
Abstract
This cross-sectional study investigates the association between hedonic hunger and lifestyle and nutritional factors among hospital employees with different work schedules. A total of 220 healthcare professionals participated. Hedonic hunger, mindful eating, sleep quality, occupational stress, and diet quality were evaluated using validated scales. Compared to non-shift workers, those on rotating shifts had significantly higher levels of hedonic hunger (p = 0.013) and job stress (p < 0.001), alongside lower mindful eating scores (p < 0.001). Hedonic hunger was moderately correlated with poorer sleep quality (r = 0.335, p < 0.001) and increased job stress (r = 0.333, p < 0.001). Logistic regression analysis revealed that poor sleep quality increased the likelihood of elevated hedonic hunger by 27.8%, retaining significance after adjusting for age and sex (24.7%). Job stress was associated with a 3.0% increase in hedonic hunger risk. These findings highlight the need to integrate stress reduction, mindful eating, and sleep optimisation strategies, especially for shift-working healthcare professionals.
Introduction
Shift work refers to employment during hours outside of normal working schedules, which are typically 9:00 AM–5:00 PM (Reinganum and Thomas, 2025; Saviano et al., 2025). Shift work is prevalent in many industries that operate 24/7, particularly in the healthcare sector. Although hospitals provide continuous 24-hour services, healthcare professionals do not work continuous 24-hour stretches; instead, they typically work extended shifts that exceed the standard 8–9-hour workday (Reinganum and Thomas, 2025; Roque et al., 2025). Remaining awake for extended periods beyond normal working hours can negatively affect the circadian rhythm, sleep quality, nutritional status, diet quality, and mindful eating (Imes et al., 2023; Kulak and Yeşil, 2022; Nea et al., 2015; Souza et al., 2019). Furthermore, this work schedule can increase occupational stress and anxiety among healthcare workers (Al-Khafajy et al., 2022; Ljevak et al., 2020). This burden is often exacerbated by additional post-shift responsibilities such as household duties and caregiving (Cohen and Ventre, 2020; Vitale et al., 2015). Such stress and anxiety negatively affect eating behaviours (Roskoden et al., 2017; Souza et al., 2019). Additionally, shift work disrupts daily routines, including sleep patterns, dietary habits, and lifestyle, potentially leading to various health problems (Imes et al., 2023; Robinson et al., 2025; Roskoden et al., 2017). Moreover, shift work has been associated with an increased risk of diet-related non-communicable diseases such as obesity and metabolic disorders; individuals working in shifts are at greater risk than those in non-shift conditions (Peplonska et al., 2015; Robinson et al., 2025; Vimalananda et al., 2015).
Similar to other consumers, shift workers can consume food even if they do not experience physiological hunger. The urge or desire to consume food for pleasure in the absence of a real energy need is termed hedonic hunger (Lowe and Butryn, 2007). Hedonic food consumption is characterised by eating in response to emotional states rather than physiological hunger. This can result in eating beyond nutritional needs, such as consuming appetising —but often unhealthy —foods for enjoyment, self-motivation, or as part of reward-punishment patterns (Lowe and Butryn, 2007). The tendency towards hedonic eating involves an increase in food intake driven by the pleasure evoked by food. The majority of foods consumed during hedonic hunger episodes are characterised by high levels of salt, sugar, fat, and energy, and are often less healthy or of poor diet quality. These dietary patterns have demonstrated strong associations with obesity-related chronic diseases, thereby stimulating growing research interest in hedonic hunger. Although hedonic hunger has been linked to various health-related outcomes, the underlying factors that influence its emergence remain insufficiently explored (Alonso-Alonso et al., 2015; Lee and Dixon, 2017; Lowe et al., 2016).
The demanding nature of shift work frequently exposes employees to elevated stress levels, which may contribute to more frequent episodes of mindless eating. The inconsistency of meal times and the limited time available for eating during shift work can also make mindless eating a habit for these people (Choi and Lee, 2020). Changes in dietary habits due to the stress of shift work affect the quality of workers’ diets. Evidence suggests that individuals working night shifts tend to have poorer overall diet quality and face a higher risk of nutritional deficiencies compared to their non-shift counterparts with more sedentary daily routines (Hakim et al., 2016; Hornzee et al., 2021; Nea et al., 2015; Strzemecka et al., 2014).
Previous studies have demonstrated that hedonic hunger is negatively associated with sleep quality, indicating that individuals with higher hedonic tendencies tend to experience poorer sleep quality (Abdulla et al., 2023; Açik et al., 2021). Disturbed sleep patterns are a frequently observed outcome among shift workers, especially those on night schedules, due to the misalignment of circadian rhythm–regulated physiological processes (Rahim et al., 2021). In one investigation, night shift employees reported significantly lower sleep quality, along with increased sleep latency, reduced sleep duration, greater sleep disruptions, and impaired daytime functioning (Lim et al., 2018).
Among shift workers, sleep quality tends to decline and is often accompanied by elevated levels of job-related stress (Bhatti et al., 2017; Truong et al., 2016). Shift work itself is known to be a significant occupational stressor (Farrokhi et al., 2017). Studies have shown that occupational stress is more prevalent in shift workers, particularly in the health care sector (Dodia and Parashar, 2020; Farrokhi et al., 2017; Lin et al., 2015). While stress is widely acknowledged as a key driver of unhealthy dietary patterns, research on the impact of work-related stress on dietary behaviour is insufficient (O’Connor et al., 2008; Vasiļjeva et al., 2023).
Although several studies have linked shift work to metabolic outcomes, the interplay between hedonic hunger, mindful eating, and occupational stress remains under-explored in the healthcare context. This study fills this gap in the literature by simultaneously examining these behavioural and psychological drivers. Understanding these associations is vital for the occupational health of healthcare professionals, as their well-being directly impacts both their long-term health and the quality of care they provide. Thus, this research aims to explore the associations between hedonic hunger and health-related behaviours—including diet quality, mindful eating, sleep quality, and occupational stress—among shift and non-shift hospital employees.
Methods
Study setting, period, and participants
This descriptive cross-sectional study was carried out at a district hospital in Denizli, Türkiye, between March and June 2023. As the total number of night shift staff was limited to 148 individuals, the sample size was calculated based on this subgroup. Using a 5% margin of error and a 95% confidence level, the required sample size was determined to be 107 shift workers through a standard sample size estimation method. The study was carried out on a total of 220 hospital employees, including 110 night shifts workers and 110 employees who worked regular daytime schedules (typically 8:30 AM–5:30 PM). Participants were recruited on a voluntary basis.
Data collection
The study included 220 hospital staff (110 shift and 110 non-shift staff) who were >18 years of age, did not have an eating disorder or alcohol dependence, had not undergone bariatric surgery, did not have diseases that interfere with nutrient absorption, and were not taking psychiatric medications that could affect appetite status. Data for the study were collected using a structured questionnaire including questions on sociodemographic characteristics, health status, eating habits, hedonic hunger, mindful eating, sleep quality, and occupational stress levels, administered via face-to-face interviews. In addition, the food consumption of the subjects was recorded for 3 days (2 weekdays and 1 weekend), and body weight and height were assessed by trained investigator following standard anthropometric protocols. The body mass index (BMI) of each participant was derived using the standard formula (weight (kg)/height (m2)) and categorised in accordance with World Health Organisation (WHO) guidelines (WHO, 2025).
Power of Food Scale (PFS): Hedonic hunger was assessed using the PFS, originally developed by Lowe et al. (2009; Cronbach’s alpha = 0.91). It was later adapted into Turkish and validated in a Turkish adult population by Ulker et al. (2021; Cronbach’s alpha = 0.922). The five-point Likert scale, which consists of 13 items in Turkish, includes three subscales: “food available,” “food present” and “food tasted.” As the score obtained from the scale increases, so does hedonic hunger (Ulker et al., 2021). In the present study, the Cronbach’s alpha coefficient for the total scale was 0.891, with total scores ranging from 1.38 to 5.00. Participants were classified as having low (⩽2.77) or high (>2.77) hedonic hunger based on the median score.
Mindful Eating Questionnaire (MEQ-30): Mindful eating levels were evaluated using the MEQ, originally developed by Framson et al. (2009; Cronbach’s alpha = 0.64) , which was adapted and validated for Turkish use by Köse et al. (2016; Cronbach’s alpha = 0.733). The scale employs a five-point Likert format and consists of seven subscales: “disinhibition, emotional eating, control of eating, awareness, eating discipline, mindfulness, and interference.” Higher scores indicate greater mindfulness in eating behaviours (Köse et al., 2016). In the present study, the Cronbach’s alpha coefficient for the total scale was 0.696, with scores ranging from 1.93 to 4.33. Based on the median score distribution, participants classified as having low (⩽3.10) or high (>3.10) mindful eating.
Diet Quality Index-International (DQI-I): Diet quality was assessed using the DQI-I, calculated from the participants’ 3-day food diaries. Dietary records were analysed using the Nutrition Information System (BeBIS, version 8.2) and nutrient and energy data were entered by a licenced dietitian. According to Kim et al. (2003), scores <60 indicate “poor diet quality,” whereas scores ⩾60 indicate “good diet quality.” The DQI-I consist of four subscales—variety (0–20), adequacy (0–40), moderation (0–30), and overall balance (0–10)—with a total possible score of 100 (Kim et al., 2003).
Pittsburgh Sleep Quality Index (PSQI): Sleep quality was assessed using the PSQI, originally developed by Buysse et al. (1989; Cronbach’s alpha = 0.83) and adapted into Turkish by Ağargün et al. (1996; Cronbach’s alpha = 0.80). The instrument consists of 24 items and seven subscales: —subjective sleep quality, sleep latency, sleep duration, habitual sleep efficiency, sleep disturbances, use of sleep medication, and daytime dysfunction—with total scores ⩽5 indicating good and >5 indicating poor sleep quality (Ağargün et al., 1996). In the present study, Cronbach’s alpha coefficient for the total scale was 0.61. This is considered an acceptable for multidimensional indices with heterogeneous components such as medication use and sleep duration.
A Job Stress Scale-20 (JSS-20): Occupational stress was assessed using the JSS-20, developed by Tatar (2020; Cronbach’s alpha = 0.91) and consisting of a single dimension and 20 items. Higher scores on the scale reflect elevated levels of job-related stress (Tatar, 2020). In the present study, the Cronbach’s alpha coefficient for the scale was found to be 0.911, with total job stress scores ranging from 20 to 100. Participants were classified into low (⩽47.00) and high (>47.00) job stress groups based on the median cutoff value.
Statistical analysis
All statistical analyses were performed using SPSS software, version 26.0. Categorical variables were summarised as frequencies (n) and percentages (%), and comparisons between groups were made using the chi-square test. Quantitative variables obtained by measurement are presented as the median and inter quartile range (IQR). The Kolmogorov–Smirnov test was employed to assess the normality of continuous variables. Mann–Whitney U test was applied for non-normally distributed variables. Correlational relationships were examined using Spearman’s rank-order correlation. Binary logistic regression was performed after checking the assumptions of the model. A p-value less than 0.05 was considered statistically significant across all analyses. The evaluation of food consumption records to calculate the diet quality index score was performed via the Nutrition Information System (BeBIS).
Results
Table 1 presents the distribution of participants’ sociodemographic characteristics by work schedule. Of the total sample, 59.5% were female and 40.5% were male and the majority of shift (58.2%) and non-shift workers (60.9%) were female (p = 0.680). The overall median age was 36.00 years (IQR: 10.00), and age did not significantly differ between shift and non-shift healthcare professionals (median: 35.00, IQR: 8.25 and 38.00, IQR: 13.25 years, respectively; p = 0.176). There was no statistically significant difference in educational status between shift and non-shift healthcare professionals (p = 0.140). However, non-shift workers were more likely to hold bachelor’s or postgraduate degrees, while shift workers were predominantly educated at the high school level. The proportion of nurses, as well as security and cleaning personnel, was significantly higher among shift workers compared to non-shift workers. In contrast, medical secretaries, psychologists, pharmacists, and physiotherapists, as well as health technicians were more frequently employed in non-shift positions than in shift-based roles within the same professional categories (p < 0.001). A total of 57.3% of shift and 67.3% of non-shift healthcare professionals had no chronic diseases (p = 0.126). While the difference was not statistically significant, the prevalence of smoking was higher among shift workers compared to their non-shift counterparts (p = 0.862). Low alcohol consumption, on the other hand, was comparable between the two groups (p = 0.884). Comparison of BMI values between shift and non-shift workers revealed no statistically significant difference (p > 0.05). More than half of the shift workers (52.7%) and nearly half of the non-shift workers (45.5%) were pre-obese (p > 0.05).
Sociodemographic characteristics of participants by work schedule.
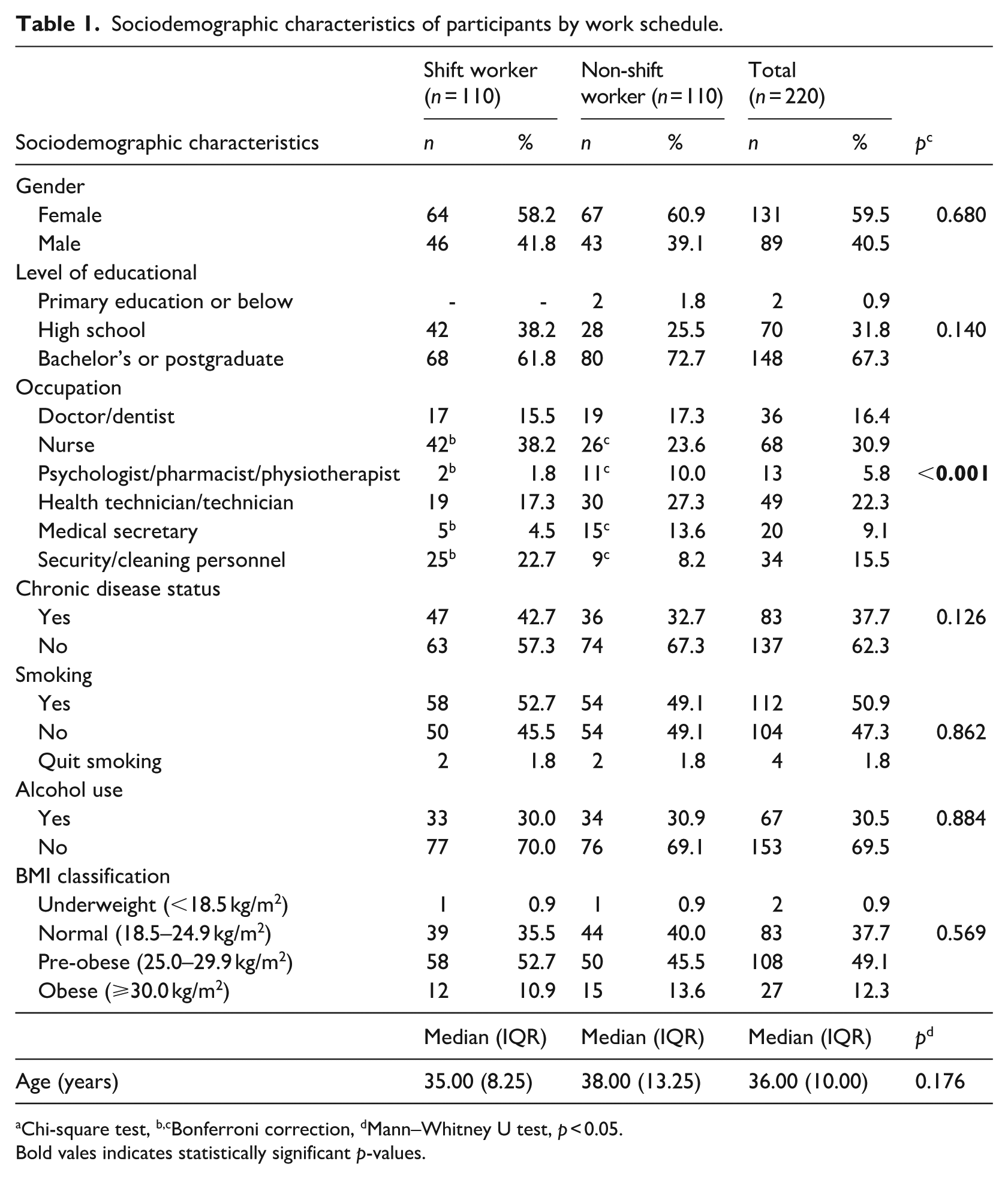
aChi-square test, b,cBonferroni correction, dMann–Whitney U test, p < 0.05.
Bold vales indicates statistically significant p-values.
A greater proportion of both shift and non-shift workers reported consuming three main meals per day (73.6% and 62.7%, respectively; p = 0.082), according to Table 2. However, breakfast skipping was significantly more common among shift healthcare professionals compared to non-shift (p = 0.049). Although skipping lunch was less frequent overall, it was still more common among non-shift compared with shift workers (Table 2).
General dietary habits by work schedule.
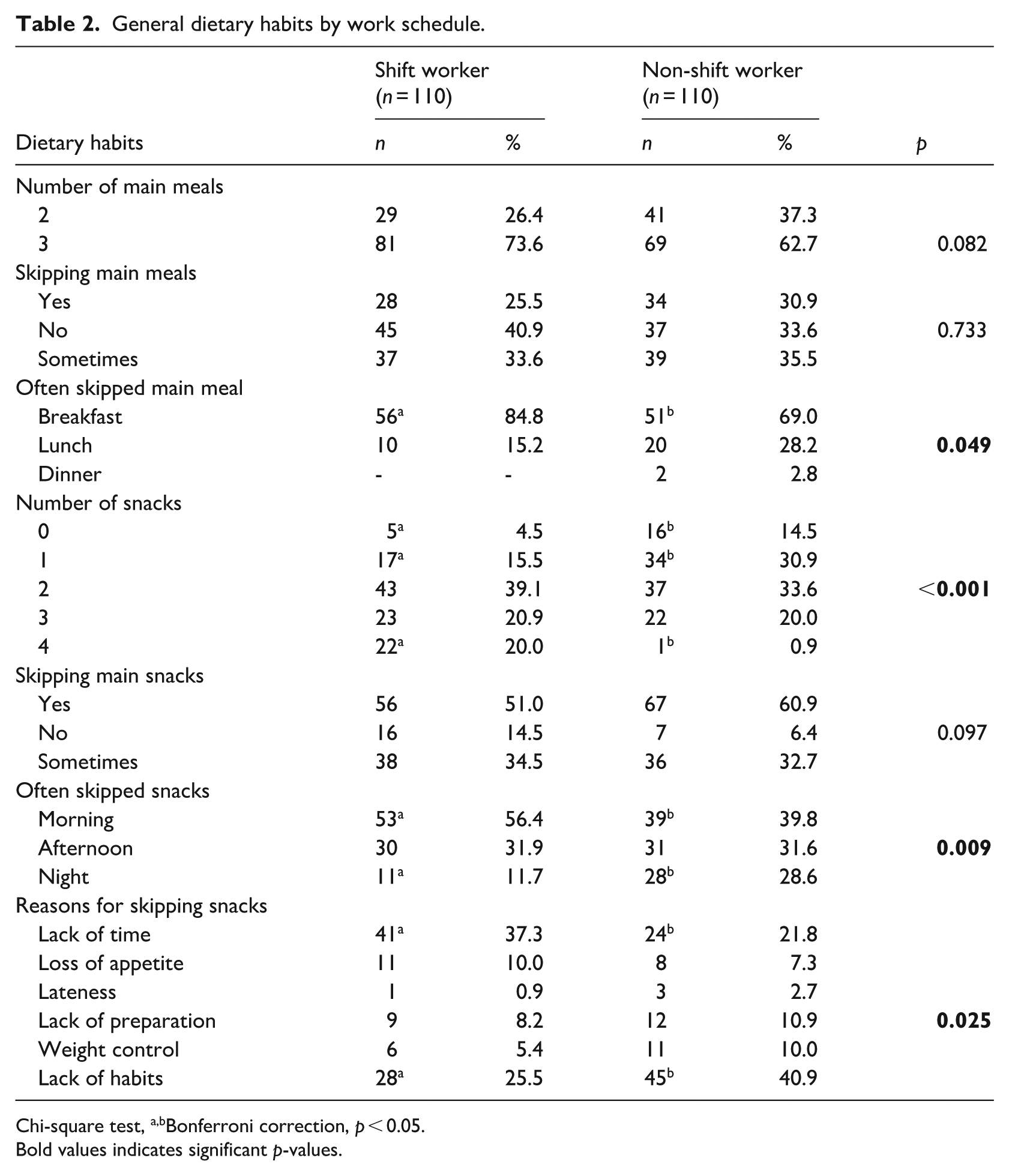
Chi-square test,a,bBonferroni correction, p < 0.05.
Bold values indicates significant p-values.
The number of workers who had no snacks or only one snack was significantly greater among workers with standard daytime schedules than among shift workers. Additionally, the frequency of consuming four snacks per day was significantly higher among shift workers (p < 0.001). Shift workers frequently skipped the mid-morning snack, whereas non-shift workers frequently skipped the night snack (p = 0.009). When the reasons for skipping snacks were analysed, it was found that shift workers mostly skipped snacks due to a lack of time, whereas non-shift workers skipped snacks because they did not have a habit of snacking (p = 0.025; Table 2).
The participants’ scale scores and the classification of hedonic hunger, mindful eating, sleep quality, diet quality, and occupational stress levels are presented in Tables 3 and 4. The hedonic hunger status of the participants showed that shift workers had significantly higher scores on the PFS (median: 2.85, IQR: 0.77) compared to non-shift workers (median: 2.46, IQR: 1.13; p = 0.013). Similarly, shift workers scored higher on the subscales of food taste (median: 2.80, IQR: 1.15 vs median: 2.40, IQR: 1.35; p = 0.028) and food availability (median: 2.75, IQR: 0.75 vs median: 2.50, IQR: 1.00; p = 0.001). Although shift workers showed a higher prevalence of high hedonic hunger compared to non-shift workers, the difference was not statistically significant (p = 0.177).
Comparison of scale scores by work schedule.
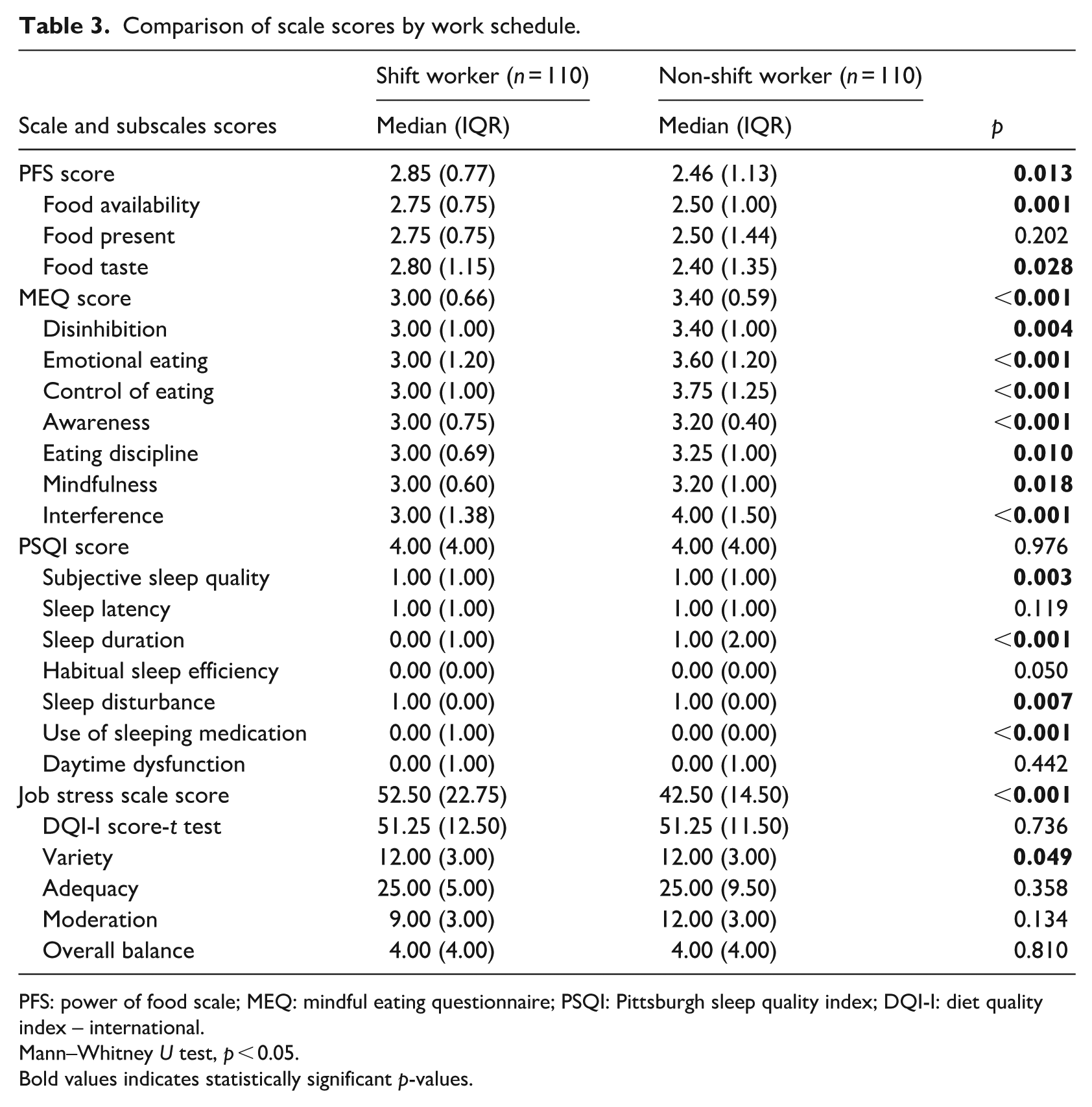
PFS: power of food scale; MEQ: mindful eating questionnaire; PSQI: Pittsburgh sleep quality index; DQI-I: diet quality index – international.
Mann–Whitney U test, p < 0.05.
Bold values indicates statistically significant p-values.
Classification of participants by hedonic hunger, mindful eating, sleep quality, occupational stress, and diet quality scale scores.
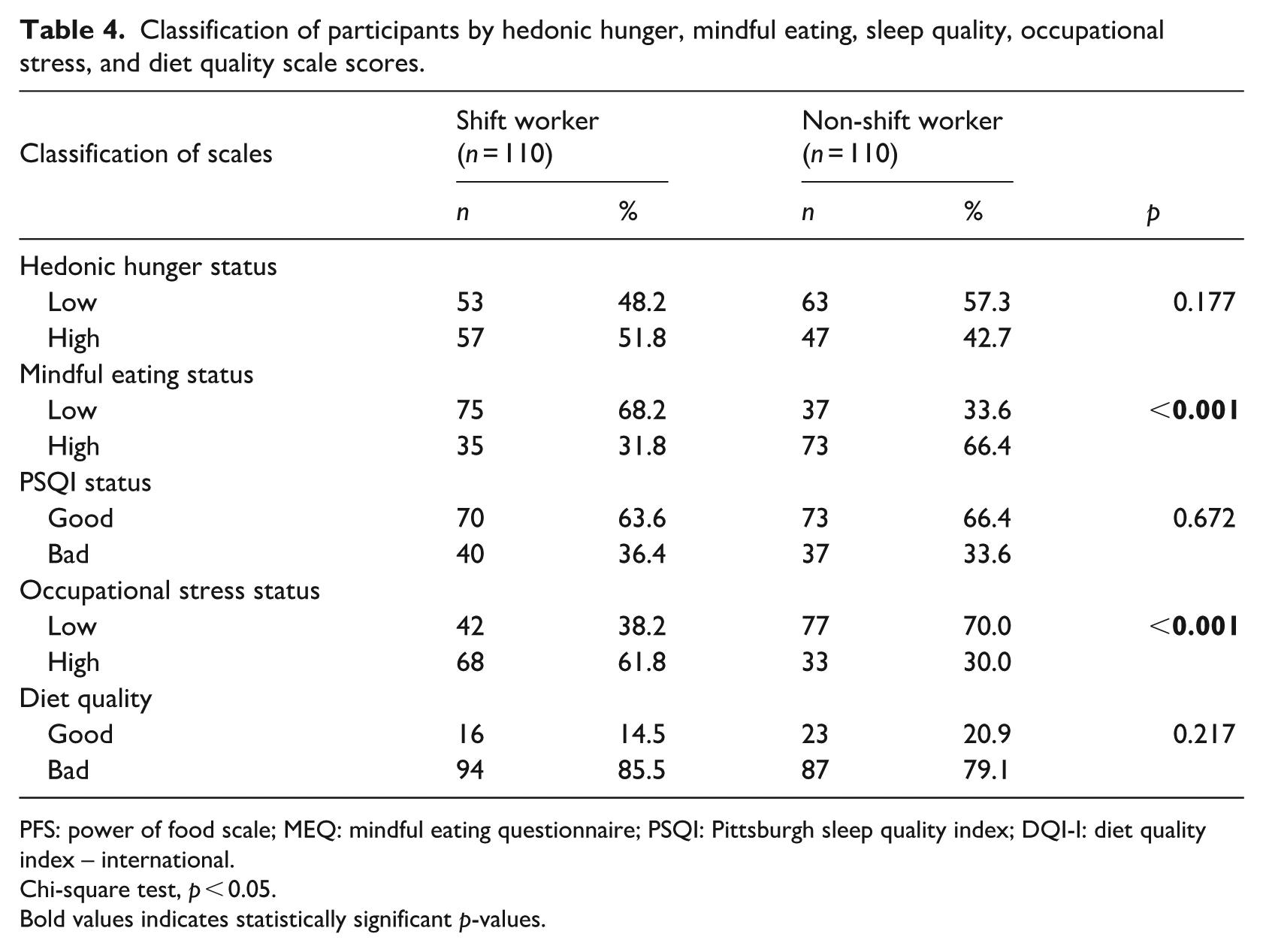
PFS: power of food scale; MEQ: mindful eating questionnaire; PSQI: Pittsburgh sleep quality index; DQI-I: diet quality index – international.
Chi-square test, p < 0.05.
Bold values indicates statistically significant p-values.
Mindful eating score was significantly higher among non-shift (median: 3.40, IQR: 0.59) compared to shift workers (median: 3.00, IQR: 0.66; p < 0.001), with a significantly greater proportion of shift workers exhibiting low mindful eating levels compared to non-shift workers (68.2% vs 33.2%, respectively; p < 0.001). Scores on the MEQ subscales—including disinhibition (p = 0.004), emotional eating (p < 0.001), control of eating (p < 0.001), awareness (p < 0.001), eating discipline (p = 0.010), mindfulness (p = 0.018), and interference (p < 0.001)—were all significantly higher among participants with regular daytime work schedules compared to those engaged in shift-based roles (Tables 3 and 4).
Evaluation of sleep quality revealed no statistically significant difference in PSQI scores between shift-based and non-shift-based employees (p = 0.976). Overall, the majority of participants had relatively good sleep quality (63.6% and 66.4%, respectively). An assessment of the sleep quality subscales revealed that subjective sleep quality was worse (p = 0.003), and that sleep disturbance was greater (p = 0.007) in shift workers, whereas the use of sleeping medications (p < 0.001) and sleep duration (p < 0.001) were greater in non-shift workers (Tables 3 and 4).
The occupational stress levels of the participants, based on their working patterns, indicated that shift workers reported significantly higher job stress scores (median: 52.50, IQR: 22.75) compared to non-shift workers (median: 42.50, IQR: 14.50; p < 0.001). In addition, a higher proportion of shift-based employees experienced elevated levels of job stress compared to those with non-shift (61.8% and 30.0%, respectively; p < 0.001). Assessment of diet quality indicated that a substantial proportion of both shift workers (85.5%) and non-shift workers (79.1%) exhibited poor diet quality. No statistically significant differences were observed between the two groups in total diet quality scores (p > 0.05; Tables 3 and 4).
The relationships between the hedonic hunger states of the subjects and their mindful eating, sleep quality, job stress and diet quality are shown in Table 5. No significant relationships were found between hedonic hunger and mindful eating or diet quality (p > 0.05). However, a moderate positive relationship was observed between hedonic hunger and sleep quality (i.e. worse sleep quality), as well as between hedonic hunger and job stress (r = 0.335, p < 0.001; r = 0.333, p < 0.001, respectively). In addition, a weak negative correlation was found between mindful eating and sleep quality (i.e. worse sleep quality; r = −0.142; p = 0.036) and between mindful eating and job stress (r = −0.163; p = 0.016). Moreover, a significant positive correlation was observed between sleep quality (i.e. worse sleep quality) and job stress (r = 0.304; p < 0.001).
Relationships between hedonic hunger and mindful eating, sleep quality, job stress, and diet quality.
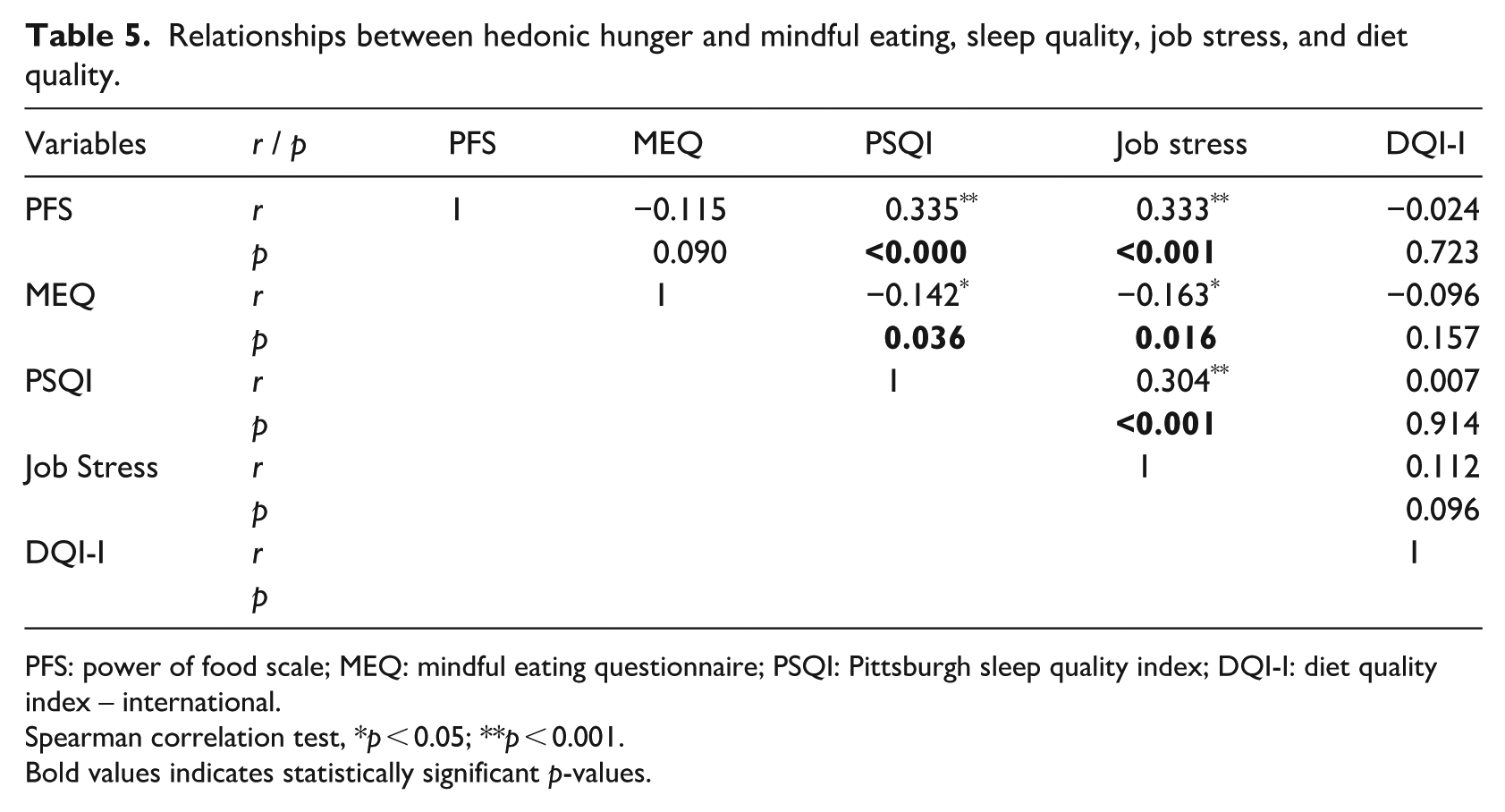
PFS: power of food scale; MEQ: mindful eating questionnaire; PSQI: Pittsburgh sleep quality index; DQI-I: diet quality index – international.
Spearman correlation test, *p < 0.05; **p < 0.001.
Bold values indicates statistically significant p-values.
A regression model was constructed and tested to assess the relationships between hedonic hunger and diet quality, mindful eating, sleep quality, and job stress in shift-based and non-shift-based employees (Table 6). In the unadjusted model, hedonic hunger was not associated with employment status, DQI-I score, or MEQ score. However, elevated PSQI scores—reflecting poorer sleep quality—were positively related to higher levels of hedonic hunger (p = 0.001, OR = 1.278). A significant association was found between elevated hedonic hunger and job stress (p = 0.010, OR = 1.031). Shift work status, diet quality, and mindful eating were not significant predictors in Model 1 (adjusted for gender and age). However, in Model 1, elevated PSQI scores—indicating poorer sleep quality—were found to be a predictor of increased hedonic hunger risk (Model 1: p = 0.001, OR = 1.247). Higher job stress was also found to increase the risk of greater hedonic hunger in Model 1 (p = 0.013, OR = 1.030).
Effects of hedonic hunger on diet quality, mindful eating, sleep quality and job stress by work schedules.
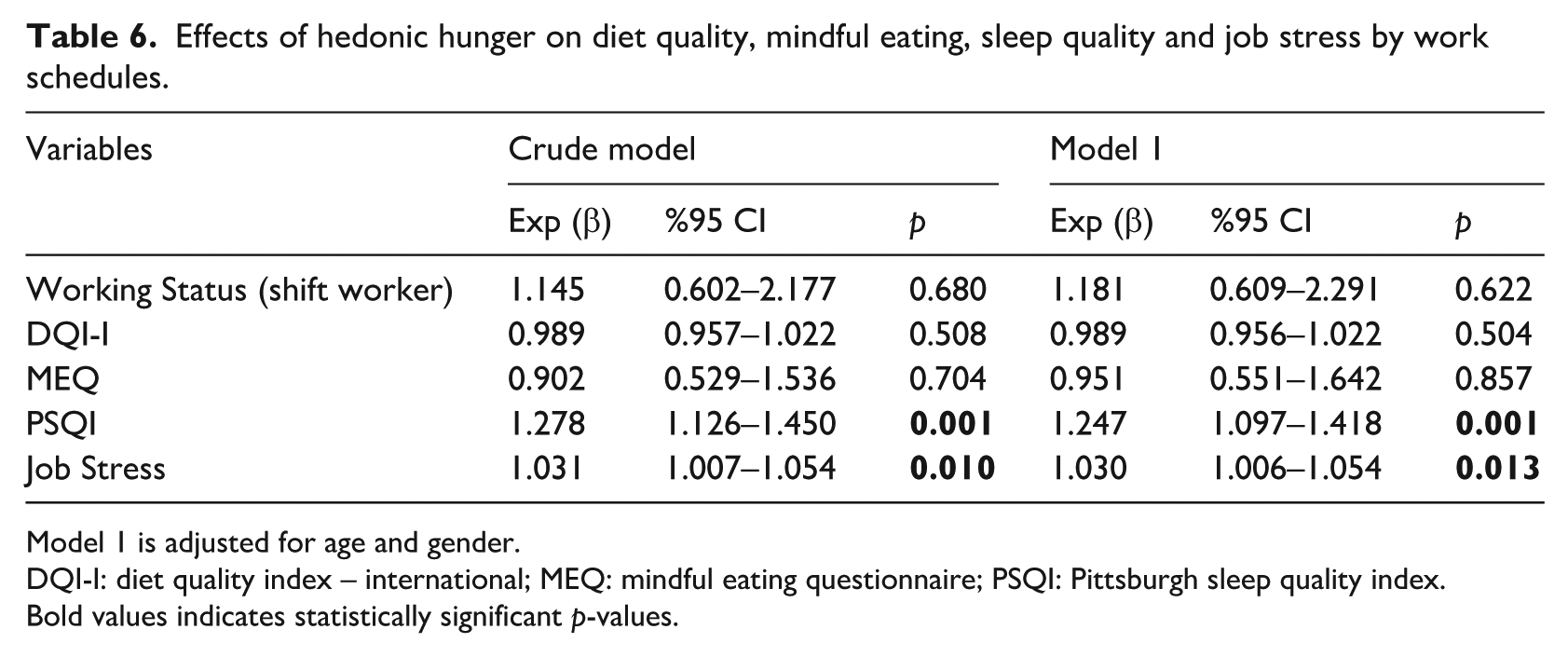
Model 1 is adjusted for age and gender.
DQI-I: diet quality index – international; MEQ: mindful eating questionnaire; PSQI: Pittsburgh sleep quality index.
Bold values indicates statistically significant p-values.
Discussion
Work schedules outside normal working hours are generally referred to as shift work (Wu et al., 2022). The International Labour Organisation has reported that approximately 20% of the world’s workforce works in shift-based schedules (Maul, 2020). As in many other countries, a large proportion of shift workers in Türkiye is healthcare professionals who provide services around the clock (Aleksynska et al., 2019). In line with the findings of the present study, unfavourable lifestyle changes associated with shift work primarily manifest as disruptions in sleep quality, increased occupational stress, and poorer diet quality, which may contribute to maladaptive eating behaviours (Nea et al., 2015; Rajaratnam et al., 2013).
As observed in this study, prior evidence suggests that shift work in the healthcare field is largely carried out by nurses (38.2%), most of whom are women (60.5%; Cheng et al., 2021; McElroy et al., 2020). In the present sample, participants generally reported low alcohol consumption and a relatively low prevalence of chronic disease. However, a considerable proportion were classified as pre-obese. This suggests that adverse health outcomes among shift-working healthcare professionals may be influenced by factors beyond traditional lifestyle risk behaviours. Previous research indicates that circadian disruption associated with shift work can lead to homeostatic imbalance, encouraging excessive food intake, increasing hedonic hunger, and disrupting sleep patterns, which may in turn elevate the risk of pre-obesity, as also observed in this study (shift 52.7% vs non-shift workers 45.5%; McHill et al., 2014; Shechter et al., 2014; Vidafar et al., 2020). Additionally, despite relatively high levels of education, mindful eating scores were low. This suggests that nutritional knowledge alone may not lead to healthier eating habits when working shifts that are demanding.
Dietary habits are among the lifestyle factors that are most affected by shift work. Changes in infrequent consumption (skipping) of main meals and excessive snacking may occur depending on shift schedules. A study among nurses reported that night shift workers consume fewer main meals and more snacks (Sahu and Dey, 2011). Another study suggested that night shift workers eat more irregularly, skip breakfast more often, snack more at night and have a poorer habit of eating three meals a day (Han et al., 2016). Similarly, this study showed that hospital staff working night shifts skipped breakfast more often (p = 0.049), had fewer snacks (p < 0.001), mostly skipped the mid-morning snack (p = 0.009), and non-shift workers skipped the evening snack (p = 0.009; Table 2).
Research investigating the impact of hedonic hunger on shift workers is limited. In a study conducted in Türkiye, hedonic hunger was found in 53.85% of shift workers and was higher among those with longer shift hours, which are generally associated with shift work (Sever and Özdoğan, 2024). In another study, hedonic hunger levels did not differ significantly between shift-based and non-shift-based employees (p > 0.05; Özpak Akkuş and Mermer, 2022). This study showed increased hedonic hunger in 51.8% of shift workers; however, in contrast to the literature, the total scores of the PFS (p = 0.013), food available (p = 0.001) and food tasting (p = 0.028) scores were significantly higher in shift-based than in non-shift-based employees. This may be due to the differences in the occupational groups participating in the study.
Shift work not only triggers hedonic hunger but also influences individuals’ dietary habits and diet quality. Shift work, owing to its demanding nature, leads to inconsistent eating times, shorter mealtimes and, consequently, a shift towards fast and mindless eating (Choi and Lee, 2020). A few studies evaluated mindful eating among shift workers. One study involving shift workers who were not healthcare professionals reported that mindful eating was significantly worse among shift workers (p = 0.049; Demirezen et al., 2023). A study conducted among healthcare professionals indicated that night shift workers, compared to their daytime counterparts, had elevated total scores in mindful eating (p = 0.000), along with higher scores in all subgroups except for mindfulness (p < 0.05). Night shift workers were found to have higher levels of mindful eating than day shift workers (Hamurcu and Taş, 2022). In this study, as expected, MEQ (p < 0.001) and all subscales’ scores were significantly lower in shift-based employees than in non-shift-based (p < 0.05).
Both hedonic hunger and mindful eating are key factors affecting diet quality among shift-based and non-shift-based healthcare professionals. Existing research presents inconsistent findings regarding the diet quality of employees working standard versus shift-based schedules. Some research report that shifts work does not affect diet quality (Beebe et al., 2017; Hulsegge et al., 2016), whereas other studies propose that it decreases diet quality (Hakim et al., 2016; Nea et al., 2015; Yoshizaki et al., 2016). A study showed that the diet quality of shift workers was significantly lower (p < 0.001) and that it was particularly higher in those working night shifts (Hornzee et al., 2021). Consistent with previous studies, the present study found that shift work did not significantly affect diet quality (p > 0.05), and that the majority of participants in both groups (85.5% and 79.1%) had poor diet quality (Beebe et al., 2017; Hulsegge et al., 2016).
Sleep quality disturbances are frequently observed among shift-based work, particularly those working night shifts. This is associated with the disturbance of physiological processes governed by the circadian rhythm (Rahim et al., 2021). Many studies have reported poor sleep quality among shift workers. An Asian study reported that sleep quality disturbance was 198% higher among shift workers than among those with standard working hours (OR = 2.98; 95% CI: 1.53–5.81; Thach et al., 2020). Another study revealed that individuals working night shifts had significantly lower sleep quality (6.3 ± 2.6 and 4.8 ± 2.8, respectively; p < 0.001), with prolonged sleep latency, reduced sleep duration, more frequent sleep disturbances, and increased levels of daytime dysfunction compared to those on regular work schedules (p < 0.05; Lim et al., 2018). In a study conducted with female hospital employees, weak correlations were identified linking shift schedules to sleep quality, efficiency, and latency (Lajoie et al., 2015). In this study, contrary to the literature, most shift workers (63.6%) had good sleep quality, and there was no difference in this respect them and non-shift workers (p = 0.976). This may be explained by the fact that the research site is a small district hospital with a low number of inpatients, allowing night shift workers to take turns sleeping during their shifts. Coinciding with the literature, subjective sleep quality (p = 0.003) and sleep disturbances (p = 0.007), which are subscales of sleep quality, were worse among shift workers, whereas sleep duration was longer among non-shift workers (p < 0.001).
Nonstandard work hours are a well-known occupational stress factor, especially for hospital employees. A previous study revealed that 60% of nurses have different levels of occupational stress, ranging from moderate to high (Farrokhi et al., 2017). Another study among nurses found that night shifts increased occupational stress (Lin et al., 2015) and a study in Taiwan similarly suggested that most nurses experienced a moderate level of occupational stress (56.6%; Lin et al., 2014). Dodia and Parashar (2020) reported that night shift workers (145.0 ± 17.2) had higher job stress scores than did day shift workers (127.7 ± 11.8). In line with previous studies, the current findings indicated that shift workers had significantly higher job stress scores (median: 52.50, IQR: 22.75) compared to their non-shift counterparts (median: 42.50, IQR: 14.50; p < 0.001).
There is a lack of empirical evidence examining the association between hedonic hunger and mindful eating, diet quality, sleep quality and occupational stress in shift and non-shift healthcare employees. Studies on hedonic hunger in shift workers have generally focussed on sleep quality (Özpak Akkuş and Mermer, 2022; Vidafar et al., 2020). A study reported a positive association between poor sleep quality and food cravings among shift-based employees (r = 0.26; p = 0.04; Vidafar et al., 2020). Similarly, this study suggested a moderate positive relationship between hedonic hunger and impaired sleep quality (r = 0.335; p < 0.001). It has been reported that increased ghrelin due to disrupted circadian rhythms in shift workers may increase hedonic hunger (Hanlon et al., 2016; Özpak Akkuş and Mermer, 2022). Considering the correlation between hedonic hunger and mindful eating, it is evident that mindful eating is poor in those with high hedonic hunger. Moreover, hedonic hunger and mindless eating negatively affect dietary habits and consequently diet quality (Paolassini-Guesnier et al., 2023; Ünal et al., 2025). In this study, no significant relationships were found between hedonic hunger status, mindful eating and diet quality (p > 0.05). The occupational stress caused by shift work negatively affects dietary habits. Joseph et al. (2018) reported a low-level positive relationship between perceived job stress and hunger (r = 0.26; p = 0.008). Likewise, the current study revealed a positive association between job stress levels and increased hedonic hunger (r = 0.333; p < 0.001). Moreover, findings revealed that sleep quality decreased (r = 0.304; p ⩽ 0.001) and mindful eating worsened (r = −0.163; p = 0.016) as job stress increased.
In this study, deterioration in sleep quality and job stress were found to be positively associated with hedonic hunger. Regression analyses revealed that a 1 -unit deterioration in sleep quality increases the odds of high hedonic hunger by 27.8%. Crucially, when the model was adjusted for age and gender (Model 1), this association remained statistically significant, with the odds increasing by 24.7% (Table 6). Adjusting for demographic confounders reinforces the technical validity of our findings, suggesting that sleep quality’s impact on hedonic appetite is independent of participants’ age or gender. Moreover, each unit increase in job stress was found to increase the likelihood of high hedonic hunger by 3.0%.
Conclusion
This study analyses the relationships between hedonic hunger, diet quality, mindful eating, sleep quality, and occupational stress among healthcare professionals working in shifts and those with regular schedules. The findings indicate that shift-based workers have significantly higher hedonic hunger scores (p = 0.013), demonstrate lower levels of mindful eating (p < 0.001), experience poorer sleep quality and greater job stress (p < 0.001). Additionally, low levels of mindful eating and unhealthy food consumption patterns and preferences negatively impact on diet quality. Furthermore, regression analysis showed that poor sleep quality increased the likelihood of high hedonic hunger by 27.8%, while each unit increase in job stress was associated with a 3.0% increase in this risk.
Although healthcare professionals are responsible for meeting the health-related needs of others, demanding and hectic shift schedules may prevent them from adequately attending to their own dietary and lifestyle needs. It is particularly important for shift workers to establish planned eating habits, manage hedonic hunger and improve mindful eating in order to improve both food quality and overall health. Dietary and lifestyle-related changes among hospital personnel—including eating behaviours, sleep patterns, and stress levels—resulting from changing shift schedules should be taken into consideration to promote healthy food choices. Moreover, individual and institutional strategies should be developed to encourage improved sleep patterns and reduce occupational stress. Improving the diet and sleep quality of shift-working healthcare professionals, and reducing their occupational stress, may also contribute to improved work performance, given their critical role in public healthcare services. Finally, the results of this study may encourage improved evaluation of these relationships in future studies with larger sample sizes and in different groups of healthcare professionals.
Limitations and strengths
Limitations of this research include its cross-sectional design and conducted in a small district hospital. In addition, the shift cycles and duration of exposure to shift work among healthcare employees were not evaluated. Diet quality was also assessed based on a 3-day food diary, which may not fully reflect habitual dietary intake.
A key strength of this study is that although separate studies have been conducted in Türkiye to assess diet quality, occupational stress or sleep quality depending on work schedule type (shift vs non-shift) in the healthcare sector, this is the first study to analyse all the parameters together in the sample.
Footnotes
Acknowledgements
We would like to thank all healthcare professionals who agreed to participate in our study.
Ethical considerations
This study was approved by the Clinical Research Ethics Committee of Akdeniz University (Approval No: KAEK-219) on March 8, 2023. All participants provided written informed consent prior to enrolment in the study. This research was conducted ethically in accordance with the World Medical Association Declaration of Helsinki.
Consent to participate
Written informed consent was obtained from all participants prior to data collection.
Consent to publication
Consent for publication is not applicable to this article as it does not contain any identifiable data.
Author contributions
SA: Conceptualisation, Methodology, Data Collection, Analysis, Writing – original draft, Visualisation. HKA: Conceptualisation, Methodology, Analysis, Writing – review & editing, Visualisation, Supervision. All authors: approved the final version of the manuscript.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.