
Abstract
Background
Doravirine (DOR) is a non-nucleoside reverse transcriptase inhibitor (NNRTI) approved for HIV-1 infection treatment. Because of its genetic barrier, DOR appears to be a good alternative in switch strategies compared to other NNRTI. Our aim was to evaluate the percentage of people living with HIV (PLWHIV) followed in our center who could be eligible to a DOR-based regimen.
Methods
We collected data from all treatment-experienced PLWHIV, never exposed to DOR and with a demonstrated virological suppression. We analyzed previous genotypic analyses, clinical history, and previous exposure to NNRTIs.
Results
We analyzed data from 653 patients, whose characteristics are shown in Table 1. 59% of them presented no resistance mutation (RAM) at genotypic analysis. The most common DOR-related RAM were V106A, Y181V, and Y188L. We also analyzed RAM that can possibly interfere with combination therapy (mostly K65R and M184V). In the end, 81.8% of our patients results to be eligible for a DOR-based therapy regimen.
Conclusions
DOR represents a good option for switch strategies in virological suppressed PLWHIV. It seems to have a higher genetic barrier and a lower risk for resistance mutation development compared to other NNRTI. In our cohort, we found 81.8% of patients who could be eligible for a regimen containing DOR and almost 2/3 of patients who can be treated with the fixed-dose combination DOR/3TC/TDF.
Introduction
Doravirine (DOR) is a new non-nucleoside reverse transcriptase inhibitor (NNRTI) developed for the treatment of HIV-1 infection in people living with HIV (PLWHIV) with no known resistance-associated mutations. DOR has been approved both as a single-agent tablet and as a fixed combination tablet with lamivudine (3TC) and tenofovir disoproxil fumarate (TDF) [1].
Phase III clinical trials demonstrated the non-inferiority of DOR-based 3-drug regimens compared to NNRTI-based or PI-based regimens in terms of efficacy while also showing a higher tolerability and a significant improvement in metabolic parameters [2,3].
The most looked-after feature of DOR, however, is its efficacy in presence of some of the most common NNRTI-resistant mutations such as K103N and Y181C [4].
In cell culture both from wild-type HIV-1 and in NNRTI-resistant HIV-1, DOR-resistant strains were selected and studied. The most important amino-acid substitutions in RT are V106A, V106I, V106M, V108I, H221Y, F227C, F227I, F227L, F227V, M230I, L234I, P236L, and Y318F. The V106A, V106M, V108I, H221Y, F227C, M230I, P236L, and Y318F substitutions are the most important mutations, which conferred 3.4-fold–70-fold reductions in susceptibility to DOR [5,6].
V106A appeared to give the most important resistance against DOR. In subtype B, even alone it can cause an intermediate reduction in DOR susceptibility. Its effect increases in association with other mutations such as L234I and F227L [7]. In subtype A, V106A is followed by a triple mutations’ pathway: V108I/L234I/V106I. Even in subtype C, the V106A-resistant pathway emerged to be the most important, followed by the appearance of V106M and F227C [8].
No effects are described with other substitutions that affect other NNRTI-based regimens, such as efavirenz (L100I and K103N) and rilpivirine (E138K and K101P) [9].
Y188L mutation is also selected by DOR and seems to be associated with a high-level resistance but, unlike other NNRTI, other mutations such as Y188C, Y188H, and Y188F seem not to decrease DOR susceptibility [10].
M230L is an uncommon mutation [11] that can be rarely selected by a DOR-based treatment [12] and associated with a high-resistance level to every NNRTI [13].
Regarding other drugs that can be combined with DOR, genotypic analysis made both in cell culture and in patients treated with lamivudine showed the appearance of M184I and M184V substitutions, while treatment with TDF mostly showed the expression of K65R and K70E substitutions [14].
In our cohort of PLWHIV, we aimed to establish the percentage of PLWHIV eligible to start a DOR-based regimen based on historical genotype analysis.
Methods
For the purpose of our study, we analyzed all treatment-experienced PLWHIV in our cohort with at least one genotypic analysis available, never-before exposed to DOR and virologically suppressed (i.e., HIV-RNA <50 copies/mL) at last available visit.
We collected data regarding previous genotypic analyses, clinical history, and previous exposure to NNRTIs and performed a prevalence analysis. All patients signed informed consent for data collection.
Results
General population’s characteristics.
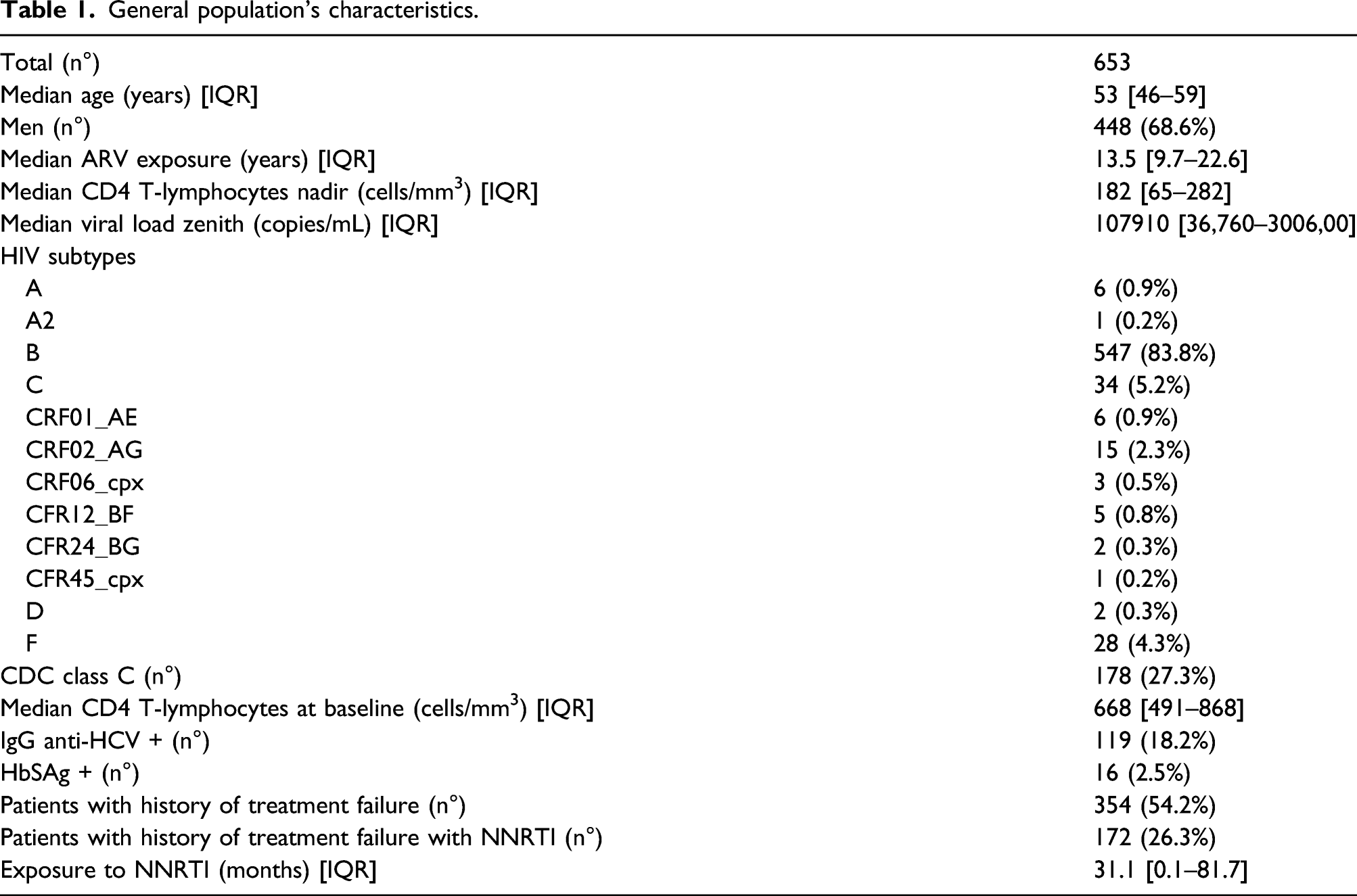
In the entire cohort, 59% (n = 385) of PLWHIV presented no resistance mutation (RAM) at genotypic analysis; the remaining 268 PLWHIV carried at least one mutation to RTIs in their historical genotype. The most common RAM was V106A, found in 38 (5.8%) of PLWHIV in our cohort: 34.2% in isolated form, while the remaining 65.8% associated with the M184V and K65R mutations, resulting in resistance to 3TC/FTC and TDF. Thirty-seven (5.7%) presented the Y181V mutation while 28 (4.3%) had the K101E mutation. Other observed mutations were the H221Y (9, 1.4%), the M230L (7, 1.1%), and the Y188L (6, 0.9%), with all six patients also presenting V106A and M184V mutations. Finally, 2 PLWHIV (0.3%) had the G190E mutation, 1 PLWHIV had the V106I, and another one presented the L234I and V106A mutations combined.
Patients with DOR-related RAM.
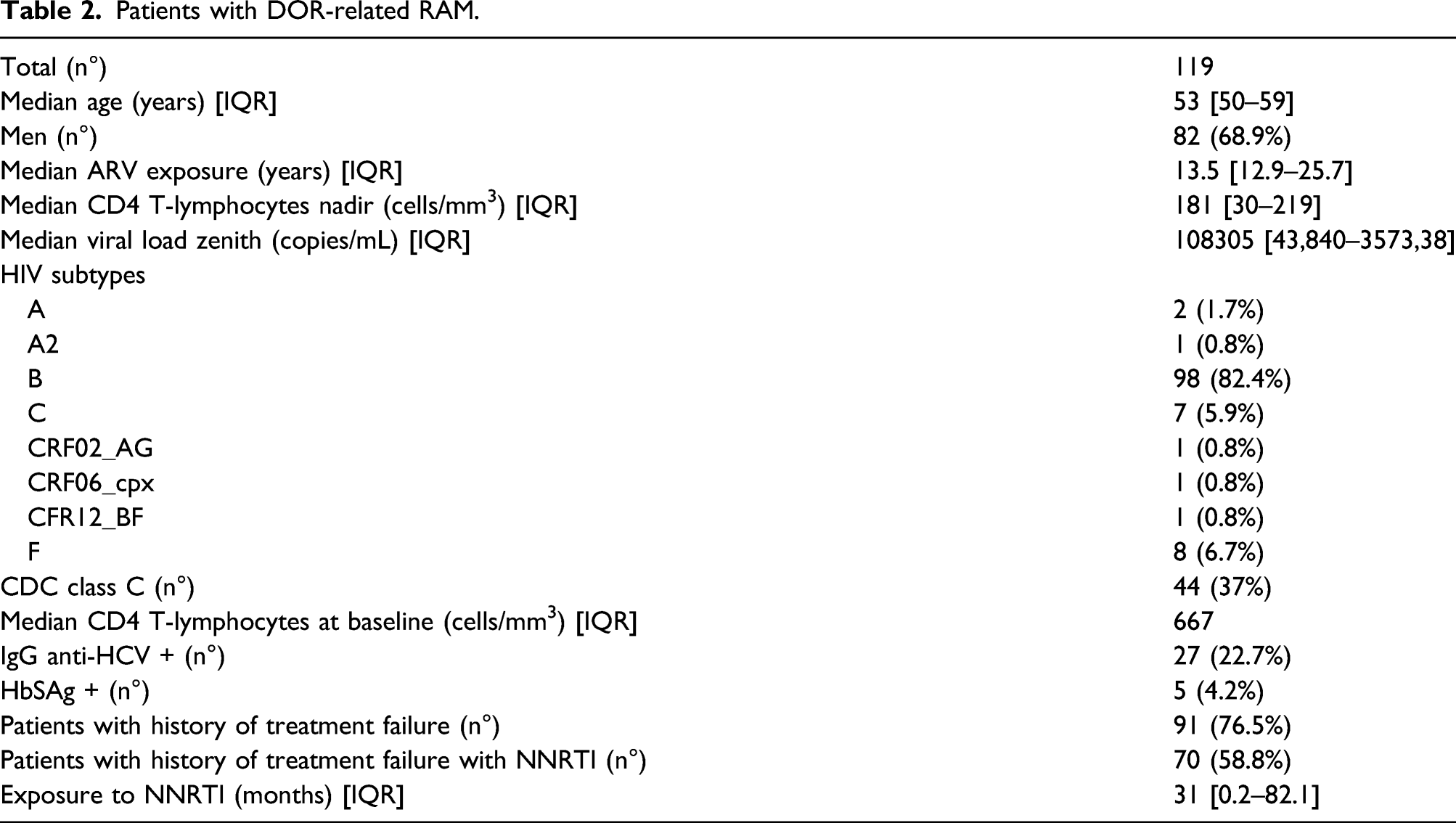
As for combination therapy, 21% (n = 137) of PLWHIV presented a mutation that guarantees resistance to TDF. In particular, 111 (17%) had a mutation in the TAM1 group (87 with M41L, 48 with L210W, and 92 with T215Y), 17 (2.6%) had the K65R mutation, and the remaining 9 (1.4%) presented other minor mutations such as K70E, Y115F, and Q151M (the latter in combination with F77L).
Finally, regarding resistance mutations to 3TC or FTC, 167 PLWHIV (25.6%) in our cohort had the M184V, 17 (2.6%) had the K65R, and 4 (0.6%) presented a combination of K70E, Q151M, and F77L.
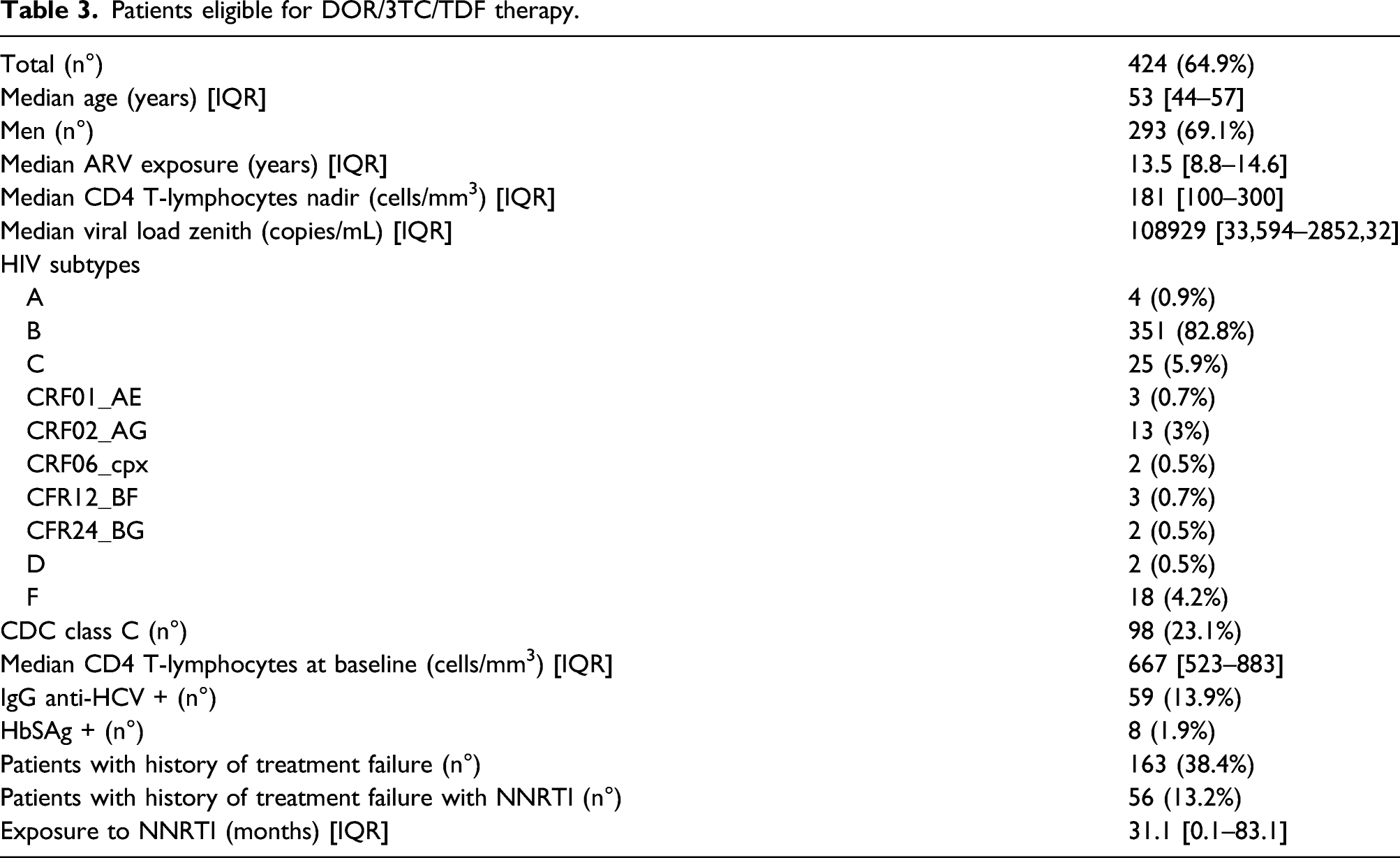
Patients eligible for DOR/3TC/TDF therapy.
Discussion
DOR represents an attractive option for the treatment of HIV-1 infection. Its efficacy and tolerability, confirmed in various clinical trials [2,3], have made DOR as a possible alternative to INIs and PIs as a switch option in clinical practice. Notably, issues of weight gain and/or metabolic toxicity have emerged with recently developed integrase inhibitors such as dolutegravir and bictegravir, as well as tenofovir alafenamide [15–17]; meanwhile, a recent meta-analysis of clinical trials shows a neutral effect of DOR, and the DOT/3TC/TDF combination, on metabolic parameters [18], making it an even more appealing switch strategies for the treatment of PLWHIV.
The extent past use of NNRTIs in the last two decades, however, has made clinicians aware of the risk of possible mutation resistances that may result in virological failure in case of inadequate therapy. DOR, however, has demonstrated a higher genetic barrier to resistance compared to older NNRTIs and, as a result, it could be used in a large proportion of PLWHIV.
In our cohort, 81.8% of PLWHIV presented a genotypic assay result appearing to be susceptible to an antiretroviral therapy containing DOR. This result is in line with previous findings from Italy [19] and confirms that DOR-based regimens may be appealing to a large proportion of PLWHIV in this country. Recent international guidelines [20] confirm the importance of performing genotypic tests, even with the availability of very-high genetic barrier regimens. In fact, as above stated, ARV toxicity in the medium-long term may force clinicians to modify ARV regimens, and thus, the availability of a baseline genotypic assay becomes crucial.
Regarding the fixed-dose combination of DOR/3TC/TDF, we found that almost 2/3 of our cohort may start said regimen, although of course the presence of RAMs to NRTIs reduce the eligible population compared to those eligible to DOR with other combinations of molecules.
Limits of our study are represented by its retrospective nature and the fact that it is a monocentric experience; nonetheless, our findings confirm that DOR-based regimens are an attractive switch option for the vast majority of treatment-experienced PLWHIV in Italy.