
Abstract

Keywords
Numerous studies confirm that residual pulmonary vascular occlusion (RPVO), prevalent in 20–50% of cases, significantly increases the recurrence risk of venous thromboembolic events (VTE).1–3 Initially designed to predict pulmonary embolism (PE) mortality, the pulmonary vascular obstruction index (PVOI) was quantified using angiographic scores like the Miller score. With the development of computed tomography pulmonary angiograms (CTPA), Qanadli et al. introduced a score considering clot location and residual perfusion, demonstrating good reproducibility and correlation with angiographic scores. 4 While early PVOI quantification did not show value in PE prognosis, a correlation between PVOI at diagnosis and RPVO emerged. 5 We conducted a retrospective study to determine the relationship between the initial PVOI and the VTE recurrence in a cohort of patients with unprovoked PE. We performed a subgroup analysis in men in whom unprovoked PE is associated with a high risk of recurrence. Recurrent VTE occurrences were captured through electronic medical records, and all patients, as well as their family doctors, were contacted via phone calls to ascertain whether they had experienced a recurrent VTE. The study was approved by the local ethical committee.
Between January 2014 and June 2016, 1067 CTPA were collected, yielding 588 eligible cases with confirmed PE diagnoses (online supplementary Table 1). Among these cases, 500 were excluded: 284 (56.8%) for provoked PE, 130 (26.0%) for long-term anticoagulation (29 had atrial fibrillation, 19 had chronic thromboembolic pulmonary hypertension), 60 (12%) for missing data or early loss of follow up, and 26 (5.2%) died within 3 months following the PE. The remaining 88 patients were included for analysis. Of these, 61.4% (n = 54) were women, mean age 56 ± 19.3 years. VTE risk factors included obesity (42%), superficial venous insufficiency (34.1%), and oral contraceptives (20.5%). Most patients (59.1%) received direct oral anticoagulants (DOACs) for an average of 19.6 ± 16.4 months. PE was isolated in 67%, predominantly proximal (60.4%). The Qanadli score indicated a mean pulmonary vascular obstruction of 32.9% (σ = 23%), with > 40% obstruction in 38.6% of patients. Inter-observer agreement for the score had a mean difference of 3.2%, with good reproducibility. Over a median 4.1-year follow-up for postanticoagulant treatment, 28 patients (31.8%) had VTE recurrence, resulting in an 8.5% recurrence rate per patient-year. PVOI ⩾ 40% significantly lowered recurrence-free survival compared to PVOI ⩽ 40% (p < 0.001) (Figure 1). The cumulative recurrence incidence at 5 years was 72.37% for PVOI > 40% versus 15.40% for PVOI ⩽ 40%. PVOI did not significantly impact overall recurrence-free survival. In the subgroup of men (n = 34), PVOI ⩾ 40% correlated with an 85.71% 5-year recurrence risk compared to 18.8% for PVOI ⩽ 40% (p < 0.001). In multivariable analysis, only PVOI ⩾ 40% (hazard ratio (HR) = 10.3; 95% CI 2.44–43.58) and personal history of VTE (HR = 8.15; 95% CI 2.17–30.48) were associated with VTE recurrence. The optimal PVOI threshold associated with the highest area under the curve was for VTE recurrence was 39% for VTE (sensitivity = 0.69; specificity = 0.8).
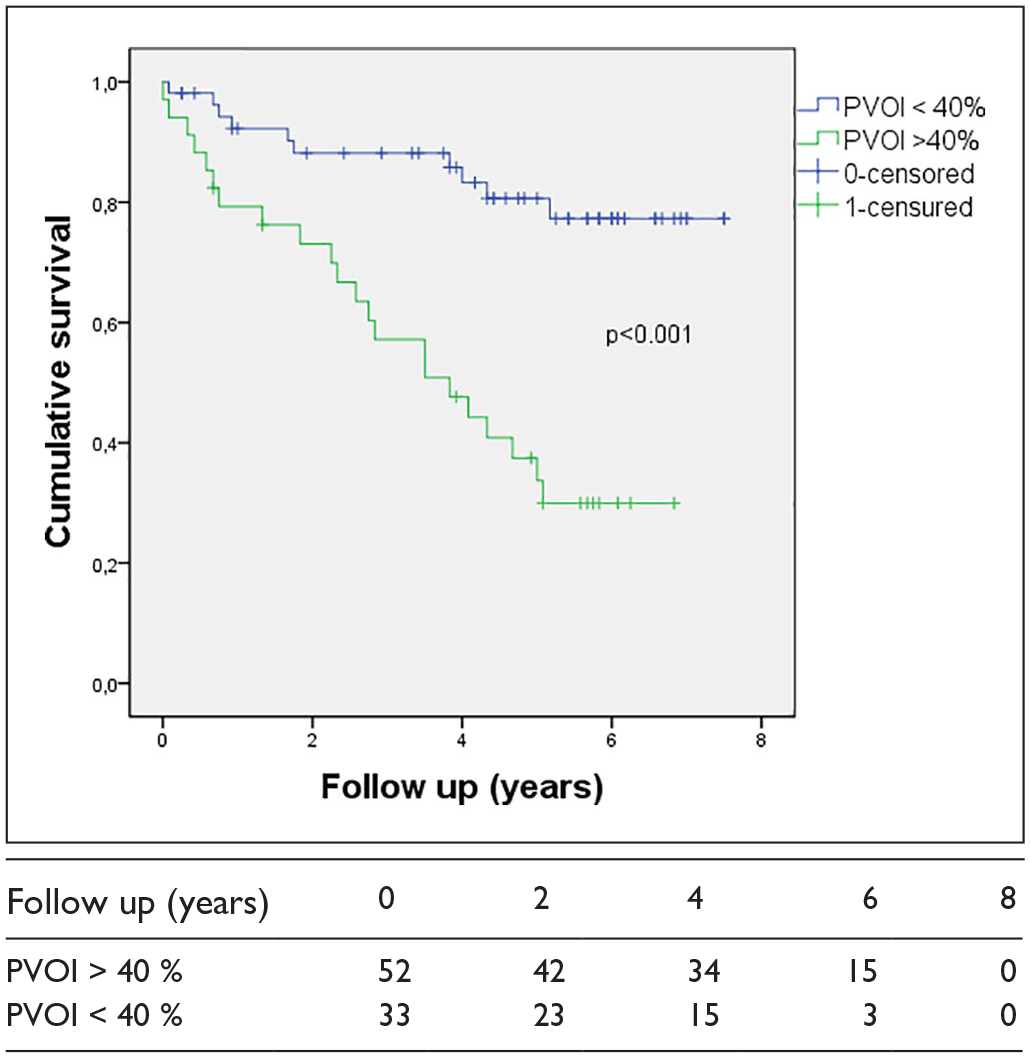
Cumulative survival for recurrent thromboembolic event or death related to thromboembolic disease (log-rank p < 0.001).
In this retrospective study of 88 patients with unprovoked PE anticoagulated for ⩾ 3 months, an initial PVOI ⩾ 40% on CTPA independently predicted recurrent VTE postanticoagulation cessation. Patients with unprovoked PE experience an almost 10% annual recurrence risk, constituting a group for which the prolongation of anticoagulation is debated.6,7 Although the HERDOO2 rule identifies a low risk of VTE recurrence subgroup, it applies to only 12% of patients. 8 We included patients between 2014 and 2016 when anticoagulant interruptions were more common and DOAC use was prevalent. The Qanadli score for initial PVOI estimation and a ⩾ 40% PVOI threshold was chosen based on studies demonstrating its discriminatory ability for recurrence risk in unprovoked populations. 9 ROC curve analysis confirmed its sensitivity and specificity trade-off. Our study found an independent association between PVOI ⩾ 40% and increased recurrence risk of VTE. Subgroup analysis of men revealed a significantly higher 5-year recurrence risk for PVOI ⩾ 40%.
Although the recurrence rate is higher in the group with an initial obstruction of more than 40%, this rate remains unacceptable to solely guide the decision to discontinue anticoagulant treatment. 10 It would be interesting in future research to associate initial PVOI with clinical and biological parameters to define a group of patients in which stopping anticoagulant treatment can be safely considered. Incorporating PVOI into existing scoring systems could refine recurrence risk stratification, particularly in men.
Supplemental Material
sj-pdf-1-vmj-10.1177_1358863X241239648 – Supplemental material for Pulmonary vascular obstruction increases the risk of recurrent thrombotic events after cessation of anticoagulation in unprovoked pulmonary embolism: A retrospective cohort study
Supplemental material, sj-pdf-1-vmj-10.1177_1358863X241239648 for Pulmonary vascular obstruction increases the risk of recurrent thrombotic events after cessation of anticoagulation in unprovoked pulmonary embolism: A retrospective cohort study by Romain Stichelbout, Calliste Sinzogan Eyoum, Paul Billoir, Ygal Benhamou, Matthieu Demeyere and Sebastien Miranda in Vascular Medicine
Footnotes
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Supplementary material
The supplementary material is available online with the article.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.