
Abstract

Keywords
Fibromuscular dysplasia (FMD) is a nonatherosclerotic, noninflammatory arteriopathy associated with vessel tortuosity, stenosis, aneurysm, and dissection. There is a concern that patients from minoritized racial and ethnic groups and those with lower socioeconomic status are underdiagnosed and underrepresented in clinical trials and registries. Currently, the North American Registry for FMD shows a predominance of White patients being affected (95.4% White vs 4.6% non-White). 1 However, there is no indication that FMD is genetically associated with any race. Thus, this report aims to identify racial differences in patients with FMD.2,3
A single-center retrospective chart review was performed on patients who were seen by an Emory FMD clinician from 01/01/2012 to 01/01/2022, ages 18–100 years. Patients without a confirmed FMD diagnosis or diagnostic imaging, lacking self-identifiable data on race, or < 18 or > 100 years old were excluded. Patients who identified as Asian (n = 1), the only other race identified, were excluded from the analysis due to small sample size. Notably, patients with Hispanic ethnicity also had a small sample size (n = 6), so were grouped according to their self-identified race. Institutional review board approval was obtained through Emory University. Demographics, diagnosis, treatment, and outcome variables were obtained. Further analysis was performed to compare socioeconomic status based on zip code, distance traveled, and insurance status.
A total of 201 patients (79% White, 21% Black) were included in the analysis. Black patients, compared to White patients, were more likely to have hypertension (p = 0.031), diabetes (p = 0.049), cerebrovascular accident (CVA) (p = 0.014), and chronic kidney disease (CKD) (p = 0.007), and were prescribed more antihypertensives (p = 0.020). Black patients had a longer mean time from first symptom and/or FMD-related medical diagnosis to FMD diagnosis compared to White patients (5.67 vs 1.1 years, p < 0.001). The first symptom and/or FMD-related medical diagnosis was defined as the first report of chronic headaches/migraines, tinnitus, syncope, chest pain, dizziness, myocardial infa-rction (MI), CVA, transient ischemic attack (TIA), aneurysms, or dissection. Differences were also found in White versus Black patients’ comorbidities and medi-cal history (diagnoses existing on presentation to FMD clinic).
Diagnostic testing performed demonstrated that White patients had a greater number of imaging studies (5+) compared to Black patients (96% vs 79%, p < 0.001), yet had a similar likelihood of completed ‘head to pelvis’ computed tomography angiography (CTA) imaging (CTA of head, neck, chest, abdomen, and pelvis) (54.7% vs 57.1%, p = 0.779). Vascular bed involvement differed between racial groups. White patients had more involvement of the renal artery (50% vs 24%, p = 0.002), whereas Black patients had more involvement of the internal carotid artery (95% vs 78%, p = 0.010) and upper-extremity arteries (5% vs 0%, p = 0.006) (Table 1).
Demographics, medical history, presenting symptoms, and vascular territories in patients with fibromuscular dysplasia (FMD) stratified by race.
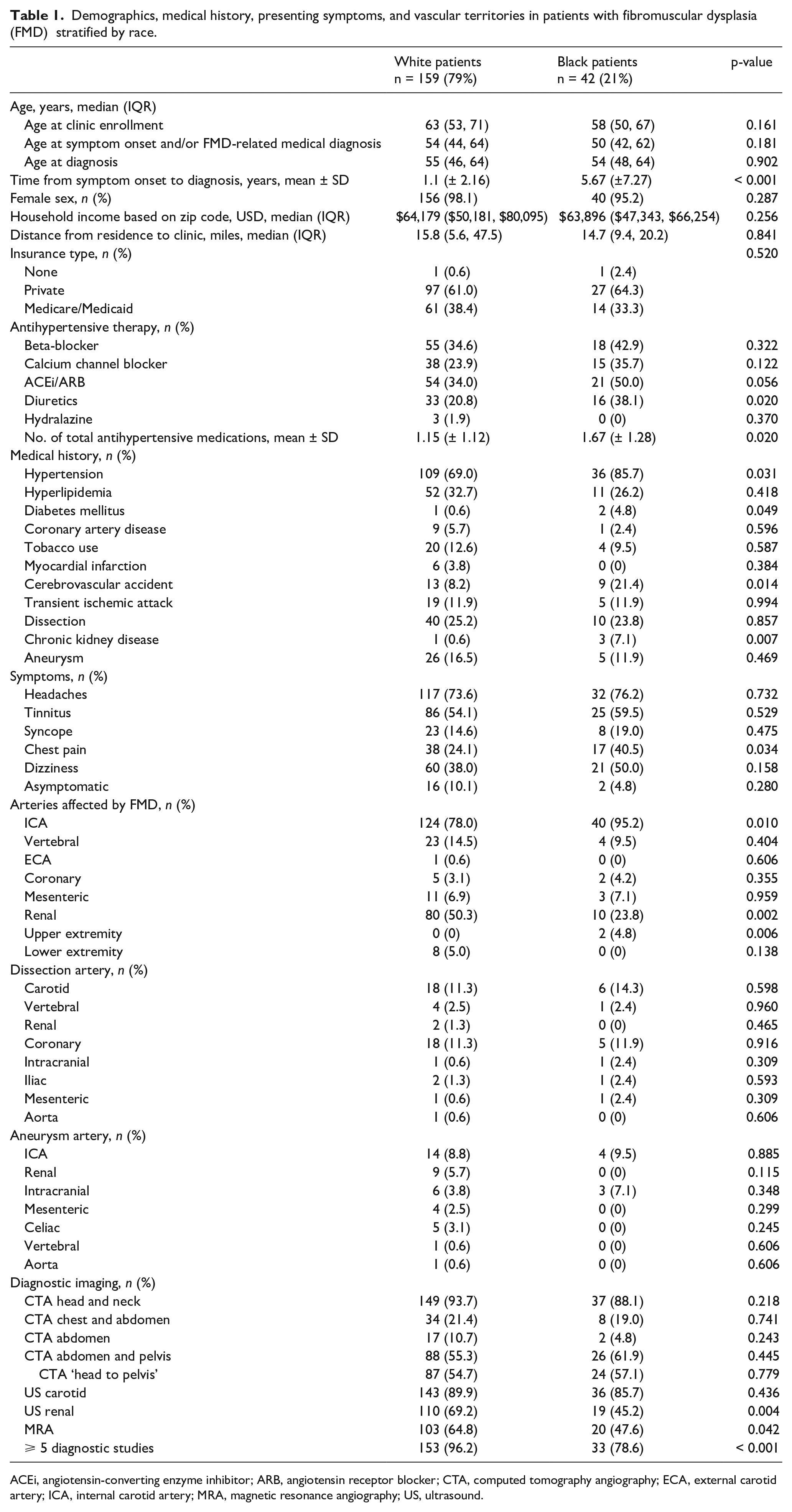
ACEi, angiotensin-converting enzyme inhibitor; ARB, angiotensin receptor blocker; CTA, computed tomography angiography; ECA, external carotid artery; ICA, internal carotid artery; MRA, magnetic resonance angiography; US, ultrasound.
Among a single-center population of patients with FMD that is more diverse compared to the US National FMD Registry, we found that it took longer to diagnose Black patients with FMD from initial symptom/FMD-related diagnosis, and they received less imaging when compared to their White counterparts. 1 Our findings suggest there may be racial differences among patients with FMD that are underreported, possibly due to decreased access to providers specializing in FMD and/or access to hospitals that are registry sites, and/or lower suspicion of FMD by providers evaluating these patients. Prior studies have reported FMD as a disease primarily of White patients, potentially leading to systemic detection bias. The time to diagnosis for Black patients being longer compared to White FMD patients is likely multifactorial, with potential barriers within the social and healthcare system for Black versus White patients – leading to potential negative repercussions in the patients’ care and outcomes.1,4,5 Additionally, the discrepancies in diagnostic studies performed have not been fully investigated. A potential explanation is that White patients receive more thorough imaging and surveillance to evaluate for FMD and progression of aneurysms and dissections, whereas Black patients receive more focused diagnostic imaging by anatomical location of the reported condition. Furthermore, Black patients had a significantly higher percentage of CVAs compared to White patients, yet not a higher percentage of dissections. Thus, the etiology of the CVA may be more likely attributed to dissection in White patients and CVA in Black patients may be due to traditional risk factors such as hypertension and diabetes.
This study has limitations to consider. It is retrospective in nature, derived from single-center data, and a smaller sample size. Further, although diverse, our population may not be fully representative of minoritized or lower socioeconomic status patients. Notably, Black patients in this study had similar household income and percentage of private health insurance as their White counterparts, suggesting similar socioeconomic status. Patients seen by Emory FMD clinicians may have greater access to care and financial stability due to the required insurance and copays.
In conclusion, this study found racial differences in the time to diagnosis, comorbidities, and diagnostic imaging among patients with FMD. The difference in population of the National FMD Registry compared to the patients seen at the Emory FMD Clinic suggests institutional differences of FMD and the need for increased awareness of minoritized patients in registries and other studies. Research is needed to further investigate these racial differences.
Footnotes
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.