
Abstract
Introduction:
The absence of coronary artery calcium (CAC = 0) is associated with low risk of stroke events; however, predictors of incident stroke among those with CAC = 0 are not known.
Methods:
Individual participant-level data were pooled from three prospective cohorts (Multi-Ethnic Study of Atherosclerosis [MESA], Jackson Heart Study, and Framingham Heart Study). Multivariable-adjusted Cox proportional hazards models were used to study the association between cardiovascular risk factors and incident adjudicated stroke among individuals with CAC = 0 who were free of clinical atherosclerotic cardiovascular disease at baseline.
Results:
Among 6180 participants (mean age 53 [SD 11] years, 62% women, and 44% White, 36% Black, and 20% other individuals), over a median (IQR) follow up of 15 (12–16) years, there were 122 strokes (95 ischemic, 27 hemorrhagic) with an overall unadjusted event rate of 2.0 per 1000 person-years. After multivariable adjustment, risk factors associated with overall stroke included (hazard ratio [95% CI]) systolic blood pressure (SBP): 1.19 (1.05–1.36) per 10-mmHg increase and carotid intima–media thickness (CIMT): 1.21 (1.04–1.42) per 0.1-mm increment. Current cigarette smoking: 2.68 (1.11–6.50), SBP: 1.23 (1.06–1.42) per 10-mmHg increase, and CIMT: 1.25 (1.04–1.49) per 0.1-mm increment were associated with ischemic stroke, whereas C-reactive protein was associated with hemorrhagic stroke risk (0.49, 0.25–0.93).
Conclusion:
In a large cohort of individuals with CAC = 0, the rate for incident stroke was low (2.0 per 1000-person years) and was associated with modifiable risk factors.
Introduction
The incidence of stroke has decreased in the overall population, yet contemporary data suggest that there is an increase in the proportion of strokes among young adults.1–3 This rise has tracked a parallel increase in the prevalence of cardiometabolic risk factors such as hypertension, dyslipidemia, and diabetes. Stroke often results in significant morbidity and mortality, including long-term disability, which has a significant economic impact. 1
Coronary artery calcium (CAC) measures subclinical calcified coronary atherosclerotic burden and is the most powerful tool for atherosclerotic cardiovascular disease (ASCVD) risk prediction.4,5 A prior study from the CAC consortium showed that an increasing burden of CAC is associated with a higher risk of stroke deaths compared to participants with absent CAC. 6 However, the overall 10-year stroke risk is about 1% in individuals with a CAC score of 0. 7
As CAC is absent in nearly 50% of adults, 8 there is a need to study which risk factors remain associated with stroke events in the absence of CAC. In the present analysis, we evaluated modifiable risk factors that are independently associated with incident stroke events among those without CAC (CAC = 0). We analyzed markers related to glucose and lipid metabolism, blood pressure, and inflammation. We also assessed ultrasound-based carotid imaging biomarkers as a biomarker of subclinical carotid atherosclerosis.
We leveraged the detailed assessment of cardiovascular risk factors and adjudicated stroke events in three large cohorts to determine which modifiable risk factors are associated with incident stroke events in those with CAC = 0.
Methods
Study population
Individual participant-level data were pooled from three prospective cohort studies: Multi-Ethnic Study of Atherosclerosis (MESA), Jackson Heart Study (JHS), and Framingham Heart Study (FHS). Study design, participant characteristics, and event adjudication were previously reported.9–13
Briefly, MESA is a multi-ethnic, community-based cohort study, which enrolled 6814 participants, 45–84 years of age, with no known cardiovascular disease. The initial enrollment of MESA occurred at four sites from 2000 to 2002 and is considered the baseline visit. The JHS is the largest single-site, population-based prospective study of African Americans; it enrolled 5301 adults ages 21–94 years from the Jackson, Mississippi tri-county area. CAC assessment by computed tomography (CT) was first performed in visit 2 (2005–2008) and is the baseline for the present study. The FHS first incorporated a CAC assessment by multidetector computed tomography (MDCT) in the Framingham Offspring and Third Generation cohorts’ examinations in participants who attended the offspring seventh examination cycle (1998–2001) and third-generation first examination cycle (2002–2005). Details on CAC assessment in each of the three cohorts are demonstrated in Supplementary Figure S1.
The present study included participants from all three cohorts who, at baseline, were free of prevalent ASCVD (including prevalent coronary heart disease and stroke). Participants with baseline CAC > 0 and those with missing information on CAC were excluded from the present analysis.
The protocol for each study was approved by the Institutional Review Board (IRB) of each participating center, and all participants provided informed consent for study enrollment. This subanalysis was exempt from additional IRB review.
Assessment of baseline covariates in the study cohorts
All participants underwent comprehensive examinations using standardized protocols described previously.9–13 Age, sex, race/ethnicity, annual income, education, cigarette smoking status, physical activity, and medication use were self-reported using validated questionnaires. Risk factors included waist circumference, low-density lipoprotein cholesterol (LDL-C), high-density lipoprotein cholesterol (HDL-C), triglycerides, lipoprotein(a), C-reactive protein, diabetes mellitus, systolic blood pressure (SBP) and current smoking. The 10-year ASCVD risk of each participant was calculated using the ACC/AHA 2013 Pooled Cohort Equations.14,15 Atrial fibrillation was defined using hospitalization discharge codes in MESA, self-report in JHS, and electrocardiogram (ECG) review in FHS.
All three cohorts used comparable methods for the measurement of carotid intima–media thickness (CIMT) and assessment of carotid plaque.16–18 High-resolution B-mode ultrasound of the left and right common carotid arteries was used for assessment of mean CIMT of both common carotid arteries. The 75th percentile was defined using measurements from the pooled cohorts. Internal CIMT was defined as mean of the mean far wall IMT for the left and right internal carotid arteries. The presence of carotid plaque was defined as focal absolute wall thickness (IMT) > 1.5 mm or relative focal thickening of > 50% compared with the adjacent IMT.
Assessment of CAC
CAC was measured using a noncontrast cardiac-gated electron-beam CT or MDCT in MESA 19 and using MDCT in FHS and JHS.11,20 CAC was calculated using the method described by Agatston based on the number, area, and peak Hounsfield units of calcified coronary plaques. 21
Outcome variable
Incident stroke included both ischemic and hemorrhagic strokes and was adjudicated as previously described.22–24 For all three cohorts, trained physicians reviewed and adjudicated incident stroke events, including the first occurrence of definite nonfatal or fatal stroke and was further stratified by ischemic and hemorrhagic stroke subtypes.
In MESA, interim hospitalization was inquired from study participants or their next of kin every 9–12 months. Stroke events were adjudicated by a MESA committee using medical records and death certification, as detailed previously. Three vascular neurologists reviewed all events that were thought to be possibly related to stroke and further adjudicated these events based on symptoms, signs, and imaging results.
In FHS, study visits occurred every 4 years where detailed information on medical records and family history, and cerebrovascular and cardiac symptoms was obtained. Any concerning event or symptom was reviewed by a neurologist with stroke expertise for further adjudication. An in-person visit was conducted by a study neurologist if the symptoms were consistent with stroke. Information was subsequently reviewed by a panel including at least two neurologists with stroke expertise.
In JHS, stroke was defined on the basis of history of stroke (personal history or self-reported signs and symptoms), carotid endarterectomy or angioplasty. Patient queries during annual telephone follow up and ongoing surveillance of hospitalizations were used to ascertain stroke events. Hospital records and death certificates were sent to a medical record abstraction unit for review. Hospitalized and fatal stroke events were classified using a computer-generated diagnosis with physician adjudication.
For the current analysis, only incident adjudicated stroke events were included. Transient ischemic attack (TIA) was not included as an endpoint for the following reasons: (1) the diagnosis of TIA can be challenging because it can be nonspecific, and transient in nature. Many patients may not seek medical attention and those who do may present after a delay, which may obscure the diagnosis; (2) TIA captures many entities that are not cerebrovascular disease in origin, such as seizure, or migraine; and (3) though TIA is part of the American College of Cardiology/American Heart Association definition of ASCVD, we aimed to determine the cerebrovascular consequences of cardiovascular disease and therefore we focused our analysis on stroke only.
Statistical analysis
Baseline characteristics were tabulated for those with CAC = 0 at baseline. Continuous variables were summarized using mean (SD) or median (IQR), and categorical variables were summarized as count (percentage). Unadjusted incidence rates (IR) of stroke events (overall and subtype) were calculated as the number of events per 1000 person-years according to the presence or absence of cardiovascular risk factors.
After confirming the proportionality assumption, multivariable Cox proportional hazards models were used to examine the association between each cardiovascular risk factor and incident stroke events (overall and subtype). Among participants with more than one type of stroke event adjudicated during the follow-up period, the first event was used in this analysis. Models were adjusted for the following confounders: age, sex, race/ethnicity, education level, annual income, study site, physical activity, aspirin use, cholesterol-lowering medication use, and atrial fibrillation (Model 1). Model 2 included all variables in model 1 and risk factors for stroke that were chosen a priori based on their known associations with stroke, including current smoking, diabetes, SBP, waist circumference, HDL-C, LDL-C, triglycerides, lipoprotein(a) levels, presence of carotid plaque, and CIMT.
Stratified analyses by age, sex, and race were performed given known differences in stroke risk and etiology. 25 The association of internal CIMT and incident stroke was examined in sensitivity analyses. A p-value less than 0.05 was considered statistically significant. All analyses were conducted using Stata, version 16.1 (StataCorp LLC, College Station, TX, USA).
Results
The pooled cohort consisted of 11,217 individuals without missing information on CAC. After excluding participants with CAC > 0, the study population consisted of 6180 individuals with CAC score 0, including 3416 from MESA, 1063 from JHS, and 1701 from FHS (Table 1). For the MESA cohort, the mean (SD) age was 58 (9) years, with 63% women, and 33% White and 31% Black individuals. In JHS, the mean (SD) age was 55 (10) years, with 70% women and 100% Black individuals. In FHS, the mean age (SD) was 43.3 (6) years, with 55% women and 100% White individuals (Table 1).
Baseline characteristics by study cohort in individuals without prevalent ASCVD and with a coronary artery calcium score of zero in the Multi-Ethnic Study of Atherosclerosis, Jackson Heart Study, and Framingham Heart Study cohorts.
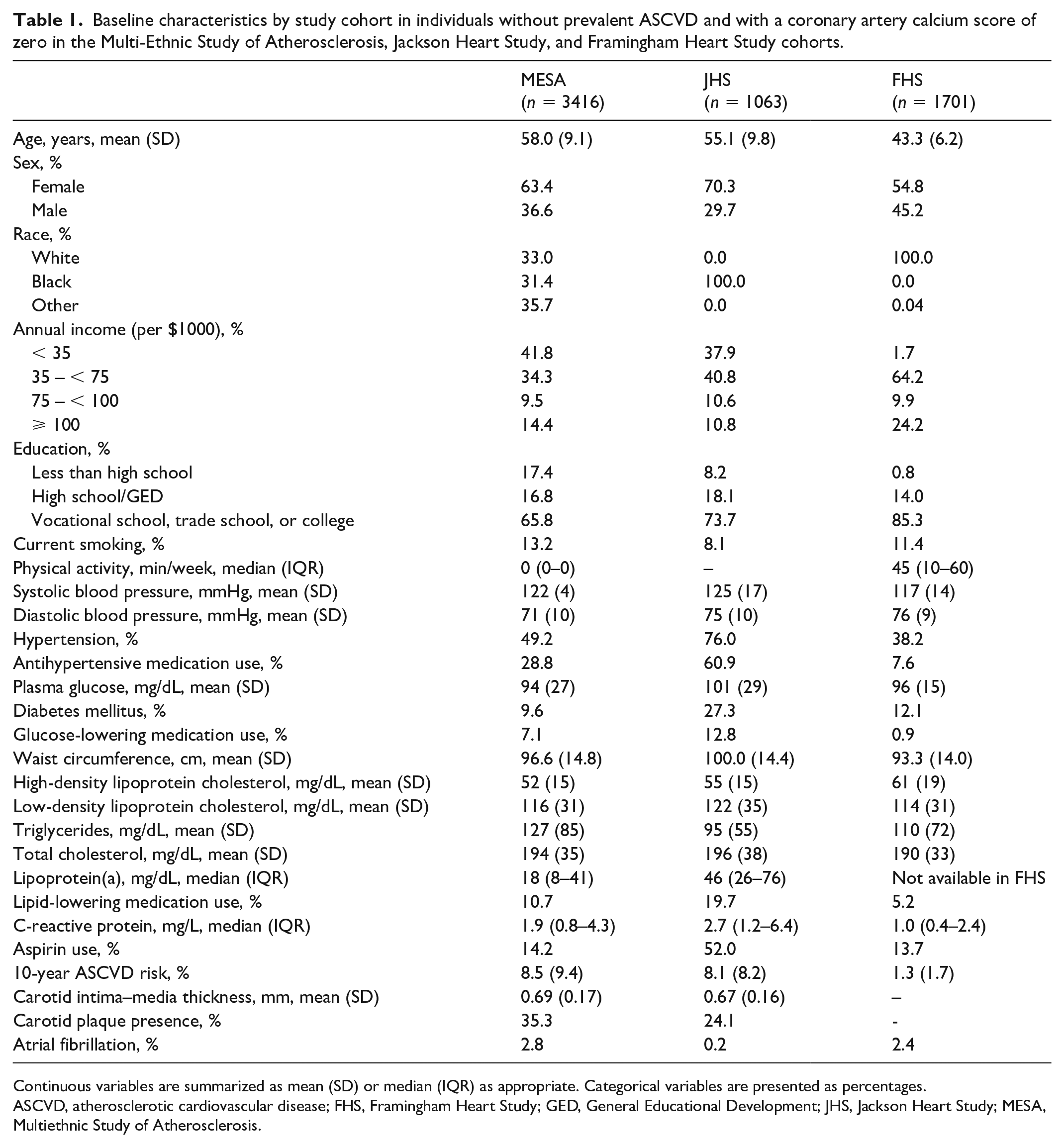
Continuous variables are summarized as mean (SD) or median (IQR) as appropriate. Categorical variables are presented as percentages.
ASCVD, atherosclerotic cardiovascular disease; FHS, Framingham Heart Study; GED, General Educational Development; JHS, Jackson Heart Study; MESA, Multiethnic Study of Atherosclerosis.
Over a median (IQR) follow-up time of 15 (12–16) years, there were 122 total stroke events (95 ischemic, 27 hemorrhagic strokes), with an IR of overall stroke events of two per 1000 person years (Supplementary Table S1). The IR of stroke was ⩽ 2 per 1000 person-years for subgroups defined by most risk factors, with the exception of current cigarette smoking (2.7), diabetes mellitus (2.9), hypertension (2.2), and CIMT > 75th percentile (3.3) (Table 2).
Incidence rate of stroke events (per 1000 person-years) according to presence of risk factors among patients with a coronary artery calcium score of zero and without prevalent ASCVD in the Multi-Ethnic Study of Atherosclerosis, Jackson Heart Study, and Framingham Heart Study cohorts.
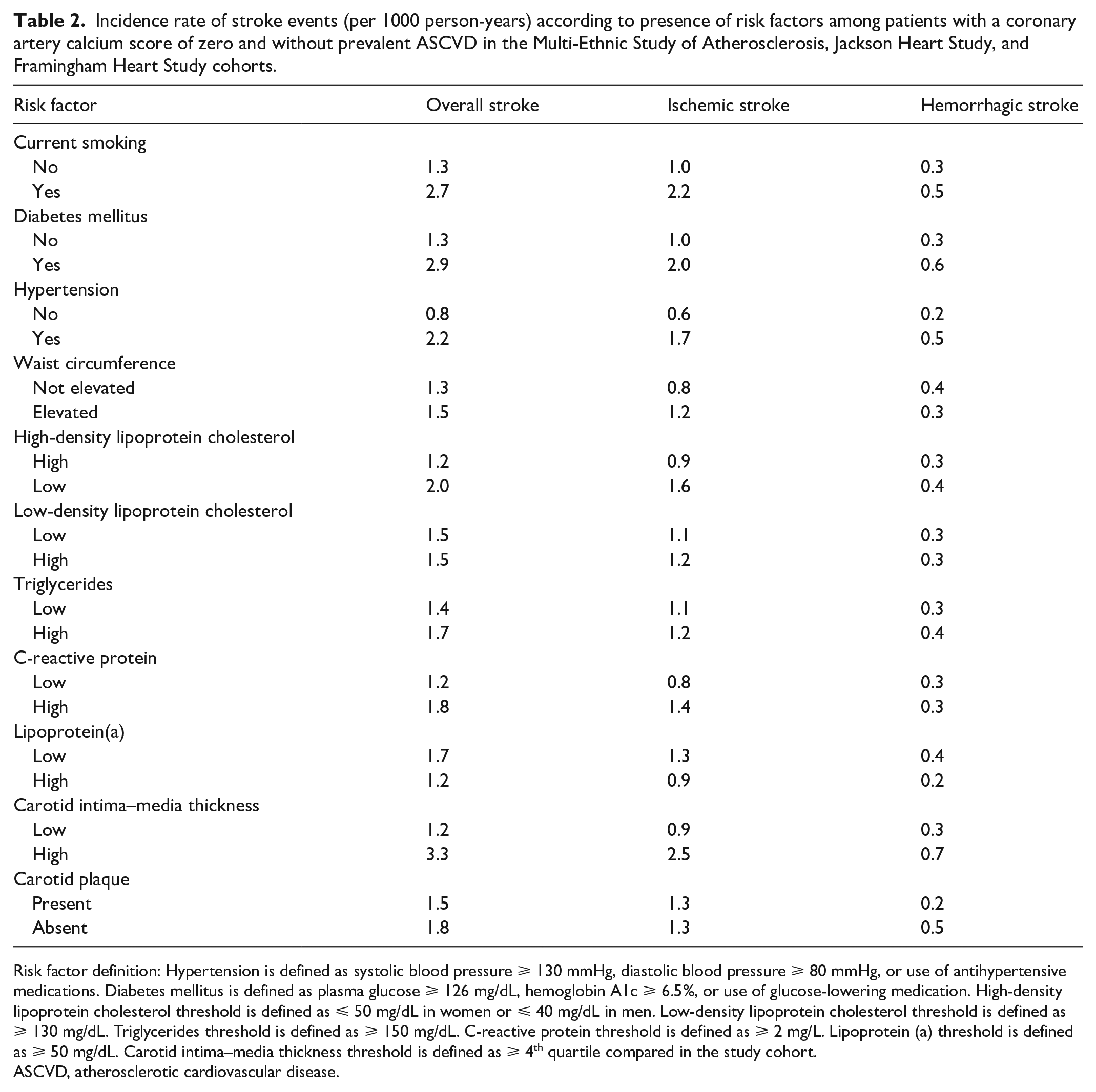
Risk factor definition: Hypertension is defined as systolic blood pressure ⩾ 130 mmHg, diastolic blood pressure ⩾ 80 mmHg, or use of antihypertensive medications. Diabetes mellitus is defined as plasma glucose ⩾ 126 mg/dL, hemoglobin A1c ⩾ 6.5%, or use of glucose-lowering medication. High-density lipoprotein cholesterol threshold is defined as ⩽ 50 mg/dL in women or ⩽ 40 mg/dL in men. Low-density lipoprotein cholesterol threshold is defined as ⩾ 130 mg/dL. Triglycerides threshold is defined as ⩾ 150 mg/dL. C-reactive protein threshold is defined as ⩾ 2 mg/L. Lipoprotein (a) threshold is defined as ⩾ 50 mg/dL. Carotid intima–media thickness threshold is defined as ⩾ 4th quartile compared in the study cohort.
ASCVD, atherosclerotic cardiovascular disease.
After multivariable adjustment (Model 2), factors that remained significantly associated with incident overall stroke events (hazard ratio [95% CI]), included SBP: 1.19 (1.05–1.36) per 10-mmHg increase and CIMT: 1.21 (1.04–1.42) per 0.1-mm increment (Table 3).
Association of risk factors with incident overall stroke events among participants with a coronary artery calcium score of zero without prevalent ASCVD in the Multi-Ethnic Study of Atherosclerosis, Jackson Heart Study, and Framingham Heart Study cohorts.
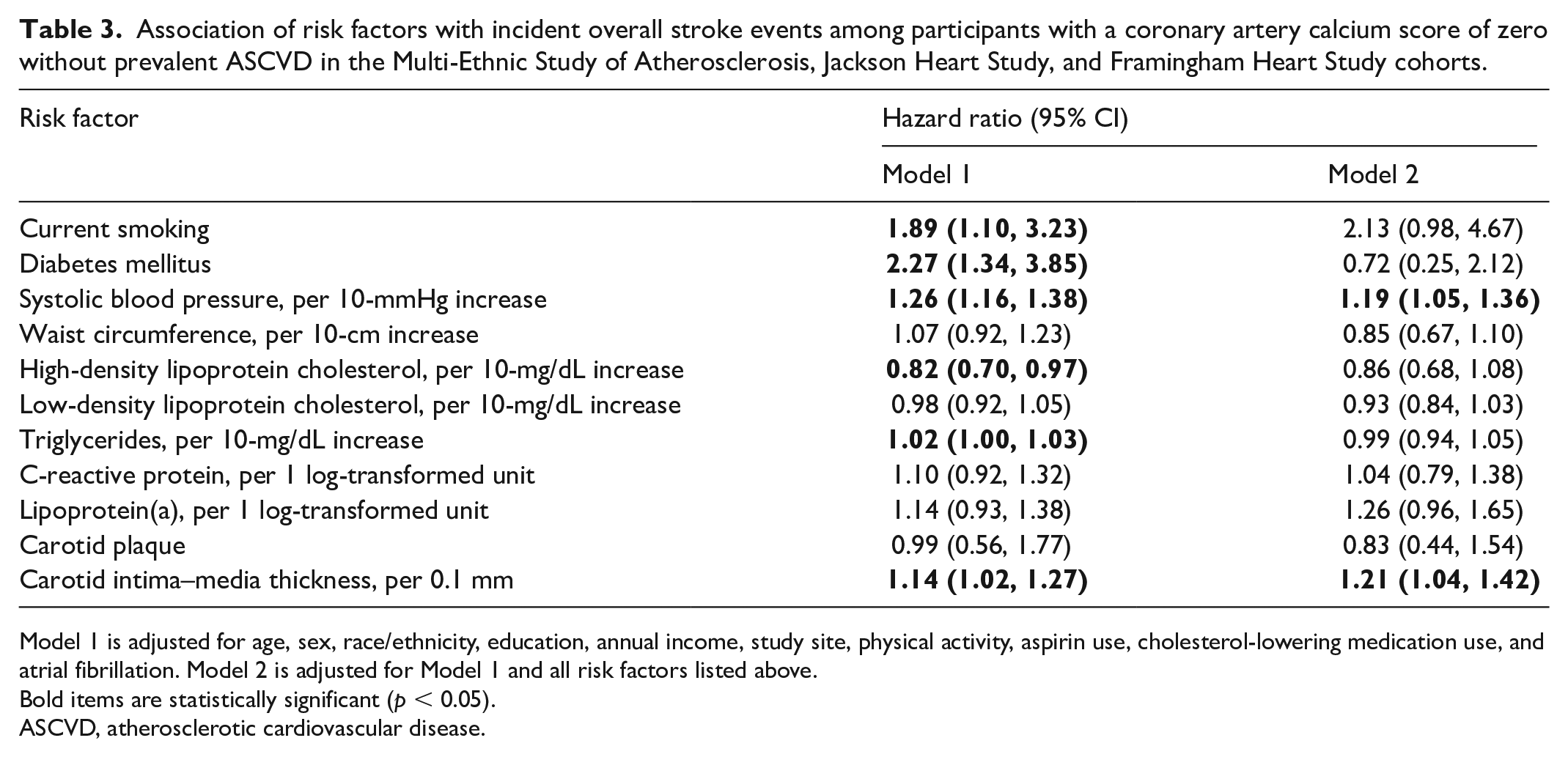
Model 1 is adjusted for age, sex, race/ethnicity, education, annual income, study site, physical activity, aspirin use, cholesterol-lowering medication use, and atrial fibrillation. Model 2 is adjusted for Model 1 and all risk factors listed above.
Bold items are statistically significant (p < 0.05).
ASCVD, atherosclerotic cardiovascular disease.
When stratified by stroke subtype (Supplementary Table S2), factors that were significantly associated with incident ischemic stroke events (HR [95% CI]) included: current cigarette smoking: 2.68 (1.11–6.50), SBP: 1.23 (1.06–1.42) per 10-mmHg increase, and CIMT: 1.25 (1.04–1.49) per 0.1-mm increment. On the other hand, C-reactive protein was significantly associated with a lower risk of hemorrhagic stroke (0.49, 0.25–0.93).
In age-stratified analyses, there was no significant interaction between age and any cardiovascular risk factors in the multivariable-adjusted Cox regression model (p for interaction > 0.05; Supplementary Table S3). Similarly, there was no significant interaction with any cardiovascular risk factors in sex and race-stratified analyses (Supplementary Tables S4 and S5, respectively).
There was no significant association between internal CIMT with risk of overall stroke events: 1.01 (0.97, 1.06), ischemic stroke: 1.02 (0.97, 1.08), or hemorrhagic stroke: 0.96 (0.84, 1.10).
Discussion
In a large, pooled analysis from three cohort studies of 6180 individuals without ASCVD and a CAC score of zero at baseline, the overall event rate for incident stroke events was low (two events per 1000 person-years). Current cigarette smoking, higher SBP, and higher CIMT were associated with a higher risk of incident ischemic stroke events. There were no significant differences by age, sex, or race/ethnicity in the association of risk factors and incident stroke events.
The results of this study demonstrate that stroke event rates in individuals with a CAC score of zero are low over a long follow-up period, consistent with prior work. 26 The present study sought to evaluate determinants of stroke events in this group. Modifiable risk factors remained significantly associated with higher risk of stroke events, which reaffirms the importance of risk factor control in all individuals regardless of subclinical atherosclerosis burden. Clinicians should continue to advocate for healthy lifestyle choices and optimize cardiovascular risk factors that may predispose individuals with a CAC score of zero to develop stroke, especially current smoking and SBP. CIMT may be used for additional risk stratification of ischemic stroke events in those with CAC = 0. More research is needed on the potential role of selective carotid imaging to identify risk of stroke in this group.
There were some differences in risk factors associated with ischemic and hemorrhagic stroke likely due to differences in the pathogenesis of these two entities. 25 Ischemic stroke was associated with risk factors involved in either the initiation or progression of atherosclerosis, including current smoking and higher SBP. Optimal strategies for ischemic stroke prevention must focus on addressing and mitigating these modifiable risk factors that are directly involved in stroke pathogenesis. Hypertension has long been recognized as the most important modifiable risk factor for both ischemic and hemorrhagic strokes. According to the Centers for Disease Control, nearly half of US adults have hypertension and hypertension is controlled in about one in four adults. The present study further demonstrates the importance of blood pressure control to prevent risk of ischemic stroke among adults free of subclinical atherosclerosis. Current smoking is an established risk factor for stroke and has a stronger association with ischemic stroke. 27 Diabetes mellitus was associated with a higher risk of stroke events but not after adjustment for all risk factors (Model 2).
A prior meta-analysis found that higher baseline levels of C-reactive protein are associated with a higher risk of ischemic but not hemorrhagic stroke. 28 In the present study, C-reactive protein was associated with a nonsignificantly higher risk of both ischemic and hemorrhagic stroke in Model 1. After concomitant adjustment for all factors (Model 2), C-reactive protein remained nonsignificantly associated with ischemic stroke but significantly and inversely associated with risk of hemorrhagic stroke. It is noteworthy that unadjusted hemorrhagic stroke event rates were very low and identical in individuals with low versus high C-reactive protein levels (0.3 and 0.3 per 1000-person years, respectively). Thus, the observed signal in multivariable adjustment may be a chance finding that is not clinically significant.
Use of noninvasive carotid imaging can help detect subclinical atherosclerotic disease in the early stages. A CIMT measurement higher than the 75th percentile for the cohort was associated with higher risk of ischemic strokes among individuals with CAC = 0. In fact, absolute event rates of incident stroke in the highest quartile of CIMT were higher than event rates among individuals who smoked cigarettes or who had diabetes. Although CIMT has been shown to correlate well with most of the major cardiovascular risk factors and is strongly associated with cardiovascular events in prior studies,29–31 its additive value over traditional risk factors in cardiovascular risk prediction has not been consistently demonstrated. This is believed to be due to heterogeneity in the ultrasound and CIMT measurement protocols employed, reproducibility issues, and the fact that small measurement errors are sufficient to reclassify an individual from one percentile group to another. Therefore, it is recommended that rigorous and high-quality protocols are employed for measuring CIMT. With improved quantification using 3D ultrasound and advances in plaque characterization, the clinical utility of carotid ultrasound for stroke risk prediction will continue to evolve. Carotid plaque was not significantly associated with risk of overall stroke or stroke subtypes in the present study. This is consistent with a prior MESA study showing that carotid plaque was not associated with stroke events in those with CAC = 0. 32
The strengths of our study are a large cohort of both White and Black individuals with standardized protocols for coronary and carotid assessment, detailed cardiovascular phenotyping, long-term follow up (median 15 years), and stroke event adjudication.
The study has limitations. Incident stroke rates were low, which likely underpowered the study in subgroup analyses to evaluate risk factors associated with each stroke subtype (ischemic vs hemorrhagic) and assess risk factors related to different mechanisms of stroke (lacunar/small vessel, extracranial large vessel, intracranial large vessel, cardioembolic). The prevalence of carotid plaque was low, which might explain the lack of significant association with incident stroke in the pooled study population with CAC = 0. More granular information on CIMT, such as distal common carotid and carotid bifurcation, was not uniformly available across the included studies. The impact of preventive therapy and change in risk factors over time, whereby patients may have been instituted on statin, antihypertensive, and antiplatelet medications over follow up, could not be adequately assessed. Lastly, information on important confounders such as diet and family history of stroke was not uniformly available, which may have resulted in residual confounding.
Conclusion
Incident stroke events remain low in individuals with CAC = 0. Modifiable risk factors including current smoking and SBP remain associated with stroke in this group.
Supplemental Material
sj-pdf-1-vmj-10.1177_1358863X241270911 – Supplemental material for Predictors of incident stroke among individuals without coronary artery calcification: A pooled cohort analysis from the Multi-Ethnic Study of Atherosclerosis, Jackson Heart Study, and Framingham Heart Study
Supplemental material, sj-pdf-1-vmj-10.1177_1358863X241270911 for Predictors of incident stroke among individuals without coronary artery calcification: A pooled cohort analysis from the Multi-Ethnic Study of Atherosclerosis, Jackson Heart Study, and Framingham Heart Study by Aliza Hussain, Michelle C Johansen, Michael J Blaha, Mouaz H Al-Mallah, Miguel Cainzos-Achirica, Vijay Nambi, Jerome I Rotter, Xiuqing Guo, Jie Yao, Stephen S Rich, Jaideep Patel, John W McEvoy, Khurram Nasir, Rebecca Gottesman, Roger S Blumenthal, Christie M Ballantyne, Salim S Virani and Mahmoud Al Rifai in Vascular Medicine
Footnotes
Acknowledgements
The authors thank the other investigators, the staff, and the participants of the MESA study for their valuable contributions. A full list of participating MESA investigators and institutes can be found at ![]() . This paper has been reviewed and approved by the MESA Publications and Presentations Committee.
. This paper has been reviewed and approved by the MESA Publications and Presentations Committee.
Declaration of conflicting interests
The authors declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article:
Funding
The MESA projects are conducted and supported by the National Heart, Lung, and Blood Institute (NHLBI) in collaboration with MESA investigators. Support for MESA is provided by contracts 75N92020D00001, HHSN268201500003I, N01-HC-95159, 75N92020D00005, N01-HC-95160, 75N92020D00002, N01-HC-95161, 75N92020D00003, N01-HC-95162, 75N92020D00006, N01-HC-95163, 75N92020D00004, N01-HC-95164, 75N92020D00007, N01-HC-95165, N01-HC-95166, N01-HC-95167, N01-HC-95168, N01-HC-95169, UL1-TR-000040, UL1-TR-001079, UL1-TR-001420, UL1TR001881, DK063491, and R01HL105756.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.