
Abstract
Keywords
Vascular medicine specialists have been integral in the evaluation, diagnosis, and treatment of venous thromboembolism (VTE) but its role in inferior vena cava (IVC) filter placement and management is not well established. Societal guidelines for IVC filters have a strong history in interventional societies but the importance of input from medical societies is now recognized. 1 The goal of this study was to evaluate the impact of vascular medicine involvement in initial IVC filter utilization in hospitalized patients. After institutional review board approval of data collection and analysis, inpatient consults to vascular medicine from June 1, 2018 to December 31, 2022 were identified using a text-based search to select consults with the word ‘filter’. Manual review removed duplicate patients and identified only consults requesting evaluation for initial IVC filter placement. Excluded consults were those with questions about IVC filters already in place, IVC filter thrombosis, or IVC filter removal. Additional chart review determined if vascular medicine follow-up, either inpatient or outpatient, occurred between placement and retrieval of the IVC filter. The type of filter, indication, and time to retrieval when vascular medicine was involved were cross-referenced to data in an institutional tracking system.
Vascular medicine specialists received IVC filter consults on 496 unique patients, 360 for initial evaluation of IVC filter insertion. Vascular medicine specialists recommended IVC filter placement in approximately one-third of consults per year (26–35%, online Supplemental Table). Over the study timeframe, 114 out of 360 consults (31.7%) ultimately had IVC filters placed for treatment of VTE (95.6%), mostly in the setting of bleeding concerns (>90%), with predominantly retrievable filter types (86.0%). This demonstrates that vascular medicine specialists identified alternative strategies to IVC filter placement in an average of 68% of consults. From 2019 to 2021, the annual percentage of filters avoided was steady but increased to 74% in 2022. Vascular medicine consultation contributed to lower IVC filter use at our institution with an estimated cost saving of $525,000 to $765,000 annually for placement (based on an estimate of $15,000 per procedure). 2 Cost savings are even higher if costs for removal are factored in.
Retrieval of IVC filters recommended by vascular medicine was variable from 17% to 55%, with average time to removal of 131 days from 2019 to 2022 (online Supplemental Table). Evaluating the degree of vascular medicine follow-up after IVC filter placement emphasized the impact of vascular medicine. Vascular medicine inpatient evaluation resulted in the follow-up of 63% of IVC filter patients, with increased annual retrieval between 50% and 83% per year. Annual retrieval when vascular medicine follow-up occurred increased from 2019 to 2021 but decreased in 2022 for unclear reasons (Figure 1). Of the 42 hospitalized patients vascular medicine evaluated but did not follow-up, 34 had retrievable IVC filters and 18% were removed. Overall, when vascular medicine follow-up occurred, retrieval was always higher than patients without vascular medicine follow-up, equaling a 42% cumulative increase in retrieval with vascular medicine involvement. Five patients seen in follow-up underwent shared decision-making to defer removal due to health status, difficult access based on imaging, or desire to avoid further procedures.
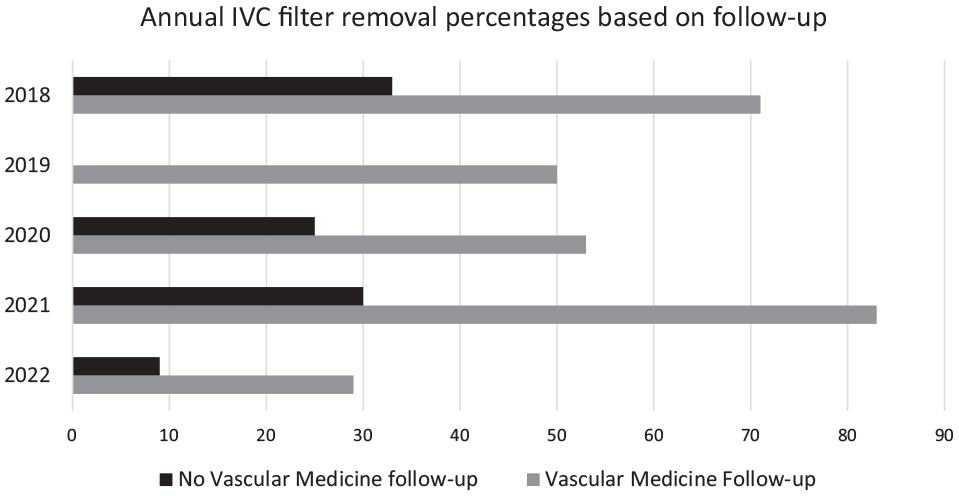
Vascular medicine consult follow-up and IVC filter retrieval percentages by year.
Retrieval was complicated by sick patients with high mortality, noting that in patients without IVC filter removal, 37.7% died within 3 months, 46.4% died within 6 months, and 58% died within 1 year of placement. Malignancy was noted in 45.3% of patients who were evaluated by vascular medicine overall; more specifically, 53.8% of those who died within 3 months, 59.4% of those who died within 6 months, and 67.5% of those who died within 1 year of IVC filter placement, reinforcing that both death and cancer limit retrieval rates. 3 Thus, it also appears that vascular medicine specialists contributed to appropriate deferral of IVC filter retrieval in patients with limited life expectancy where there would be no clear benefit to retrieval.
The retrieval rates analyzed were influenced by a vascular medicine-led multispecialty endeavor initiated to increase vena cava filter tracking, which was started in 2016. 4 Vena cava filters placed at Mayo Clinic in Rochester, MN were entered into a tracking system maintained by vascular nurses to increase appropriate follow-up and removal when indicated. Though no restrictive institutional policies were initiated, there was a steady reduction of vena cava filter use from 2016 to 2019 without an increase in inpatient mortality. In 2019, there were 120 vena cava filters placed, a 50% reduction from 2016, which had a preemptive impact on retrieval rates analyzed in this study, as the annual percentage has minimally changed from 2019. Additionally, evaluating patients at a tertiary facility with a referred population also creates limitations and increases loss to follow-up, despite efforts by nurses to contact patients and facilitate appropriate retrieval.
Vascular medicine was not involved in all initial IVC filter placement decisions; however, this analysis focused on formal consults with a question of IVC filter use and could not assess the impact of informal ‘curbside’ consults or cases where vascular medicine specialists recommended filter use without the question being posed in the consult. Additionally, this analysis focused on consults where vascular medicine providers had the opportunity to impact filter placement and excluded consults after IVC filter placement. A total of 13 consults regarding IVC filters to other inpatient services such as internal medicine, vascular surgery, orthopedic surgery, hematology, and trauma/general surgery were found, but only two consults had the question of initial placement, and no direct consults to interventional radiology were identified. Minimal consults to other inpatient services demonstrate a preference for vascular medicine involvement. IVC filters placed without vascular medicine consults combine inpatient services that place requests directly to interventional radiology and outpatient IVC filter placement.
This analysis demonstrates the role of vascular medicine in clarifying the risks, benefits, and alternatives for IVC filter placement, given vascular medicine specialists’ extensive knowledge of, and experience with, IVC filters as well as varying types of anticoagulants and their indications. Bringing that knowledge to the bedside emphasizes engagement in shared decision-making with the patient, which is critical in these complex and high-risk patients. This specialized knowledge base overcomes the perceived need for IVC filters in many patients who were evaluated by vascular medicine, noting that 68% of consults resulted in deferral of IVC filter placement. Subsequent, intentional vascular medicine follow-up after IVC filter placement allowed for vascular medicine to determine if anticoagulation and risk factors were acceptable to negate the need for ongoing IVC filters and individualize patient evaluation to improve retrieval rates. In conclusion, these data indicate that vascular medicine involvement positively influences both use of IVC filters and retrieval rates within our facility.
Future initiatives led by vascular medicine to continue to improve evaluation, tracking, and follow-up would benefit the facility. Focusing on implementing vascular medicine-initiated participation in IVC filter evaluation, instead of the passive involvement analyzed in this review, would extend vascular medicine influence to ensure that institutional IVC filter use is appropriate and retrieval is thoughtfully maximized.
Supplemental Material
sj-pdf-1-vmj-10.1177_1358863X231224326 – Supplemental material for Impact of vascular medicine specialists on inpatient utilization and management of inferior vena cava filters
Supplemental material, sj-pdf-1-vmj-10.1177_1358863X231224326 for Impact of vascular medicine specialists on inpatient utilization and management of inferior vena cava filters by Danielle T Vlazny and Damon E Houghton in Vascular Medicine
Footnotes
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
This study was supported by a Building the Evidence Base for Vascular Medicine Award from the Society for Vascular Medicine.
Supplementary material
The supplementary material is available online with the article.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.