
Abstract
Introduction:
Sex differences exist in risk factors and comorbidities of older adults (aged ⩾ 65 years) with pulmonary embolism (PE). Clinically relevant sex-based treatment disparities for PE have not been adequately addressed. The few existing show conflicting results due to small sample size (type II error) and suboptimal methods (overreliance on p-value, which may detect differences of small clinical relevance).
Methods:
We assessed sex differences in anticoagulation and advanced therapies for PE in older adults, utilizing data from Registro Informatizado Enfermedad TromboEmbolica (RIETE), a large PE registry with predominant participation from Europe, and data from US Medicare beneficiaries. We prespecified a standardized difference (SRD) > 10% as clinically relevant. RIETE included 33,462 (57.7% female) and Medicare included 102,391 (55.0% female) older adults with PE.
Results:
In RIETE, there were no overall sex differences in the use of anticoagulation (median: 181 vs 180 days, SRD < 1%), fibrinolysis (SRD < 3%), thrombectomy (SRD < 2%), or inferior vena cava (IVC) filters (SRD: 4.4%). However, fibrinolytic therapy (systemic or catheter-based) was less often used in female than male patients with intermediate-risk PE (8.0% vs 12.1%, SRD: 13.6%). No sex differences were noted with advanced PE therapies in Medicare beneficiaries. In unadjusted analyses, fibrinolysis and IVC filter placement were more frequent in Medicare than RIETE participants regardless of sex (p < 0.001).
Conclusion:
In a predominantly European PE registry and a US study of older adults, there were no overall sex differences in anticoagulation patterns or advanced therapy utilization. Future studies should determine if sex disparities in fibrinolytic therapy for intermediate-risk PE and greater use of advanced therapies in US older adults correlate with clinical outcomes.
Keywords
Introduction
Sex-based disparities in cardiovascular disease may predispose patients to poor health outcomes, and yet, have remained under-recognized and understudied. 1 Disparities in treatment strategies may be due to both the influence of biological sex on choice of therapies by clinicians or patients, sex differences in access to optimal care, or implicit or explicit biases within the healthcare system.2,3
Pulmonary embolism (PE) is a potentially life-threatening thrombotic disease in which disparities may exist in treatment strategies. PE has the highest incidence among older adults, as most PEs occur in individuals older than 60 years.4 –7 Sex differences in treatment may be particularly relevant in this population. Unlike younger individuals, if differences in treatment strategies are identified, they are unrelated to factors such as pregnancy or breastfeeding that account for a large proportion of events in younger patients and impact many treatment choices by patients and clinicians alike. Prior smaller studies suggest that sex disparities may exist in the use of anticoagulation8,9 in older patients with PE. Other studies suggest that fibrinolytic therapy is used less frequently in women, although they present with hemodynamic instability more frequently compared with men. 10 However, these prior studies either did not report specific findings in older adults or included only a small number of patients. Additionally, the earlier studies were unable to assess different subgroups of patients based on their baseline PE risk and did not assess potential sex differences in the use of other advanced therapies, many of which have become available only in the past several years. Moreover, very limited knowledge exists about the presence and extent of treatment disparities in regions outside of the United States. 11
SEx differences in presentation, RIsk factors, drug and interventional therapies, and OUtcomeS of elderly patients with Pulmonary Embolism (SERIOUS-PE) is an ongoing multidisciplinary international collaborative using two large data sources to understand the sex differences in PE clinical presentation and treatment strategies among adults aged 65 years or older. 12 The current study was designed to investigate the possible sex differences in anticoagulation patterns and advanced treatment strategies for older adults with acute PE, and to explore potential reasons for such differences.
Methods
Data source and general design
The rationale and general design features of the SERIOUS-PE study have been described previously. 12 Two distinct large data sources were used: data from the Registro Informatizado Enfermedad TromboEmbolica (RIETE) and data from US Medicare Fee-For-Service.
RIETE is the largest available prospective registry of patients with objectively confirmed venous thromboembolism (VTE) and includes detailed information about patient characteristics, treatment patterns, and outcomes. Initially started in Spain in 2001, in more recent years, RIETE has enrolled patients from several countries in Europe, but also Africa, the Americas, and Asia. Details about methodology of RIETE and participating centers have been extensively described previously.7,13 Additional details are available online (https://rieteregistry.com/). As of February 8, 2024, RIETE included 120,539 patients with VTE. Patients who agree and give informed consent are enrolled in the registry. In this study, female and male patients aged ⩾ 65 years with objectively confirmed acute PE from 2001 to 2021 were included. The Institutional Review Board in each RIETE site approved enrollment in RIETE and data entry.
Because most enrollees from RIETE (nearly 90%) are from Europe, data from the US Medicare Fee-For-Service beneficiaries were analyzed to offer an additional viewpoint from the United States. To identify hospitalized patients with PE, validated principal discharge diagnosis codes based on the International Classification of Diseases (ICD) were used (ICD-10 codes: I26, I26.0, I26.02, I26.09, I26.9, I26.92, I26.93, I26.94, I26.99). 14 Analyses from Medicare data were exempt from additional review by the Human Investigation Committee at Yale University because all data were de-identified.
Similar to prior SERIOUS-PE investigations,12,15 we planned to include patients from 2001 through 2019. However, owing to unforeseen circumstances with access to the database, analyses of Medicare used data from 2019, which included more than 100,000 hospitalizations with PE.
Grouping variable
Sex reported by the patient was the main exposure variable in both databases. In RIETE, sex was defined as female or male by patient reports and medical record documentation. In the US Medicare beneficiaries’ database, sex was defined by patient self-report. Sex encompasses the biological and physiological characteristics, whereas gender is a social construct that can be nonbinary. In this article, sex will be implied when female adults and male adults are referred to as women and men.
Therapies
We assessed the sex differences in treatment strategies in older adults with PE from RIETE and US Medicare beneficiaries’ databases. In RIETE, we compared the use, type, intensity, and median duration of anticoagulation therapy in female versus male patients. RIETE includes time stamps per day but not minute or hour. Therefore, although other datapoints were also available, day 2 was chosen for the description of ‘baseline’ anticoagulation. We also reported sex differences in use of anticoagulation at days 90, 180, and 360. Additionally, we analyzed the use of direct oral anticoagulants in female and male patients. Further, we reviewed the use of systemic fibrinolysis, catheter-directed fibrinolysis, surgical embolectomy, percutaneous thrombectomy, and inferior vena cava (IVC) filters within 7 days from diagnosis of PE. Data from RIETE made it possible to further assess the risk of PE according to European Society of Cardiology classification 16 and to report the advanced therapies across these risk subgroups. Patients with systolic hypotension (⩽ 90 mmHg) were considered high risk, those who were not hypotensive but had imaging or biomarker evidence of right ventricular dysfunction, or an elevated simplified PE severity index were considered intermediate risk. If both imaging (right to left ventricular ratio > 1 either by computed tomography or echocardiography) and laboratory biomarkers were abnormal, patients were considered intermediate–high risk. 16 Such data elements are available in RIETE based on patient interview and medical records.
In the US Medicare beneficiaries, we assessed the use of systemic fibrinolysis, catheter-directed fibrinolysis, surgical embolectomy, percutaneous thrombectomy, IVC filter placement, and extracorporeal membrane oxygenation. The procedure codes were based on those assessed and validated in prior studies. 14
Statistical analysis
Percentages were reported for categorical variables. Mean and SD or median and IQR were reported for continuous variables.
Considering the very large size of both databases, many of the differences between female and male patients were expected to reach statistical significance by traditional cut-offs (such as p < 0.05). However, some may not be clinically relevant. Therefore, standardized differences (SRDs) were reported between female and male patients to identify comparisons with clinical relevance rather than just statistical significance. An SRD > 10% in absolute value difference was considered large enough to be clinically relevant. 17 For continuous variables, the SRD was calculated by dividing mean differences by a common SD (square root of the sum of variances of each group divided by 2). For binary variables, the SRD was calculated as a difference of proportions divided by a common SD (calculated based on a binomial distribution (p*(1 – p)). If clinically relevant sex differences were noted, bivariate and multivariable logistic regression were considered to identify potential factors associated with differential use of therapies for subgroups that were not considered too small per consensus among the Steering Committee. When conducting hypothesis tests, no adjustment for multiple comparisons between RIETE and Medicare Fee-For-Service databases was necessary as these databases operate independently. Statistical analyses were performed by Stata, version 17.1 (StataCorp LLC, College Station, TX, USA) and SAS, version 9.4, 64-bit (SAS Institute, Inc., Cary, NC, USA).
Results
We have previously described the baseline clinical characteristics of participants from RIETE and from Medicare that were included in SERIOUS-PE. 15 Briefly, in both databases, female patients were older than male patients (mean age: 78.4 vs 76.4 years, SRD: 34% in RIETE; 77.9 vs 75.7 years, SRD: 30% in Medicare), and more frequently had a history of hormonal therapies, immobility, and depression. Data related to history of trauma were also available in both databases and were more common in female than male patients with PE (4.0% vs 2.1%, SRD: 11% in RIETE; 11.1% vs 8.1%, SRD: 10.0% in Medicare). In contrast, they less frequently had a history of cancer, atherosclerotic cardiovascular disease, or chronic lung disease. 15 The current investigation included 33,462 patients from RIETE and 102,391 patients from Medicare.
In the RIETE participants, the ESC risk classification was assessed. Among female patients, 11.3% were low risk, 34.2% were intermediate–low risk, 3.9% were intermediate–high risk, and 3.4% were high risk; the corresponding estimates for male patients were 11.7%, 33.4%, 3.3%, and 3.3%. In some participants (47.7%), women and men alike, the ESC risk classification could not be determined because of a lack of the necessary data elements.
Hospitalization status and hospital length of stay
In RIETE, 12,996 (95.3%) female patients were hospitalized with a mean hospital length of stay of 10.1 days, and 9647 (94.8%) male patients were hospitalized with a mean hospital length of stay of 10.4 days (SRD: 2.6%).
Analyses in US Medicare beneficiaries were limited to hospitalized patients. The mean length of hospital stay was 4.6 days in women and 4.5 days in men (SRD: 2.7%).
Anticoagulation strategies
In RIETE, the type of anticoagulation among women on day two postdiagnosis was unfractionated heparin in 7.7% of cases, low-molecular-weight heparin (LMWH) in 86.8%, and direct oral anticoagulants in 2.1%. The proportions of men receiving these therapies were 7.8%, 86.1%, and 2.5% for unfractionated heparin, LMWH, and direct oral anticoagulants, respectively, without clinically relevant sex differences (Table S1).
Of the women who were alive on day 90, 94.5% were on anticoagulation, and for men, the respective proportion was 94.6% (SRD: 0.6%), with a similar gradual drop in the proportion of patients remaining on anticoagulation over time in female and male patients. The median duration of anticoagulation was similar between the sexes (181 vs 180 days). Figure 1A summarizes the breakdown of anticoagulation use in both sexes over time.
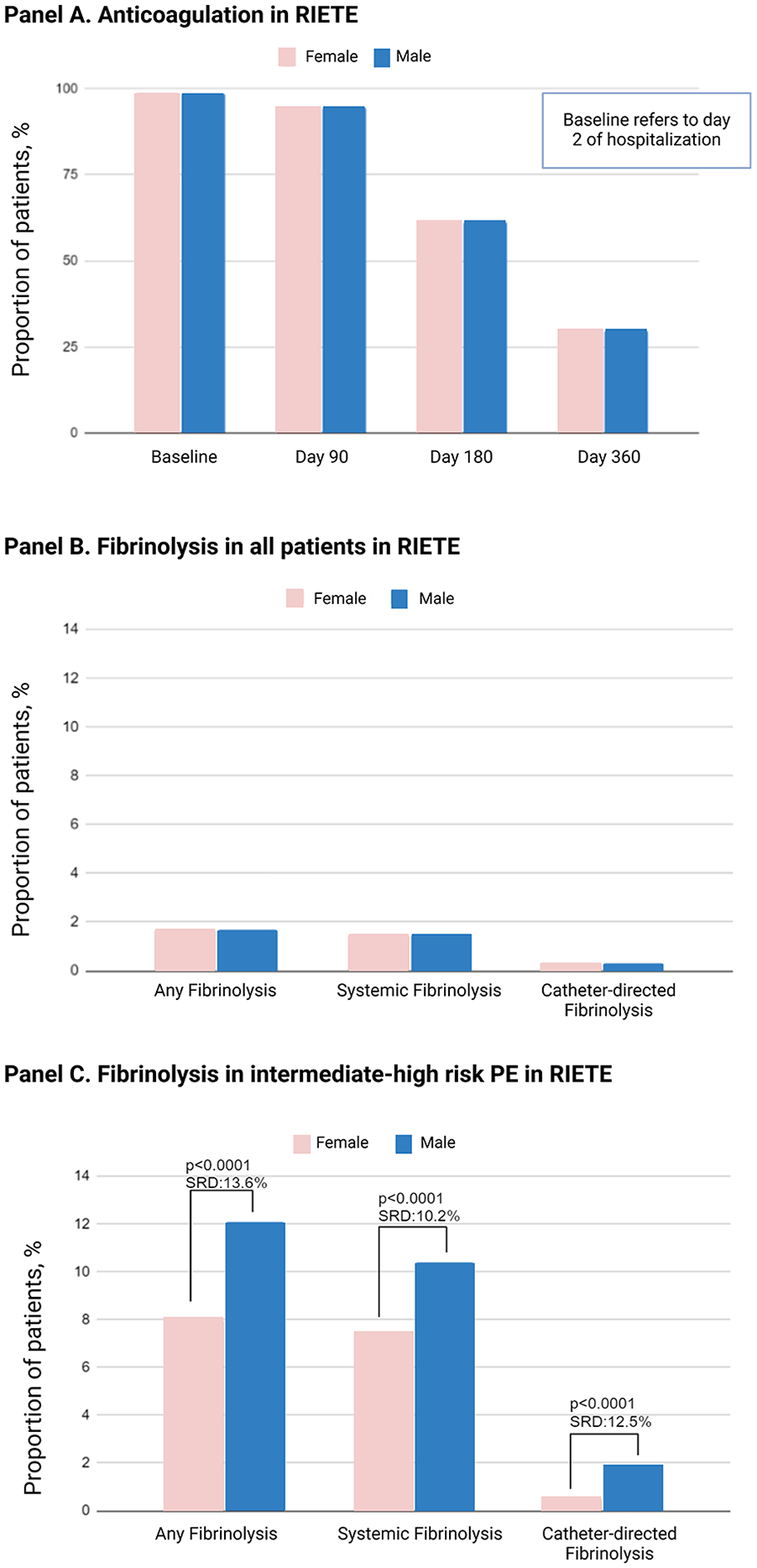
Sex differences in use of anticoagulation in older adults with pulmonary embolism
Advanced therapies in RIETE
In RIETE, in the overall cohort of older adults with PE, 0.6% of female patients underwent surgical embolectomy, and the corresponding number for male patients was 0.8% (SRD: 1.9%). The utilization of percutaneous thrombectomy occurred in 0.3% for both female and male patients (SRD: 0.2%). Systemic fibrinolysis was used in 1.5% of both women and men (SRD: 0%). Catheter-directed fibrinolysis was utilized in 0.3% of women and men (SRD: 0.1%). The use of IVC filters within the first 7 days since PE diagnosis was 1.2% in women and 1.8% in men (SRD: 4.4%). The use of extracorporeal membrane oxygenation (ECMO), available in RIETE only in recent years, in women and men was reported in 0.3% of patients, with only five instances recorded for each sex (SRD: 0.7%; Table S2).
Among RIETE patients with intermediate–high-risk PE, female patients less frequently received fibrinolysis (8.0% vs 12.1%, SRD: 13.6%). This included systemic fibrinolysis (7.5% vs 10.4%, SRD: 10.2%) and catheter-directed fibrinolysis (0.5% vs 1.9%, SRD: 12.5%) (Figure 1B and 1C). By consensus among coauthors, sex, age, history of major bleeding in the prior 30 days, baseline creatinine, active cancer, and sex of the treating clinician were considered as potential covariates for use of fibrinolysis in patients with intermediate-risk PE. It was prespecified to run tests of interaction between these covariates. In addition to female sex (odds ratio [OR]: 0.63, 95% CI: 0.43, 0.93), other bivariate predictors of lower odds of fibrinolytic therapy included active cancer (OR: 0.48, 95% CI: 0.25, 0.92) and older age (OR: 0.90, 95% CI: 0.87, 0.93); there was no significant association in bivariate analysis with other variables. Interestingly, the test of interaction between sex of the patient and sex of the treating clinician was positive (p = 0.035) such that the results of multivariable analysis should be reported separately based on the sex of the treating clinician. In multivariable analysis adjusted for active cancer and age, among patients whose treating clinician was a man, there were no sex differences in use of fibrinolytic therapy in patients with intermediate-risk PE (OR: 1.05, 95% CI: 0.62, 1.79). However, among patients whose treating clinician was a woman, once adjusted for active cancer and age, female sex of the patient was associated with reduced odds of using fibrinolytic therapy (OR: 0.53, 95% CI: 0.28, 0.99).
Among RIETE participants with high-risk PE (i.e., those with systemic arterial hypotension), there were no clinically relevant differences between female and male adults in use of fibrinolysis (14.5% vs 14.3%, SRD: 0.8%), including systemic fibrinolysis (13.9% vs 14.0%, SRD: 0.4%) and catheter-directed fibrinolysis (0.8% vs 0.2%, SRD: 7.9%). However, women were less likely to receive an IVC filter (1.8% vs 4.0%, SRD: 13.1%).
In Medicare beneficiaries, 0.11% of women and men had surgical embolectomy (SRD: 0%). Percutaneous embolectomy was used in 0.92% of women and 1.17% of men (SRD: 2.5%). Systemic thrombolysis was utilized in 2.88% of women and 2.77% of men (SRD: 0.7%). The utilization of catheter-directed thrombolysis in women was 3.59% and 4.08% in men (SRD: 2.6%). IVC filters were placed in 5.45% of women and 6.17% of men (SRD: 0.31%). ECMO was utilized in 0.11% of women and men (SRD: 0%; Table S3).
Compared with RIETE, use of IVC filters and percutaneous thrombectomy were more frequent among older adults from Medicare, without a clear distinction across sex groups (Figure 2; p < 0.001 for both comparisons).
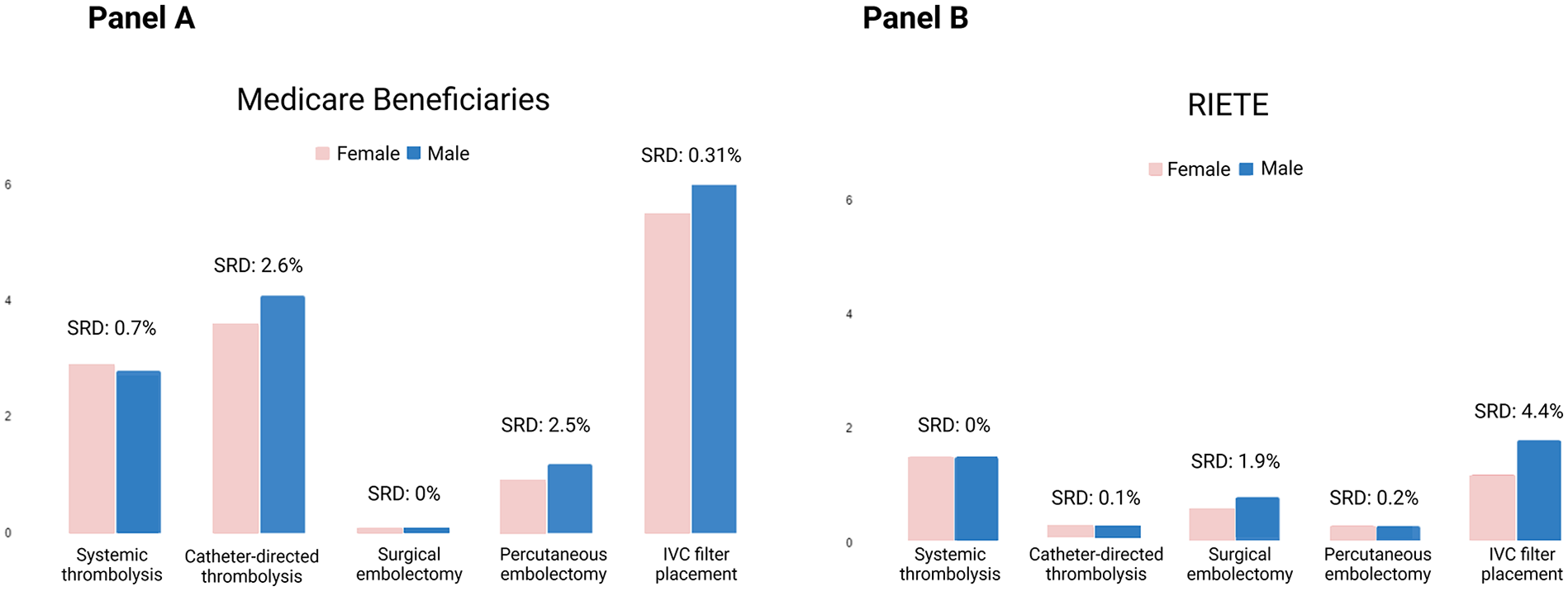
Sex differences in advanced therapies in older adults with pulmonary embolism from Medicare Fee-For-Service beneficiaries
Discussion
In this prespecified analysis of the SERIOUS-PE study using data from the RIETE registry and US Medicare beneficiaries, clinically relevant sex differences were not observed in use, type, or duration of anticoagulation, or for most advanced therapies in patients with PE. The exception was the use of fibrinolytic therapy, both catheter-directed and systemic, in the subgroup with intermediate–high-risk PE, which occurred less frequently in female patients, compared with male patients (Figure 3).
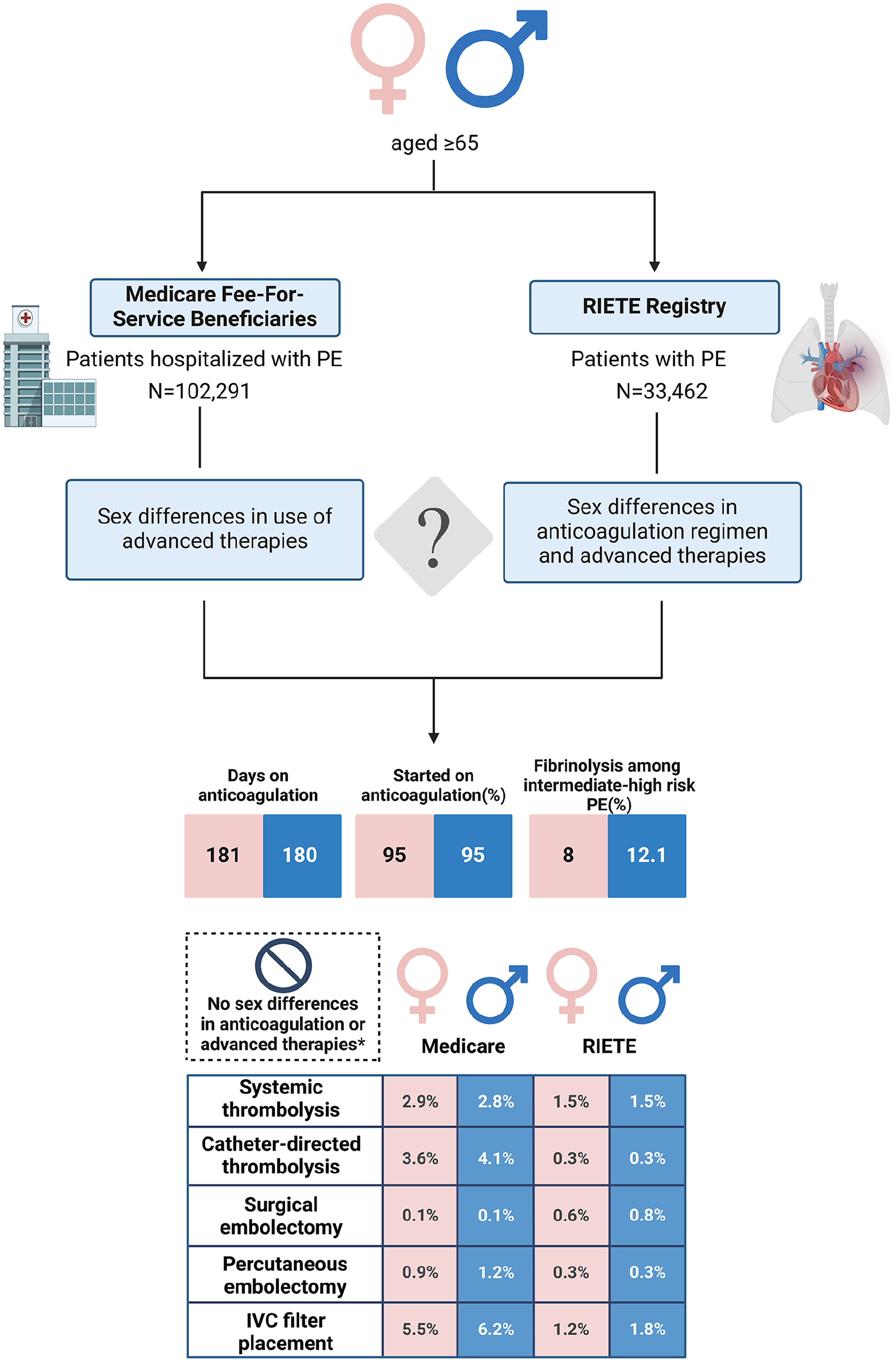
Graphical abstract of study design and results shows that no sex differences were noted in anticoagulation patterns or use of advanced therapies in older adults with pulmonary embolism. Anticoagulation was assessed only in RIETE.
Our finding of no major disparities in the type or duration of anticoagulation between female versus male older adults contributes to the body of the literature related to treatment strategies for PE among sexes. Most prior studies did not investigate or report on sex differences in anticoagulation, and the few that did have revealed conflicting findings.8,10,18 –22 In addition to anticoagulation, similar to our study, some prior studies did not show a noticeable sex difference in the overall use of fibrinolysis,10,18,20 although a few studies showed less frequent use, 23 or more frequent use 19 among female adults. It is important to consider that most prior studies that assessed sex differences in therapies were not adjusted for age and did not report the results among older adults (Table 1).
Studies reporting sex differences in anticoagulation regimen and advanced therapies.
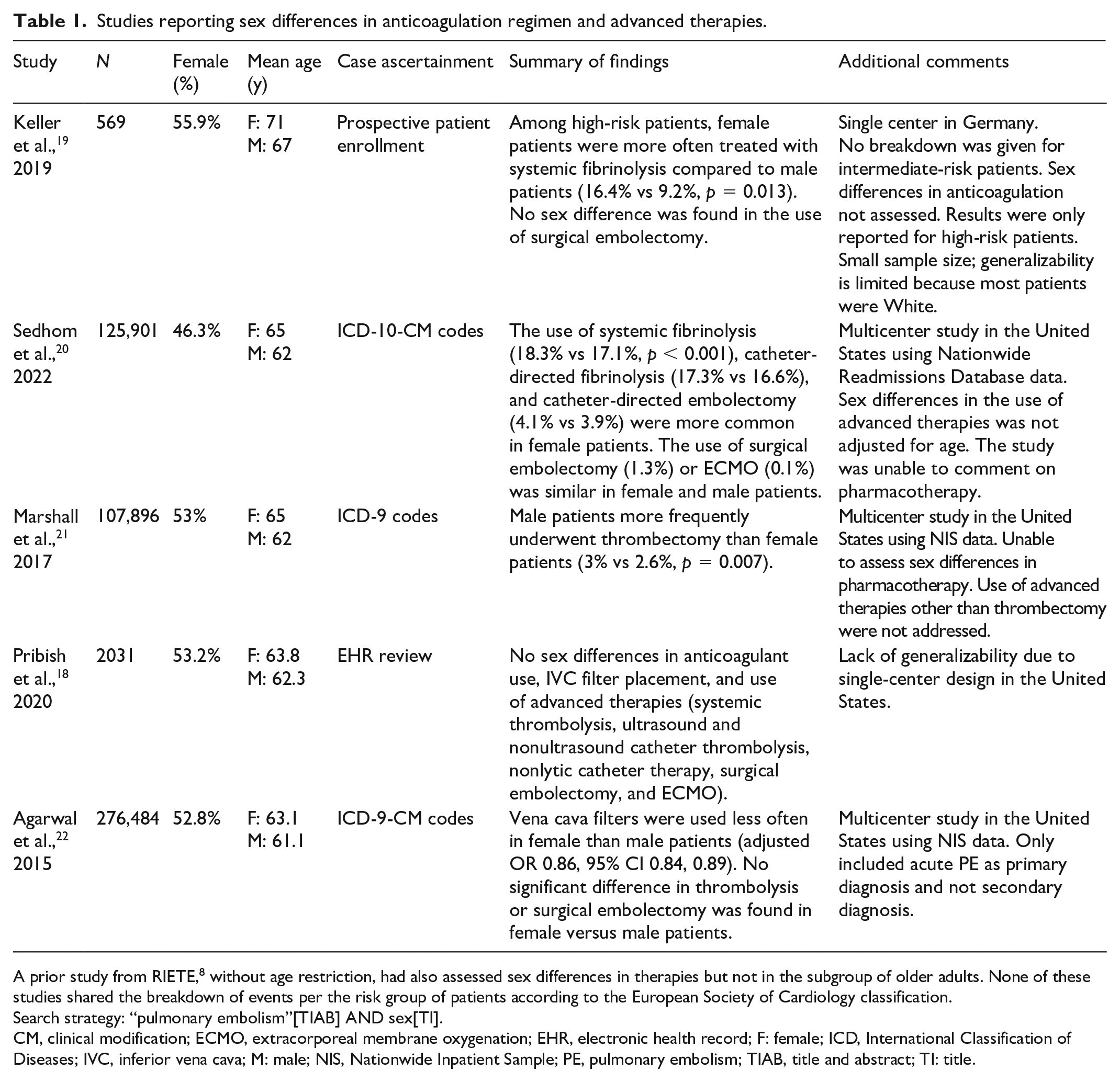
A prior study from RIETE, 8 without age restriction, had also assessed sex differences in therapies but not in the subgroup of older adults. None of these studies shared the breakdown of events per the risk group of patients according to the European Society of Cardiology classification.
Search strategy: “pulmonary embolism”[TIAB] AND sex[TI].
CM, clinical modification; ECMO, extracorporeal membrane oxygenation; EHR, electronic health record; F: female; ICD, International Classification of Diseases; IVC, inferior vena cava; M: male; NIS, Nationwide Inpatient Sample; PE, pulmonary embolism; TIAB, title and abstract; TI: title.
A clinically relevant sex difference in utilization of advanced therapies was observed in RIETE among patients with intermediate-risk PE, in whom older female adults were less likely, compared with male patients, to receive fibrinolytic therapy. Findings were consistent both for systemic fibrinolysis and for catheter-directed fibrinolysis. Surprisingly, we noted a statistical interaction between sex of the patient and that of the treating clinician, such that there was a lower chance of use of fibrinolysis in women with intermediate-risk PE treated by female clinicians. This may warrant additional research, including qualitative research to understand the reasons for such decisions, and future analyses to understand the treatment appropriateness and whether such decisions correlated with adjusted short- and long-term clinical outcomes. We remain unaware of findings reported from other large studies about sex-specific utilization of fibrinolysis in patients with intermediate-risk PE. The critical question from a clinical and societal perspective is whether such differences in use of fibrinolysis are related to differences in clinical characteristics, perceived or actual excess risk of bleeding, or truly represent disparities that may correlate with clinical outcomes, which deserve additional attention. Additional sex differences in the use of other advanced therapies were also observed. However, despite the large size of the registry, several of those were driven by a small number of patients and, as such, we tempered the interpretation of these findings. Nevertheless, these observations will be critical for the subsequent investigations from SERIOUS-PE that will explore both short-term and 1-year clinical outcomes. 10
Findings from this study lay the foundation for investigating the clinical outcomes between elderly female and male patients with intermediate–high-risk PE in unadjusted models and when adjusting for the use of advanced therapies. In fact, assessing the sex differences in clinical outcomes in unadjusted analyses, and also in sequentially adjusted models that account for clinical characteristics, treatment strategies, and clustering of observations within sites, will be critical to better understand if sex disparities exist in PE care. Nevertheless, the current investigation is also valuable because assessment of treatment strategies in outcomes research studies indicate resource allocation and cost implications, in addition to the potential for impacting safety or effectiveness outcomes.
We also observed more frequent use of advanced therapies such as catheter-directed fibrinolysis and vena cava filter placement in US Medicare beneficiaries compared with RIETE participants, who are predominantly from Europe. These findings are consistent with prior studies24,25 that showed several-fold higher utilization rates for vena cava filters in the US compared with Europe. Though this study cannot ascertain the cause of these differences, they may be connected to a lower threshold for using (overuse) certain technologies more frequently in the US. 26
This study has several limitations. It is difficult to track, with high accuracy, the use and duration of anticoagulation using administrative claims data from Medicare. However, we were able to explore the use of advanced therapies similarly in RIETE and among Medicare Fee-For-Service beneficiaries. Pharmacotherapy was, in turn, explored in detail using RIETE, which was full of granular patient-level data. Even though unforeseen issues with Medicare data for the intended study period occurred, the included cohort from 2019 was still very large, with more than 100,000 hospitalizations, making it possible to explore clinically relevant sex differences. Further, as prespecified in the plan of the study, we have not yet initiated the assessment of clinical outcomes. 12 Therefore, we are unable to comment on the link between treatment patterns and outcomes. For those analyses to be most informative, the study protocol planned to assess the sex differences (or lack of clinically relevant sex differences) in patient characteristics 15 and treatment strategies for acute PE ahead of time, to pave the way for assessment of outcomes in unadjusted as well as sequential adjusted models. Data are being processed for such analyses that will be performed over the next several months. Finally, we must acknowledge the inherent differences between the data sources, which were complementary for sex differences comparisons and not primarily planned for sex-neutral comparisons across the databases, which can be subject to confounding by differences in case mix. Though the comparisons between US Medicare beneficiaries and RIETE participants are exploratory and unadjusted, the higher length of stay in RIETE than US Medicare beneficiaries may be related to different reimbursement policies, and some differences in case mix and practice patterns, including bridging anticoagulation that necessitates inpatient stay, particularly in earlier years of RIETE.
Conclusion
In conclusion, data from RIETE, a global PE registry with dominant representation from Western European countries, and that of US Medicare Fee-For-Service beneficiaries did not reveal any clinically relevant sex differences in anticoagulant therapy, or in utilization of advanced therapies in the majority of older adults with PE except with the use of fibrinolysis in those with intermediate-risk PE. Future investigations from SERIOUS-PE should determine if a lower utilization rate of fibrinolytic therapy in female patients with intermediate-risk PE and greater use of advanced therapies in US older adults – noted as a post hoc observation – correlate with clinical outcomes.
Supplemental Material
sj-pdf-1-vmj-10.1177_1358863X241292023 – Supplemental material for Sex differences in treatment strategies for pulmonary embolism in older adults: The SERIOUS-PE study of RIETE participants and US Medicare beneficiaries
Supplemental material, sj-pdf-1-vmj-10.1177_1358863X241292023 for Sex differences in treatment strategies for pulmonary embolism in older adults: The SERIOUS-PE study of RIETE participants and US Medicare beneficiaries by Behnood Bikdeli, Hannah Leyva, Alfonso Muriel, Zhenqiu Lin, Gregory Piazza, Candrika D Khairani, Rachel P Rosovsky, Ghazaleh Mehdipour, Michelle L O’Donoghue, Olga Madridano, Juan Bosco Lopez-Saez, Meritxell Mellado, Ana Maria Diaz Brasero, Elvira Grandone, Primavera A Spagnolo, Yuan Lu, Laurent Bertoletti, Luciano López-Jiménez, Manuel Jesús Núñez, Ángeles Blanco-Molina, Marie Gerhard-Herman, Samuel Z Goldhaber, Shannon M Bates, David Jimenez, Harlan M Krumholz and Manuel Monreal in Vascular Medicine
Supplemental Material
sj-pdf-2-vmj-10.1177_1358863X241292023 – Supplemental material for Sex differences in treatment strategies for pulmonary embolism in older adults: The SERIOUS-PE study of RIETE participants and US Medicare beneficiaries
Supplemental material, sj-pdf-2-vmj-10.1177_1358863X241292023 for Sex differences in treatment strategies for pulmonary embolism in older adults: The SERIOUS-PE study of RIETE participants and US Medicare beneficiaries by Behnood Bikdeli, Hannah Leyva, Alfonso Muriel, Zhenqiu Lin, Gregory Piazza, Candrika D Khairani, Rachel P Rosovsky, Ghazaleh Mehdipour, Michelle L O’Donoghue, Olga Madridano, Juan Bosco Lopez-Saez, Meritxell Mellado, Ana Maria Diaz Brasero, Elvira Grandone, Primavera A Spagnolo, Yuan Lu, Laurent Bertoletti, Luciano López-Jiménez, Manuel Jesús Núñez, Ángeles Blanco-Molina, Marie Gerhard-Herman, Samuel Z Goldhaber, Shannon M Bates, David Jimenez, Harlan M Krumholz and Manuel Monreal in Vascular Medicine
Footnotes
Acknowledgements
The authors acknowledge Sanofi Spain and ROVI for supporting the RIETE Registry with an unrestricted educational grant. The authors thank the RIETE Registry Coordinating Center and S&H Medical Science Service for their quality control data and logistic and administrative support. The full list of members of the RIETE group is provided in the ![]() .
.
A commentary by Javanmardi et al. 27 accompanies this article.
Declaration of conflicting interests
Outside the submitted work, the authors disclosed the following. Dr Bikdeli is supported by a Career Development Award from the American Heart Association and VIVA Physicians (#938814) and the Heart and Vascular Center Junior Faculty Award from Brigham and Women’s Hospital. Dr Bikdeli is a member of the Medical Advisory Board for the North American Thrombosis Forum and serves in the Data Safety and Monitory Board of the NAIL-IT trial funded by the National Heart, Lung, and Blood Institute, and Translational Science. Dr Goldhaber reports research support from Bayer, BMS, Boston Scientific, Janssen, and the National Heart, Blood, and Lung Institute (NHBLI). Dr O’Donoghue reports grants from Amgen, Novartis, AstraZeneca, Merck, and Janssen, and consulting for Amgen, NovoNordisk, Janssen, Novartis, and AstraZeneca. Dr Rosovsky reports research support ( to the institution) from BMS and Janssen. She is an advisor/consultant to Abbott, BMS, Dova, Inari, Janssen, and Penumbra; national lead investigator for the Storm-PE trial funded by Penumbra; and President of the Pulmonary Embolism Response Team Consortium. Dr Piazza reports grants from BMS/Pfizer, Janssen, Bayer, Amgen, BSC, Esperion, and 1R01HL164717-01. He has an advisory role with BSC, Amgen, BCRI, PERC, NAMSA, BMS, Janssen, and Regeneron. Dr Bertoletti reports personal fees and nonfinancial support from Aspen, Bayer, BMS-Pfizer, Léo-Pharma, MSD, and Johnson & Johnson. Dr Bates receives unencumbered salary support from the Eli Lilly Canada/May Cohen Chair in Women’s Health at McMaster University. She reports honoraria from Léo Pharma Canada, Inc., ROVI, and Sanofi, as well as payment for work from Elsevier. Dr Krumholz is associated with contracts, through Yale New Haven Hospital, from the Centers for Medicare and Medicaid Services, Janssen, Johnson & Johnson Consumer, and Pfizer; is a recipient of grants from AHA, Agency for Healthcare Research and Quality, NIH, Centers for Disease Control and Prevention; is a consulting expert for Massachusetts Medical Society, EyeDentifeye, F-prime, UpToDate, and Ensight; serves on the Data Safety Monitoring Board for Element Science; holds stocks for Element Science and EyeDentifyeye; and is a cofounder of Refactor Health, Ensight AI, and Hugo Health. Dr Monreal received an unrestricted grant for research from Sanofi and Rovi laboratories to sponsor the RIETE registry. All other authors have no disclosures to report.
Funding
The SERIOUS-PE study was supported by the Scott Schoen and Nancy Adams IGNITE Award (Dr Bikdeli) and is supported by the Mary Ann Tynan Research Scientist award (Dr Bikdeli) from the Mary Horrigan Connors Center for Women’s Health and Gender Biology at Brigham and Women’s Hospital.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.