
Abstract
Autism spectrum disorder and anxiety are highly comorbid conditions. Understanding the underlying traits of anxiety in autism spectrum disorder is crucial to prevent and treat it efficiently. Hence, this study determined whether social communication difficulties or restricted repetitive behaviors are stronger risk factors for anxiety symptoms in autistic adults in a large cohort. Data on 742 autistic adults from the Netherlands Autism Register were included in the study. Hierarchical regression was implemented to evaluate whether social communication difficulties (Autism-Spectrum Quotient social behavior factor) and restricted repetitive behaviors (Adult Routines Inventory) were predictive of anxiety (Hospital Anxiety and Depression Scale) controlling for age and sex. When considered together, restricted repetitive behaviors stood out as significant positive predictors of anxiety symptoms (lower-order restricted repetitive behaviors, β = 0.32, p < 0.001; higher-order restricted repetitive behaviors, β = 0.15, p = 0.001), whereas social communication difficulties did not (β = 0.06, p = 0.11). Sex did not moderate these associations (p > 0.05). Non-social autistic traits are stronger predictors of anxiety symptoms than social traits in autistic adults. Increased attention to restricted repetitive behaviors should be given to improve current support programs for autistic adults with anxiety and to identify autistic individuals at risk.
Keywords
Introduction
Autism spectrum disorder (ASD) is a developmental condition characterized by difficulties in social communication and by restricted repetitive behaviors (RRBs) (American Psychiatric Association, 2013). One of the most common comorbidities in ASD is anxiety—approximately 30% of autistic adults meet a diagnosis for an anxiety disorder (Hollocks et al., 2019). Comorbid anxiety in autism has been associated with personal burden, including suicidality or self-injurious behavior (Storch et al., 2013), and substantial societal costs (van Steensel et al., 2013). Given the high rates of comorbid ASD and anxiety, and its personal and societal burden, it is essential to determine which key features of autism—namely, social communication difficulties or RRBs—are stronger risk factors for the development of anxiety in autistic adults.
Social communication concerns a variety of different skills, including social engagement, initiation, and maintaining (Vicker, 2009). Autistic individuals find it challenging to interpret social cues (Meyer et al., 2006) or maintain conversations (Volden, 2004), often resulting in a lower quality of social relationships (Baron-Cohen & Wheelwright, 2003). These difficulties with social communication may give rise to anxiety and further social withdrawal. Indeed, previous studies have shown a significant association between impaired social communication skills or social deficits and anxiety in autistic children (Chang et al., 2012; Eussen et al., 2013). However, when considered together with RRBs, social communication difficulties have not significantly contributed to anxiety (Magiati et al., 2016; Teh et al., 2017).
RRBs can be divided into two types: lower-order and higher-order (Bishop et al., 2013). Lower-order RRBs focus on repetitive sensory–motor behaviors (e.g. body rocking), whereas higher-order RRBs focus on the insistence on sameness behaviors (e.g. routines). A significant positive association between RRBs and anxiety in autistic children has been reported, even when RRBs have been considered together with social communication difficulties (Magiati et al., 2016; Teh et al., 2017). However, the evidence for the particular type of RRBs is inconsistent. Some findings have indicated that anxiety is significantly associated with higher, but not lower-order, RRBs in autistic children (Russell et al., 2019), while other evidence has revealed that both types of RRBs are significantly linked to anxiety in autistic youth (Joyce et al., 2017). Some argue that both types of RRBs facilitate anxiety, while others point to RRBs, especially higher-order, acting as a coping mechanism for anxiety (Joyce et al., 2017; Spiker et al., 2012). In either case, engagement in RRBs may undermine an individual’s interaction with their environment, thereby increasing their worry about the uncertainty of the world.
To our knowledge, only one cohort study has been conducted to understand the differential contribution of social communication difficulties and RRBs to anxiety symptoms in ASD. When considered together, RRBs were significantly associated with anxiety, while social communication difficulties were not associated with anxiety both cross-sectionally (Magiati et al., 2016) and longitudinally (Teh et al., 2017) within the same sample. However, the results were limited to a relatively small sample of children, parent reports, and no exploration of different types of RRBs. Providing further insights on whether social or non-social autistic traits contribute more to anxiety in adulthood is essential, as to date, research predominantly has relied on children samples and parent reports. Evidence in adults may shed more light on how age uniquely influences these associations across the developmental period, help to prevent comorbid anxiety in adults at risk, and improve interventions mostly focusing on social skills (Ung et al., 2015). Hence, this study aimed to determine the relative contribution of social communication difficulties and RRBs as predictors of anxiety symptoms in autistic adults in a large cohort using self-reported instruments.
Methods
Sample
Data from a longitudinal cohort database—the Netherlands Autism Register (NAR) (Wierda et al., 2015)—were used. The NAR invites registered participants to fill out an online survey annually. The original sample includes 1709 autistic adults (18–65 years old) with a formal diagnosis of ASD made by a qualified clinician, based on the Diagnostic and Statistical Manual of Mental Disorders (4th ed.; DSM-IV) or Diagnostic and Statistical Manual of Mental Disorders (5th ed.; DSM-5). The sample of this study included 742 participants (43.4% of the original sample) with an available measure of social communication difficulties, RRBs, and anxiety symptoms (assessed between 2016 and 2018 data collection of the NAR). All participants provided self-reported data, meaning that the sample is restricted to those participants able to complete online surveys. More detailed information about the NAR can be found on https://www.nederlandsautismeregister.nl/english/.
Instruments
Autism Quotient-Short
To determine self-reported social communication difficulties, the Autism Quotient-Short (AQ-Short) (Hoekstra et al., 2011) was used. The AQ-Short is a 28-item four-point Likert-type (1–4) measure (total score range = 28–112) assessing autistic social behavior traits (23 items; range = 23–92) and fascination by numbers and/or patterns (five items; range = 5–20). The social behavior factor (Autism Quotient social behavior (AQ-SB)) is divided into social skills (seven items; range = 7–28), routine (four items; range = 4–16), switching (four items; range = 4–16), and imagination (eight items; range = 8–32). In this study, data from the AQ-SB were used. A higher score indicates more social communication difficulties.
Adult Routines Inventory
To assess self-reported RRBs, the Adult Routines Inventory (ARI) (Evans et al., 2017) was administered. The ARI is a 55-item five-point Likert-type (1–5) measure assessing repetitive sensory–motor behaviors/compulsions (ARI-RSMBC, lower-order, 28 items) and rigidity/insistence on sameness (ARI-RIS, higher-order, 23 items). A higher score indicates more engagement in RRBs (range = 28–140 for the ARI-RSMBC; range = 23–115 for the ARI-RIS).
Hospital Anxiety and Depression Scale
To determine self-reported anxiety symptoms, the Hospital Anxiety and Depression Scale (HADS) (Zigmond & Snaith, 1983) was used. The HADS is a 14-item four-point Likert-type (0–3) measure assessing symptoms of depression (seven items, HADS-D) and anxiety (seven items, HADS-A). The severity of symptoms for each subscale is indicated as normal (0–7), mild (8–10), moderate (11–14), or severe (15–21). In this study, data from the HADS-A were used.
Data analysis
Before the main analysis, sample characteristics were explored descriptively and presented as mean (M) values with standard deviations (SDs), or numbers with percentages. Internal consistency (Cronbach’s alpha, α) was determined for the measures of social communication difficulties (AQ-SB), RRBs (ARI), and anxiety symptoms (HADS-A). To determine whether participants in our sample significantly differed in age and sex from those of the original NAR sample who did not take part in the 2016–2018 data collection (n = 967), independent samples t-test and chi-square test were performed.
To determine the contribution of social communication difficulties and RRBs as predictors of anxiety symptoms in autistic adults, a six-model hierarchical regression analysis was conducted. Age was entered in the first model, followed by sex in the second model to control for age and sex effects. Social communication difficulties (AQ-SB) were included in the third model, followed by lower-order RRBs (ARI-RSMBC) in the fourth model, and higher-order RRBs (ARI-RIS) in the fifth model. To determine the potential moderating role of sex, interaction variables (social communication difficulties × sex, lower-order RRBs × sex, and higher-order RRBs × sex) were included in the sixth model. Anxiety symptoms (HADS-A) were the dependent variable in all the models. Every questionnaire required full completion for the submission; therefore, missing data on questionnaire items were not an issue. On the basis of having 742 participants, a post hoc power to detect small to large effect size (f2 = 0.02–0.35) with eight predictors was high (79%–100%, α = 0.05, two-tailed, G*Power). All data were interpreted using the IBM SPSS 25 (International Business Machines (IBM) Corp., 2017).
Results
Sample characteristics
The mean age of participants was 43.82 years (SD = 12.19), with the majority being female (58.8%; Table 1). Most of the sample had a high level of education (44.1%) and a high-average self-reported intelligence quotient (IQ) score (48.1%). When compared to the adults of the original NAR sample who did not take part in the 2016–2018 data collection (n = 967), our sample was significantly older and included more females (age, M = 33.85, SD = 13.59 vs M = 43.82, SD = 12.19, p < 0.001; female, 40.6% vs 58.8%, p < 0.001, respectively). Internal consistency of the measures ranged from good to excellent: α = 0.86 for the AQ-SB, α = 0.88 for the ARI-RSMBC, α = 0.93 for the ARI-RIS, and α = 0.85 for the HADS-A.
Demographic characteristics of participants.
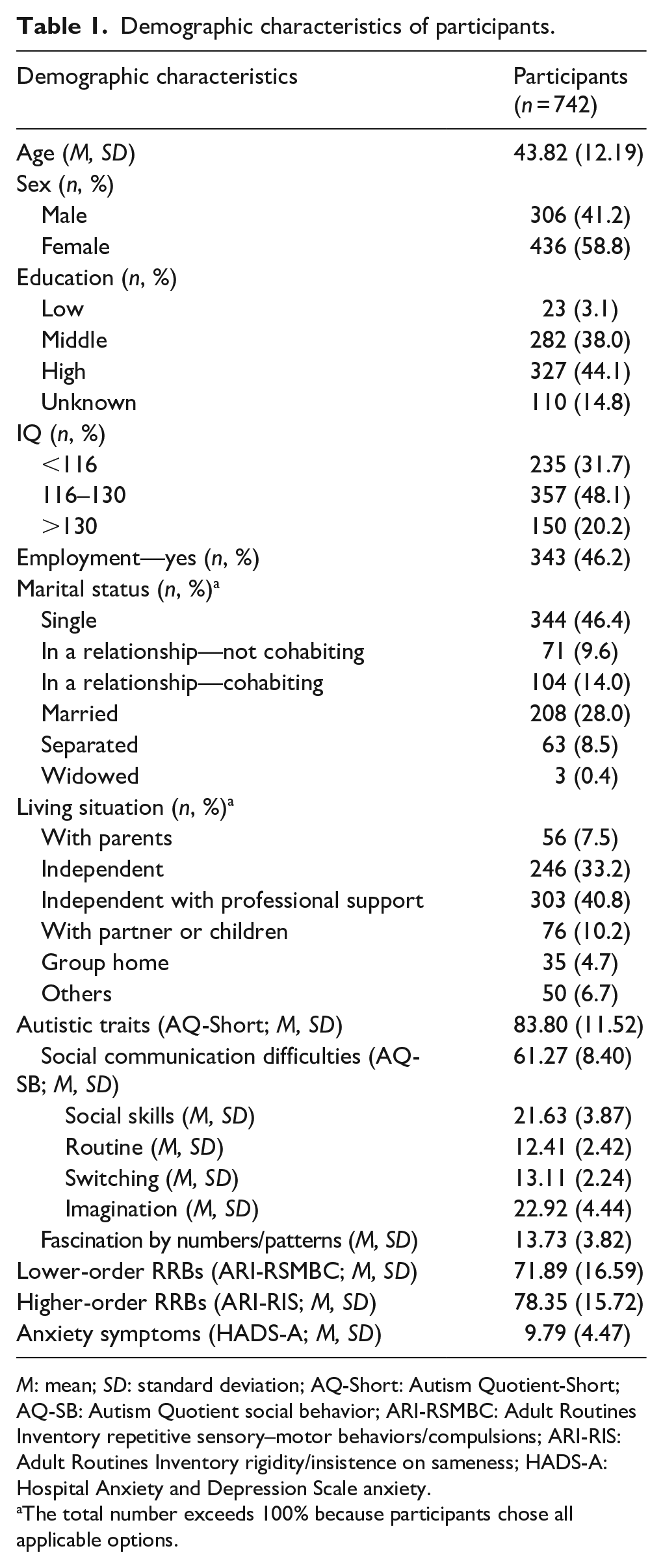
M: mean; SD: standard deviation; AQ-Short: Autism Quotient-Short; AQ-SB: Autism Quotient social behavior; ARI-RSMBC: Adult Routines Inventory repetitive sensory–motor behaviors/compulsions; ARI-RIS: Adult Routines Inventory rigidity/insistence on sameness; HADS-A: Hospital Anxiety and Depression Scale anxiety.
The total number exceeds 100% because participants chose all applicable options.
Associations between social communication difficulties, RRBs, and anxiety
A summary of the six hierarchical regression analyses is provided in Table 2. Model 1 including age only was not significant (R2 = 0.001, F(1, 740) = 0.71, p = 0.40). Model 2 additionally including sex was significant (R2 = 0.05, F(1, 739) = 37.64, p < 0.001), as well as Model 3 including social communication difficulties (R2 = 0.11, F(1, 738) = 45.61, p < 0.001). The addition of lower-order RRBs in Model 4 also resulted in a significant change of the variance explained by the model (R2 = 0.23, F(1, 737) = 124.64, p < 0.001), as well as the addition of higher-order RRBs in Model 5 (R2 = 0.25, F(1, 736) = 11.59, p = 0.001). The latter model including social communication difficulties and both types of RRBs accounted for 25% of the variance in anxiety symptoms. Both lower- and higher-order RRBs significantly predicted anxiety (ARI-RSMBC, β = 0.32, p < 0.001; ARI-RIS, β = 0.15, p = 0.001) when considered together with age, sex, and social communication difficulties. Lower-order RRBs explained a larger proportion of the variance in anxiety (12% on top of age, sex, and social communication difficulties), as compared to higher-order RRBs (2% on top of age, sex, social communication difficulties, and lower-order RRBs). Social communication difficulties did not significantly predict anxiety when age, sex, and both types of RRBs were considered together (AQ-SB, β = 0.06, p = 0.11, 6% of the variance explained on top of age and sex). Females scored significantly higher on social communication difficulties (M = 62.07, SD = 7.67 vs M = 60.13, SD = 9.23, p = 0.002), lower-order RRBs (M = 74.37, SD = 16.06 vs M = 68.37, SD = 16.73, p < 0.001), higher-order RRBs (M = 80.33, SD = 14.69 vs M = 75.53, SD = 16.70, p < 0.001), and anxiety symptoms (M = 10.61, SD = 4.15 vs M = 8.61, SD = 4.65, p < 0.001) when compared to males. However, sex did not moderate the associations between the independent and dependent variables, as indicated by no significant social communication difficulties × sex (p = 0.32), lower-order RRBs × sex (p = 0.31), and higher-order RRBs × sex (p = 0.78) interactions in Model 6 (R2 = 0.25, F(3, 733) = 0.72, p = 0.54).
Summary of hierarchical regression with six models predicting anxiety symptoms (HADS-A).
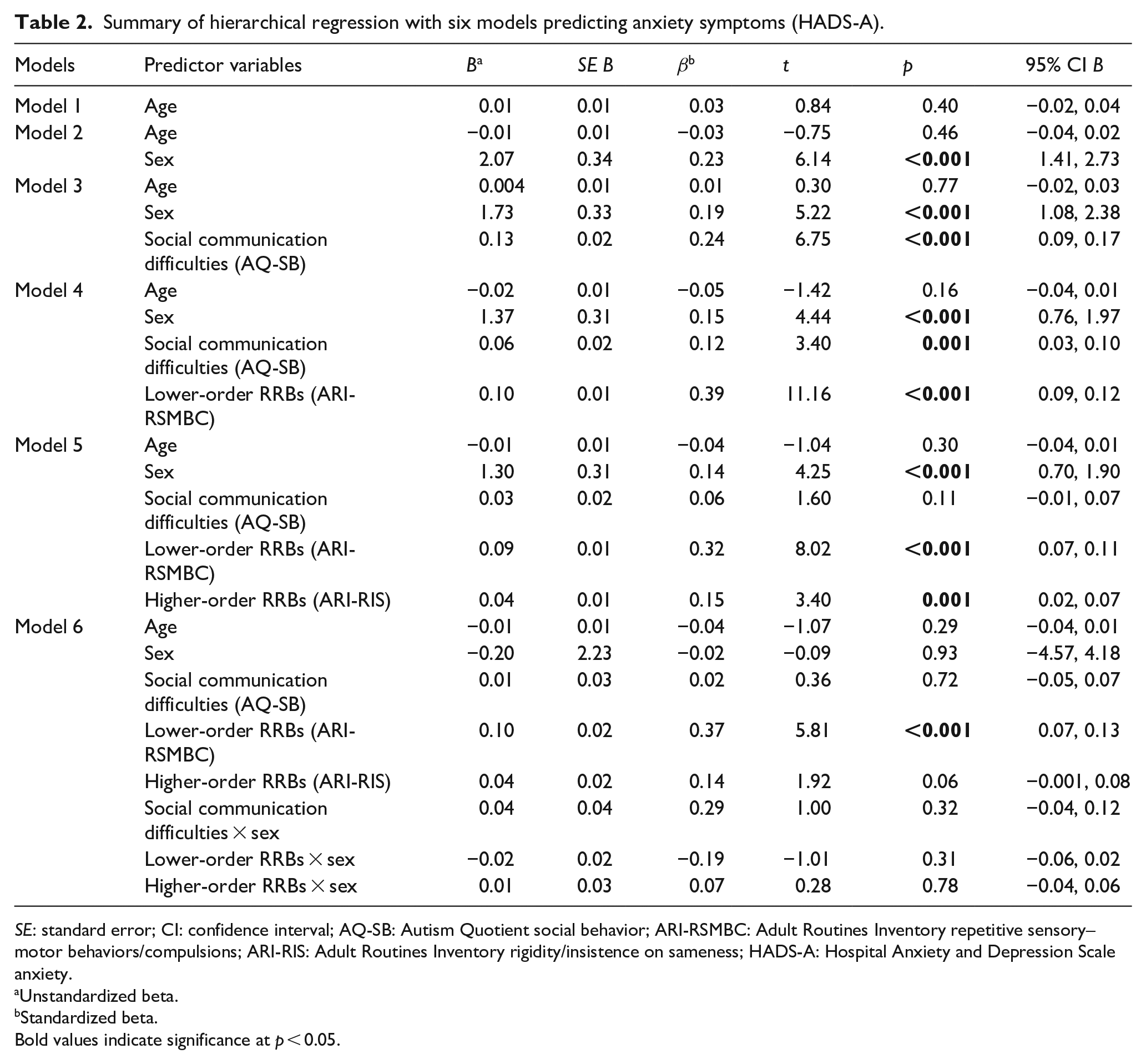
SE: standard error; CI: confidence interval; AQ-SB: Autism Quotient social behavior; ARI-RSMBC: Adult Routines Inventory repetitive sensory–motor behaviors/compulsions; ARI-RIS: Adult Routines Inventory rigidity/insistence on sameness; HADS-A: Hospital Anxiety and Depression Scale anxiety.
Unstandardized beta.
Standardized beta.
Bold values indicate significance at p < 0.05.
Discussion
This study examined whether social communication difficulties or RRBs are stronger risk factors for anxiety symptoms in autistic adults. The mean level of anxiety in the present sample was mild and comparable to that identified in Australian and British adolescents and young autistic adults (Uljarevic et al., 2018). Our findings indicated that both higher-order and lower-order RRBs significantly and positively predicted anxiety symptoms when controlling for age, sex, and social communication difficulties. In contrast, when considered together with RRBs, social communication difficulties did not predict anxiety in autistic adults. These findings are in line with the results of a study in autistic children using parent-reported measures (Magiati et al., 2016). The latter study identified a significant positive association between RRBs and parent-reported anxiety, while no unique association was observed with social communication difficulties either cross-sectionally (Magiati et al., 2016) or longitudinally (Teh et al., 2017). Our study adds to these results, reporting that both higher- and lower-order RRBs contributed to adult anxiety, while social communication difficulties did not uniquely contribute to anxiety symptoms. These findings provide new insights, indicating that both lower-order and higher-order RRBs contribute to anxiety, and extend Magiati et al. (2016) and Teh et al. (2017) findings to adult samples.
While sex was not determined as a significant moderator between autistic traits and anxiety, females, on average, scored significantly higher on social communication difficulties, RRBs, and anxiety symptoms. This is consistent with previous findings showing that autistic adolescent females, on average, have poorer social skills (Mahendiran et al., 2019), engage in more RRBs (Antezana et al., 2019), and have more anxiety symptoms when compared to males (Wijnhoven et al., 2018). Our findings show that this is true for autistic adult females as well.
It is important to note that social communication difficulties significantly predicted anxiety when considered with lower-order RRBs, but this relationship disappeared after controlling for higher-order RRBs. This could be a result of some social communication difficulties’ items (i.e. items assessing preference for routine and difficulty with attention switching) mapping on the higher-order RRBs. However, the correlation between social communication difficulties and higher-order RRBs was only moderate (r = 0.54, p < 0.001), suggesting that multicollinearity was not an issue. Loading of the routine and switching subscales on social communication difficulty factor was previously explained as a cognitive demand for successful social communication, requiring novelty and attentional switching skills (Hoekstra et al., 2011).
The findings of this study can be interpreted in various ways. Social communication difficulties may not be a significant predictor of broader anxiety symptoms compared with RRBs, but a more unique predictor of anxiety, specifically concerning the social world. This is consistent with previous research reporting a significant link between autistic social traits and social anxiety (Spain et al., 2018), while no association with broader anxiety symptoms (Hollocks et al., 2014). The idea is further supported by a study in which both types of RRBs showed a significant relationship with broader anxiety symptoms in autistic youth (Joyce et al., 2017). The finding of not only higher but also lower-order RRBs predicting anxiety in autistic adults supports ideas of both types of RRBs acting either as contributors to the development or as coping mechanisms for anxiety (Spiker et al., 2012). For instance, adult engagement in the insistence on sameness or repetitive sensory–motor behaviors may limit interaction with the environment, thereby increasing worry about the uncertainty of the world, or act as a way to control the unpredictable environment. However, longitudinal research on a broader range of risk factors for comorbid anxiety in autism is necessary to compare and interpret existing findings.
Strengths and limitations
With a sample of more than 700 adult participants and using previously validated instruments, this study possesses adequate power to determine the importance of RRBs in anxiety. Self-reports rather than parent reports were used to provide a better picture of autistic traits and anxiety symptoms from the perspective of autistic adults themselves. The main limitation of this study is the nature of its design. Reliance on self-reported data means that these results may not generalize to autistic individuals unable to complete questionnaires themselves. However, as both autistic traits and anxiety are personal and inevitably viewed through an individual lens, the best person to ask is the autistic individuals themselves. The AQ-SB subscale can also be considered not a “pure” measure of social communication difficulties, as it includes items that may map on higher-order RRBs. Hence, future studies should carefully consider the measure of social communication difficulties. Finally, the cross-sectional data do not allow an examination of developmental trajectories among autistic traits and anxiety. To disentangle causal links between social communication difficulties, RRBs, and anxiety in autistic adults, the longitudinal design is necessary. Considering that NAR invites participants to fill out the instruments annually, the direction of the relationship between the variables is expected to be determined in future studies.
Implications and conclusion
This is the first study to examine the differential contribution of social communication difficulties and engagement in RRBs to anxiety symptoms in autistic adults. To date, research has predominantly relied on children samples with parent reports. Hence, we have expanded the knowledge using self-reports of autistic adults themselves. Based on our results, it can be concluded that both higher- and lower-order non-social autistic traits are stronger risk factors for comorbid anxiety than autistic social traits in adulthood. Increased attention to the engagement in RRBs should be given, to not only optimize the efficacy of current support programs for autistic adults with anxiety but also to prevent the development of anxiety by identifying autistic individuals at risk.
Footnotes
Acknowledgements
The authors acknowledge the contribution of participants and the funder.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The Netherlands Autism Register was financially supported by the NWO (grant no. Aut.17.006) and the ZonMW (grant no. 40-00812-98-16064).