
Abstract

Keywords
What is post-pulmonary embolism syndrome?
Pulmonary embolism (PE) is the medical term for blood clots that are located in the arteries of the lungs. PE affects between 300,000 and 400,000 people in the United States annually. With anticoagulation therapy (i.e., blood thinners), blood clots typically resolve without permanent damage; however, approximately half of patients who have a new PE will experience some degree of exercise limitation. Post-PE syndrome includes a spectrum of patients with persistent shortness of breath, exercise limitation, and/or impaired quality of life after at least 3 months of treatment with anticoagulation therapy.
What is chronic thromboembolic pulmonary disease (CTEPD) and chronic thromboembolic pulmonary hypertension (CTEPH)?
Post-PE syndrome may range from persistent shortness of breath to chronic thromboembolic pulmonary disease (CTEPD) with or without pulmonary hypertension.1,2 CTEPD is defined by persistent thrombosis (blood clots) within the pulmonary vasculature (arteries of the lung), causing chronic thrombotic obstructions without the presence of elevated blood pressure in the pulmonary arteries. Chronic thromboembolic pulmonary hypertension (CTEPH) represents the most severe form of post-PE syndrome, characterized by chronic residual thrombotic obstructions with elevated blood pressure in the pulmonary arteries.
How common are post-PE syndrome, CTEPD, and CTEPH?
Up to 50% of patients will have persistent problems following a PE. The true incidence of post-PE syndrome, including CTEPD and CTEPH, is unknown. Approximately 30–50% of patients will have evidence of residual blood clots months after the acute PE, but not all patients with residual blood clots will develop CTEPH. A recent meta-analysis of 16 studies reported that approximately 3% of PE survivors develop CTEPH.1–3
What are the risk factors for developing CTEPD and CTEPH?
The exact cause of CTEPD and CTEPH is unknown. In general, obesity, smoking, pregnancy, or use of oral contraceptives containing estrogen increase the risk of developing blood clots (including PE). Most patients (75%) have a history of a PE, and most are ‘unprovoked’ PE.1–3 A blood clot is considered ‘unprovoked’ when there is no clear trigger for the event (e.g., surgery, prolonged immobilization > 72 hours during or after a hospitalization, or long periods of inactivity such as car rides or flights > 6 hours).1–3
Other factors that may increase the risk of CTEPD or CTEPH include a history of cancer, chronic inflammatory diseases, low thyroid hormone levels, non-O blood type groups, prior spleen removal, long-term intravenous catheter use, history of prior blood clot events, certain medical conditions, and blood-clotting disorders (hypercoagulable state or thrombophilia).1–4 Antiphospholipid syndrome (APS) is a blood clotting disorder that is particularly associated with an increased risk for CTEPH. In one study, 20% of patients with CTEPH also had APS antibodies.1–3 Interestingly, up to 25% of patients with CTEPH do not carry a prior history of PE.
Unfortunately, the natural course of post-PE syndrome remains poorly understood and challenging to characterize because there can be months to years between the initial PE event (which may go undetected) and the CTEPD and CTEPH diagnosis.1–3
What are the signs and symptoms of CTEPD and CTEPH?
CTEPD and CTEPH are difficult to diagnose because the symptoms are nonspecific and can resemble other heart and lung disorders like asthma, chronic obstructive pulmonary disease (COPD), obesity (overweight), and congestive heart failure. Common signs and symptoms include progressive shortness of breath and/or fatigue, especially during exercise or when climbing stairs. When CTEPH develops, more severe symptoms may occur, including fluid retention with swelling of the feet, ankles, legs, and/or abdomen; dizziness or fainting spells; intermittent chest pain, tightness, or pressure; palpitations (heart pounding in the chest); dry cough; and in rare cases, coughing up blood.1–3 The oxygen levels in the blood may become very low, making the lips, fingers, or skin turn blue. 5
What are the potential complications of CTEPH?
High pressures in the arteries of the lungs due to CTEPH can affect the heart. CTEPH can make it harder for the right side of the heart to pump blood into the lungs, resulting in right heart enlargement and failure. Failure of the right side of the heart can also lead to the signs and symptoms described above (fatigue and fluid retention with swelling of the feet, legs, ankles, and abdomen). 5
How are CTEPD and CTEPH diagnosed?
Diagnosis of post-PE syndrome remains challenging because of the nonspecific signs and symptoms, particularly in the early stages. Therefore, following up after an acute PE is crucial in the early detection of CTEPD and CTEPH.
Importantly, patients who experience any of the signs and symptoms described above should be evaluated by their healthcare provider for pulmonary hypertension, even if they do not have a history of blood clots.
To help with diagnosis, the following tests might be performed:
•
•
•
•
•
Table 1 summarizes the similarities and differences between CTEPD and CTEPH.
Similarities and differences between CTEPD and CTEPH.
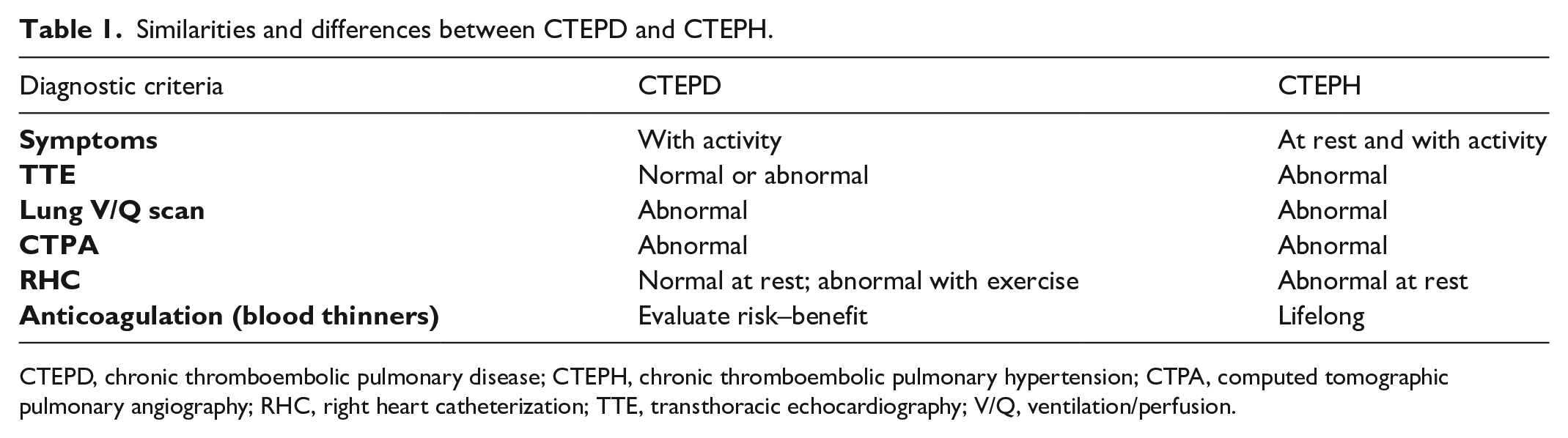
CTEPD, chronic thromboembolic pulmonary disease; CTEPH, chronic thromboembolic pulmonary hypertension; CTPA, computed tomographic pulmonary angiography; RHC, right heart catheterization; TTE, transthoracic echocardiography; V/Q, ventilation/perfusion.
What are the treatments for post-PE syndrome, CTEPD, and CTEPH?
To prevent blood clot recurrence, a lifetime regimen of blood thinners is recommended for patients with CTEPD and CTEPH. Anticoagulants are not necessarily recommended for all patients with post-PE syndrome. The duration of anticoagulation after a PE will depend on the underlying reason for the PE and other patient-related factors, such as bleeding risk and other chronic diseases. Warfarin was used for many years, but a newer type of blood thinner called direct oral anticoagulants (DOACs, e.g., apixaban and rivaroxaban) have been prescribed more frequently over the last decade.8,9 If blood oxygen levels are low, some patients may need supplemental oxygen. Exercise is encouraged and can improve breathing and endurance. To help achieve the goal of restoring the patient to better health, pulmonary rehabilitation programs offer a supervised medical exercise program.
What additional treatment may be needed for CTEPH?
All patients with CTEPH should be evaluated by a multidisciplinary and multispecialty team at an expert center, as outlined in Table 2. Additional treatment may be necessary, including surgery, endovascular therapy (minimally invasive procedures), and other medications. A combination of procedures and/or medical therapy has been increasingly utilized in these patients, as outlined below, and illustrated in Figure 1. 10
•
•
•
Key members of a multispecialty/multidisciplinary physician team for patients with CTEPD and CTEPH.
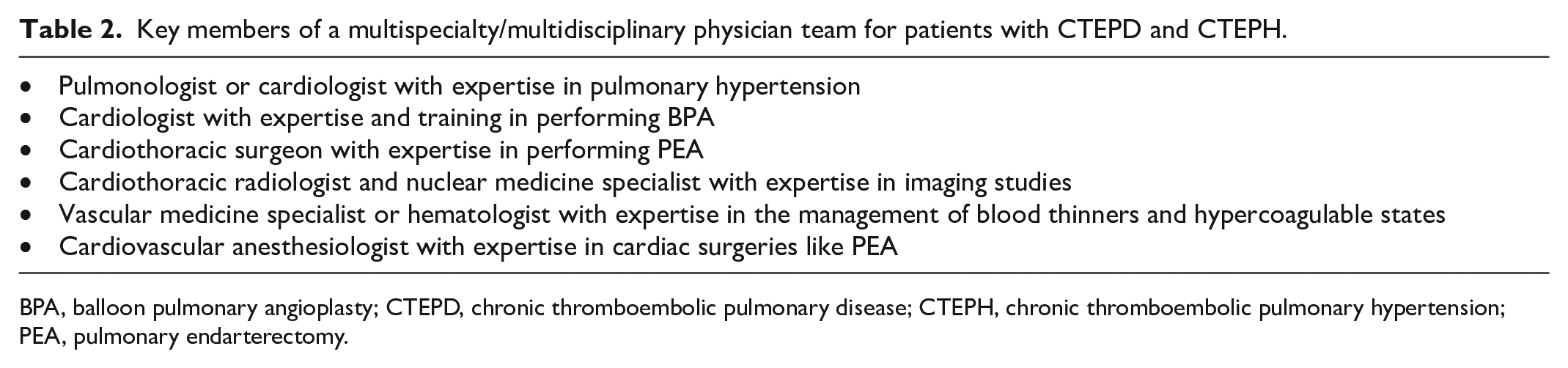
BPA, balloon pulmonary angioplasty; CTEPD, chronic thromboembolic pulmonary disease; CTEPH, chronic thromboembolic pulmonary hypertension; PEA, pulmonary endarterectomy.
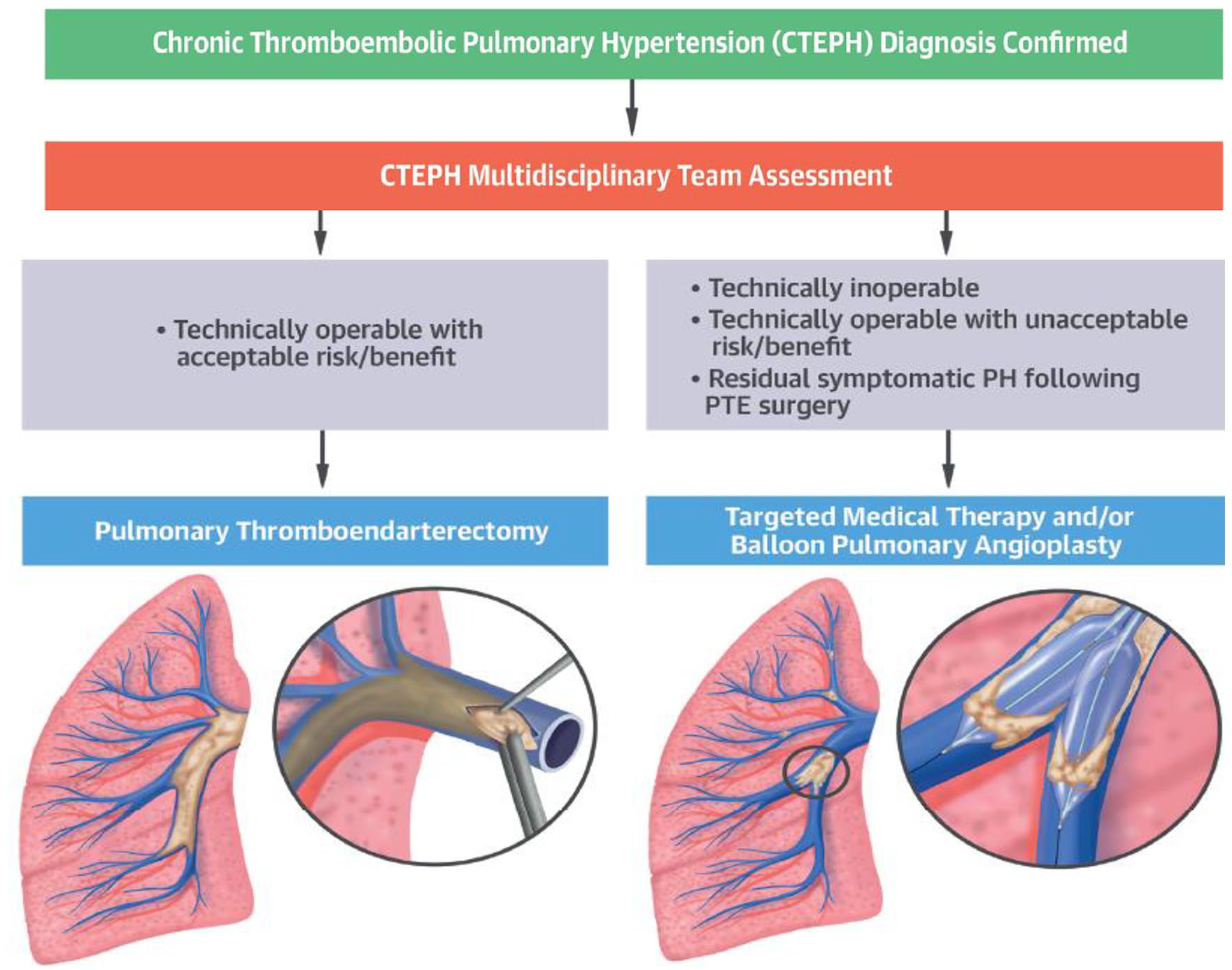
CTEPH multimodality therapeutic algorithm. Once the diagnosis of CTEPH is confirmed, patients are evaluated for PTE surgery. In cases deemed unsuitable for surgery or those with an unacceptable risk for complications during or after the surgery, targeted medical therapy and/or BPA may be considered. Often patients undergo combined medical therapy and BPA for optimal results.
Additional information
The following list includes helpful website resources of professional scientific organizations that provide valuable information for patients with pulmonary hypertension and CTEPH.
• Pulmonary Hypertension Association (PHA)
• International CTEPH Association
• PHA Europe (European Pulmonary Hypertension Association)
• American Thoracic Society (ATS)
• American Heart Association (AHA)
• American College of Chest Physicians (ACCP) Chest Foundation
• National Organization for Rare Diseases (NORD)
• American Lung Association (ALA)
Conclusion
In patients who survived an acute PE episode, the post-PE syndrome may occur, representing a well-known complication. CTEPD and CTEPH may not cause signs or symptoms in the early stages but represent important long-term consequences of PE. They may also develop in patients without a prior history of blood clots. Diagnostic testing can differentiate CTEPD from CTEPH. A specialized, multidisciplinary team can personalize evaluation and treatment, with the goals of improving quality of life and survival.
Footnotes
Acknowledgements
A Spanish translation of this article is available online. 11
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
Dr Elizabeth Ratchford’s work was supported in part by the generosity of David Kotick (1926–2021).