
Abstract
Introduction:
This study compared the effectiveness of customized graduated elastic compression stockings (c-GECS) based on individual lower-leg parameter models with standard graduated elastic compression stockings (s-GECS) in patients with occupational edema (OE).
Methods:
A single-blind, randomized controlled trial was conducted with 70 patients with OE, randomly assigned to the c-GECS or s-GECS group. Follow-up assessments were performed at 1 and 3 months. Primary outcomes comprised visual analog scale scores (1–10) for lower-limb symptoms and comfort level of GECS. Secondary outcomes included GECS usage duration, calf volume, and interface pressure at B and C points (B: minimal ankle circumference point; C: maximum calf circumference point).
Results:
Both groups exhibited significant improvements in pain, heaviness, and swelling symptoms at the 1- and 3-month follow up. At the 3-month follow up, the c-GECS group showed significantly superior improvement in symptoms. Comfort assessment revealed that c-GECS (16.2 ± 2.9) provided significantly greater comfort than s-GECS (13.6 ± 3.2) (p < 0.001). However, the two groups showed no significant difference in GECS wear duration. At 3 months, the c-GECS group showed superior maintenance of stocking tension at point B (p = 0.018). Both types of GECS significantly reduced calf volume at both time points, with no notable difference between the groups.
Conclusion:
c-GECS effectively alleviated pain, heaviness, and swelling symptoms in patients with OE. Although c-GECS did not exhibit a clear advantage in reducing calf volume as compared to s-GECS, it provided more stable and enduring pressure, enhanced the overall fit of GECS, and improved comfort during wear.
Keywords
Introduction
After prolonged periods of sedentary or standing work, individuals with good health may experience occupational edema (OE), a condition commonly observed in various professional groups, including doctors, teachers, and lumberjacks. Despite the absence of apparent reflux in the ultrasound scans of patients with OE, these patients often report concurrent sensations of fatigue, leg heaviness, and discomfort. 1 Previous studies have extensively investigated the efficacy of graduated elastic compression stockings (GECS) in preventing and managing OE.2–4 The pressure exerted by GECS is thought to amplify the effectiveness of the calf muscle pump. Nonetheless, many individuals frequently express dissatisfaction with GECS by citing tightness and discomfort as pronounced concerns. 5 Moreover, because of differences in calf muscle size, body fat percentage, height, and weight among various patients, the shapes of their calves also vary. Some individuals may experience challenges with standard GECS (s-GECS) as these stockings may not appropriately conform to the contours of their calves, thereby exacerbating the discomfort associated with GECS.
Recently, a novel approach has emerged that involves the production and in vitro evaluation of customized GECS (c-GECS) based on parametric modeling of human calves.6,7 Despite the lack of extensive clinical application reports, this novel approach has the potential to enhance compliance and comfort with the use of GECS, thereby improving treatment outcomes. Hence, the present study aimed to compare s-GECS and c-GECS in terms of patient comfort and effectiveness in treating OE.
Methods
The study was registered with the Chinese Clinical Trial Registry (registration number: ChiCTR2100042894). The study protocol was approved by the Research Ethics Committee of Beijing Chaoyang Hospital, affiliated with Capital Medical University (Approval Number: 2020-Sci-7). Informed consent was obtained from all patients prior to inclusion in the study. The patients could withdraw from the study at any time without any obligation to provide reasons for their decision.
Participant selection
Participants were enrolled at the Vascular Surgery Clinic of Beijing Chaoyang Hospital from June 2022 to August 2022. The following inclusion criteria were considered: (1) experiencing discomfort in the lower limbs after a day’s work; (2) staying standing or sitting throughout their work shift; (3) age between 18 and 65 years; and (4) provision of signed informed consent. Exclusion criteria were as follows: (1) patients with venous diseases and other causes of edema, including cardiac, kidney, and liver-related diseases and orthopedic disorders, which cause calf pump dysfunction; (2) patients with contraindications to the use of GECS, such as severely impaired arterial blood flow in the extremities (ankle–brachial index < 0.5), limb deformity, acute calf dermatitis, confirmed hypersensitivity to GECS materials, severe diabetic neuropathy with sensation loss or microangiopathy, and severe heart failure (New York Heart Association class IV); (3) patients currently using diuretic medication; and (4) pregnant patients. Before enrollment, each patient underwent color duplex ultrasound examination of the lower limb to exclude venous pathophysiology. The duplex ultrasound was conducted with patients in a standing position. The criteria for abnormal reflux were defined as follows: reflux duration > 500 ms in both superficial and deep calf veins, reflux duration > 1000 ms in the femoral-popliteal veins, and outward flow duration > 350 ms in perforating veins. Patients exhibiting pathological reflux according to these criteria were excluded from the study. Most of the patients in this study were operating room nurses and surgeons, totaling 41 individuals (58.6%). Additionally, there were seven teachers (10.0%), nine sales professionals (12.9%), eight office employees (11.4%), and five individuals (7.1%) in other occupations.
Randomization and blinding
To ensure unbiased results, patients were randomly assigned to treatment groups in a 1:1 ratio using a list randomizer (http://www.random.org/lists/). The patients were unaware of their assigned group. To maintain blinding and prevent performance bias, identical stockings were used, which were produced from the same material by a single manufacturer.
Description of s-GECS and c-GECS
Group A received off-the-shelf, knee length, Class 2 GECS (Zhende Medical Supplies Co., Ltd, Shaoxing, Zhejiang province, China) with a compression range of 23–32 mmHg at the ankle level. The choice of s-GECS depended on the circumference at points B and C (B: minimal ankle circumference point; C: maximum calf circumference point). Group B received c-GECS (Zhende Medical Supplies Co., Ltd) with the same specifications (knee length, Class 2, 23–32 mmHg at the ankle level), which was produced using identical materials and industry standards (RAL-GZ387). The c-GECS were fabricated by circular knitting. Nylon Lycra-wrapped yarns with different fineness and elasticity were used to produce GECS with varying compression levels. The key factor that differentiated the two types was that c-GECS were generated using a parametric model based on the patient’s calf measurements performed with a 3D laser scanner.
Study protocol
After enrollment, the following baseline information was collected, including age, sex, body mass index (BMI), family history of chronic venous disease, and prolonged standing. Throughout the study, the patients were encouraged to maintain their usual lifestyle. Patients in both groups were instructed to wear the GECS in the morning before getting out of bed and to remove them at night before going to sleep. If the stockings needed to be cleaned during the wearing period, only room temperature water was allowed for cleaning, and the use of chemical detergents or forceful stretching of the stockings during the cleaning process was prohibited. The leg with more severe symptoms was designated as the index leg. The outcomes of the trial were measured based on the visual analog scale (VAS, 1–10) for symptoms, duration of stocking usage, the Wearable Assessment Scale for comfort of GECS, calf volume, and interface pressure (IP). Owing to the influence of circadian rhythms, data collected at different times of day may vary. Measurements were performed in a quiet room with a constant temperature of approximately 24°C at the same time of day (between 6 p.m. and 7 p.m.). Study visits were scheduled at baseline, month 1, and month 3. During each visit, the above-mentioned five follow-up parameters were recorded. The calf volume was also measured on the morning of the first day of the experiment, which allowed comparison with the volume measured in the afternoon.
Outcome measures
The lower-limb symptoms in patients were evaluated with the VAS score. Common symptoms reported by patients with OE include heaviness, pain, swelling, night cramps, burning sensation, restless legs, throbbing, and a tingling sensation.1,8 The present study specifically focused on the four most frequently reported symptoms obtained from the preliminary questionnaire: pain, heaviness, swelling sensation, and burning sensation. The daily duration of GECS usage for each patient during each follow up was accurately recorded. To comprehensively evaluate the comfort of GECS, a Wearable Assessment Scale (Table S1) was methodically designed; this scale systematically assessed fitting, pressure distribution, maintenance of position stability, and ease of donning and doffing, with scores assigned from 1 to 5 for each aspect and a maximum total score of 20. The scale was completed at the end of the follow-up period. IP between the GECS and the skin was measured at points B and C with the participants in the standing position. A pneumatic pressure transducer connected to a pressure probe (Department of Electronic Engineering, Tsinghua University, Beijing, China) was used. A 3D laser scanner (Easy Max Intelligent Technology Co., Ltd, Wuxi, Jiangsu Province, China) was used to assess leg edema. To ensure consistent measurement conditions, the patients were instructed to position their legs perpendicular to the ground during each assessment. Calf volume was measured between the level of the minimum ankle girth and the level of the tibial tuberosity below the knee; the same measurement site was used at different time points. The accuracy and reliability of the device were validated previously. 9
Statistical analysis
A priori power calculations were based on a preliminary study in which the mean VAS score for heaviness was 2.4/10 with s-GECS. Assuming that the use of c-GECS would reduce this score to 1.5, and considering a SD of 1 for both groups, a sample size of 28 individuals per group was determined to be sufficient to achieve adequate power. Considering potential patient dropouts, we enrolled 70 patients, with 35 patients allocated to each group.
GraphPad Prism 9 (GraphPad Inc., San Diego, CA, USA) was used to create graphs. SPSS Statistics, version 26 (IBM Corp., Armonk, NY, USA) was used for statistical analyses. The normality of continuous data was assessed using the Shapiro–Wilk test, and homogeneity of variance was tested using Levene’s test. Independent sample t-test or Mann–Whitney U-test was used for comparing continuous data between the groups. Categorical data were compared using the chi-squared test or Fisher’s exact test, depending on the sample size and data distribution. For data with normal distribution, within-group repeated measurement data were analyzed using repeated-measures analysis or a generalized estimating equation model. Spearman’s rank correlation test was used to assess the correlation between two sets of nonnormally distributed data.
Results
A total of 70 patients were enrolled in this randomized controlled trial, all of whom successfully completed a 3-month follow up (Figure 1). The average age of the patients was 41.8 ± 8.2 years, and the two groups showed no significant differences in baseline characteristics (Table 1).
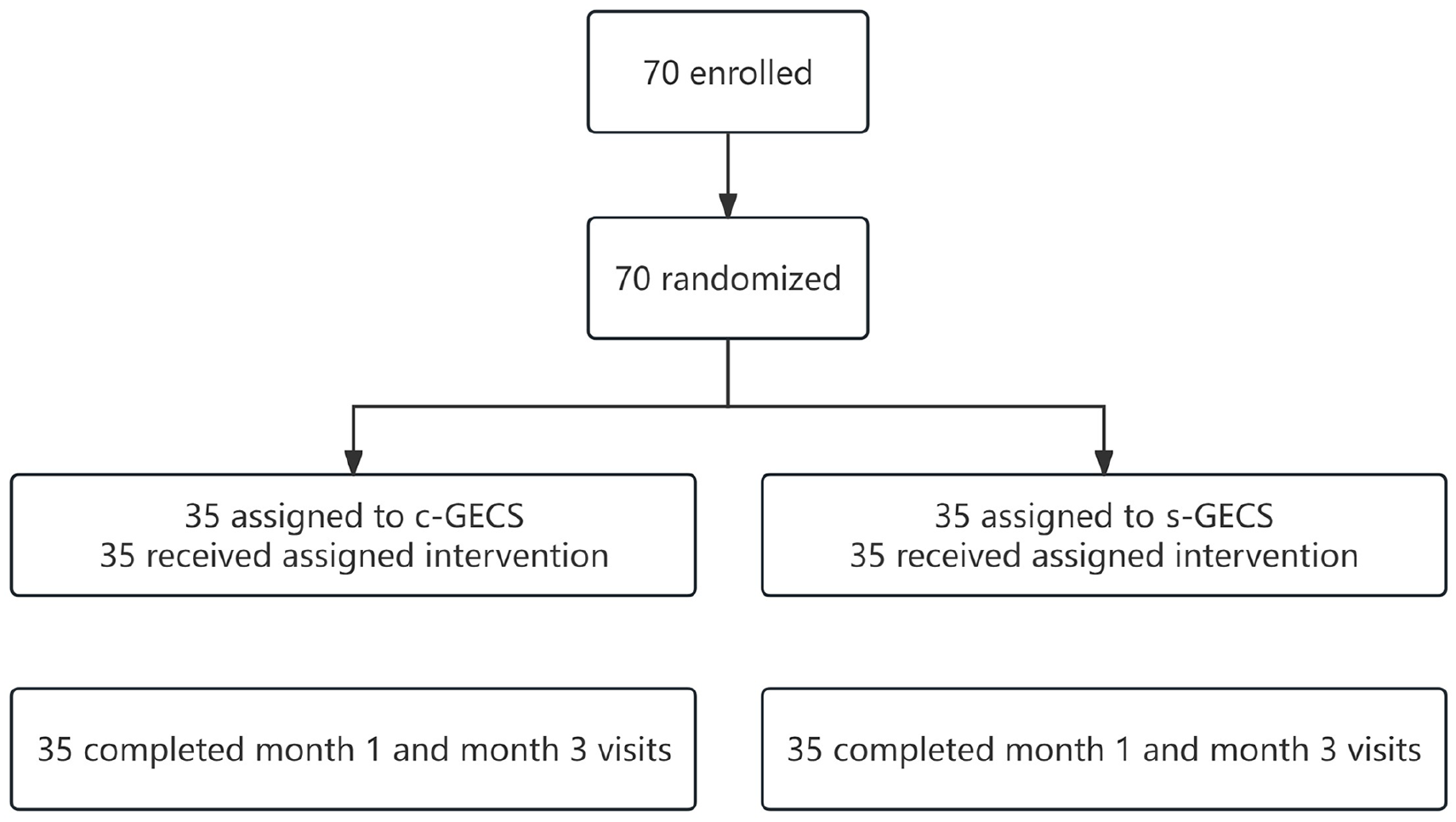
CONSORT flowchart showing the number of patients during the phases of the study.
Participant characteristics.

BMI, body mass index; c-GECS, customized graduated elastic compression stockings; s-GECS, standard graduated elastic compression stockings.
Lower-limb symptoms
Table 2 presents the VAS scores for pain, heaviness, swelling sensation, and burning sensation in patients with OE. During the 1-month and 3-month follow up, both groups showed significant improvements in patients’ symptoms of pain, heaviness, and swelling (p < 0.001). At the 1-month follow up, no significant differences in symptom improvement were observed between the two groups (heaviness: median [IQR] 1 [0–2] vs 1 [0–3], p = 0.532; pain: 1 [0–2] vs 1 [0–2], p = 0.065; swelling: 0 [0–1] vs 1 [0–2], p = 0.249). However, at the 3-month follow up, the c-GECS group exhibited significantly better improvement in symptoms as compared to the s-GECS group (heaviness: 1 [0–2] vs 2 [1–3], p = 0. 012; pain: 1 [0–2] vs 2 [1–3], p < 0.001; swelling: 1 [0–1] vs 2 [0–2], p = 0.006) (Figure 2). Notably, the burning sensation in the lower limbs of the patients showed no significant improvement (p = 0.129). A noteworthy finding is that four and five patients in the c-GECS and s-GECS groups, respectively, did not experience a burning sensation at the time of enrollment but developed symptoms after wearing elastic stockings.
Visual analog scale scores.
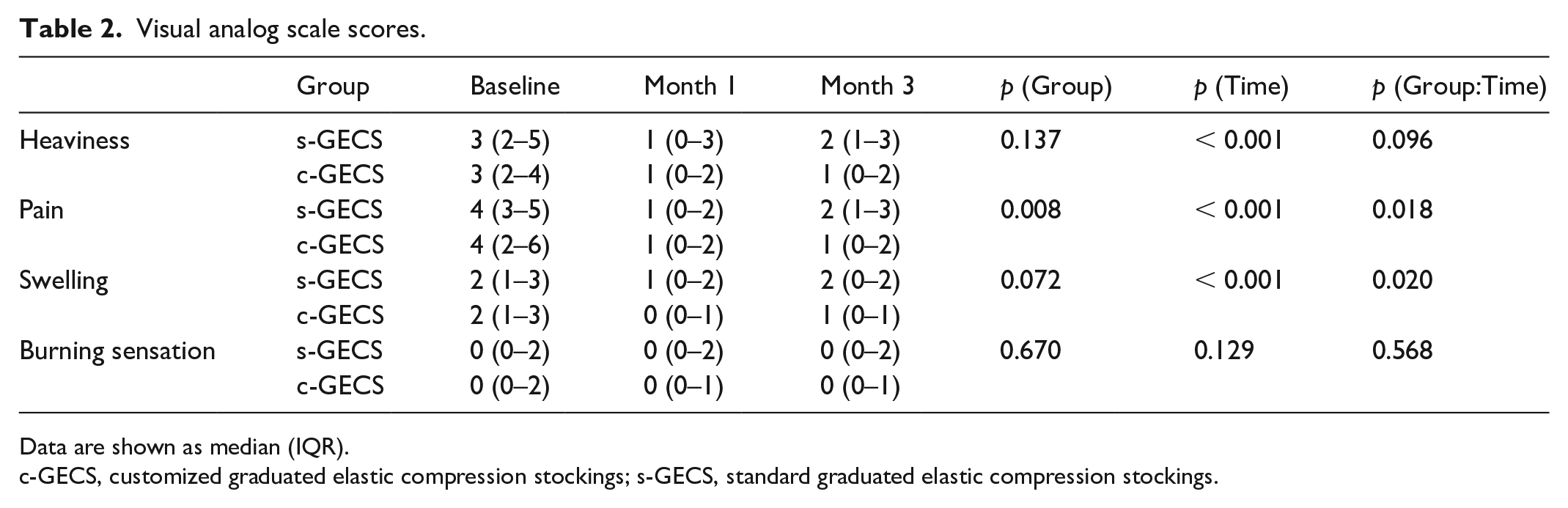
Data are shown as median (IQR).
c-GECS, customized graduated elastic compression stockings; s-GECS, standard graduated elastic compression stockings.
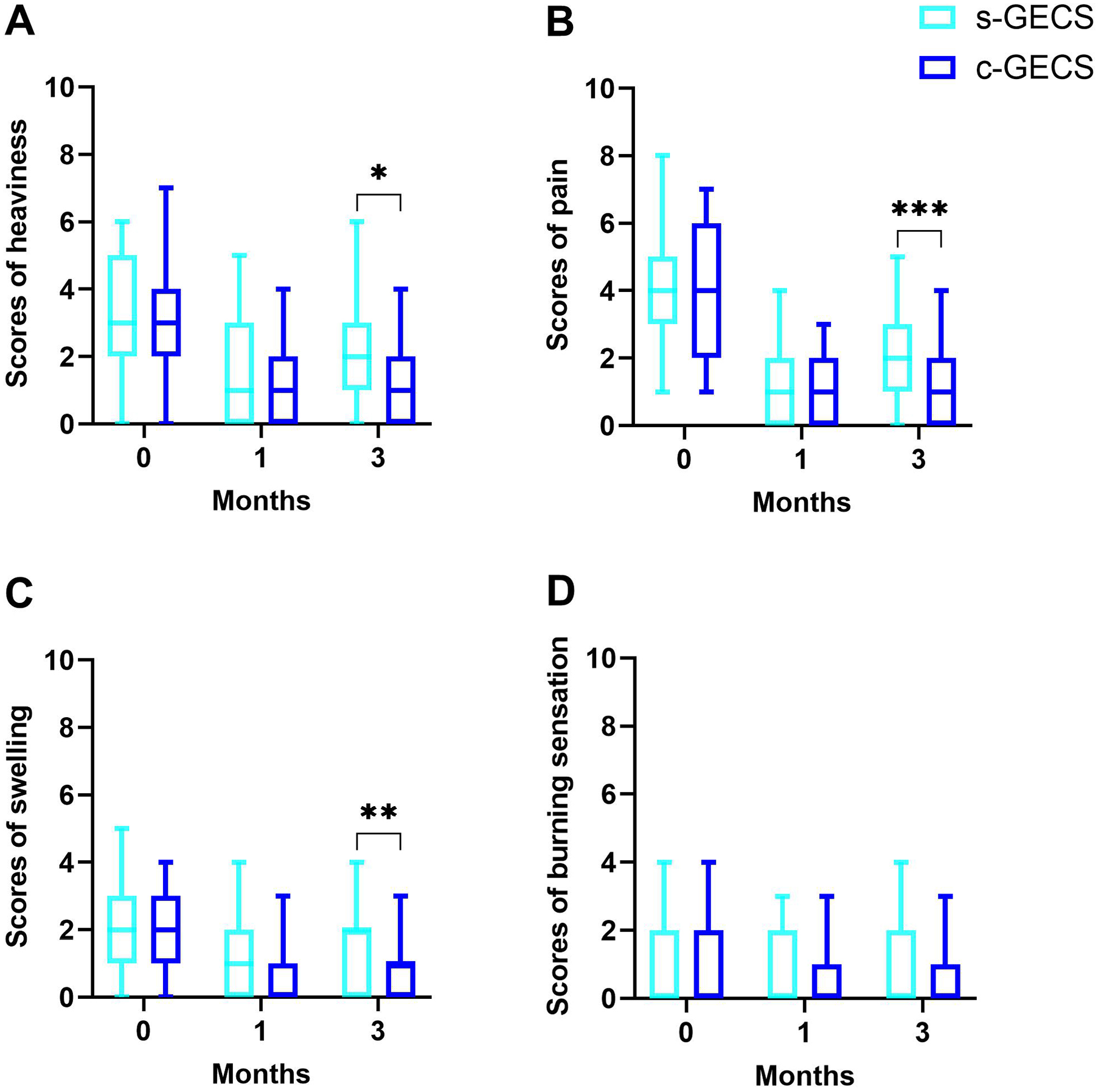
Changes in scores of
Duration of stocking use
Table 3 presents the duration of GECS wear for both groups. Both groups showed no significant differences in the duration of elastic stocking wear during the 1-month (p = 0.895) and 3-month (p = 0.767) follow up. At month 1, the improvement in the symptoms of heaviness and swelling sensation showed a positive correlation with the duration of elastic stocking wear. At the 3-month follow up, the improvement in the symptoms of heaviness, pain, and swelling sensation was positively correlated with the duration of elastic stocking wear (Table S2).
Duration of stocking use.
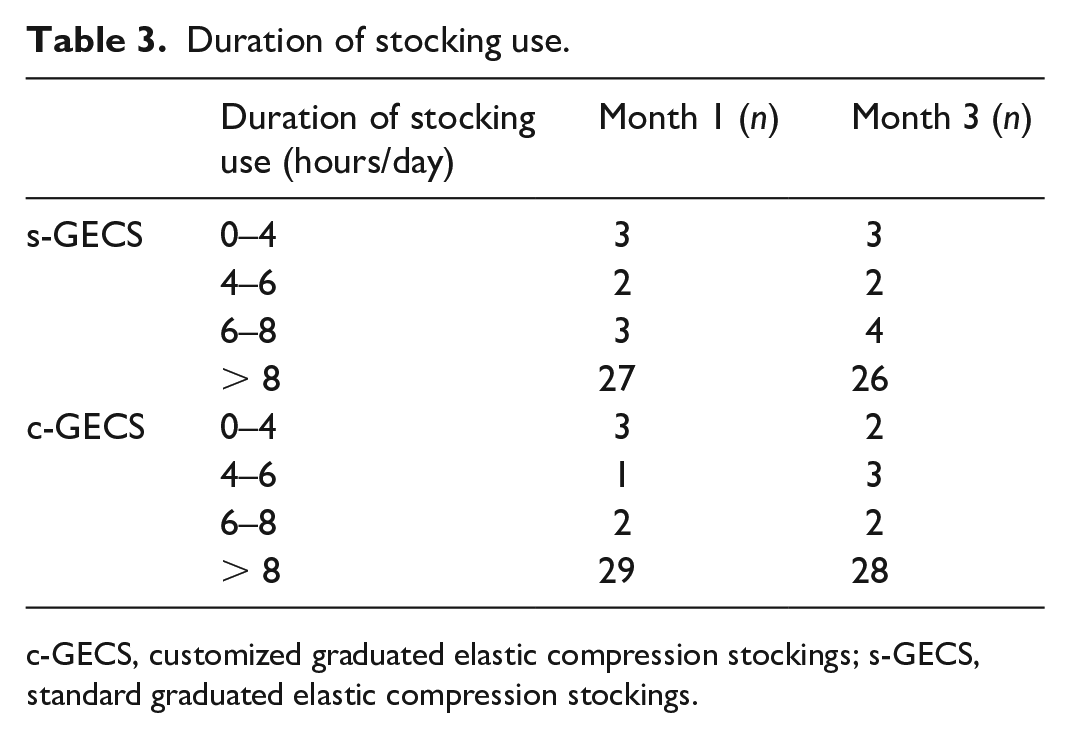
c-GECS, customized graduated elastic compression stockings; s-GECS, standard graduated elastic compression stockings.
Comfort
The c-GECS group demonstrated significantly superior comfort compared to the s-GECS group (16.2 ± 2.9 vs 13.6 ± 3.2, p < 0.001).
Interface pressure (IP)
IP measurements were conducted after the application of both types of GECS (Table 4). At baseline, no significant differences were observed in pressure at points B and C between the two stockings (Figure 3). However, a notable distinction in variance emerged, with s-GECS displaying considerably larger variances than c-GECS at points B and C, yielding F-values of 10.22 (p = 0.002) and 5.97 (p = 0.017), respectively. In the s-GECS group, the pressure at point B was higher than the RAL-GZ387 standard in eight patients. In the c-GECS group, the stocking pressure exceeded the standard only in one patient.
Outcome variables.
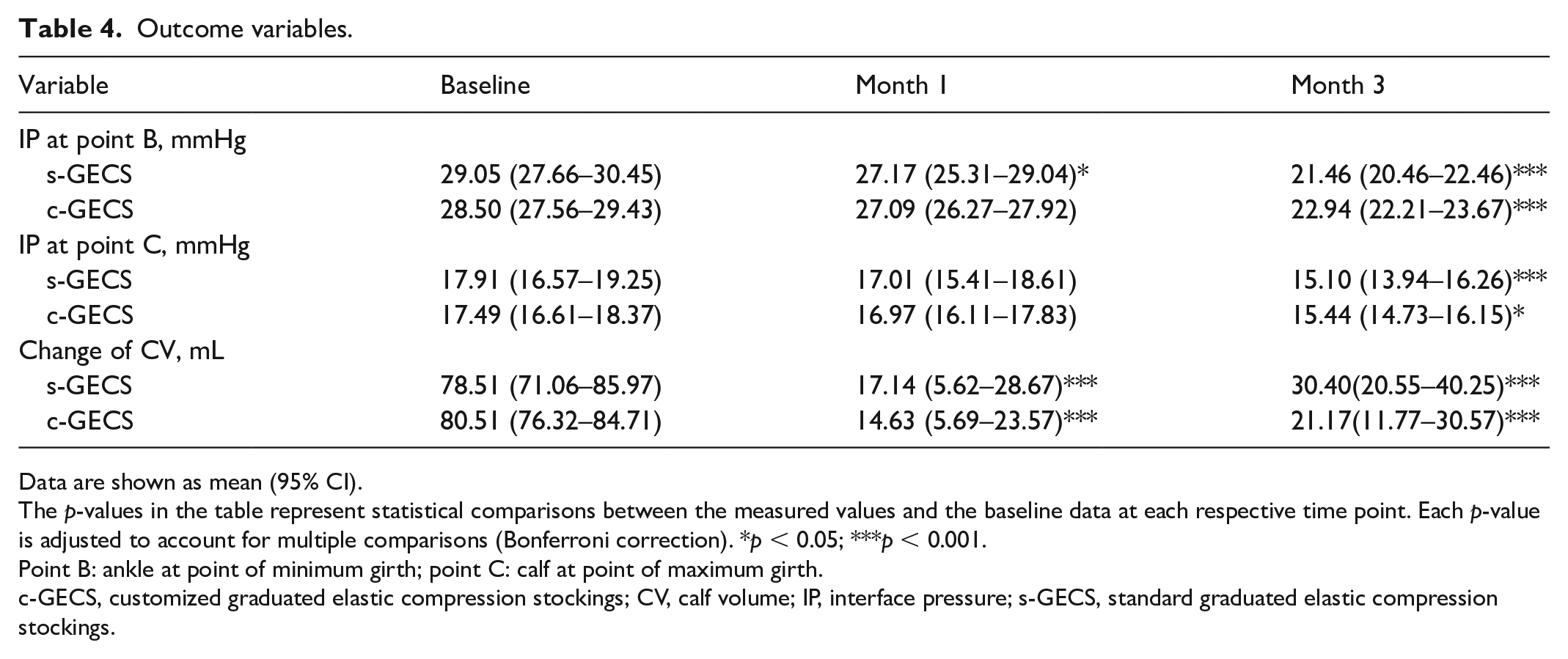
Data are shown as mean (95% CI).
The p-values in the table represent statistical comparisons between the measured values and the baseline data at each respective time point. Each p-value is adjusted to account for multiple comparisons (Bonferroni correction). *p < 0.05; ***p < 0.001.
Point B: ankle at point of minimum girth; point C: calf at point of maximum girth.
c-GECS, customized graduated elastic compression stockings; CV, calf volume; IP, interface pressure; s-GECS, standard graduated elastic compression stockings.
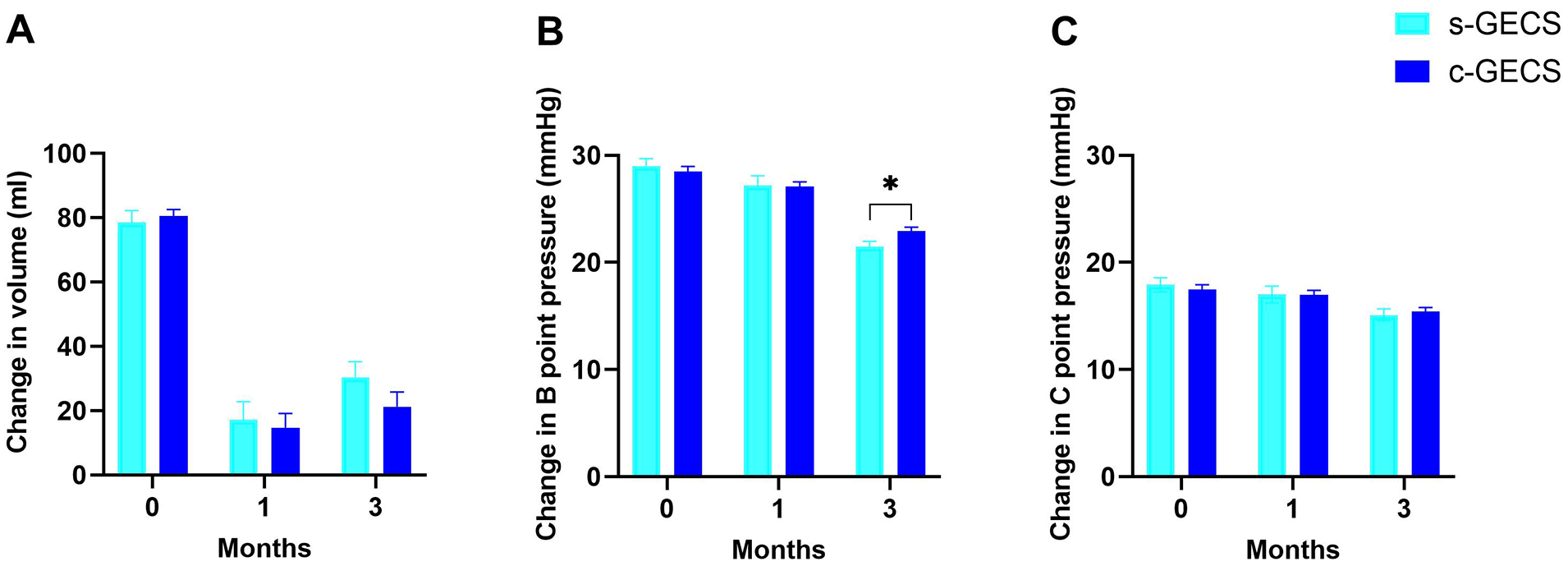
Changes in
During the 1-month follow up, both the c-GECS (27.1 ± 0.7 vs 28.5 ± 0.6, p = 0.004) and s-GECS (27.2 ± 0.7 vs 29.1 ± 0.6, p < 0.001) groups showed a significant decrease in pressure values at point B, whereas the pressure values at point C remained stable. At the 3-month follow up, both groups showed a noticeable decrease in pressure values at points B and C. In the inter-group comparison, at 1 month, no difference was observed in pressure values at point B between the two groups (27.2 ± 0.7 vs 27.1 ± 0.7, p = 0.939); however, at 3 months, the c-GECS group exhibited better maintenance of tension in the GECS at point B compared to the s-GECS group (22.9 ± 0.4 vs 21.5 ± 0.4, p = 0.018) (Figure 3).
Calf volume
For both types of GECS, a significant reduction in calf volume was observed at both time points compared to that at the baseline (Table 4). However, the two groups showed no significant difference in volume reduction at follow-up month 1 and month 3. The interaction effect between time and group was not statistically significant (p = 0.311).
Discussion
Occupational edema is a common workplace-related issue, with a prevalent occurrence of various symptoms such as leg pain, swelling, and a sense of heaviness among the majority of the population. Current treatment measures include pharmaceutical interventions, neuromuscular electrical stimulation, 10 active compression bandages, and GECS with different pressure levels. 11 Despite limited research, GECS have shown distinct advantages in terms of effectiveness, safety, and health economics. 4 However, because of individual differences and insufficient precision in matching GECS with the patient’s leg shape, there is considerable variability in the actual pressure and pressure distribution during GECS wear. This leads to suboptimal comfort, low compliance, and challenges in achieving the expected therapeutic effects with GECS. 12 To address this issue, c-GECS based on a lower-limb parameter model may offer a promising solution. c-GECS can better adapt to the patient’s leg shape, effectively maintain gradient pressure, enhance patient comfort, and consequently improve treatment outcomes. Our previous studies have already validated the efficacy of c-GECS in patients with venous insufficiency. 13
Similar to the studies conducted by Kakkos et al., 8 Quilici Belczak et al., 11 Blazek et al., 14 and others, we observed a positive effect of GECS on alleviating pain, heaviness, and swelling symptoms in patients. Compared to other studies, our present research involved a longer follow-up period, thus providing a more detailed examination of the efficacy at different follow-up time points. At the 1-month follow up, both types of GECS showed similar improvements in symptoms; however, at the 3-month follow up, despite no significant difference in the duration of stocking use between the two groups, c-GECS continued to demonstrate superior effectiveness. This may be attributed to better conformance of c-GECS to the patient’s leg contour and more effective maintenance of the gradient pressure of the stockings. Although s-GECS were selected based on the strict criteria for the diameter of the patient’s calf and ankle, in practical use, they may not conform well to the patient’s leg shape or maintain the gradient pressure effectively compared to c-GECS. Nearly one-third of patients had pressure values exceeding 32 mmHg at point B, which led to a higher variance in pressure for the s-GECS group than for the c-GECS group. This might result in uneven distribution of compression, local discomfort, and deformation of stockings during activity, leading to suboptimal symptom improvement for some patients. IP measurements indicated that c-GECS had a certain advantage in maintaining pressure. At the 3-month follow up, the s-GECS group exhibited a faster decline in IP, possibly due to mismatches between the elastic material and the patient’s leg shape, resulting in relatively poor pressure maintenance in s-GECS. Moreover, the burning sensation symptoms of the patients showed no significant improvement with both types of GECS. Factors such as a low proportion of patients with itching symptoms in the study population and potential localized allergies and itching induced by wearing GECS could have contributed to this observation. In clinical practice, the use of better materials for producing GECS may help address these issues.
In addition to symptom improvement, the comfort achieved after wearing GECS is a crucial indicator for evaluating GECS. Compliance with wearing GECS has been a challenge in clinical practice because of difficulties in wearing and discomfort after wearing, 15 with reported compliance rates as low as 33%. 12 In our present study, c-GECS demonstrated better comfort due to better adaptation to the patient’s leg shape, more uniform pressure distribution, and better stability during movement. Although our study showed differences in comfort between the two groups, compliance with wearing GECS did not show a significant difference. This might be because the requirement for daily wear of GECS during working hours was mandated as part of our study design. Further real-world research is required to investigate the role of c-GECS in improving compliance among patients with OE.
Regarding the reduction in edema, the change in calf volume after wearing GECS in our present study was relatively small compared to that reported by Mosti and Partsch. 2 This difference may be attributed to the use of water displacement during volume measurement in the study of Mosti and Partsch, which includes swelling of the entire calf and foot. In the study of Blazek et al., the change in calf volume was only approximately 20 mL. 14 This smaller change might be due to the use of Class I GECS and the inclusion of some participants with healthy lower limbs. In the present study, although both types of GECS improved edema in the lower extremities, no significant difference was observed between the two groups at various time points. A previous study suggested that the severity of lower-limb edema does not have a direct linear relationship with subjective discomfort symptoms. 16 Moreover, although some patients experienced significant improvement in subjective symptoms after wearing GECS, their edema did not significantly improve. The specific mechanisms underlying OE are yet to be fully understood, and patients may manifest a variety of symptoms. Some features of the syndrome reflect an emotional disorder, and others mirror venous insufficiency. 1
Although c-GECS showed superior performance in pressure distribution and comfort in OE treatment, thereby presenting a novel approach to treat OE, cost-effectiveness analysis remains crucial in clinical practice for healthcare providers and decision-makers to determine the optimal treatment method. Though there is no significant difference in material costs between custom and standard GECS, the production and labor costs of c-GECS are approximately 25–30% higher due to the need for individual design and production. The relatively high production cost of c-GECS, the need for a prewearing 3D scan of the lower limbs, and the waiting time of nearly 2 weeks for customization could cause some inconvenience in implementing routine use of c-GECS in clinical application.
c-GECS can be obtained either through hospitals or directly from manufacturers that offer personalized services. As long as the parameters are provided, c-GECS can be easily acquired worldwide. In cases where 3D scanning is unavailable, manual measurements with a soft ruler can be taken, although they may be less accurate compared to 3D scanning.
This study has some limitations. First, the sample size is relatively small, which potentially limited the generalizability of the results; a larger cohort could provide more robust conclusions. Second, the majority of participants in this study were hospital healthcare workers, which potentially resulted in poor representativeness of the overall population. Third, variations in work intensity, posture, and standing time among different patients with OE may influence the study results and require further investigations.
Conclusion
The customized graduated elastic compression stockings (c-GECS) based on individual lower-limb parameter models effectively alleviated pain, heaviness, and swelling symptoms in patients with occupational edema. Although c-GECS did not exhibit a clear advantage in reducing calf volume as compared to standard graduated elastic compression stockings (s-GECS), it provided more stable and enduring pressure, enhanced the overall fit of elastic compression stockings, and improved comfort during wear.
Supplemental Material
sj-pdf-1-vmj-10.1177_1358863X241290801 – Supplemental material for Mid-term effect of customized graduated elastic compression stockings for managing occupational edema: A randomized controlled trial
Supplemental material, sj-pdf-1-vmj-10.1177_1358863X241290801 for Mid-term effect of customized graduated elastic compression stockings for managing occupational edema: A randomized controlled trial by Sheng-Xing Wang, Wen-Tao Yang, Zhen-Yi Jin, Jia-Hao Wen, Hua-Liang Ren, Ying Xiong, Xiao-Ming Tao and Chun-Min Li in Vascular Medicine
Supplemental Material
sj-pdf-2-vmj-10.1177_1358863X241290801 – Supplemental material for Mid-term effect of customized graduated elastic compression stockings for managing occupational edema: A randomized controlled trial
Supplemental material, sj-pdf-2-vmj-10.1177_1358863X241290801 for Mid-term effect of customized graduated elastic compression stockings for managing occupational edema: A randomized controlled trial by Sheng-Xing Wang, Wen-Tao Yang, Zhen-Yi Jin, Jia-Hao Wen, Hua-Liang Ren, Ying Xiong, Xiao-Ming Tao and Chun-Min Li in Vascular Medicine
Footnotes
Conflict of interest
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
This work was supported by grants from Beijing Chaoyang Hospital, Capital Medical University Science and Technology Innovation Fund (grant no.: 21kcjj-11), and the Innovation and Technology Commission, The Government of the Hong Kong Special Administrative Region (grant no.: ITP/041/19TP).
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.