
Abstract

Peripheral artery disease (PAD) is common, can manifest as intermittent claudication (IC), and is associated with functional impairment and poor quality of life. 1 Treatment options for IC include medical therapy, endovascular intervention, and importantly exercise therapy (ET). There is strong evidence demonstrating that ET, particularly supervised exercise therapy (SET), is associated with improved functional outcomes.2–4 Despite this, ET is heavily underutilized in PAD and little is known about referral rates, and factors associated with referral and participation in ET. 5 The Patient-Centered Outcomes Related to Treatment Practice in Peripheral Arterial Disease: Investigating Trajectories (PORTRAIT) registry is used to better characterize ET in a symptomatic cohort. 6
PORTRAIT was an international, multicenter, prospective registry of patients referred to vascular clinics for PAD symptoms, enrolling between June 2011 and December 2015. 6 Sixteen vascular clinics from the United States, five centers from the Netherlands and one clinic from Australia participated in the study. Adults with new-onset or worsening PAD symptoms and with an ankle–brachial index (ABI) < 0.90 or a post-exercise ankle pressure drop > 20 mmHg were included. At baseline and at 3 months, patients were interviewed about severity of PAD symptoms, Peripheral Artery Questionnaire (PAQ), referral to ET, participation in ET, and reasons for not participating in ET. The aim of this research letter is to detail the characteristics of patients referred for SET and unsupervised ET (USET) and to identify barriers to participation.
The registry enrolled 1275 patients and after exclusion of 74 patients who were in an alternate exercise program and deemed ineligible for ET referral, 1201 patients were included in the current analysis. A total of 280 (23.3%) of these patients were referred to SET, 455 (37.9%) to USET, and 466 (38.8%) of eligible patients received no formal exercise therapy referral. Referral patterns starkly differed by country: 87.5% (n = 245) of SET referrals were from the Netherlands and 95.0% (n = 432) of USET referrals were from the US. The characteristics of patients referred to SET versus no referral and USET versus no referral significantly differed (Table 1). Compared with those not referred for ET, patients referred to SET were younger, more likely to be of White race, and had lower rates of education level above high school. No difference in referral by sex was observed. Rates of comorbid conditions were also significantly lower among those referred to SET, including history of myocardial infarction, congestive heart failure, coronary revascularization, chronic kidney disease, and peripheral interventions. Rutherford classification (RC) of IC symptoms was also generally lower among those referred to SET versus no ET (RC I). PAQ scores were also higher, indicating less disease-specific limitation, among those referred to SET. Compared with those not referred for ET, patients referred for USET were older, more likely to be female, more likely to be non-White, and more likely to have higher rates of education. There were minimal differences in comorbid conditions between those referred to USET versus no ET. IC symptoms by RC were significantly less severe, and PAQ scores higher among those referred to USET versus no ET.
Baseline characteristics of patients referred to supervised exercise therapy and unsupervised exercise therapy.
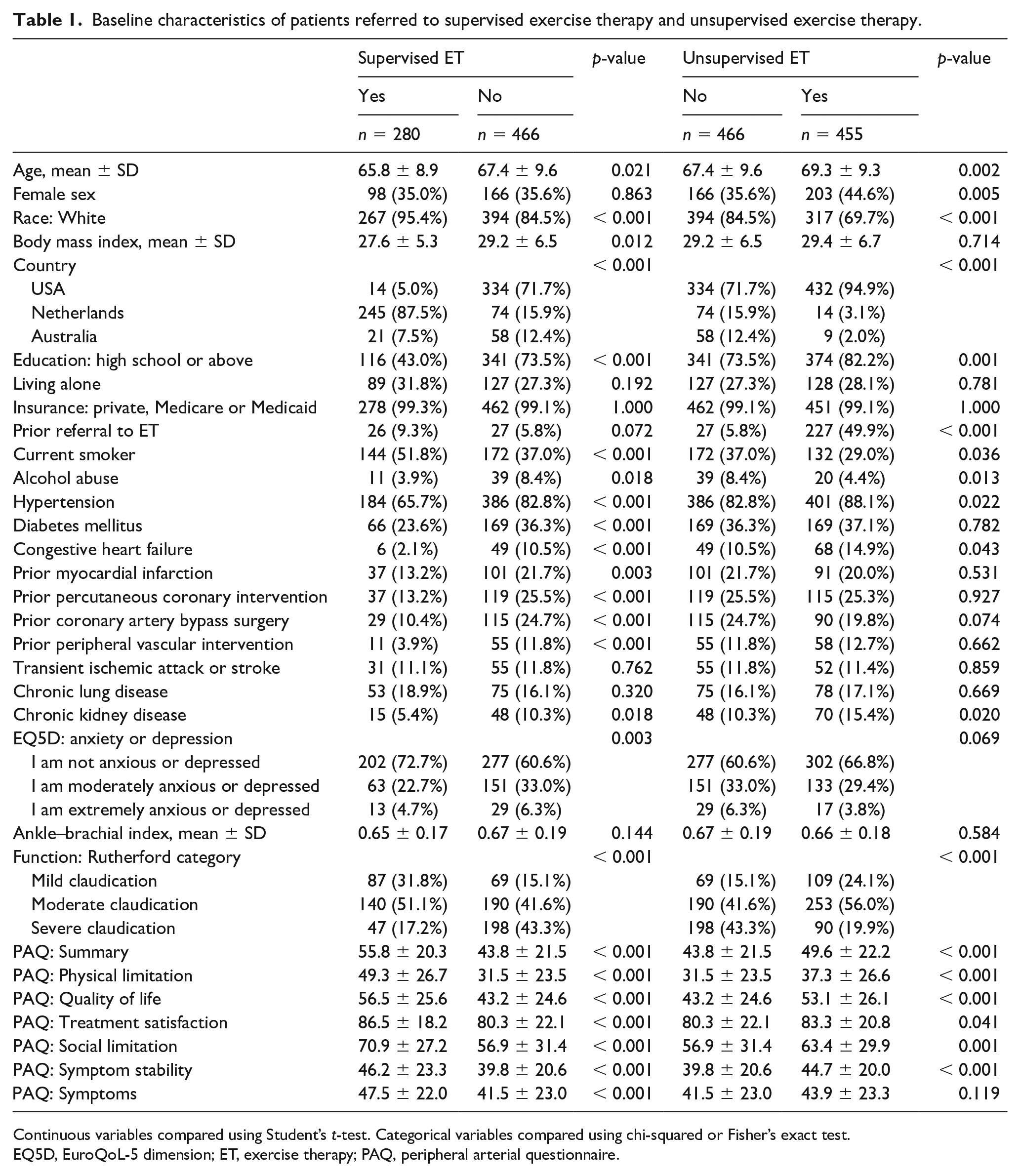
Continuous variables compared using Student’s t-test. Categorical variables compared using chi-squared or Fisher’s exact test.
EQ5D, EuroQoL-5 dimension; ET, exercise therapy; PAQ, peripheral arterial questionnaire.
Three-month follow-up interviews were obtained in 89.9% of patients. Among those referred for ET, 40.1% reported having participated in at least one session. Participation occurred in 198 of 262 (75.6%) patients referred for SET and 75 of 404 (18.6%) patients referred for USET. Among patients referred to SET who did not participate in or complete the program (n = 108), the reasons included: preference to walk myself (28.9%), medical (14.1%), not offered nearby (6.7%), feeling worse (6.7%), insurance does not (adequately) cover (5.9%), cost (5.9%), schedule conflict (3.7%), feeling better (3.7%) (online supplemental figure).
This study uniquely evaluates practice patterns of ET referral, who preferentially gets referred, and subsequent patient participation. The principal findings of this study are that 38.8% of eligible patients receive no ET referral from vascular clinics, marked variation in referral existed in the US and the Netherlands, and participation rates were significantly higher among those referred to SET. This study notably took place prior to a 2017 Centers for Medicare and Medicaid decision to reimburse the cost of SET in the US. Even if referral rates improve, our study suggests that other barriers to participation and program completion exist. Only 40% of referred patients participated in ET and, although consistent with prior systematic reviews, this low participation remains a concerning statistic. 7 The most commonly identified barrier to participation in SET was a preference to walk by myself, which signals an important opportunity for patient education and development of technology that can teach and track individuals exercising individually.
There are notable limitations of this observational study. The historical context relative to payment coverage has been mentioned. That patients were enrolled from PAD specialty clinics may represent a selection bias. Only three countries participated in this study, with no representation from low or middle-income countries; therefore, findings may not be generalizable. In addition, the Netherlands is well known for its referral programs in PAD. 8 The use of subjective data was collected via questionnaires, which are potentially subject to self-reporting and recall bias. However, in conclusion, it remains clear that there is significant room for improvement in promoting and facilitating access to ET for patients with PAD.
Supplemental Material
sj-pdf-1-vmj-10.1177_1358863X211033649 – Supplemental material for Exercise therapy referral and participation in patients with peripheral artery disease: Insights from the PORTRAIT registry
Supplemental material, sj-pdf-1-vmj-10.1177_1358863X211033649 for Exercise therapy referral and participation in patients with peripheral artery disease: Insights from the PORTRAIT registry by Tripti Gupta, Patrick Manning, Dhaval Kolte, Kim G Smolderen, Nancy Stone, Jessica G Henry, Jingyan Wang, Kensey L Gosch, Christopher J White, John Spertus and J Dawn Abbott in Vascular Medicine
Footnotes
Declaration of conflicting interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: Dr Smolderen receives research grants from Johnson & Johnson, Cardiva, and Abbott, and she is a consultant for Optum Labs. The remaining authors have nothing to disclose.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Supplementary material
The supplementary material is available online with the article.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.