
Abstract
Diverse adaptive and maladaptive eating behaviours exist, yet research is needed to understand their inter-relationships. This study investigated the factor structure underlying a broad spectrum of eating attitudes and behaviours, and their associations with wellbeing outcomes and clinical impairment. Two samples of women (Mage = 24 years; n1 = 400, n2 = 423) completed a survey measuring intuitive eating, mindful eating, disinhibited eating, dietary restraint and restriction, and orthorexia tendencies. Exploratory factor analysis in Sample 1 suggested a five-factor structure, which was supported by confirmatory factor analysis in Sample 2. Results demonstrated one adaptive factor, characterised by Body-Centric Eating; three maladaptive factors, characterised by Dietary Restraint, Disinhibited Eating, and Severe Restriction; and Mechanical Eating, characterised by adherence to routine-based eating. Identifying how adaptive and maladaptive eating behaviours cluster empirically provides insight into the potential role of adaptive eating strategies in reducing maladaptive eating and enhancing wellbeing.
Introduction
Eating behaviours are multifaceted, including both maladaptive and adaptive patterns. Maladaptive eating, such as dietary restraint and disinhibited eating, is marked by rigidity and disconnection from physical or nutritional needs, and is a well-established risk factor for eating disorders (Harrer et al., 2020). While research has largely focussed on reducing these behaviours, adaptive eating approaches, such as intuitive and mindful eating, promote a flexible, attuned response to bodily signals (Augustus-Horvath and Tylka, 2011; Mantzios, 2021). These approaches have more recently emerged as promising targets in eating disorder treatment (Kristeller et al., 2014; Richards et al., 2017). Despite the potential use of adaptive eating strategies within eating disorder treatment (Kristeller et al., 2014; Richards et al., 2017), adaptive eating has typically been conceptualised independently from maladaptive eating (Belon et al., 2022). It therefore remains unclear which aspects of adaptive eating drive reductions in which aspects of maladaptive eating, and vice versa. As such, it is imperative to examine the degree to which adaptive and maladaptive eating behaviours are distinct or overlap, as how they cluster empirically can guide prevention and interventions for eating disorders, and the promotion of wellbeing.
Intuitive and mindful eating as adaptive eating styles
Intuitive and mindful eating styles are recognised as two dominant forms of adaptive eating (Mantzios, 2021; Tylka et al., 2024). The most widely accepted model of intuitive eating suggests it comprises four underlying dimensions including unconditional permission to eat (UPE; an individual’s willingness to eat what they desire and avoid labelling foods as “good” or “bad”), eating for physical rather than emotional reasons (EPR; the capacity to self-soothe using coping strategies that do not involve food), reliance on hunger and satiety cues (RHSC; an individual’s trust in bodily signals to guide how, when, and how much to eat), and body-food choice congruence (BFCC; the tendency to choose foods that nourish the body; Tylka et al., 2024). Despite the absence of a uniform definition, mindful eating has been conceptualised as consisting of two core components: present-moment awareness whilst eating and having a non-judgemental approach to eating choices (Mantzios, 2021).
Supporting their conceptualisation as forms of adaptive eating, both intuitive and mindful eating demonstrate strong positive relationships with psychological health, including higher levels of self-esteem, optimism, social support, problem-solving, body appreciation, and self-compassion in women (Linardon et al., 2021; Shaw and Cassidy, 2022).
While also relevant for men (Linardon et al., 2021), most research on intuitive eating has focussed on women, illustrating how gendered processes both shape and are shaped by adaptive eating behaviours (Augustus-Horvath and Tylka, 2011). Both intuitive and mindful eating are recognised as adaptive regulation strategies that help women respond to eating disorder risk factors. For example, research has demonstrated that mindful eating moderates the relationship between emotion dysregulation and disinhibited eating (Czepczor-Bernat et al., 2020), and intuitive eating mediates the effects of negative affect on eating disorder symptoms (Cardoso et al., 2020). As such, intuitive and mindful eating have received attention as possible targets in the prevention and/or treatment of eating disorders in women.
Empirical issues in adaptive eating styles
Existing measures of intuitive and mindful eating reveal conceptual variations within the constructs themselves, alongside ongoing debate about how they relate to each-other (Hulbert-Williams et al., 2014; Tylka and Kroon Van Diest, 2013; Winkens et al., 2018). These issues highlight the need to empirically identify the core components of adaptive eating utlising an integrated approach that is not limited to investigating the constructs in isolation. Intuitive eating has been most robustly operationalised via the Intuitive Eating Scale-2 which enables calculation of a total intuitive eating score and four subscale scores representing each of its components (IES-2; Tylka and Kroon Van Diest, 2013). Despite extensive use, critiques of the super-ordinate structure of intuitive eating have emerged (Martin-Wagar and Heppner, 2023; Román et al., 2021). Adaptations of the IES-2 in cross-cultural and clinical samples found support for the four-factor model, however failed to replicate the higher-order structure (Román et al., 2021), or found variability in item functioning (Martin-Wagar and Heppner, 2023), prompting recommendations for use of subscale rather than total scores in research. Additionally, how the subscales relate to each other has challenged a higher-order model, as the UPE and BFCC subscales are shown to negatively correlate with one another (Linardon et al., 2021; Román et al., 2021). As a solution to critiques of the super-ordinate model, a bifactor model of intuitive eating has been proposed which allows for the four subscales to be represented as distinct from each-other, and distinct from an over-arching intuitive eating construct (Swami et al., 2022). This approach suggests that a total score provides a valid index of intuitive eating, but utilising the four distinct subscales can provide more nuance and elucidate subgroup differences.
The empirical definition of mindful eating has posed challenges as existing measures seek to define it as an eating-specific construct distinct from a manifestation of general mindfulness (Hulbert-Williams et al., 2014). However, the extent to which mindful and intuitive eating delineate is also questioned, with certain facets such as awareness of hunger cues sharing overlap (Winkens et al., 2018). Consequently, it remains unclear how these adaptive eating behaviours cluster conceptually or empirically across constructs. Such inconsistencies underscore the need for a re-examination of the underlying structure of adaptive eating.
Conceptualising adaptive and maladaptive eating together
The conceptualisation of adaptive eating may be better informed by examining how intuitive and mindful eating processes relate to maladaptive eating. Such relationships are also of importance given the potential use of adaptive strategies in the prevention and treatment of disordered eating (Richards et al., 2017). In exploring facets of intuitive eating, Tylka and Wilcox (2006) found that the RHSC and EPR subscales contributed unique variance to wellbeing outcomes beyond that accounted for by maladaptive dieting and food preoccupation. In contrast, UPE did not significantly predict wellbeing once maladaptive eating variables were accounted for (Tylka and Wilcox, 2006). This may be explained via previous research which demonstrates that UPE is strongly inversely associated with dietary restraint (Linardon et al., 2021), and cognitive models which posit that allowing oneself to eat reduces cognitive deprivation and thereby disrupts restrictive–binge cycles (Stice, 2002). Considering their strong associations, when dietary restraint is accounted for, UPE may not explain additional variance as reductions in restraint represent the more proximal factor influencing wellbeing.
While there are numerous correlational studies investigating the relationship between adaptive and maladaptive eating constructs (Linardon et al., 2021), these have yielded mixed results. Some studies demonstrate negative associations with maladaptive eating (Hulbert-Williams et al., 2014; Tylka et al., 2024), whilst others demonstrate no associations when utilising total intuitive or mindful eating scores (Anderson et al., 2016). Discrepancies using total scores suggest a need to investigate eating constructs at a subgroup level as components of intuitive eating are likely to hold differing relationships to maladaptive eating in light of bifactor models highlight the distinctiveness of the subscales (Swami et al., 2022).
The capacity to discern whether facets of adaptive eating are conceptually distinct from maladaptive eating is also limited as existing research has predominantly examined their relationships with dietary restraint as the sole indicator of maladaptive eating (Anderson et al., 2016; Tylka and Wilcox, 2006). Broadening the scope of maladaptive constructs to include forms of disinhibited eating may provide important insights that cannot be captured by restraint measures alone. Disinhibited eating, including binge eating, emotional eating, and external eating, represent distinct types of maladaptive eating (Stice, 2002), and may relate differently to adaptive constructs. For instance, examining these behaviours can clarify the extent to which EPR overlaps with or is distinct from emotional and external eating tendencies.
Including a wider range of maladaptive eating constructs (beyond dietary restraint) may provide a stronger test of which components of intuitive and mindful eating are truly adaptive. While BFCC is suggested to be adaptive due to its non-significant relationships with restrained eating, (Tylka and Kroon Van Diest, 2013), some studies report and positive associations, which presents as a challenge for characterising BFCC as adaptive (Linardon et al., 2021). These discrepancies may partly reflect variation in specific types of dietary restraint. For example, orthorexia nervosa is one form of restraint defined as a maladaptive obsession with healthy eating which leads to restrictive dietary practices (Dunn and Bratman, 2016). Given that both intuitive eating and orthorexia entail attention to diet quality, the greater presence of orthorexia tendencies might contribute to positive associations between BFCC and restraint in some studies (Coimbra and Ferreira, 2021). The potential for BFCC to be associated with greater orthorexia tendencies calls into questions its characterisation as adaptive and warrants further investigation utilising various types of dietary restraint.
In summary, further investigation is necessary to clarify adaptive eating styles such as intuitive and mindful eating and their subcomponents by understanding their relationships with a broad spectrum of maladaptive eating behaviours. To better conceptualise eating constructs, factor analytic methodologies can be utilised to examine these relationships through the identification of latent constructs (Dakin et al., 2024; Kerin et al., 2019). When investigating aspects of intuitive eating, studies which have employed this methodology have found components of intuitive eating such as EPR inversely load onto disinhibited eating factors (Dakin et al., 2024; Kerin et al., 2019), whilst RHSC and BFCC were found to form constructs independent from maladaptive eating (Dakin et al., 2024; Kerin et al., 2019). Interestingly, UPE was found to inversely load onto the dietary restraint factor and loaded onto the adaptive eating factor represented by RHSC and BFCC, suggesting that certain items within UPE may represent inverse dietary restraint whilst others may represent the presence of adaptive eating (Dakin et al., 2024). This highlights the importance of item-level analysis, as relying heavily on single subscale scores to represent latent constructs may preclude identifying nuances.
The current study
The present study aimed to investigate the factor structure of eating behaviours and attitudes at the item-level across a spectrum of adaptive and maladaptive constructs in women. The study sought to identify which aspects of adaptive eating share conceptual overlap with maladaptive eating, compared to those which are distinct. The study also aimed to assess how the latent constructs related to validation measures to determine their adaptive or maladaptive qualities; with higher body appreciation, self-compassion, and positive affect, and lower eating-related impairment indicating adaptive eating, and the opposite pattern indicative of maladaptive eating.
Method
Participants
Two samples of women living in Australia were recruited. These samples were collected sequentially, and participants could only take part in one iteration of the study. The study was restricted to participants who identified as female to ensure that the results could be contextualised within the majority of previous research, and to prevent gender-based confounds previously identified within the literature (Augustus-Horvath and Tylka, 2011). Sample 1 consisted of 400 participants aged between 18 and 58 years (Mage = 24.10, SD = 9.47). Sample 2 consisted of 423 participants aged between 18 and 60 years (Mage = 23.02, SD = 6.97). Demographic information related to recruitment method, ethnicity, education-level, body mass index (BMI = kg/m2), food intolerance, and eating disorder clinical impairment are reported in Table 1.
Demographic characteristics for Sample 1 and 2.
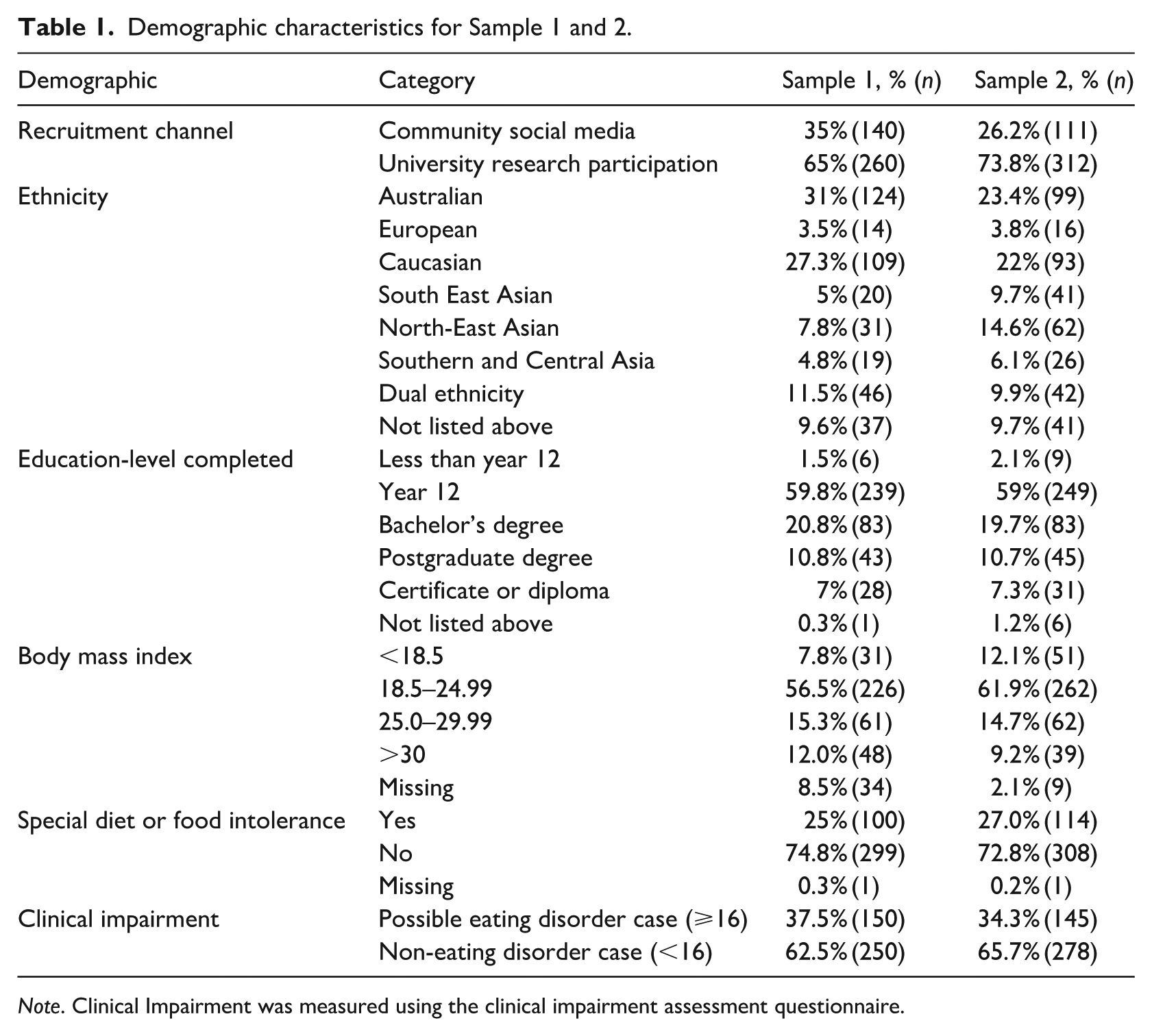
Note. Clinical Impairment was measured using the clinical impairment assessment questionnaire.
Eating items
An initial item pool was derived from psychometrically sound self-report questionnaires listed below. All items within the item pool were revised to be rated on a scale from 0 (never) to 5 (almost always), with higher scores reflecting higher levels of the construct.
The 23-item Intuitive Eating Scale-2 was used to capture the four components: unconditional permission to eat (UPE), eating for physical rather than emotional reasons (EPR), reliance on hunger and satiety cues (RHSC), and body-food choice congruence (BFCC; IES-2; Tylka and Kroon Van Diest, 2013). Additionally, three items based on content from a revised conceptualisation of intuitive eating for clinical practice (Wood-Barcalow et al., 2021), and three constructed items to further reflect gentle nutrition were also included (Supplemental Material A).
The 29-item Mindful Eating Scale was used to assess the following components of mindfulness: acceptance, awareness, distractibility/act with awareness, non-reactivity, routine, and unstructured eating subscales (MES; Hulbert-Williams et al., 2014).
Additionally, items from the Restraint and Eating Concerns subscales of the Eating Disorder Examination Questionnaire (10 items- EDE-Q; Fairburn and Beglin, 1994), and the Binge Eating and Restricting subscales of the Eating Pathology Symptoms Inventory (14 items- EPSI; Forbush et al., 2013) were used to assess dietary restraint and disinhibited eating. The Eating Habits Questionnaire Problems subscale (9 items- EHQ-P; Gleaves et al., 2013) and its revised version (6 items- Bóna et al., 2020) were also used to assess orthorexia nervosa.
Validation measures
The following psychometrically-sound self-report questionnaires were used as validation measures to interpret the adaptive or maladaptive nature of the eating constructs that emerged through factor analysis.
Body appreciation
The 10-item Body Appreciation Scale-2 was rated on a scale from 1 (never) to 5 (always; BAS-2; Tylka and Wood-Barcalow, 2015). Cronbach’s alpha was in the excellent range for Samples 1 (α = 0.951) and 2 (α = 0.953).
Self-compassion
The 13-item Self-Kindness, Common Humanity, and Mindfulness subscales of the Self-Compassion Scale were rated on a scale from 1 (almost never) to 5 (almost always; Neff, 2003). Cronbach’s alpha was in the excellent range for Samples 1 (α = 0.904) and 2 (α = 0.991).
Positive affect
The 10-item Positive subscale of the Positive and Negative Affect Schedule was rated on a scale of 1 (very slightly) to 5 (extremely; PANAS; Watson et al., 1988). Cronbach’s alpha was in the good range for Samples 1 (α = 0.889) and 2 (α = 0.881).
Eating related clinical impairment
The 16-item Clinical Impairment Assessment Questionnaire was rated on a scale of 0 (not at all) to 3 (a lot; CIA; Bohn et al., 2008). Cronbach’s alpha was in the excellent range for Samples 1 (α = 0.950) and 2 (α = 0.961).
As a data quality check, attentive responding was assessed via the Conscientiousness Responders Scale, with scores greater than three indicative of inattentive responding (Marjanovic et al., 2014).
Procedure
Following the provision of informed consent, participants completed an online survey assessing demographic items including age, level of education, ethnicity, weight in kilograms, height in centimetres, and whether they consumed a special diet or experienced any food intolerance. Participants then completed the eating-based items in randomised order, followed by the validation measures. The study was approved by the Australian National University ethics committee (Protocol 2021/648).
Statistical analysis plan
Analyses were conducted using JASP 0.16.4. Seventeen participants were removed across both samples due to not meeting criteria for attentive responding.
Sample 1
Exploratory factor analysis (EFA) was utilised to determine the initial factor structure of eating behaviours. EFA simulation analyses suggest samples greater than 400 are acceptable (Fabrigar et al., 1999), with the current samples meeting this criterion (n1 = 400, n2 = 423). Suitability of the data for EFA was confirmed by a significant Bartlett’s test of sphericity (p < 0.001) and adequate Kaiser-Meyer-Olkin sampling adequacy (KMO = 0.931).
EFA was based on a polychoric correlation matrix and utilised minimum residual estimation given the ordinal nature of the data (Holgado–Tello et al., 2010). An oblique (Promax) rotation was employed to allow for theoretically meaningful correlations between emergent factors, as previous research has demonstrated eating constructs to be correlated (Linardon et al., 2021). A minimum factor loading criterion of >0.40 was chosen to ensure specific facets of eating were not lost during item reduction, given eating is a theoretically broad construct. Cross-loading items (those loading onto more than one factor at any value) were removed iteratively as they were not considered to distinguish between constructs adequately (Tabachnick and Fidell, 2007).
Confirmatory Factor Analysis (CFA) was conducted using Diagonally Weighted Least Squares estimation given the ordinal data. Goodness of fit was evaluated using standardised root mean square residual (SRMR) <0.08 (acceptable fit <0.10), root mean square error of approximation (RMSEA) <0.06 (acceptable fit 0.05–0.08), comparative fit index (CFI) > 0.90 (acceptable fit 0.90–0.95), and non-normed fit index (NNFI) >0.90 (acceptable fit 0.90–0.95; Hu and Bentler, 1999). Model refinement was permitted through the evaluation and removal of items with large modification indices.
Validation analyses using bivariate correlations between the emergent factors, and between the emergent factors and total scores on the validation variables, were conducted.
Sample 2
CFA in Sample 2 was conducted for replication and validation of the initial findings, following the same procedure, however no model changes were conducted using modification indices.
Sample invariance of the final factor structure was assessed using multigroup CFA. An unconstrained configural model (equivalent factor structures) was compared to a metric invariance model (equivalent factor structures and loadings) and scalar invariance model (equivalent factor structures and intercepts). Change in model fit of ΔCFI <0.01 indicated invariance between samples (Chen, 2007).
Bivariate correlations between the emergent factors, and between the emergent factors and total scores on the validation variables, were conducted for the purpose of replication and validation of Sample 1 findings.
Results
Exploratory factor analysis: Sample 1
A total of 97 items were subjected to EFA. A five-factor solution was favoured by a scree-plot elbow test, with parallel analysis indicating a five-factor solution should be retained. Models utilising one to six factor structures were explored for comparison. Models with one to three factors did not appear to form theoretically meaningful constructs, excluded a large portion of items from the final model (non-loading items), and accounted for minimal variance in eating (<44%). The five-factor solution offered an additional 2% of the variance explained compared to the four-factor solution, whilst the six-factor solution also offered an additional 2% of variance explained compared to the five-factor solution (Tabachnick and Fidell, 2007). The five-factor model was chosen as it allowed for meaningful construct breadth and delineation compared to fewer factor solutions, whilst also taking into account parsimony and the elbow test when considering a six-factor solution. The five factors accounted for 55% of the variance in eating behaviours and attitudes.
A total of 16 items were removed from the final solution one-by-one as they did not load on to any factor >0.40 (Ford et al., 1986). Of these 16 items, 12 were from the Mindful Eating Scale (MES; Hulbert-Williams et al., 2014), including the entire awareness subscale. A total of five items that cross-loaded were also iteratively removed. The final EFA solution comprised of 76 items across the 5 factors.
Confirmatory factor analysis: Sample 1
CFA was conducted in Sample 1 on the 76 remaining items suggested via the five-factor EFA. The CFA solution indicated an acceptable model fit; χ2 = 8897.810 p < 0.001, CFI = 0.923, NNFI = 0.921, RMSEA = 0.075, and SRMR = 0.093. Six items from the Dietary Restraint and Disinhibited Eating factors were iteratively removed due to large modification indices suggesting error covariance or cross-loading (modification index >180).
CFA on the final 70-item five-factor model was conducted, χ2 = 6042.07, p < 0.001. Relative fit, measured by CFI and NNFI, were in the near excellent range (0.947 and 0.946 respectively). Absolute fit, measured by RMSEA and SRMR suggested acceptable fit (0.063 and 0.083 respectively; Browne and Cudeck, 1992). The internal consistency (Cronbach’s alpha) for each factor ranged between acceptable to excellent (α = 0.792–0.966; Cronbach and Meehl, 1955). Final factor loadings and indicative item content are reported in the Supplemental Material B.
Final five-factor structure
Factor one, “Dietary Restraint” (28.5% of item variance), comprised 31 items. Dietary Restraint included positive loadings for Restraint and Eating Concern items from the Eating Disorder Examination Questionnaire (EDE-Q), and orthorexia tendencies from the Eating Habits Problems Subscale (EHQ-P; e.g. “I punish myself if I don’t follow my health-food diet”). It also included negative loadings for items from the unconditional permission to eat (UPE) subscale of the Intuitive Eating Scale-2 (IES-2) and acceptance items from the MES (e.g. “I allow myself to eat what food I desire in the momen”).
Factor two, “Disinhibited Eating” (12.9% of item variance), comprised 24 items. It reflected positive loadings for binge eating items from the Eating Pathology Symptoms Inventory (EPSI) and distractibility/act with awareness items from the MES (e.g. “I snack when ’,m bored”). Disinhibited Eating was also represented by negative loadings for items from the eating for physical reasons (EPR) subscale of the IES-2 (e.g. “I find other ways to cope with stress and anxiety than by eating”).
Factor three, “Body-Centric Eating” (6.3% of item variance), comprised 11 items. Body-Centric eating comprised positively loading items from the reliance on hunger and satiety cues (RHSC) and body-food choice congruence (BFCC) subscales from the IES-2 (e.g. “I trust my body to tell me when to eat”).
Factor four, “Severe Restriction” (4.4% of item variance), comprised five items that measured restrictive eating from the EPSI (e.g. “people told me that I do not eat very much”).
Factor five, “Mechanical Eating” (2.5% of item variance), comprised five items from the routine subscale of the MES (e.g. “I eat the same thing for lunch each da”,).
Confirmatory factor analysis: Sample 2
CFA on the final 70-item solution was conducted in Sample 2 to validate findings from Sample 1. The five-factor model fit the data well, χ2 = 5735.52, p < 0.001, CFI and NNFI in the excellent range (0.959 and 0.958, respectively), and RMSEA and SRMR in the acceptable range (0.059 and 0.081, respectively).
Sample invariance
Multigroup CFA assessed the invariance of the five-factor structure across the two samples. The unconstrained configural model, χ2(4670) = 11777.956, CFI = 0.954, the constrained metric model, χ2 (4735) = 12521.249, CFI = 0.949, and the constrained scalar model, χ2 (4800) = 12572.00, CFI = 0.949, were found to fit the data well. Factor structure and loadings were considered invariant across the datasets, Δχ2(65) = 743.293, p < 0.001, ΔCFI = 0.005. Factor structure and intercepts were also considered invariant across the datasets Δχ2(65) = 50.754, p < 0.001, ΔCFI = 0.000. Overall, the results suggest that the observed factor structure was robust and equivalent across samples and provides strong evidence for the reproducibility of the five-factor structure.
Correlations between the five factors
Bivariate correlations revealed significant associations between most emergent factors in both samples. The adaptive factor, Body-Centric Eating, was inversely correlated with the maladaptive eating factors, most strongly with Dietary Restraint (r = −0.45 and −0.54 in Samples 1 and 2, respectively; Cohen, 1988). Maladaptive Dietary Restraint and Severe Restriction demonstrated moderate-positive correlations with each other in Sample 1, which was replicated in Sample 2 (Table 2). The maladaptive factors Disinhibited Eating and Dietary Restraint were moderately positively correlated (r = 0.28 and 0.39 in Samples 1 and 2, respectively), whilst Disinhibited Eating and Severe Restriction were not significantly correlated with each other in Sample 1, which was replicated in Sample 2.
Bivariate correlations between factors in Samples 1 and 2.
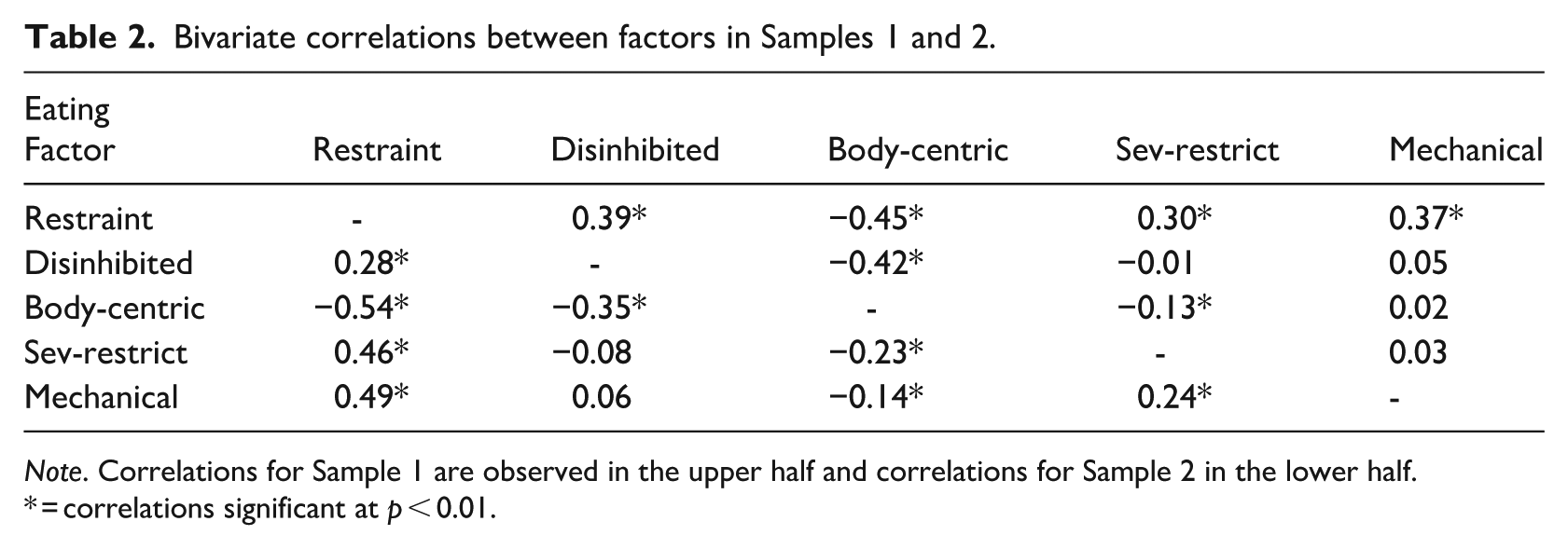
Note. Correlations for Sample 1 are observed in the upper half and correlations for Sample 2 in the lower half.
= correlations significant at p < 0.01.
Correlations between factors and validation measures
In Sample 1, moderate-to-large positive associations were reported between Body-Centric Eating and body appreciation (r = 0.64), positive affect (r = 0.43), and self-compassion (r = 0.45), and a large negative association with clinical impairment (r = −0.50). These results were replicated in Sample 2 (Table 3), providing further support for the adaptive qualities of this style of eating. In contrast, the maladaptive factors Dietary Restraint, Disinhibited Eating, and Severe Restriction demonstrated small-to-large negative associations with body appreciation, positive affect, and self-compassion, and moderate-to-large positive correlations with clinical impairment in Samples 1 and 2. Mechanical Eating demonstrated moderate positive correlations with clinical impairment (r = 0.21 and 0.37 in Sample 1 and 2, respectively), however, was not significantly correlated with self-compassion or positive affect in either sample.
Correlations between the factors and validation measures and Cronbach’s alpha for the factors.
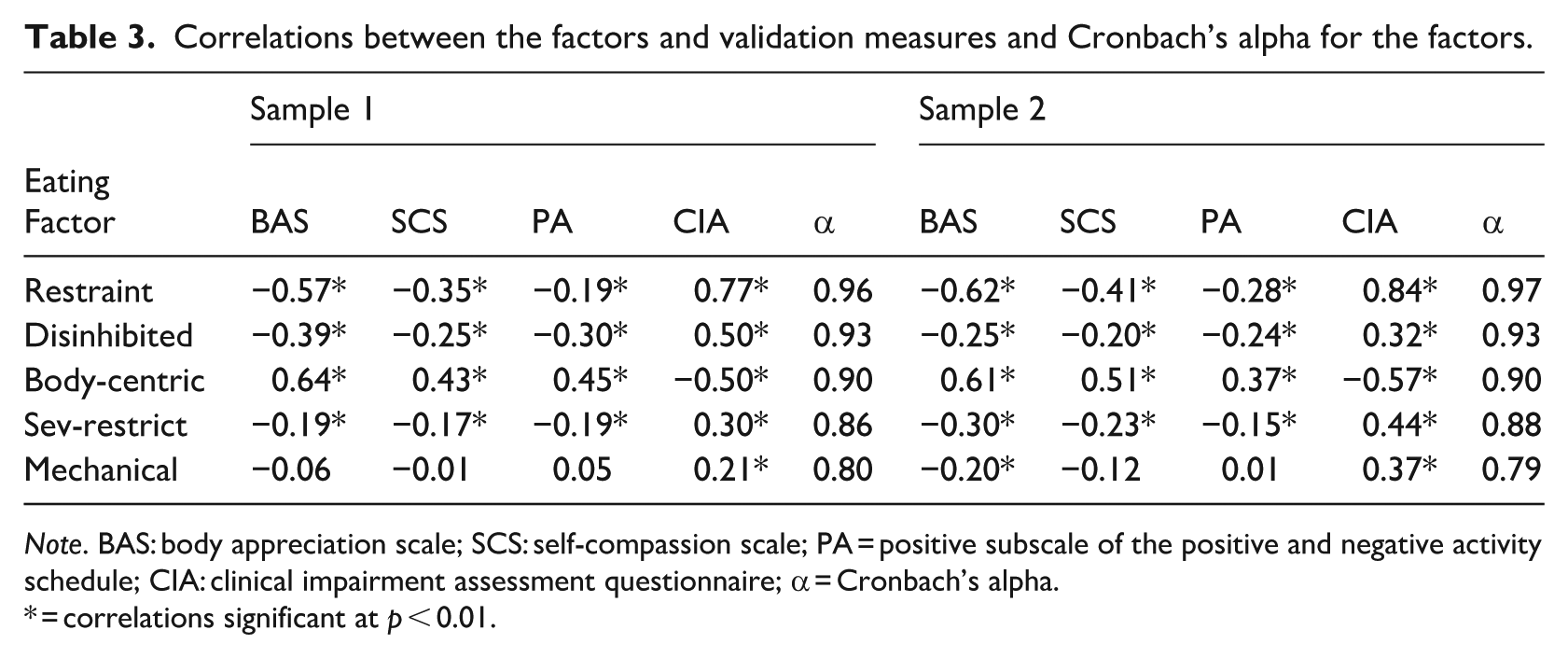
Note. BAS: body appreciation scale; SCS: self-compassion scale; PA = positive subscale of the positive and negative activity schedule; CIA: clinical impairment assessment questionnaire; α = Cronbach’s alpha.
= correlations significant at p < 0.01.
Discussion
The present study investigated the interrelations between a broad range of eating constructs to empirically derive a factor structure of eating attitudes and behaviours, and to identify the extent to which adaptive and maladaptive eating are distinct or overlapping. A five-factor structure was supported and replicated in an independent sample, with invariance demonstrated across two samples of women.
Five-factor structure
The first factor, Dietary Restraint, comprised positively loading items capturing dietary restraint and orthorexia tendencies, and inverse loading items representing UPE and acceptance. The latter finding challenges original conceptualisations of UPE and acceptance as adaptive eating styles that are distinct from maladaptive eating (Hulbert-Williams et al., 2014; Tylka and Kroon Van Diest, 2013). However, it is also reflective previous factor-analytic research, suggesting these constructs do share considerable conceptual overlap with maladaptive eating styles (Dakin et al., 2024; Kerin et al., 2019). When reviewing the items that loaded positively onto this factor, it is unsurprising that UPE items such as “I have forbidden foods I don’t allow myself to eat” (reverse scored on the original UPE scale; Tylka and Kroon Van Diest, 2013) index the dietary restraint dimension. Indeed, previous research suggests certain items within this construct (e.g. “I try to avoid certain foods. . .”) may actually tap “limited permission to eat” (Dakin et al., 2024: p.7). Given this, it is possible that Dietary Restraint comprises a curvilinear spectrum of maladaptive and adaptive eating whereby low-to-moderate levels entail flexible dietary restraint. Dietary Restraint was most strongly associated with clinical impairment, likely reflecting the emotional distress associated with breaking rigid dietary rules (e.g. feeling guilt and punishing the self) and attempts to limit intake and uphold rules (e.g. spending multiple hours thinking about food). This style of eating was also associated with low levels of self-compassion, positive affect, and body appreciation, consistent with the maladaptive nature of rigid dieting (Tylka et al., 2015).
The second factor, Disinhibited Eating, comprised positively loading items capturing emotional eating, external eating, and under-control of eating, and inverse loadings for items reflecting eating for physical rather than emotional reasons (EPR). This factor also represented maladaptive eating due to its moderate associations with clinical impairment and lower levels of psychological well-being. Whilst the EPR subscale of the IES-2 is intended to measure adaptive eating behaviours, it primarily uses items which assess the absence of a maladaptive behaviour rather than the presence of an adaptive process (e.g. “I do NOT turn to food for comfort”; Tylka and Kroon Van Diest, 2013). This may explain why items from this subscale loaded onto Disinhibited Eating rather than forming distinct, adaptive factors. This conclusion is consistent with revisions to the EPR subscale of the recently published IES-3 (Tylka et al., 2024), which has included items to reflect the presence of eating for a variety of physical reasons (e.g. to provide nourishment) rather than the absence of emotional eating.
Given that UPE and EPR are shown to index Dietary Restraint and Disinhibited Eating, respectively, this may suggest that these dimensions of intuitive eating act adaptively through direct impacts on reducing maladaptive processes, whilst their utility at enhancing well-being may be limited, or operating in an indirect manner. Moreover, considering that items reflecting dietary restraint and disinhibited eating loaded most strongly onto their respective factors (Supplemental Material B), it may be that it is the reduction in these maladaptive behaviours rather than the presence of their adaptive counterparts (UPE and EPR) that predicts associations with well-being. This finding is consistent with previous research demonstrating that UPE was unable to predict well-being outcomes beyond shared variance accounted for by its relationship with dietary restraint, as dietary restraint demonstrated stronger relationships with well-being (Tylka and Wilcox, 2006).
The finding that Dietary Restraint and Disinhibited Eating factors include items typically measuring UPE and EPR may also suggest that the four-factor structure of intuitive eating is too broad, and that UPE and EPR more closely align with restraint and disinhibited eating dimensions rather than adaptive conceptualisations. This would align with theoretical positions on adaptive eating that suggest adaptive eating is distinct from maladaptive eating (Tylka and Wilcox, 2006). Given the established relationships between UPE, EPR and maladaptive eating, the use of a global intuitive eating score is also perhaps problematic if conceptualising intuitive eating as an adaptive construct. Cautions against calculating a total score is consistent with critiques of the high-order model (Román et al., 2021), and in light of differential subscale relationships or item loadings in eating disorder populations (Martin-Wagar and Heppner, 2023).
A refined construct such as Body-Centric Eating which emerged as the third factor, might be a more appropriate measure of adaptive eating. Body-Centric Eating consisted of positive loadings for eating in accordance with hunger and satiety cues (RHSC items), and making food choices to nourish the body (BFCC items). Its adaptive nature was further supported by significant associations with greater levels of self-compassion, positive affect, and body appreciation, and lower levels of clinical impairment. Consistent with previous research, Body-Centric Eating may constitute a form of self-actualising behaviour enabling individuals to respond in a nurturing way towards their body despite exposure to sociocultural pressures promoting dieting behaviour (Czepczor-Bernat et al., 2020). Further support for the adaptive interpretation of Body-Centric Eating was demonstrated by its inverse associations with the three maladaptive eating factors identified, and is also consistent with previous research distinguishing BFCC and RHSC from maladaptive eating such as emotional eating, external eating, and dietary restraint (Dakin et al., 2024; Kerin et al., 2019). In addition, the emergence of Body-Centric Eating as distinct from items measuring orthorexia tendencies (contained within Dietary Restraint), is consistent with prior research identifying gentle nutrition as an adaptive and flexible eating approach that differs from a rigid and impairing focus on the health-quality of food (Tylka and Kroon Van Diest, 2013).
The presence of Severe Restriction in factor four, as an eating style independent from Dietary Restraint, supports previous research highlighting differences between cognitive attempts to control eating versus physiological under-eating (Stice et al., 2007). Severe Restriction appears to capture an actual reduction in food intake, as opposed to the cognitive component of restraint reflected in Dietary Restraint. Severe Restriction may reflect individuals who were successful at upholding their dietary rules and therefore derive a sense of achievement (rather than distress) from these behaviours (Fairburn, 2008), which may explain why Dietary Restraint produced stronger relationships with clinical impairment compared to Severe Restriction. Despite this, the strong positive correlations between Severe Restriction and clinical impairment underscore the damaging effects of starvation on functioning (Fairburn, 2008). Providing concurrent evidence of its pathological nature, Severe Restriction was also associated with lower levels of self-compassion, positive affect, and body appreciation.
Finally, Mechanical Eating emerged as an ambiguous fifth factor characterised by adhering to a routine to guide eating behaviours. How best to characterise this factor presents a challenge as Mechanical Eating may be capturing a combination of adaptive and maladaptive eating attitudes and behaviours, which could explain why it demonstrated the lowest internal consistency of all five factors. For example, high scores on Mechanical Eating may reflect individuals who are eating in accordance with a regular meal plan as a strategy to reduce binge eating, consistent with Cognitive Behavioural Therapy for eating disorders (Fairburn, 2008). In contrast to this adaptive function, endorsement of Mechanical Eating might also reflect those unable to relinquish control over their diet plans, which may explain its associations with Dietary Restraint. Such rigidity may suggest associations with comorbidities such as Avoidant-Restrictive Food Intake Disorder or Autism Spectrum Disorder (Schröder et al., 2022), or other eating motivations among individuals who follow eating routines due to medical conditions, athletic diets or cultural reasons. Future research utilising a broader variety of validation measures capturing these motivations for eating is needed to further elucidate the nature of this eating style.
Implications for research, theory, and clinical practice
The five-factor structure identified in this study provides insight into the relationship between adaptive and maladaptive eating styles, and can thus inform the application of adaptive eating strategies in the reduction of eating pathology and enhancement of well-being. For example, given the finding that the Dietary Restraint factor was indexed by inverse loadings for dietary acceptance and unconditional permission to eat, strategies such as engaging in a non-judgemental approach towards eating or not labelling food as “good” or “bad” might prove beneficial strategies to reduce dietary restraint (Stice, 2002). Moreover, Disinhibited Eating comprising a spectrum of binge eating and to eating for physical reasons aligns with intervention approaches such as the mood intolerance module of Enhanced Cognitive Behaviour Therapy, which seeks to reduce disinhibited eating behaviours through the promotion of broader coping strategies to soothe emotions independent of eating (Fairburn, 2008). Similarly, mindful eating strategies such as present-moment awareness might be used to address binge eating behaviours by disrupting symptoms such as eating on auto-pilot (Kristeller et al., 2014). Targeting dietary restraint and disinhibited eating through these pathways of cognitive deprivation and emotion regulation is consistent with the dual-pathway model of bulimia nervosa, which stipulates these two mechanisms as the key factors maintaining disordered eating cycles (Stice, 2002).
Body-Centric Eating was represented as a distinct construct that was positively associated with wellbeing outcomes. This conforms with positive psychological theory which stipulates that adaptive constructs are not merely the absence of pathology, but exist as separate entities which allow individuals to flourish (Iasiello et al., 2020). Body-Centric Eating also provides some concordance with a dual-continua model whereby adaptive and maladaptive processes exist on separate continua (Keyes, 2005). Given that Body-Centric Eating is represented as an independent construct, it is unclear whether the reduction of various maladaptive eating styles such as dietary restriction and disinhibited eating will result in increased levels of adaptive Body-Centric Eating, or whether Body-Centric Eating would be effective at reducing maladaptive eating behaviour. The large inverse correlations between Dietary Restraint and Body-Centric Eating factors suggest they may influence each-other; whereby reductions in cognitive load associated with dieting allow for greater interoceptive awareness and regulation of internal bodily signals to engage in Body-Centric Eating, or vice versa. Future research is necessary to establish causal and temporal relationships between these two eating styles.
Limitations and future directions
To contextualise the results within previous research, the present study utilised a sample of women. This reduces the generalisability of the findings and may limit our capacity to understand the complex relationship between sociocultural pressures across genders and their impacts on eating behaviours (Linardon et al., 2021). For example, curvilinear relationships between aspects of intuitive eating (RHSC and BFCC) and orthorexia nervosa have been found in research conducted in men, but not women (Rodgers et al., 2021). This variation by gender highlights the need for the current findings to be replicated in samples of men to ascertain whether the separation of Body-Centric Eating from Dietary Restraint can be replicated, or if Body-Centric Eating is tapping adaptive eating in men.
Additional demographic characteristics which limit the generalisability of the current findings include the age of the participants (i.e. mean age in early adulthood) and the lack of ethnic diversity as the majority of participants identified as Australian or Caucasian. Intuitive eating is shown to increase across the lifespan, whilst many disordered eating behaviours are shown to decrease, highlighting variance in eating across age (Augustus-Horvath and Tylka, 2011; Hudson et al., 2007). This has potential to change the observed factor structure, such as the emergence of additional distinct adaptive eating factors due to a decline in their association with maladaptive eating in older adults. Similarly, cross-cultural variations in eating constructs are observed, including a failure to replicate the higher-order factor structure of the IES-2 in a German sample (Román et al., 2021). To overcome such methodological limitations, the present study utilised item-level analysis, which is considered one of its strengths. However, whether the observed factor structure is invariant across samples with a greater representation of ethnic groups is an area requiring further study.
The study sought to provide a comprehensive evaluation of eating styles, yet further work would benefit from the inclusion of other styles of eating such as flexible dieting, a construct that is shown to be distinct from intuitive eating, yet shares overlap with restrictive dieting (Tylka et al., 2015). In addition, given critiques of mindful eating measures (Mantzios, 2021), further refinement of mindful eating measures would be beneficial to the understanding of it as a potential adaptive eating style, alongside the use of the recently developed IES-3 which addresses limitations of the IES-2 (Tylka et al., 2024).
Finally, future research is needed to explore potential differences in the adaptive versus maladaptive nature of the identified eating patterns among those with and without an eating disorder. Preliminary research has suggested that certain facets of intuitive eating do not appropriately tap the original constructs when measured in eating disorder samples, where “adaptive behaviours” might be endorsed for pathological reasons (Martin-Wagar and Heppner, 2023). Examples include engaging in “gentle nutrition” behaviours due to beliefs that healthy eating will result in weight loss, or using UPE principles as permissive beliefs to engage in binge eating (Martin-Wagar and Heppner, 2023). Given the data collected was at the group-level, idiographic or qualitative research investigating the motives behind endorsement of certain items may provide greater clarity into these possibilities.
Conclusion
This study is the first to simultaneously assess item-level indicators of adaptive and maladaptive eating constructs, providing insight into the relationships between eating constructs, and their associations with psychological wellbeing and impairment. Results suggested a five-factor model, with one factor representing adaptive processes (Body-Centric Eating), three factors characterising maladaptive process (Dietary Restraint, Disinhibited Eating, and Severe Restriction), and one suggestive of a combination of eating styles (Mechanical Eating). An integrated understanding of the relationships between eating styles sheds light on the degree of overlap and distinctiveness of adaptive and maladaptive eating behaviours and attitudes. This in turn provides insight into which adaptive processes might reduce maladaptive eating given their overlap versus those that are distinct and enhance general wellbeing.
Supplemental Material
sj-docx-1-hpq-10.1177_13591053261418428 – Supplemental material for Clarifying the relationship between intuitive eating, mindful eating, and maladaptive eating: A factor analytic study
Supplemental material, sj-docx-1-hpq-10.1177_13591053261418428 for Clarifying the relationship between intuitive eating, mindful eating, and maladaptive eating: A factor analytic study by Emily Bell, Elizabeth Rieger, Kristen Murray and Conal Monaghan in Journal of Health Psychology
Supplemental Material
sj-docx-2-hpq-10.1177_13591053261418428 – Supplemental material for Clarifying the relationship between intuitive eating, mindful eating, and maladaptive eating: A factor analytic study
Supplemental material, sj-docx-2-hpq-10.1177_13591053261418428 for Clarifying the relationship between intuitive eating, mindful eating, and maladaptive eating: A factor analytic study by Emily Bell, Elizabeth Rieger, Kristen Murray and Conal Monaghan in Journal of Health Psychology
Footnotes
Ethical considerations
The study was approved by the Australian National University Ethics Committee (protocol 2021/648).
Consent to participate
Participants provided written informed consent prior to completing the study.
Consent for publication
Informed consent for publication was provided by the participants.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This research was funded by the Australian National University PhD Scholarship Stipend however the funding source did not have any input into the study design. The study did not receive any additional grants from funding agencies in the public, commercial, or not-for-profit sectors.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data availability statement
The data can be made available upon reasonable request to the lead author.
Supplemental material
Supplemental material for this article is available online.