
Abstract
Erythromelalgia is a rare disorder characterized by episodic burning pain with redness and warmth of the extremities. Topical and systemic medications are the mainstay of management. We reviewed the published evidence for using procedural interventions to manage erythromelalgia, including their proposed mechanism of action and possible adverse effects, and included information in this review on epidural infusion, sympathetic ganglion block, sympathectomy, pulsed radiofrequency, spinal cord stimulation, dorsal root ganglion stimulation, brain stimulation, transcranial magnetic stimulation, and botulinum toxin injections. Both successful and unsuccessful outcomes have been reported. Although these procedural interventions extend the therapeutic options for erythromelalgia, the evidence for their use is limited. Case reports and small case series comprise most of the evidence. Based on our review, a multidisciplinary approach to management may be needed for patients with erythromelalgia.
Introduction
Erythromelalgia is a rare, often debilitating disorder characterized by episodes of burning pain with red, hot extremities, most commonly the hands and feet (Figure 1). 1 Episodes of erythromelalgia frequently are triggered by physical activity and heat exposure. Pain typically is eased by cooling the affected areas with ice for short periods, cold water, or fans, and patients instinctively engage in these behaviors. Patients with erythromelalgia have poorer quality of life, increased morbidity, and increased risk for suicide than the US general population. 2

Erythromelalgia involving extremities with changes of ‘immersion foot’ from excessive use of immersion in iced water to cool the feet.
Erythromelalgia can be categorized into primary and secondary erythromelalgia. Primary erythromelalgia can be inherited or idiopathic in nature. In primary erythromelalgia that is inherited, mutations of the SCN9A gene encoding the Nav1.7 sodium channel cause hyperexcitability of nociceptive fibers. 3 Secondary erythromelalgia can result from myeloproliferative diseases such as essential thrombocythemia and polycythemia vera and other conditions like large fiber or small fiber neuropathy, metal poisoning, and autoimmune disorders. 4 Treatment of the underlying case may alleviate symptoms of secondary erythromelalgia though some patients fail to see sufficient benefit. Erythromelalgia is a challenging condition to treat with many patients persistent symptoms despite lifestyle changes, pharmacological treatments, and procedural interventions.
We have recently published a review of the medical treatments available for this condition. 5 Briefly, an initial evaluation for underlying causes such as myeloproliferative disorders and neuropathy is recommended because it can provide clues to the most responsive pharmacologic treatment. Topical treatments are the first-line therapies for erythromelalgia and include topical lidocaine, topical amitriptyline-ketamine preparations, and others. When trials of topical therapy fail, systemic medications can be introduced to the treatment regimen as adjuvant therapy. Aspirin is the first-line systemic therapy. Other systemic medications include corticosteroids, sodium channel blockers, sodium nitroprusside, antidepressants, anticonvulsants, prostaglandin analogues, calcium channel blockers, antihistamines, and beta blockers.5,6 Treating erythromelalgia may be complex with no single effective therapy, and a multidisciplinary approach to management is highly recommended. For patients with refractory erythromelalgia who failed to experience sufficient benefit with topical and/or systemic medications taken orally, procedural interventions may be a consideration. Procedural interventions reported in the literature (albeit limited to case reports and case series), include epidural infusion, sympathetic blockade, sympathectomy, pulsed radiofrequency (PRF), spinal cord stimulation (SCS), dorsal root ganglion stimulation (DRGS), brain stimulation, transcranial magnetic stimulation (TMS), and botulinum toxin injections.
In this scoping review, we briefly describe the interventions, their proposed mechanism of action, their possible adverse effects, their efficacy rates, and their reported uses to treat erythromelalgia. We acknowledge reporting bias as a major limitation to scoping reviews such as this study but believe in the need for a current and comprehensive study to direct treatment recommendations.
Methods
A comprehensive database search of Scopus and MEDLINE via PubMed was performed with erythromelalgia and erythermalgia as keywords for the interventional procedures mentioned earlier. We identified 2543 studies. Two independent reviewers screened each title and abstract from our database searches to select studies for full-text review. Studies were selected using our inclusion and exclusion criteria. Duplicates were removed and studies of erythromelalgia were included if they were published between 1985 and June 1, 2024, in the English language, and they reported trials of interventional procedures for erythromelalgia refractory to medical management. Studies were excluded if they were duplicates, not in the English language, or did not include treatment data. All studies were case studies and case reports. A total of 59 patients in 42 studies were included in this review (Figure 2). The studies are summarized in Table 1 in order of evidence levels.
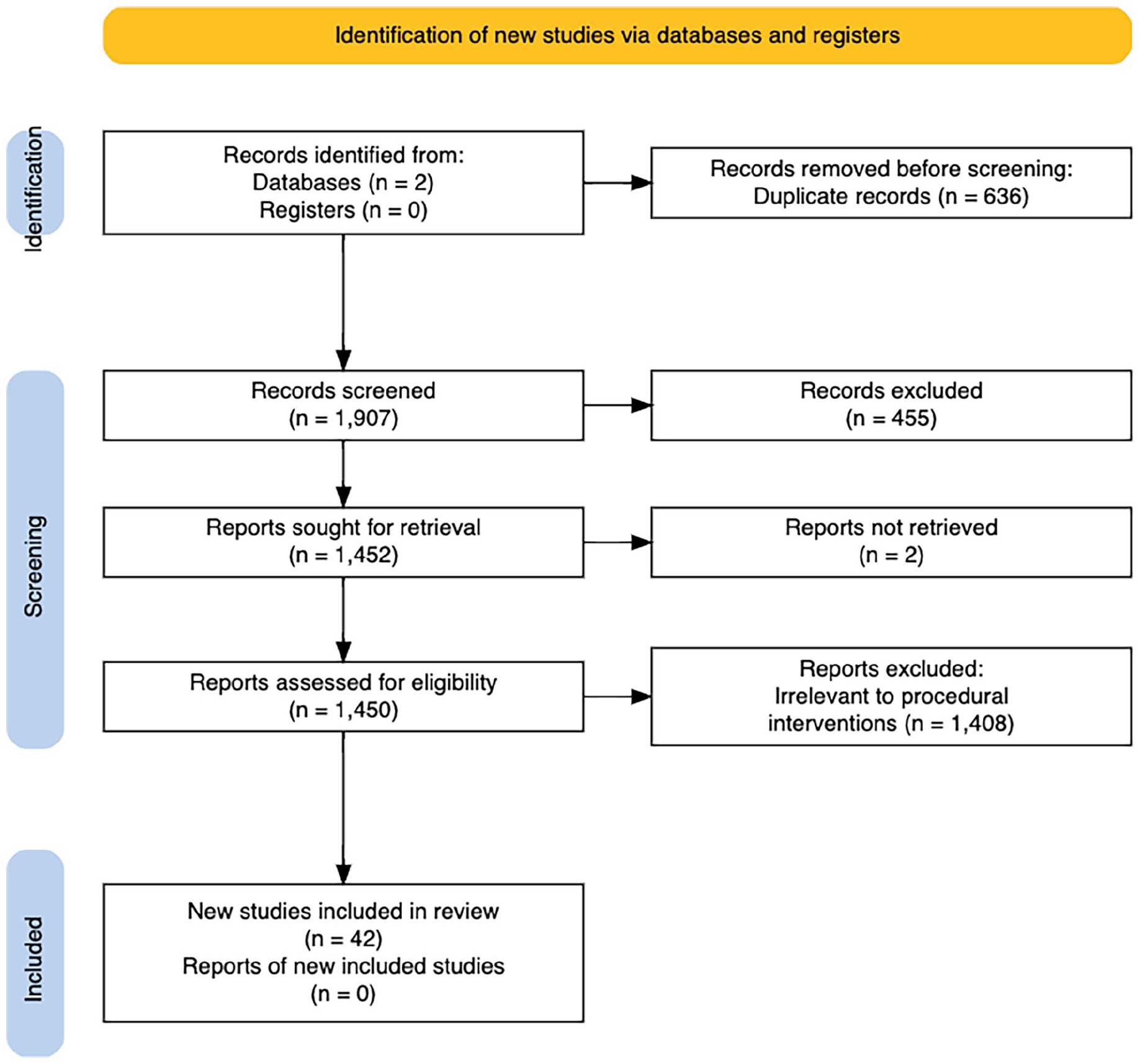
PRISMA flow diagram of study selection. PRISMA, Preferred Reporting Items of Systematic reviews and Meta-Analyses.
Procedural interventions reported for patients with erythromelalgia.
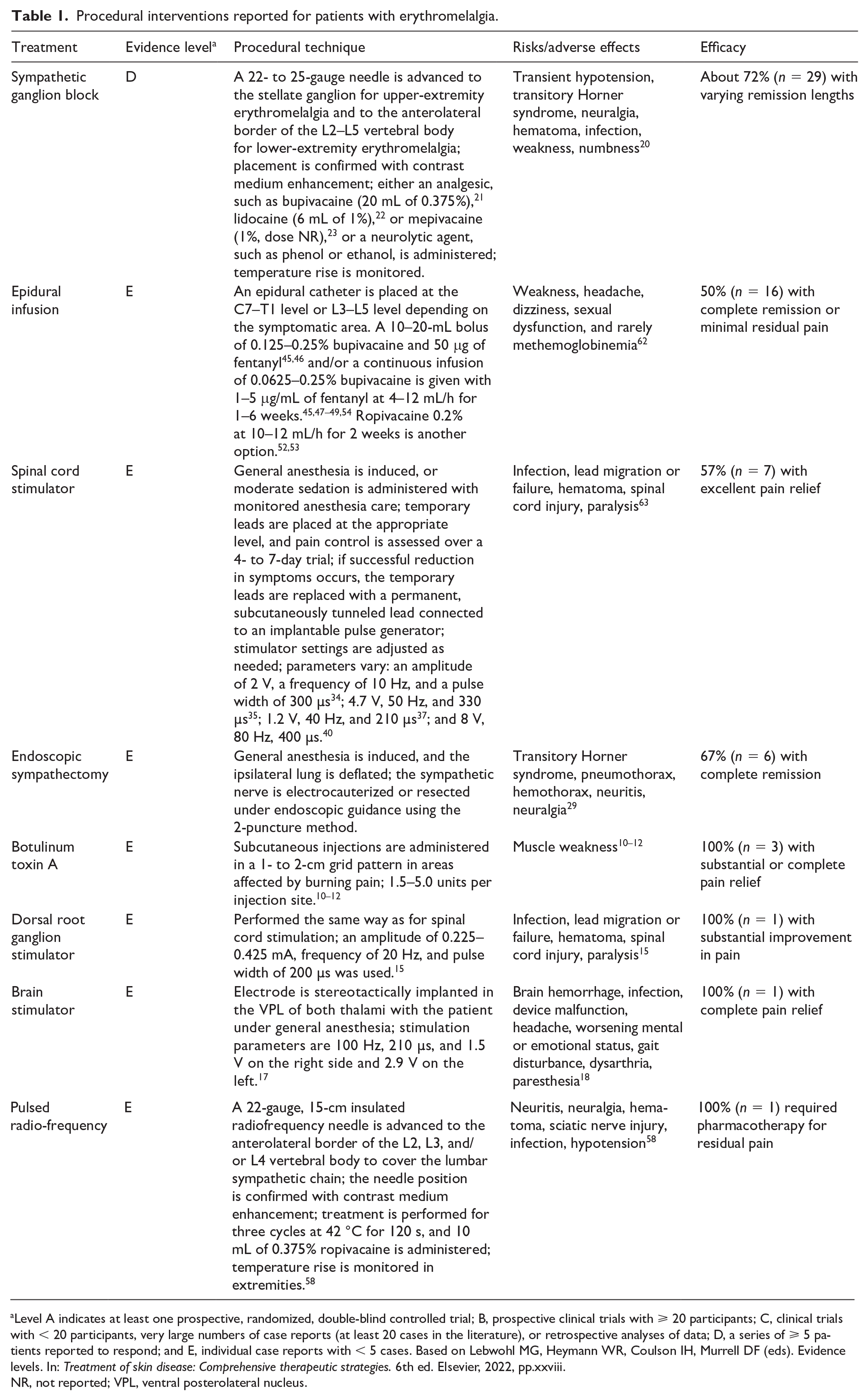
Level A indicates at least one prospective, randomized, double-blind controlled trial; B, prospective clinical trials with ⩾ 20 participants; C, clinical trials with < 20 participants, very large numbers of case reports (at least 20 cases in the literature), or retrospective analyses of data; D, a series of ⩾ 5 patients reported to respond; and E, individual case reports with < 5 cases.
Based on Lebwohl MG, Heymann WR, Coulson IH, Murrell DF (eds). Evidence levels. In: Treatment of skin disease: Comprehensive therapeutic strategies. 6th ed. Elsevier, 2022, pp.xxviii.
NR, not reported; VPL, ventral posterolateral nucleus.
Interventional procedures
The interventional procedures are presented. Note that the evidence for the use of any of these procedures is very limited. (Figure 3).
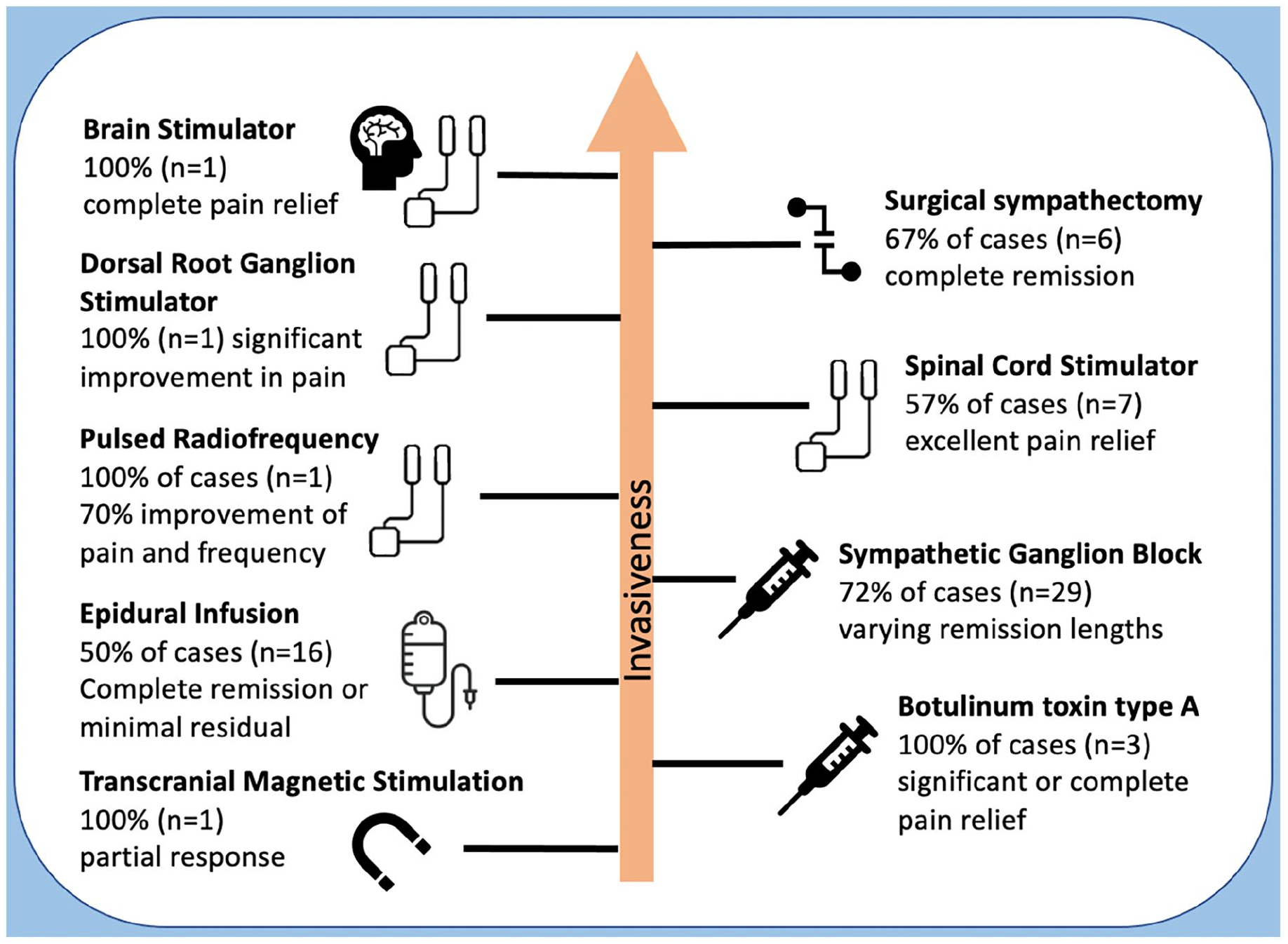
Procedural interventions reported for patients with erythromelalgia.
Botulinum toxin type A
Three reports were available for review for the use of botulinum toxin type A injections in refractory erythromelalgia. Botulinum toxin type A is a neurotoxin that inhibits release of acetylcholine from axons at neuromuscular junctions. The primary mechanism of action by which botulinum toxin provides pain relief is by attenuating muscle activity. However, botulinum toxin also has analgesic properties for treating neuropathic pain, usually when administered subcutaneously in small 0.1-mL aliquots in a grid pattern covering the localized area of neuropathic pain.7,8 The proposed mechanism by which botulinum provides analgesic effects is central and peripheral desensitization through inhibiting inflammatory neurotransmitters such as glutamate, substance P, and calcitonin gene-related peptide. 9
A few published reports support the use of botulinum toxin A for erythromelalgia. In three individual case reports, subcutaneous injections of botulinum toxin A of the left hand in one patient, bilateral cheeks in one patient, and left arm and anterior thighs in one patient provided substantial or complete pain relief to patients with refractory erythromelalgia.10–12 One of these patients reported a posttreatment reduction not only in pain intensity but also in the number of subsequent episodes. 10 Results from botulinum toxin injections were reported to last up to 9 weeks for another patient, and regular treatment was necessary to avoid return of symptoms. 11 Assessing the optimal dose of botulinum toxin A can be challenging because of dose-related muscle weakness, but this adverse effect diminishes in 2 months. 12
Transcranial magnetic stimulation
One case report was reviewed for the use of TMS in refractory erythromelalgia. TMS is a noninvasive treatment that uses magnetic fields to promote activity of brain regions controlling mood and depression. Although TMS is typically used to treat depression, some preliminary findings show its potential role in modulating neuropathic pain with induction of slow-frequency magnetic pulses to the dorsolateral prefrontal cortex. 13 A case report described a 24-year-old woman with erythromelalgia who was treated with TMS and noted partial and prolonged response, with continued improvement of her pain ratings at 3 months after treatment. 14 To our knowledge, no other published report explores TMS as a potential therapy for erythromelalgia. Additionally, the mechanism in which TMS treats depression or pain is not completely understood, and its effectiveness requires further clinical investigation. The noninvasive nature and minimal risk associated with TMS make it an option to consider as a possible adjunct therapy for patients with refractory erythromelalgia.
Dorsal root ganglion stimulation
One case report was reviewed for the use of dorsal root ganglion stimulation (DRGS) in refractory erythromelalgia. DRGS, similar to SCS, uses electrical neuromodulation techniques to alleviate pain. The difference between the two stimulators lies in lead placement. Although SCS leads are implanted in the epidural space, DRGS leads are placed in the dorsal root ganglion, where primary afferent fibers reside. To our knowledge, only one case report describes DRGS for treatment of erythromelalgia. After DRGS, a 70-year-old woman noted 80% improvement, reporting 1 of 10 on a pain scale versus 5 of 10 before implantation of the stimulator. 15 Within 3 months after DRGS implantation, she had an erythromelalgia flare, which was reported to be less severe than before DRGS.
To compare DRGS and the more traditional SCS, investigators performed a randomized, controlled comparative trial for 152 participants with complex regional pain syndrome or causalgia. 16 Participants who received DRGS therapy had significantly better outcomes and less nonspecific stimulation of nonpainful areas. The effectiveness of DRGS for treating erythromelalgia specifically needs further investigation, as does comparison between different modes of neuromodulation.
Brain stimulation
One case report was reviewed for the use of brain stimulation in refractory erythromelalgia. Thalamic stimulation can provide pain relief by using electrical neuromodulation techniques similar to SCS and DRGS. Delivery of electrical stimuli alters aberrant nerve activity, which can relieve pain. With thalamic stimulation, leads are placed in the ventral posterolateral nucleus, the area of the thalamus where sensory information is received, and then projected to the somatosensory cortex. The need to a access structures as deep as the thalamus illustrates the invasive nature and risks involved with performing this procedure. In our literature review, only one case report described thalamic stimulation for treating erythromelalgia. Thalamic stimulation was trialed for a 12-year-old boy because of his severe symptoms and recurrent infection after SCS implantation. 17 The patient reported complete pain relief and eventually discontinued using all pain medication. After 3 years, however, he reported worsening symptoms.
Further studies are needed to determine the effectiveness of thalamic stimulation therapy for erythromelalgia. Risks to consider with this procedure are infection, brain hemorrhage, device malfunction, worsening mental or emotional status, gait disturbance, dysarthria, and paresthesia. 18 The anatomic location of the thalamus makes thalamic stimulation a highly invasive procedure with increased risk of complications, so it should be considered only when other therapies fail.
Sympathetic blockade
Sympathetic ganglion block (SGB) is an umbrella term that refers to the disruption of sympathetic nerve activity with an injection of local anesthetic or neurolytic agent into the sympathetic ganglia. The effects of lidocaine and bupivacaine are often temporary, whereas the effects of neurolytic agents such as phenol or ethanol result in permanent ablation, making SGBs with neurolytic agents the more invasive option. Why a sympathetic block can help with erythromelalgia is unclear. The theory of treating erythromelalgia with SGB is based on the hypothesis that pain in erythromelalgia results from abnormal microvascular blood flow and tissue hypoxemia 19 ; blocking sympathetic activity could increase tissue perfusion and decrease ischemic pain. Also conceivable is that sympathetic blockade blocks somatic afferent fibers and modulates the perception of pain.
Sympathetic blockade is also characterized by a transient temperature increase in the ipsilateral limb. Temperatures are measured before and after the procedure to document an adequate sympathetic block. Because heat is a frequent trigger for erythromelalgia symptoms, some providers are reluctant to perform an interventional procedure that causes limb warming for a patient with erythromelalgia because of fear of provoking erythromelalgia symptoms. The most common adverse effects are infection and transient hypotension, which is an expected result of a successful sympathetic blockade. 20
Sympathetic blockade using local anesthetics
Two case series and six case reports were available for review for the use of SGBs with local anesthetic in erythromelalgia. Adjuvant agents such as corticosteroids or clonidine are frequently included in nonneurolytic sympathetic blocks because of a purported potential to increase the duration of effect, but this belief lacks known evidence-based support. Although nine of 12 patients who received reversible SGBs reported improvement in burning pain,21–28 the number of treatments needed to alleviate erythromelalgia symptoms varied from person to person. A case report described substantial pain relief and almost complete healing of ulcers 8 weeks after a single SGB treatment in one patient. 21 Many more SGB treatment sessions, however, were required for two other patients: eight times over 4 months to achieve milder symptoms for a 21-year-old woman and 10 times for a 37-year-old woman for complete resolution.24,25 For a female patient, the frequency of erythromelalgia episodes decreased, but she still had to immerse her feet in cold water every few hours. 22 In these studies, not only the number of treatments varied but also the duration of pain relief. In a case series of one male and two female patients, erythromelalgia symptoms did not reappear for a year in one case and for 3 years in another case, whereas the third patient received continued benefit. 23
Thus, the experience with SGB with local anesthetic varies. SGB with local anesthetics is considered for patients who want to trial SGB before committing to irreversible SGB or before or instead of a sympathectomy.
Sympathetic blockade using neurolytic agents
One case series of 13 patients and four case reports was reviewed for the use of SGBs with neurolytic agents in erythromelalgia. An irreversible SGB performed with a neurolytic agent such as phenol or ethanol is also termed chemical lumbar sympathectomy (CLS). This procedure results in permanent ablation, so it is one of the more invasive approaches to treating refractory erythromelalgia. One case series described positive outcomes for nine of 13 patients who trialed CLS. 29 Dramatic analgesic responses were reported for these nine patients, with a 90–100% decrease in pain on the visual analog scale. Those effects, however, did not last for four patients; two of those patients had a slightly increased visual analog scale pain score during follow-up examinations, and the other two patients relapsed. Of interest, recurrences were more common among patients with SCN9A mutations. In four other case reports, CLS succeeded in treating refractory erythromelalgia in three patients.30–33 A 59-year-old man had a poor response to an epidural block, but after CLS he reported that his severe pain immediately disappeared and did not recur for at least 9 months. 31 Two female pediatric patients both dramatically improved after CLS, with one of them having a 5-year remission.30,32
CLS is indicated for patients who report short-lived but adequate relief with reversible SGBs. Therefore, reversible SGB with local anesthetics is recommended before irreversible SGB with neurolytic agents (CLS).
Although both reversible and irreversible SGBs are often performed with moderate bedside sedation in a fluoroscopic procedure suite, they do not require general anesthesia and are thus considered an economical option for treating chronic pain.
Spinal cord stimulation
Six case reports were found describing the use of spinal cord stimulation (SCSs) in refractory erythromelalgia. An SCS is implanted temporarily or permanently to alleviate pain by delivering electrical stimuli that alter nerve conduction. Although the mechanism of SCS is not fully understood, some authors suggest a competition between C fibers and Aβ fibers that hinders the C-fiber activity, which causes pain. 34 Of seven patients with refractory erythromelalgia who underwent SCS implantation, four of them reported excellent pain relief.35–39 Both fixed-duration SCS and continuous therapy with SCS have been reported to be effective. A 12-year-old girl who received fixed-duration SCS therapy for 10 days had a positive outcome continuing 12 months after the SCS was removed. 37 A 69-year-old woman who underwent SCS implantation reported refractory pain after the battery failed but excellent pain relief after the battery was replaced. 40 Because the duration of pain relief can vary from patient to patient, optimizing stimulator settings to achieve full benefit can take some time. One patient who did not fully benefit from SCS alone reported 0 of 10 on a pain scale with the addition of oral mexiletine therapy; 34 when SCS therapy was halted, the patient reported refractory pain within 6 hours. Oral mexiletine alone proved to be insufficient for this patient, who benefited from multimodal treatment.
Neuromodulation techniques such as SCS that use electrical stimuli to act directly on nerves are an option for patients who have adverse effects associated with pharmacotherapies and who are wary of permanent interventions such as CLS. Hardware-related complication is the most common adverse event from implantable stimulators. 41 If the lead migrates or fails, it can be repositioned or replaced.
Endoscopic sympathectomy
Two case series and three case reports were reviewed for the use of sympathectomies in refractory erythromelalgia. Sympathectomy refers to the surgical resection or electrocautery of a sympathetic ganglion or ganglia in which the distributed area is affected. Following the same therapeutic rationale as for sympathetic blockades, a sympathectomy is performed to correct abnormal microvascular blood flow and decrease pain induced by ischemia. Transitory Horner syndrome can result from a sympathectomy, but this adverse effect has become rare with the assistance of thoracic endoscopes that allow precise resections and avoidance of the stellate ganglion. Of six patients with refractory erythromelalgia, four had full remission after undergoing this procedure. Two of these patients who remained symptom free for at least 6 months after endoscopic sympathectomy previously trialed both epidural infusions and SGBs with insufficient benefit.26,33 One patient experienced full remission only after two sympathectomies were performed 6 months apart. 33 Interestingly, one patient saw delayed improvement of symptoms at 4 months. 42 Insufficient benefit and temporary relief were reported by the other two patients, one of whom controlled her symptoms solely by avoiding precipitating factors after various trials of medications and procedures.43,44
The response to epidural blockades is considered a reliable predictor in the success of sympathectomy. 33 Therefore, sympathectomy may be recommended for patients who have refractory erythromelalgia after short-term pain relief from epidural infusions. When the study results are taken together, endoscopic sympathectomy has shown varied effectiveness in treating erythromelalgia and is considered one of the more invasive treatment options. Other options such as an epidural infusion and SGB are recommended before sympathectomy is considered.
Epidural infusion
Epidural infusion with local anesthetics such as bupivacaine and ropivacaine to treat refractory erythromelalgia was described in several case reports. Complete remission or return to daily activities with minimal pain was reported for eight of 16 patients.26,27,33,39,45–51 The other eight patients reported immediate but temporary relief and required additional intervention with either pharmacotherapy, a second epidural infusion, or other procedural interventions. 52 Two of those patients were successfully treated with the surgical sympathectomies.26,33 One patient who did not improve with epidural infusion also failed to see complete benefit with SCS implantation. 39 Pharmacologic treatment (e.g., oxcarbazepine, pregabalin, mexiletine) is recommended before attempting a second infusion to achieve long-term pain relief.53–55 Our recent publication on medical management describes the mechanism of action and treatment outcomes for this intervention in more detail. 5
Pulsed radiofrequency
One case report was reviewed for the use of PRF in refractory erythromelalgia. PRF is a nonablative, minimally invasive technique that uses heat from electrical currents to modulate pain. The exact mechanism of pain relief is unknown, but one theory suggests that pulsatile electric fields attenuate proinflammatory cytokines such as tumor necrosis factor α and interleukins 1β and 6. 56 Another theory suggests that PRF enhances noradrenergic and serotonergic descending pain inhibitory pathways to cause analgesic effects. 57 Evidence, largely from case reports and small case series, suggests that a wide variety of chronic pain conditions such as radicular pain and neuralgias can be treated with PRF, but from our literature review, only one case report described the use of PRF for treating refractory erythromelalgia. A 22-year-old woman with erythromelalgia reported 70% improvement of burning pain and shorter, less frequent episodes after PRF treatment, but she continued to take aspirin and gabapentin for residual pain at her 12-week follow-up visit. 58 Whereas SCS is implanted, PRF is performed by using local anesthesia and thus is considered the less invasive option. 59 A larger clinical trial is needed to determine the efficacy of PRF in treating erythromelalgia.
Proposed procedural treatment approach
Taken together, limited evidence exists to support the use of procedural interventions to manage erythromelalgia. Generally, these interventions have been used in patients with refractory erythromelalgia who have already trialed topical and/or systemic oral medications. The current literature provides insufficient evidence to propose an evidence-based approach that recommends a specific procedural treatment. There is a lack of evidence to suggest a specific procedural treatment to be more beneficial for primary versus secondary erythromelalgia. Epidural infusion and SGB are the most documented techniques for treating refractory erythromelalgia. Therefore, we recommend trial of epidural infusion or SGB before SCS and surgical sympathectomy. An individualized approach to treating refractory erythromelalgia is recommended that considers the effectiveness, invasiveness, and risks of each procedural intervention (Figure 2, Table 1). It is important the patient understands that experience with each of these interventions is extremely limited, as detailed in this report. When discussing procedural interventions, practitioners should ensure that patients fully understand the risks and should manage their expectations. Referral to a comprehensive pain rehabilitation center can be considered for patients in whom an erythromelalgia-associated chronic pain syndrome develops.
Limitations
Reports of the use of procedural interventions for managing the pain of erythromelalgia are limited to case reports of one patient or to small series of patients with refractory pain. To minimize bias in locating studies, we performed a broad, comprehensive search of the literature using two key words in two databases, and two authors assessed each full-text article for inclusion in the study. Reporting bias can skew the reported effectiveness of these procedural interventions; cases are much more likely to be reported if the intervention was successful. Differences in outcome measures among studies is evidence of this bias. In many of the existing reports and available studies, multiple treatment modalities were used; therefore, determining which modality is truly effective was difficult. Additionally, in the case reports and case series reviewed, the clinical diagnostic criteria for the diagnosis of erythromelalgia varied, and sometimes no diagnostic criteria were provided. There is insufficient evidence to recommend different approaches for primary and secondary erythromelalgia.
Summary
Treatment of erythromelalgia is challenging, with no single effective therapy or cure. This literature review shows that the evidence exists for the effectiveness of procedural interventions in erythromelalgia is extremely limited. An individualized approach to treating refractory erythromelalgia is recommended that considers the effectiveness, invasiveness, and risks of each intervention. A multidisciplinary team with representation from dermatology, primary care, vascular medicine, neurology, and pain medicine, including clinicians with an expertise in performing the described interventions, may be necessary for the optimal management and care of patients with refractory erythromelalgia.60,61
Procedural interventions augment the range of treatments that can be considered for managing erythromelalgia. However, this review highlights the dearth of evidence to support their use. The best evidence level of success was for SGB. TMS, botulinum toxin injection, DRGS, and brain stimulation were reported to be effective and are considerations for treating severe erythromelalgia symptoms refractory to multiple therapies; however, sufficient evidence is lacking for their general use. Further studies are needed to show the effectiveness of these interventional techniques in managing erythromelalgia.
Footnotes
Disclaimer
Mayo Clinic does not endorse specific products or services included in this article.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.