregiver describing: ‘Over the past 12 months or so, he has really developed physically. He’s very strong, he loves to walk and run around’.
Behavioural strengths
Behavioural strengths were categorised as those pertaining to concrete patterns of behaviour, generally outside of interpersonal interactions. There were 10 distinct categories, with caregivers endorsing these strengths 179 times in 139 children (20.3%). Caregivers most frequently described strengths in perseverance and determination (identified 58 times across 51 children), politeness and being well-behaved (identified 29 times across 28 children), and following routines and instructions (identified 23 times across 22 children). One caregiver noted their child was ‘Very strong willed, determined and persistent’ while another suggested their daughter ‘always strives to do her best no matter how she is feeling’. Behavioural strengths were perhaps the most diverse theme, with caregivers identifying that children were variously obedient yet strong-willed, and adherent to routine, yet adaptable to change.
The CANS Checklist
The identified categories and themes were used to develop a strengths-based checklist, the CANS Checklist. We consulted community representatives (n = 6) and clinicians (n = 6) to seek feedback on the CANS Checklist. Following consultation and feedback, three modifications to the checklist were made. First, we added an ‘other’ option for each theme, enabling caregivers to list any strengths that had not been captured within the identified categories. Second, we provided brief explanations and examples for some checklist items. This was in response to suggestions from clinicians and community representatives that caregivers may benefit from examples and explanations for certain items. Third, certain checklist items were separated or expanded upon. For example, the item ‘eating and sleeping’ under the physical theme was split into two options: ‘sleeping’ and ‘eating’. In addition, a new item, ‘shared engagement and attention when playing with others’ was included under the social and interpersonal theme following clinician feedback that inclusion of specific strengths in joint attention would inform clinical assessment and feedback.
In addition, community representatives and clinicians provided feedback on how the CANS Checklist could be integrated within the clinical assessment process. Feedback included recommendations that the checklist be completed by families shortly before or at the time of their assessment, and used in conjunction with standard clinical assessments and observations to inform feedback and intervention strategies that can be tailored to child strengths. Feedback sessions also highlighted the potential utility of this checklist for families from culturally diverse backgrounds, and the need for translation into other languages. The resulting CANS Checklist is shown in Supplementary Figure 1.
Caregiver-identified strengths – differences between autistic and non-autistic children
Chi-square tests were used to compare the frequency of themes between children who received an autism diagnosis and children who did not receive an autism diagnosis. As shown in Table 2, there were no differences in the frequency of caregiver-identified strengths between autistic and non-autistic children for hobbies and passions, character and personality strengths, physical strengths or behavioural strengths. Caregivers of autistic children more frequently identified cognitive and intellectual strengths, compared to caregivers of non-autistic children, χ2(1) = 8.02, p = 0.005. In contrast, caregivers of autistic children were less likely to identify social and interpersonal strengths, compared to caregivers of non-autistic children χ2(1) = 37.32, p < 0.001. However, these themes remained common in the sample, with over a third of caregivers of autistic children identifying social and interpersonal strengths.
Chi-square results for caregiver-identified strengths between autistic and non-autistic children.
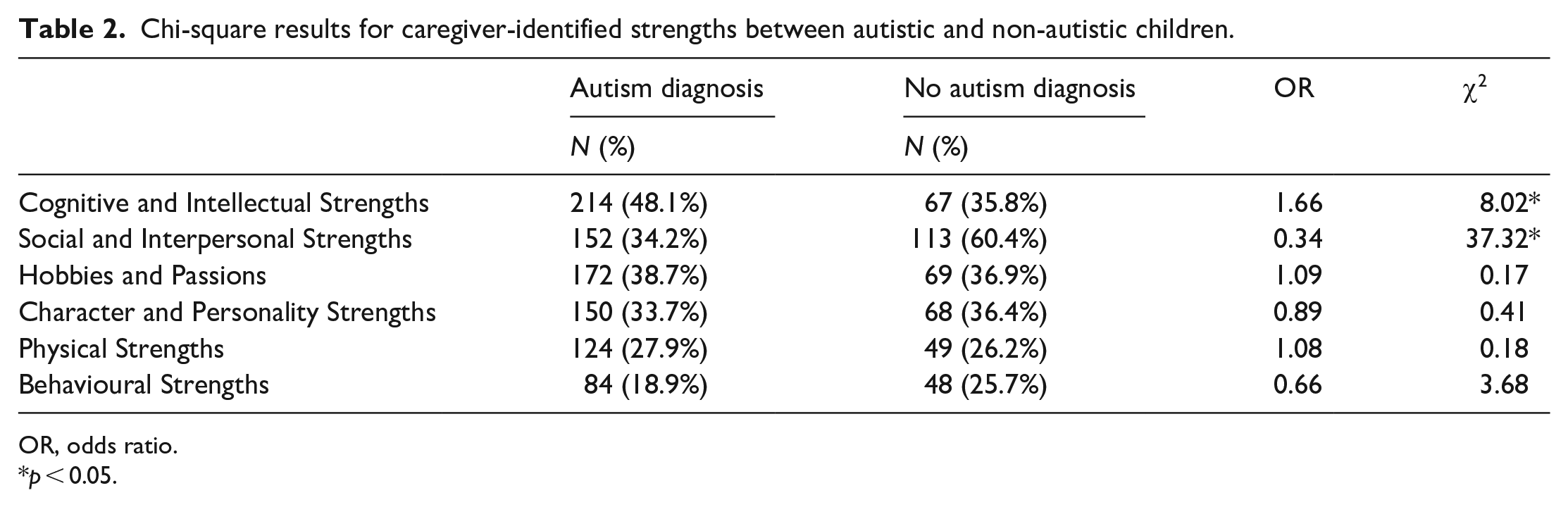
OR, odds ratio.
p < 0.05.
Discussion
To our knowledge, this is the first study to examine caregiver-identified strengths in children with neurodevelopmental concerns at the time of their first diagnostic assessment, most commonly autism assessments. While past studies have emphasised the value of understanding perceived child strengths, there is currently a lack of understanding about the breadth and types of strengths reported by caregivers at assessment. On average, caregivers nominated 2.8 strengths for their children. Strengths were categorised into six themes: cognitive and intellectual, social and interpersonal, hobbies and passions, character and personality, physical, and behavioural. There were 61 categories, each representing a unique strength, and reflecting the depth and breadth of skills, abilities, and positive qualities children with NDCs may possess (Carter et al., 2015). When comparing the frequency of caregiver-identified strengths between children who received an autism diagnosis (n = 445/632; 70%) and those who did not (n = 187/632; 30%), there were more similarities than differences. Importantly, the most frequent domains of strength are also domains that might traditionally be considered as domains of need. A total of 44.7% of caregivers nominated cognitive and intellectual skills as a strength, while 40.8% nominated social and interpersonal abilities as a strength. This aligns with prior qualitiative findings in autistic children, where certain social and interpersonal strengths, such as a kind, loving, and affectionate nature, have been identified as leading individual and caregiver-child relationship strengths to support family cohesion and relationship development (Potter, 2016). Such findings highlight the potential to integrate these common caregiver-identified strengths into the assessment process. To this end, we have presented a checklist, the CANS Checklist (see Supplementary Figure 1), that can be used by clinical services to promote a strengths-based approach to diagnostic assessments. This checklist was developed based on the categories and themes that arose from our qualitative analysis, and was modified following consultation and feedback with community and clinician representatives. Together, these findings highlight the urgent need for research to evaluate the impact of using strengths-based assessments to benefit children, caregivers and support systems.
Our findings support previous literature evaluating perceived strengths in NDCs such as autism, which consistently highlight children’s cognitive strengths (Sabapathy et al., 2017; Warren et al., 2021). When we directly compared the frequency of caregiver-identified strengths between children who received an autism diagnosis and children who did not, few differences emerged. Indeed, the only themes where differences emerged were cognitive and intellectual strengths, and social and interpersonal strengths. Relative to caregivers of non-autistic children, caregivers of autistic children more frequently identified cognitive and intellectual strengths, and less frequently identified social and interpersonal strengths. This pattern of results aligns with prior findings in paediatric autistic cohorts, where cognitive strengths are commonly reported, and social and personality strengths can be less commonly reported (Sabapathy et al., 2017). Despite these differences, these themes remained common across our cohort, with cognitive and intellectual strengths identified in over a third of non-autistic children, and social and interpersonal strengths reported in over a third of autistic children. Of note, some strengths, such as attention to detail, were not commonly identified in this cohort of children, despite being commonly reported as strengths in prior studies with older individuals on the autism spectrum (Cope & Remington, 2022). This may reflect the importance of asking caregivers about strengths in different settings, as strengths identified in the context of asking broadly about development may differ to those identified across in specific settings (e.g. at school, or when completing specific tasks). Taken together, these findings suggest that the themes and categories identified in this study are relevant for informing a strengths-based approach to assessment for children with diverse developmental concerns and NDCs, including autism.
Consideration can also be given to how these caregiver-identified strengths could inform future strengths-based assessment frameworks, while taking care not to increase clinician burden, given the scarce resources available in clinical services providing autism assessments (Vivanti & Volkmar, 2019). Themes could be used by clinicians to help capture, quantify, and report on children’s strengths in areas of the diagnostic narrative where this is not currently the focus, as well as building on other areas, such as the verbal feedback session. To support this approach, we have collated the themes and underlying categories identified in this study into a checklist. This checklist was modified following consultation and feedback with community and clinician representatives, to ensure it had utility and applicability for children, families and clinicians. These feedback sessions provided guidance around how the CANS Checklist can be integrated within the clinical assessment pathway to facilitate a strengths-based approach to assessment and diagnosis. Based on this feedback, we suggest that the CANS Checklist can be completed by caregivers before assessment and can then be used by clinicians when conducting feedback sessions and providing recommendations to families. Discussing child strengths, and personalising intervention strategies based on those strengths, will promote a strengths-based approach from the start of the diagnostic process. Providing such structure to clinical services may build collaborative opportunities to increase strengths-based feedback to families, further empowering families across their assessment journey (Boulton, Hodge, Levu, et al., 2023; Munro et al., 2023). Identified strengths within each theme could also be included alongside structured assessment results in reporting templates, to help caregivers and clinicians acknowledge where challenges, such as a need for routine, can also operate as strengths (McCrimmon & Montgomery, 2014; Warren et al., 2021). Already there are online tools and resources available that promote an emphasis not only on deficits but strengths which are easily accessible for clinicians and could be integrated into reporting processes (e.g. Positive Partnerships). Further exploration is now required into how clinicians currently identify and report on strengths during the diagnostic narrative and how caregivers and clinicians would like strengths to be accessibly and meaningfully integrated into reports. Such an approach does need to be balanced with the current funding landscape though, to ensure that changes do not result in adverse impacts with respect to how this information may be used by funding bodies who use these reports to determine funding allocation for therapies and supports.
The findings of this study can be used to inform a strengths-based neuroaffirming approach for children, adolescents and adults on the autism spectrum across a range of contexts, including diagnostic settings, as well as within schools and workplaces. Currently, many supports and interventions for individuals on the autism spectrum focus on minimising challenges (Burnham Riosa et al., 2017; Crane et al., 2018). However, the inclusion of strengths recognition and development when designing supports may facilitate awareness of strengths, as well as how traits commonly considered challenges for individuals on the autism spectrum, such as a need for routine, can also operate as strengths, provided the individual is matched with an appropriate and accommodating environment. Future research is critical for developing and evaluating the evidence base for a strengths-based approach both in terms of enhancing quality of life and in improving outcomes (e.g. school supports and sustained employment) for individuals on the autism spectrum.
This study’s strengths include its large data set of participants from diverse cultural and educational backgrounds receiving a diagnostic assessment at a hospital-based developmental assessment service. It also highlights the depth and breadth of strengths identified across a wide range of ages and presenting characteristics, rather than focusing on children with one specific NDC. Moreover, while prior research has used pre-defined frameworks when identifying and defining strengths, we utilised an open-ended question to elicit strengths from caregivers. This enabled identification of a broad range of strengths that may not be captured in existing frameworks, and may have been omitted if caregivers were required to select from a list of pre-determined strengths. Based on the categories that emerged from our qualitative analysis, we developed and sought community and clinician feedback on the CANS Checklist, and present a checklist that can be used to capture broad strengths and inform strengths-based assessments. Future research could also assess whether identified strengths vary when using our CANS Checklist versus an open-ended response, to understand whether responses differ when caregivers are asked to select versus nominate strengths.
The study has a number of limitations. First, extensive quantitative analysis was outside of the scope of study and future research should investigate how sociodemographic characteristics, child cognitive ability and child and caregiver mental health may impact caregiver-identified strengths. Second, we only included data where participants had responded to the strengths-based questions. Previous studies found a significant relationship between missing strengths-based data and socioeconomic risk factors (Cost et al., 2021), and between identified behavioural challenges and reduced ability to identify strengths (Carter et al., 2015; Cost et al., 2021). Third, as a retrospective study, data was limited to pre-written responses. Future research should further explore caregiver-identified strengths by interviewing caregivers and clinicians on how strengths are currently captured and reported and what changes they would like to see, as well as how these strengths are being drawn upon as part of a child’s ongoing treatment and/or education plan. In addition, future research would benefit from tracking caregiver-identified strengths over time to determine whether perceived strengths change across development, or in response to implemented supports and interventions. This would help to inform a strengths-based approach to future intervention and support planning. Finally, while the translation of the CANS Checklist into other languages was outside the scope of this study, it was raised as an important next step during our community and clinician feedback sessions, given the large proportion of culturally and linguistically diverse families attending these services.
Conclusion
This study demonstrates the broad range of caregiver-identified strengths in children with neurodevelopmental concerns at the time of diagnostic assessment. The depth and breadth of strengths identified in this study challenges multiple stereotypes about the characteristics of children with NDCs and provides a framework for how a strengths-based approach may be incorporated in diagnostic assessments and reports. To support clinical services in implementing a strengths-based approach from a child’s first diagnostic assessment, we present a checklist, the CANS Checklist, which can be completed by caregivers and integrated by clinicians into assessment feedback and recommendations. It is critical that future research evaluates how an accessible strengths-based reporting framework can support clinicians and caregivers to better understand children’s needs and access the most appropriate support at the point of first assessment.
Supplemental Material
sj-docx-2-aut-10.1177_13623613251325287 – Supplemental material for Caregiver-identified strengths in children attending their first neurodevelopmental assessment: Findings from the Sydney child development research registry and development of a child strengths checklist
Supplemental material, sj-docx-2-aut-10.1177_13623613251325287 for Caregiver-identified strengths in children attending their first neurodevelopmental assessment: Findings from the Sydney child development research registry and development of a child strengths checklist by Kelsie A Boulton, Lorna Hankin, Marie-Antoinette Hodge, Natalie Ong, Natalie Silove and Adam J Guastella in Autism
Supplemental Material
sj-pdf-1-aut-10.1177_13623613251325287 – Supplemental material for Caregiver-identified strengths in children attending their first neurodevelopmental assessment: Findings from the Sydney child development research registry and development of a child strengths checklist
Supplemental material, sj-pdf-1-aut-10.1177_13623613251325287 for Caregiver-identified strengths in children attending their first neurodevelopmental assessment: Findings from the Sydney child development research registry and development of a child strengths checklist by Kelsie A Boulton, Lorna Hankin, Marie-Antoinette Hodge, Natalie Ong, Natalie Silove and Adam J Guastella in Autism
Footnotes
Acknowledgements
We would like to thank all of the families who have contributed to the Sydney Child Neurodevelopment Research Registry and the staff from the Child Development Unit who have provided clinical support to families and supported data collection, as well as the research staff from Clinic for Autism and Neurodevelopment Research who have assisted data collection and database management. We thank the Brain and Mind Centre Neurodevelopment Community Research Advisory Committee for their consultation. We also thank the Brain and Mind Centre Child Development and Mental Health Team, and Sydney Health Partners Child Development and Mental Health Developmental Clinical Academic Group, for support of this project.
Author contributions
K.A.B.: Conceptualisation; Data curation; Formal analysis; Methodology; Project administration; Supervision; Visualisation; Writing – original draft; Writing – review & editing.
L.H.: Data curation; Formal analysis; Methodology; Writing – original draft.
M.-A.H.: Data curation; Investigation; Methodology; Project administration; Resources; Supervision; Writing – review & editing.
N.O.: Data curation; Formal analysis; Investigation; Methodology; Project administration; Resources; Supervision; Writing – review & editing.
N.S.: Conceptualisation; Investigation; Methodology; Project administration; Resources; Supervision; Writing – review & editing.
A.J.G.: Conceptualisation; Formal analysis; Investigation; Methodology; Project administration; Resources; Supervision; Visualisation; Writing – original draft; Writing – review & editing.
Data availability statement
Data are available upon reasonable request.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship and/or publication of this article.
Ethical statement
The study was approved by the Sydney Children’s Hospital Network Human Research Ethics Committee (LNR/17/SCHN/293; Child Development Registry).
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.