
Abstract

Keywords
What is erythromelalgia?
Erythromelalgia (also known as erythermalgia) is a rare condition in which the feet and/or hands intermittently turn bright red, hot, and painful, especially with exposure to heat. ‘Erythros’ means red, ‘melos’ means extremity (limb), and ‘algia’ means pain. Figure 1 summarizes the symptoms, which were first described in the 1870s. 1
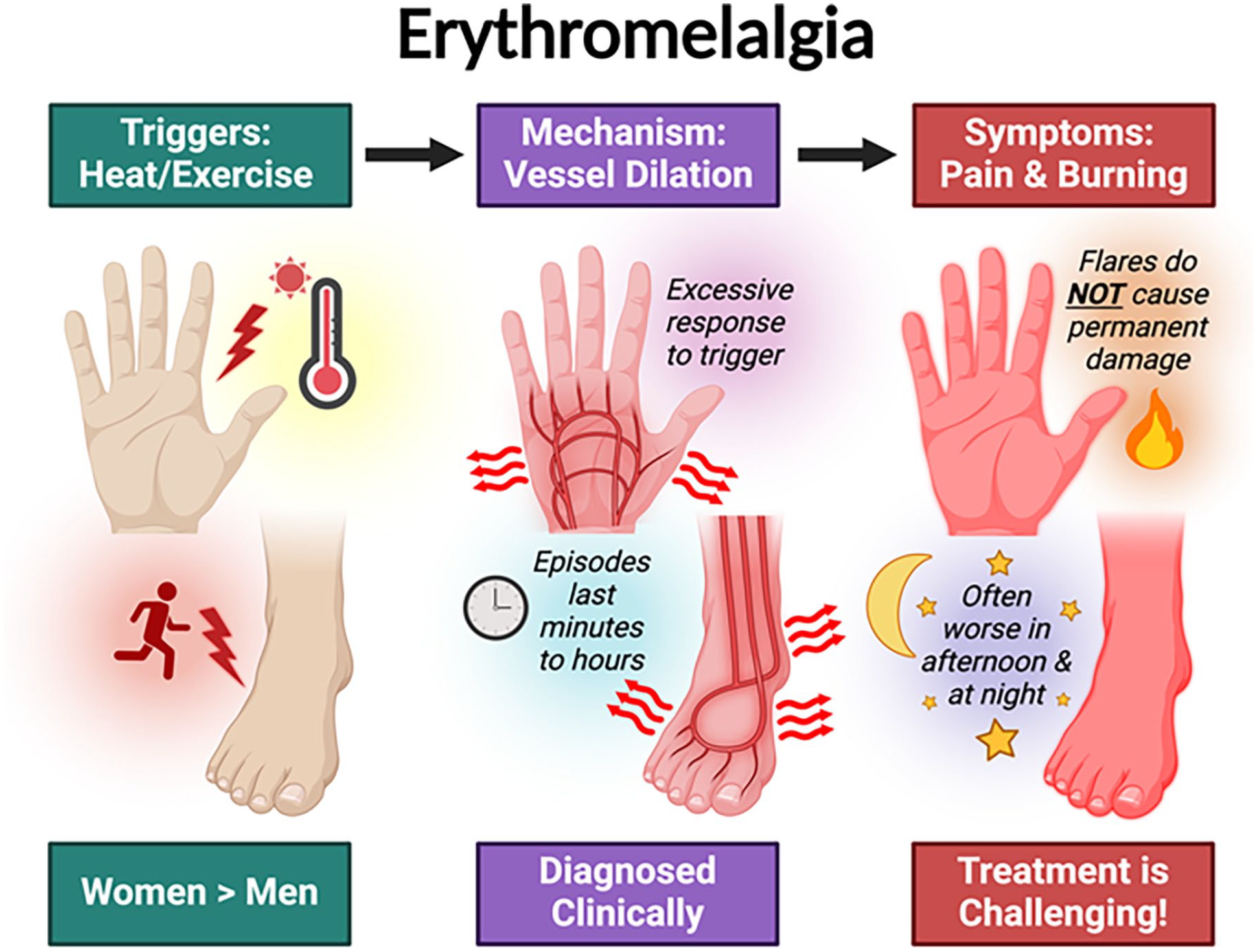
An overview of erythromelalgia.
Erythromelalgia may be divided into ‘primary’ or ‘secondary’ categories. Primary, or idiopathic, erythromelalgia has no clear associated cause or explanation for the condition; inherited erythromelalgia is also considered primary. Secondary erythromelalgia is due to a specific cause or explanation, such as an underlying medical condition or medication.
When exposed to warm temperatures or in response to exercise, the blood vessels to the extremities (feet/hands) usually dilate or expand to rid the body of excess heat. This process is called vasodilation. In the case of erythromelalgia, the vasodilation is excessive. The dramatic increase in blood flow causes the affected hands, feet, cheeks, or ears to turn red. The warmth is tied to the sensation of pain, though their exact relationship is not well understood.
Who is at risk for erythromelalgia?
Erythromelalgia can occur at any age including in children, and it is three times more common among women than men. 1 It is extremely rare, and patients may experience a long delay in diagnosis after seeking consultation with multiple medical specialists.
What are the triggers and symptoms of erythromelalgia?
A typical episode begins with the sudden onset of burning and redness in the affected area, like a severe sunburn. The symptoms are usually triggered by exposure to warm temperatures or associated with exercise; episodes can be spontaneous with no clear precipitating factors. The feet are most commonly affected, followed by the hands. Erythromelalgia may also occur in the face or on the ears. Figure 2 shows examples of feet and hands affected by erythromelalgia. Between episodes, the skin may look completely normal (Figure 2C). The episodes may last for minutes or hours. Symptoms are often reported to be worse later in the day and in the evening. Swelling may occur due to the increased blood flow.
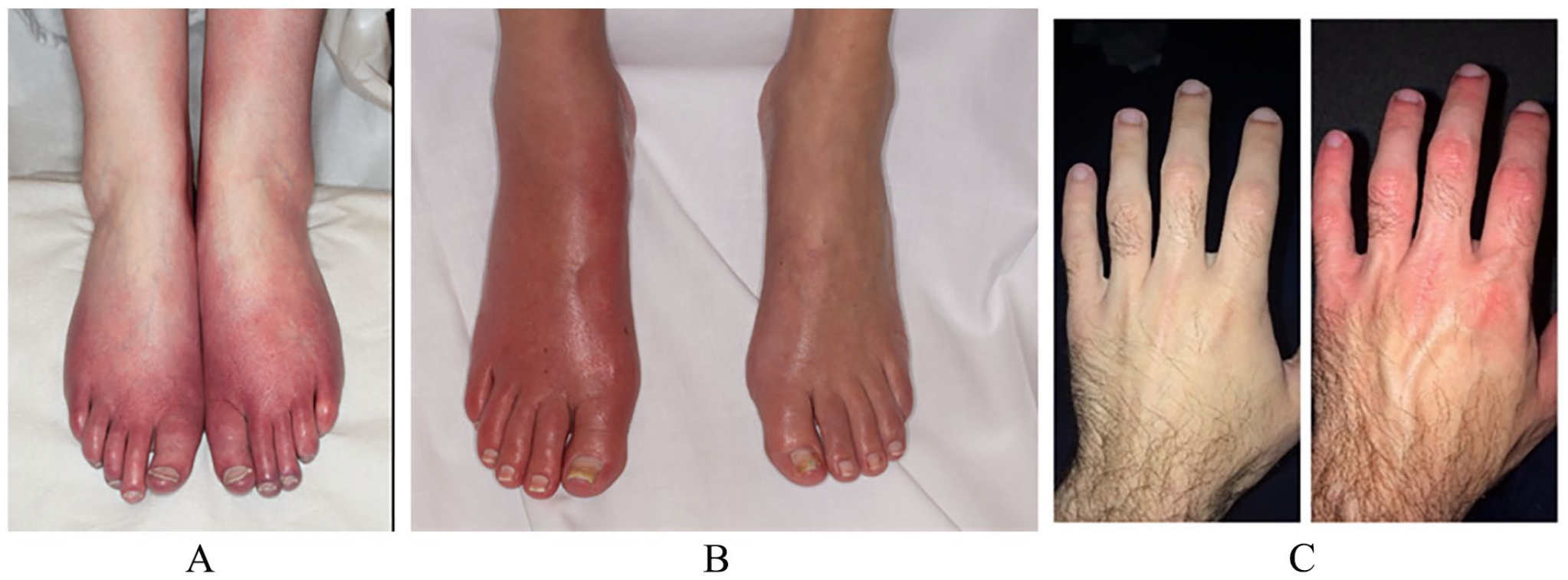
Examples of feet and hands affected by erythromelalgia. The symptoms are often symmetric
How is erythromelalgia diagnosed?
Erythromelalgia is usually diagnosed based on symptoms. The diagnosis can be confirmed by seeing photographs taken when experiencing flares to confirm the appearance and document the occurrence of the red areas during symptoms. Elaborate diagnostic testing is not needed. Tests in the vascular ultrasound laboratory to measure blood flow are generally not necessary unless another blood vessel problem is suspected.
Blood tests may be ordered to help determine whether the erythromelalgia is primary or secondary. A complete blood count (CBC) is obtained to rule out a blood disorder (myeloproliferative neoplasm, or MPN; e.g., polycythemia vera). MPN is a rare cause of erythromelalgia but important to diagnose because patients with MPN and erythromelalgia may respond well to treatment with daily aspirin.
Another common blood test is the antinuclear antibody (ANA). In primary erythromelalgia, the ANA test is negative or normal. A positive (abnormal) ANA test result does not necessarily mean that a rheumatologic or autoimmune condition is present, but it can help guide further testing. Other blood tests may include the erythrocyte sedimentation rate (ESR) or C-reactive protein (CRP) if inflammation is suspected. Age-appropriate cancer screening is reasonable. Additional blood tests are tailored to the individual’s symptoms.
Erythromelalgia is closely associated with neuropathy (both small and large fiber), though the cause and effect are not well understood. 2 Electromyography (EMG) and nerve conduction studies may be obtained to examine the large fiber nerves. Small fiber nerves are assessed through functional tests such as thermoregulatory sweat testing and the quantitative sudomotor axon reflex test (QSART). 2 Sweat glands are controlled by the small fiber nerves, which are frequently abnormal in erythromelalgia. Skin biopsy results are rarely helpful. 2
What is the relationship between erythromelalgia and Raynaud’s phenomenon?
Interestingly, patients who experience erythromelalgia in response to warmth may also have symptoms of Raynaud’s phenomenon when exposed to cold. 3 Patients with both conditions have small blood vessels that tend to overreact to changes in temperature by constricting or dilating, often inappropriately. The symptoms of Raynaud’s, however, are the opposite of erythromelalgia because the blood vessels constrict (shrink down or narrow) in response to cold exposure. With Raynaud’s, the fingers or toes may turn white or bluish when cold. Patients with overreactive small blood vessels (abnormal vasomotor function) may notice excessively cold hands in air conditioning or in the freezer section of a grocery store, and red feet in a hot shower or when walking or exercising. Patients may also experience different color changes between episodes of erythromelalgia.
For more information, please read the Vascular Disease Patient Information Page on Raynaud’s Phenomenon. 3
Is erythromelalgia inherited?
About 5% of patients with erythromelalgia will have an affected family member. 2 In these familial cases, it has an autosomal dominant pattern of inheritance, which means that a child of the affected parent will have a 50/50 chance of inheriting the gene. A specific variant in a sodium channel gene (SCN9A) has been identified in some families with inherited erythromelalgia. 4 Familial cases may not always have this particular SCN9A variant, which suggests that other genes are likely involved. Genetic testing is considered only in children or adolescents, or in cases with multiple involved family members. 1 General information can be found in the genetic testing patient information page. 5
What are the risks of having erythromelalgia?
Primary erythromelalgia poses no significant risk to overall health besides the bothersome symptoms. However, it can be quite painful and have a detrimental impact on quality of life. Chronic pain can lead to anxiety, depression, disability, and social isolation. Maintaining a normal and active lifestyle is essential to prevent this decline. With secondary erythromelalgia, other health risks may occur due to the underlying condition that caused it.
Overall, experts report that about 10% of patients will see resolution of their symptoms. 6 As a rough guide, about a third of patients will get worse, a third will improve, and a third will stay the same. However, long-term outcomes are difficult to estimate given the wide range in severity of symptoms, multiple underlying causes, and extreme variability in response to treatment. Many patients with mild or short-term symptoms may not seek medical attention.
Of note, the color changes and the painful episodes are not harmful or dangerous. The flares themselves do not damage the skin or nerves. Patients may get used to the color changes once they know they are not harmful. However, the burning pain that accompanies the color changes can impact quality of life.
How is erythromelalgia treated?
Treatment is challenging. No singular approach is universally effective, and there is no cure. Treatment goals include controlling symptoms and helping patients resume a normal life as quickly as possible.
First, identifying any underlying cause is critical. If a secondary cause is found, then the treatment should first be directed to that problem. For example, treating underlying polycythemia vera may lead to resolution of erythromelalgia; aspirin may help in this circumstance.
Patients with erythromelalgia will instinctively avoid triggers. Some patients have mild symptoms that may be managed with lifestyle adjustments. Avoiding exposure to warm temperatures may help to reduce flares. Patients often do not like to wear socks or shoes and may wear sandals or flip-flops even in winter. The balance can be delicate between avoiding triggers while maintaining a normal life. Tips to help prevent and manage erythromelalgia episodes are listed below. Cooling the skin can alleviate the symptoms, but excessive use of cooling should be avoided (e.g., from ice baths or prolonged exposure to ice water), as tissue and nerve damage and break-down/ulceration of the skin may occur. Continuous use of powerful fans close to the feet and hands can lead to reflex redness (‘windburn’) and make the symptoms worse. Elevation may be helpful to reduce excessive blood flow to the warm areas.
Tips for managing erythromelalgia symptoms
Avoid direct sun exposure. Wear a hat and sunglasses.
Apply cool water or cool washcloths to affected areas.
Do not place ice directly on the skin or submerge in ice baths to avoid frostbite, skin damage, and ulceration.
Limit use of indirect ice or submersion in cool water to ⩽ 10 minutes at a time and no more than four times daily. 1
Aim for at least 30 minutes/day of moderate-intensity aerobic exercise; swimming or walking in a pool can help.
Use ceiling fans or direct a small fan to affected areas for short periods.
Ask about stopping any unnecessary medications or supplements.
In terms of medical therapy, some medicines are directed at regulating the dilation of the small blood vessels (the redness), and some medicines are directed at the burning pain, which is considered nerve (neuropathic) pain. Keeping a symptom diary can objectively assess symptom relief as various treatments are tried. The severity and frequency of symptoms should be recorded along with the interventions.
If lifestyle changes are not enough, the symptoms may be treated with topical medications that block nerve activation like lidocaine or compounded creams (amitriptyline/ketamine). Topical medicines may have fewer side effects than oral medicines, but the results can vary. A 2- to 4-week trial is typically recommended to start.
In more severe cases, oral medications are prescribed. Working closely with a specialist with expertise in erythromelalgia can be helpful, because the process is often trial-and-error until the best medication or combination of medications is found. Common oral medications include those used for neuropathies such as gabapentin, pregabalin, amitriptyline, venlafaxine, and duloxetine. Oral steroids are not usually recommended unless the symptoms are recent and abrupt in onset,1,2 in which case a short course may be helpful. Opioids (morphine-like pain medicines) are not recommended. 2
Given that erythromelalgia is relatively rare and the response to treatment varies widely, clinical trial data are lacking on the most effective therapies. Interventional techniques like nerve blocks or epidural infusions may be tried, but little clinical evidence to support these is available. 7 Multidisciplinary pain rehabilitation may be required if the medication trials are not successful and the symptoms are debilitating. Comprehensive pain management centers typically offer an integrated approach with physicians, nurses, occupational and physical therapists, pharmacists, and psychologists. The Erythromelalgia Association (http://www.burningfeet.org) and support groups can also be helpful resources.
What about exercise and erythromelalgia?
Regular daily exercise is critical for overall cardiovascular health. Adults should achieve at least 30 minutes per day of brisk, moderate-intensity exercise. Aerobic exercise has beneficial effects on the blood vessels, and patients with erythromelalgia often notice substantial improvements once they start to exercise daily or even twice daily. Initially, exercise may be somewhat difficult as the feet or hands become warm; however, over time the symptoms will get better. Patients may turn on the fan when on the elliptical or treadmill, and they may use cold washcloths at the gym. Swimming or walking in a pool can be helpful. Daily exercise and maintaining an active lifestyle are vital to successful management of erythromelalgia.
Summary
Erythromelalgia is a rare vascular disorder involving intermittent color changes and burning pain in the feet, sometimes the hands, and occasionally the face. In primary erythromelalgia, no cause is found, but patients with secondary erythromelalgia may have other underlying medical conditions that should be treated concurrently. Several lifestyle changes can reduce the frequency of episodes, and it is important to maintain a healthy, active lifestyle despite the symptoms. Medications (topical or oral) may be used if the symptoms persist. Response to treatment varies widely. Comprehensive pain rehabilitation may be needed in severe cases.
The ‘Vascular Disease Patient Information Page’ is a regular feature of Vascular Medicine. All articles in the collection are available for free online at http://journals.sagepub.com/vmjpatientpage. The Vascular Disease Patient Information Page is provided for educational purposes only and is not a substitute for medical advice.
Footnotes
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
Dr Elizabeth Ratchford’s work was supported in part by the generosity of David Kotick (1926–2021).