
Abstract

Keywords
Case
A 43-year-old woman presented to the emergency department with 5 days of right calf cramping and ankle edema. She was noted to have rubor of her right lower leg associated with tenderness to palpation of the calf and pitting edema to the knee. Venous duplex ultrasonography demonstrated right popliteal, posterior tibial, and peroneal deep vein thrombosis (DVT). The patient did not report any dyspnea or chest discomfort and was not taking any medications. She denied any recent surgery or trauma but noted a 4-hour flight a week prior to presentation. She was started on a direct oral anticoagulant (DOAC) and discharged with follow-up in the vascular medicine clinic for determination of optimal duration of anticoagulation.
Overview
Determination of optimal duration of anticoagulation in a patient who has suffered venous thromboembolism (VTE) is one of the most common indications for referral to a vascular medicine provider. While provoked VTE, such as DVT or pulmonary embolism (PE) following surgery, trauma, or periods of immobility, is typically treated with time-limited anticoagulation of 3–6 months, the duration of anticoagulation after unprovoked (idiopathic) events remains the subject of debate in both the literature and clinical practice. We present the arguments for and against extended duration anticoagulation for secondary prevention after unprovoked VTE and provide a pathway for establishing a consensus approach.
Dr Piazza: Extended duration anticoagulation should be standard for unprovoked VTE
The 2016 American College of Chest Physicians (ACCP) guidelines for antithrombotic therapy for VTE disease suggest extended duration anticoagulation for patients with a first unprovoked VTE (Grade 2B) and recommend it for those with recurrent unprovoked VTE (Grade 1B), as long-term risk of bleeding is not high. 1 These recommendations are based, in part, on observational studies that show an enduring, increased risk of VTE recurrence following unprovoked VTE compared with provoked events. An analysis of the Danish National Registry of Patients demonstrated that patients with provoked or unprovoked VTE have increased mortality over 30 years of follow-up and that recurrent PE is an important long-term cause of death. 2
Many common VTE risk factors, such as obesity, comorbid medical illnesses, thrombophilia, and smoking do not resolve once anticoagulation is discontinued and contribute to this chronically increased risk of recurrence. Common recurrent acute and relapsing chronic illnesses resulting in hospitalization, such as infection, heart failure, and chronic obstructive pulmonary disease, contribute to a high burden of recurrent VTE and VTE-related complications. Long-term sequela of recurrent unprovoked DVT and PE, including the post-thrombotic syndrome and chronic thromboembolic pulmonary hypertension, respectively, are frequently preventable with long-term anticoagulation for secondary prevention and may result in substantial functional limitation, symptom burden, and health care expenditure.
Whether warfarin or a DOAC is prescribed, patients with unprovoked VTE benefit from a 60–95% reduction in recurrence with extended duration anticoagulation (Table 1). The DOACs improve safety, specifically reducing major bleeding, clinically relevant non-major bleeding, and intracranial hemorrhage, compared with warfarin, and offer important options for extended duration anticoagulation to patients and providers. The impact of extended duration anticoagulation after an initial unprovoked event is further emphasized by the observation that the risk of VTE recurrence rises promptly after discontinuation.
Major trials of anticoagulation for prevention of recurrence in patients with unprovoked VTE.
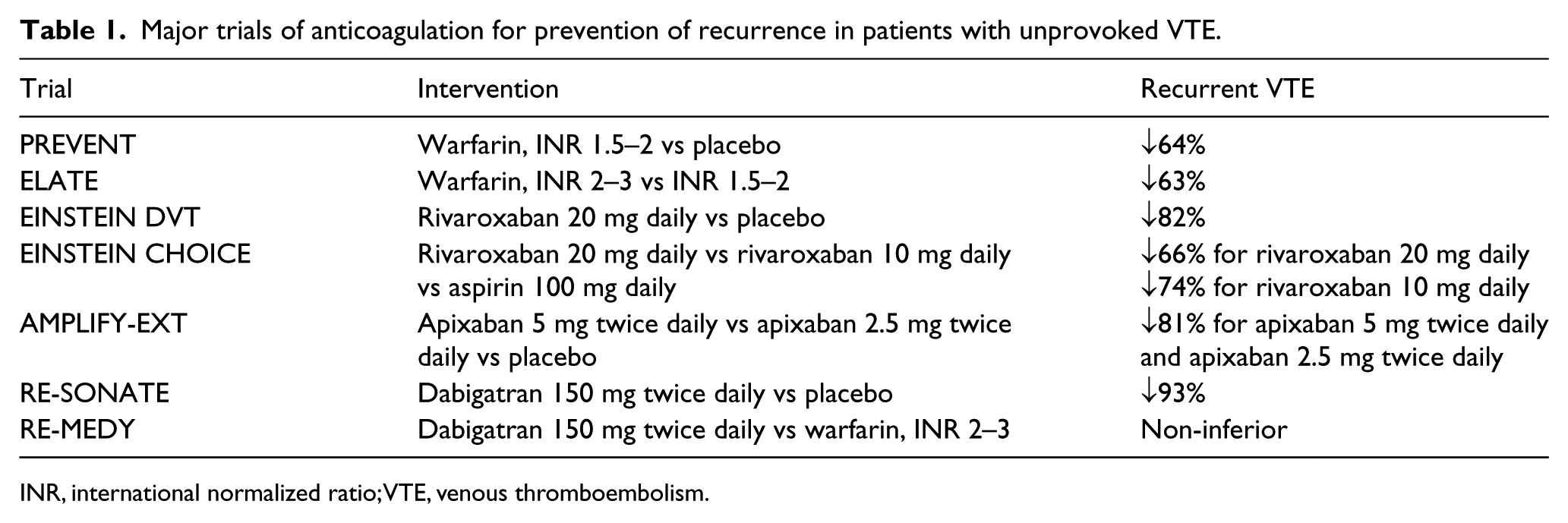
INR, international normalized ratio; VTE, venous thromboembolism.
In the most recent large randomized controlled trial of anticoagulation for secondary prevention, EINSTEIN CHOICE, extended duration anticoagulation with rivaroxaban 20 mg daily or rivaroxaban 10 mg daily, was compared with low-dose aspirin in 3396 patients with VTE. 3 In EINSTEIN CHOICE, VTE events were provoked in 60% and unprovoked in 40%. The primary efficacy outcome of symptomatic recurrent fatal or nonfatal VTE occurred in 1.5% receiving rivaroxaban 20 mg daily and in 1.2% receiving rivaroxaban 10 mg daily, compared with 4.4% receiving aspirin (hazard ratio for rivaroxaban 20 mg daily vs aspirin, 0.34; hazard ratio for rivaroxaban 10 mg daily vs aspirin, 0.26). Rates of major bleeding and clinically relevant non-major bleeding were similar in the three treatment groups. Even patients with provoked VTE, in whom the risk of VTE recurrence was generally believed to be low, extended duration anticoagulation reduced recurrent VTE.
In the AMPLIFY-EXT trial, two doses of apixaban (2.5 mg and 5 mg, twice daily) were compared with placebo in 2486 patients with unprovoked VTE who had completed 6–12 months of anticoagulation. 4 Similar to the rivaroxaban (10 mg daily) arm in EINSTEIN CHOICE, extended duration low-dose apixaban 2.5 mg twice daily was highly effective for prevention of recurrent VTE and was associated with a low risk of major and clinically relevant non-major bleeding.
Based on these randomized controlled trial data showing a balance of safety and efficacy, evidence-based clinical practice guidelines recommend extended duration anticoagulation for secondary prevention after unprovoked VTE as long as the individual patient’s risk of bleeding is not high. The recommendation for extended duration anticoagulation is also consistent with an improved pathophysiologic understanding of VTE as a chronic disease with numerous enduring risk factors. The long-term safety and efficacy of low-dose anticoagulant regimens further tip the scales in favor of extended duration anticoagulation for secondary prevention in unprovoked VTE. Accordingly, extended duration anticoagulation should be the standard for patients with unprovoked VTE in the absence of a high bleeding risk (Figure 1).
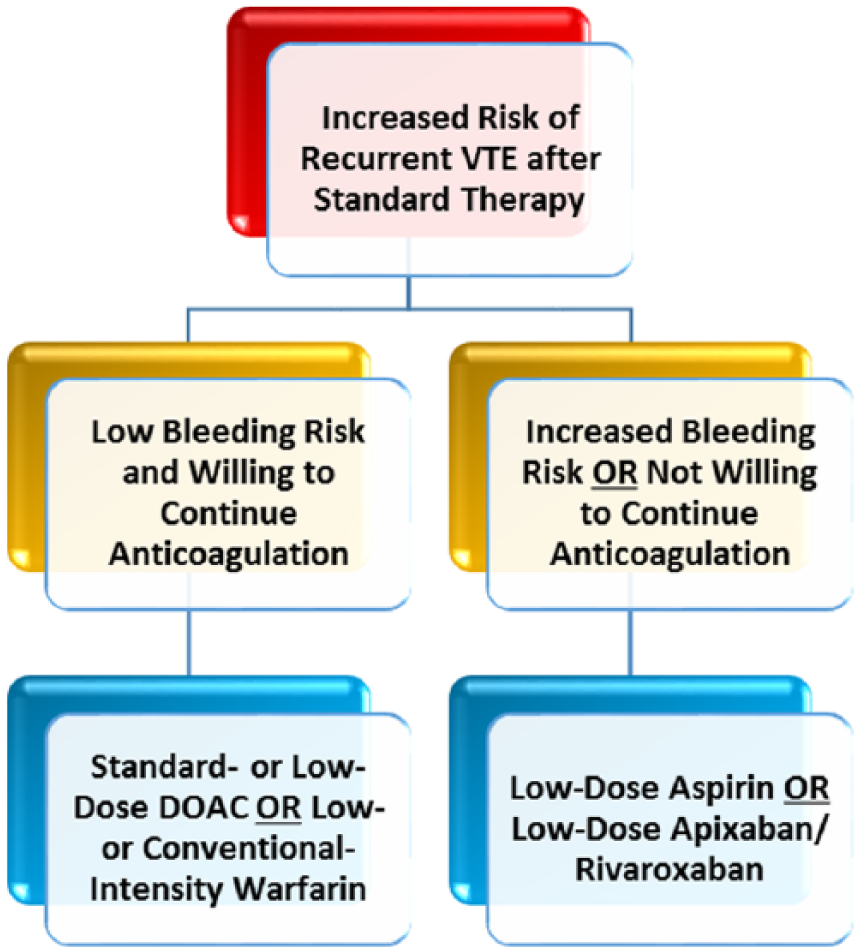
An overall algorithm for secondary prevention in patients with unprovoked VTE based on risk of recurrence and bleeding.
Dr Kanthi: Limited duration anticoagulation should be standard for unprovoked VTE
Recent randomized controlled trials show that continued treatment with anticoagulation in patients following a first episode of unprovoked DVT or PE will prevent most cases of VTE recurrence within 1–4 years (Table 1).3,4 However, the optimal duration of anticoagulation for the individual patient should be based on several factors, including: (1) the individual’s risk of recurrent thrombosis; (2) the risk of bleeding while on indefinite anticoagulation; and (3) the patient’s own personal preferences.
Recurrent VTE risk assessment
The distinction between provoked and unprovoked VTE is the major determinant in whether or not indefinite anticoagulation is recommended. Patients with verified unprovoked VTE have a higher lasting risk of recurrent VTE. However, the clinical determination of VTE as provoked or unprovoked can be imprecise. Transient risk factors, such as minor soft tissue injury, or superimposed transient and chronic risk factors may be categorized as ‘provoked’; while dehydration or antibiotic use with acute illnesses, or iliac vein compression in May–Thurner syndrome may be considered ‘unprovoked’. Not surprisingly, the categorization of VTE as provoked or unprovoked can be arbitrary, as it is difficult to assign a ‘significance factor’ to the spectrum of possible contributors to VTE. 5
As results from clinical trials are translated to clinical practice, a more precise understanding of whether a VTE is provoked or unprovoked is important in determining risk of recurrence. The International Society of Thrombosis and Haemostasis (ISTH) recently outlined recommendations to better define patients with provoked VTE by separating risk factors and comorbid conditions into ‘transient’ and ‘persistent’. 5 Transient risk factors include those associated with half the risk of VTE recurrence after anticoagulation is stopped, present up to 3 months prior to VTE, or a greater than threefold increase in risk of incident VTE, and include hospitalization, surgery, transient immobility, pregnancy and estrogen therapy. Persistent risk factors include active malignancy and chronic illnesses with a greater than twofold increase in VTE risk after stopping anticoagulation. Although not all risk factors can be classified as transient or persistent, these recommendations provide important guidance that considers the patient’s complete risk profile in determining the risk of recurrent thrombosis. 1
While the risk of VTE recurrence remains above baseline in all patients, the consequences of recurrent VTE should be considered when evaluating the benefits of long-term anticoagulation. In patients with recurrent PE, the risk of pulmonary hypertension rises 19-fold over patients with only incident PE. 6 The location of initial thrombus may predict the location of recurrence. Patients with incident PE have a higher likelihood of suffering recurrent PE and VTE-related death than patients with incident DVT. Taken together, these studies support a strategy that emphasizes prevention of recurrent PE, as the higher risk event than DVT.
Three risk scoring algorithms, HERDOO2, Vienna score, and DASH, have been developed and prospectively validated to inform decisions about anticoagulation based on likelihood of recurrent VTE.7–9 These risk prediction models incorporate key factors involved in VTE recurrence. The ‘Men and HERDOO2’ score factors sex, signs of post-thrombotic syndrome, elevated d-dimer, obesity and age into a risk prediction tool. Men, and women who had two or more risk factors (‘high risk’), had a major VTE recurrence risk of 8.1% (confidence interval (CI) 5.2–11.9%) if anticoagulation was discontinued compared to 1.6% (CI 1.1–2.3%) in patients continued on anticoagulation. Interestingly, women with one or fewer risk factors (‘low risk’) who discontinued anticoagulation had a VTE recurrence risk of 3.0 (CI 1.8–4.8%). Based on this trial, the authors recommended a limited duration of anticoagulation in low-risk women with first unprovoked VTE. The DASH and Vienna scoring models similarly incorporate risk factors including d-dimer to estimate a spectrum of recurrence risk for patients with first unprovoked VTE, although these were more effective in younger patients. In patients at low risk of bleeding from anticoagulation, risk stratification tools can help further identify those for whom the assessment of risks and benefits is not in favor of indefinite anticoagulation.
Risk of indefinite anticoagulation
Several risk assessment tools for bleeding exist for patients with VTE on anticoagulation. 10 However, they have not gained wide adoption in clinical practice as their validation is incomplete. While rates of major bleeding in the AMPLIFY-EXT and EINSTEIN CHOICE trials were similar in patients treated with DOAC, aspirin or placebo, the follow-up period in these studies was approximately 12 months.3,4 Prospective studies on the risk of bleeding in patients with VTE treated with anticoagulants beyond 5 years have not been performed. The case fatality rates of recurrent VTE are highest in the period following the initial event and decline with time, while the case fatality rates associated with major bleeding may decline at first but rise as patients age and develop stochastic illnesses.
Shared decision-making
Recommending lifelong anticoagulation to patients for prevention of recurrent VTE introduces variables that will significantly influence efficacy of the treatment. These include patient preferences and perceptions about the value placed on prevention of recurrent VTE versus risk of major bleeding complications, choice of anticoagulation agents based on monitoring versus ease of dosing and likelihood of adherence. These require well-designed and validated shared decision-making tools that can help identify where evidence-based medicine and patient value systems converge. Shared decision-making aids have been used for long-term thromboembolic prevention in patients with atrial fibrillation, but these are limited for patients with VTE.
Summary: A consensus approach to the evidence and the role of patient and provider preference
The risk of long-term VTE recurrence in patients after an unprovoked DVT or PE persists after anticoagulation is stopped. Recent clinical trials and clinical practice guidelines support a long-term anticoagulation strategy in patients with a first unprovoked VTE to prevent recurrent events in patients who are at low risk of bleeding complications. Despite differences in our two approaches, both strategies focus on balancing the risk of recurrent VTE and the complication of bleeding from extended duration anticoagulation. We favor a strategy that engages both patient and provider in shared decision-making regarding duration of anticoagulation and the optimal anticoagulant and dosing, followed by reassessing the appropriateness of anticoagulation at regular intervals (Figure 2).
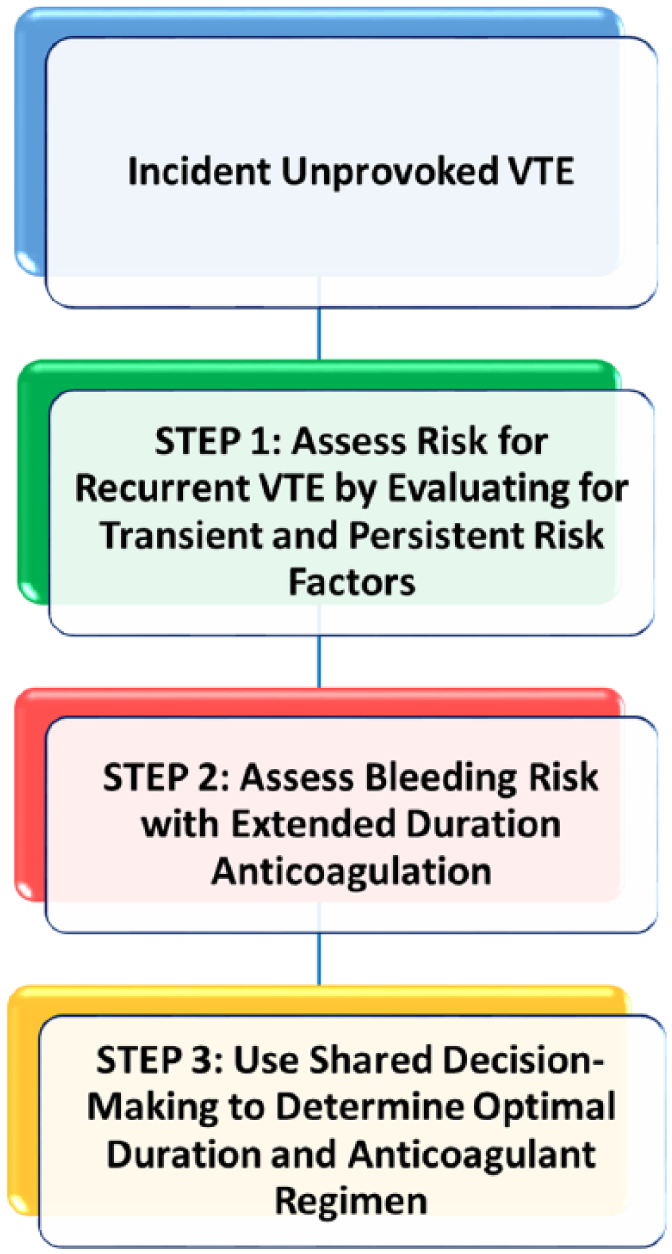
A consensus approach to decisions about anticoagulation for secondary prevention in patients with VTE.
Footnotes
Declaration of conflicting interests
The authors declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: Dr Kanthi has received research grant support from NHLBI, Jobst/American Venous Forum Foundation, and is a consultant for Wells Fargo. Dr Piazza has received research grant support from EKOS, a BTG International Group company, Bristol-Myers Squibb, Daiichi-Sankyo, and Janssen.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.