
Abstract

Keywords
Spontaneous coronary artery dissection (SCAD) is an important cause of acute coronary syndrome (ACS) in women. The reported average age of women with SCAD ranges from 45 to 53 years, although it also occurs with less frequency in older patients.1,2 Some prior SCAD studies have excluded older patients, 3 and it remains unknown whether patient demographics, clinical presentation, presence of extracoronary vascular abnormalities (EVAs), or management differ by age of presentation. To address this knowledge gap, we performed a single-center retrospective study of all consecutive patients with a clinical history of SCAD who were referred to the Vanderbilt University Medical Center SCAD Clinic from June 2017 to June 2021. This study was approved by the local institutional review board.
We systematically recorded details regarding medical history, prior noninvasive imaging, and coronary angiography. All patients underwent brain-to-pelvis computed tomography angiography (CTA) imaging to evaluate for EVAs. 1 Patients were stratified into three age groups: < 40, 40–59.9, and ⩾ 60 years old. We reported descriptive statistics on demographic and clinical characteristics, including mean (SD) and n (%) by age groups. We evaluated differences between age groups using Kruskal–Wallis tests for continuous variables and Pearson chi-squared tests or Fisher’s exact tests for categorical variables.
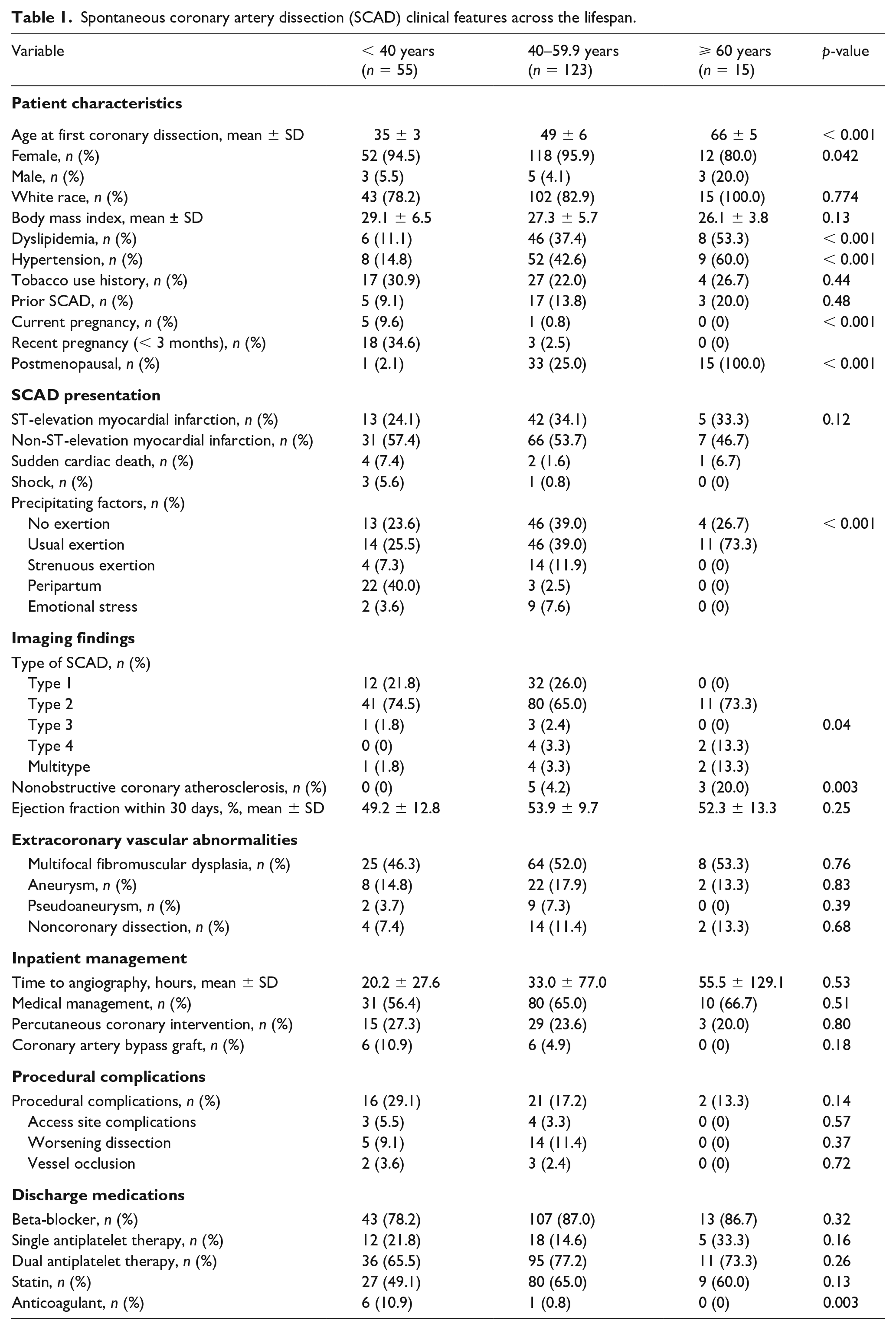
We included 193 patients, 94.3% of whom were women (Table 1). Prevalence of hypertension (14.8%, 42.6%, 60%, p < 0.001), dyslipidemia (11.1%, 37.4%, 53.3%, p < 0.001), and nonobstructive coronary atherosclerosis (0%, 4.2%, 20.0%, p = 0.003) increased across age groups. Precipitating factors were significantly different among age groups with self-reported usual exertion more commonly seen in the older cohort (25.5%, 39%, 73.3%, p < 0.001) versus self-reported strenuous exertion seen in the younger cohorts (7.3%, 11.9%, 0%, p < 0.001). Compared to older patients, younger patients had a higher prevalence of peripartum SCAD (40%, 2.5%, 0%, p < 0.001), and were more frequently discharged on anticoagulation (10.9%, 0.8%, 0%, p < 0.003). There were no significant differences in SCAD presentation or vessel involvement. EVAs, including multifocal fibromuscular dysplasia (FMD) (46.3%, 52.0%, 53.3%, p = 0.76), were highly prevalent across age groups. Of note, all instances of FMD were multifocal, rather than focal. The vascular distribution of FMD did not vary by age except for brachial artery FMD (0%, 0%, 12.5%, p = 0.004) (online supplemental Table 1). Inpatient SCAD management and procedural complications were no different between groups.
Spontaneous coronary artery dissection (SCAD) clinical features across the lifespan.
Older adults have been excluded from some SCAD cohort studies because it was believed spontaneous dissection could not be clearly delineated from atherosclerotic dissection. 3 To address this selection bias, we evaluated for coronary atherosclerosis through independent review of angiography and CTA images by a vascular cardiologist. Though our study demonstrated increased prevalence of nonobstructive coronary atherosclerosis with age, this was rare overall (4.3%), with no evidence of angiographically significant (e.g., > 50%) stenoses. This reinforces that SCAD is a distinct, nonatherosclerotic phenotype across the lifespan. Prior data from a single-center Chinese study of older individuals with SCAD (mean age 57.4 years) demonstrated concomitant coronary atherosclerosis in 72% of patients. 4 Whether this simply reflects differences in the prevalence of coronary atherosclerosis in these distinct patient populations or represents different SCAD phenotypes among different ethnic groups remains unclear, and this warrants further exploration in other cohort studies. Additionally, although we found the proportion of men with SCAD was highest in the > 60 years old age group, the number of men overall was low in our cohort. This should be further examined in larger cohorts.
EVAs, a well-documented association with SCAD, result in increased vessel wall fragility.5,6 No study to date has evaluated EVAs in elderly individuals through complete vascular imaging. EVAs, including fibromuscular dysplasia, aneurysm, pseudoaneurysm, and noncoronary dissection, were highly prevalent in all age groups. This further emphasizes the importance of cross-sectional brain-to-pelvis imaging to identify and manage these EVAs longitudinally regardless of age of presentation.1,7 Our findings of the high prevalence of EVAs match that of contemporary studies.8,9 For instance, the overall prevalence of EVAs in the iSCAD Registry was 43.3%, 8 and the prevalence of FMD among patients screened for EVAs in the Canadian SCAD registry was 50.2%. 9
This study has several limitations. Its cross-sectional design prevents the evaluation of long-term outcomes, including rehospitalization or recurrence. The clinical suspicion for SCAD may be lower in older patients, raising concern for underdiagnosis, which would be consequential in our smaller, single-center cohort. Additionally, full details regarding the rationale for specific medical therapies were incomplete.
Nevertheless, this study highlights that SCAD affects women at any age. We observed similar presentation, imaging findings, and management across groups. This suggests that the underlying SCAD pathogenesis is consistent across the lifespan. Accurate disease recognition is important in an older SCAD demographic, even with a higher prevalence of coronary atherosclerosis, as prevalence of EVAs is similar to that of younger patients with SCAD. Further studies should focus on determinants of age at first SCAD event, with particular emphasis on the contribution of hormonal, mechanical, and genetic factors.
Supplemental Material
sj-docx-1-vmj-10.1177_1358863X231191901 – Supplemental material for Prevalence of extracoronary vascular abnormalities does not vary by age of presentation in patients with spontaneous coronary artery dissection (SCAD)
Supplemental material, sj-docx-1-vmj-10.1177_1358863X231191901 for Prevalence of extracoronary vascular abnormalities does not vary by age of presentation in patients with spontaneous coronary artery dissection (SCAD) by Jacqueline M Visina, Nowrin Haque, Shi Huang, Aaron W Aday and Esther SH Kim in Vascular Medicine
Footnotes
Declaration of conflicting interests
Dr Aday reports receiving consulting fees from Aeglea outside of the current work. The remaining authors have nothing to disclose.
Funding
This work was supported by the National Institutes of Health under Award Number K23 HL151871 (Dr Aday).
Supplementary material
The supplementary material is available online with the article.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.