
Abstract
Retrievable inferior vena cava (IVC) filters are increasingly used in patients with venous thromboembolism (VTE) who have contraindications to anticoagulant therapy. However, previous studies have shown that many retrievable filters are left permanently in patients. This study aimed to identify the common indications for IVC filter insertion, the filter retrieval rate, and the predictive factors for filter retrieval attempts. To this end, a retrospective cohort study was performed at a tertiary care center in South Korea between January 2010 and May 2016. Electronic medical charts were reviewed for patients with pulmonary embolism (PE) who underwent IVC filter insertion. A total of 439 cases were reviewed. The most common indication for filter insertion was a preoperative/procedural aim, followed by extensive iliofemoral deep vein thrombosis (DVT). Retrieval of the IVC filter was attempted in 44.9% of patients. The retrieval success rate was 93.9%. History of cerebral hemorrhage, malignancy, and admission to a nonsurgical department were the significant predictive factors of a lower retrieval attempt rate in multivariate analysis. With the increased use of IVC filters, more issues should be addressed before placing a filter and physicians should attempt to improve the filter retrieval rate.
Keywords
Introduction
Inferior vena cava (IVC) filters are vascular devices implanted to prevent pulmonary embolism (PE), which can lead to fatal consequences. 1 With the improvements in insertion techniques, it has become easier to place IVC filters. 2 In addition, the introduction of retrievable filters has encouraged the use of IVC filters.3,4 The idea that retrievable filters can be an option for patients with transient contraindications to anticoagulation is attractive. However, in practice, many inserted filters are left permanently in patients. According to a recent systematic review of 37 studies, the overall filter removal rate was only 34%. 5
The result of the PREPIC 2 study showed no benefit of IVC filters in anticoagulated patients with acute PE as compared with patients receiving anticoagulation alone. 6 IVC filters are not harmless; they are associated with several complications, including filter migration, filter strut fracture, organ penetration, recurrent deep vein thrombosis (DVT), and vena cava thrombosis. 7 Despite the potential complications, the risk of retained filters tends to be underestimated in clinical practice.
Only a few studies have previously investigated the factors predictive of retrieval success,8–12 and there has been no report from Asia about the retrieval success rate and the factors associated with retrieval attempts. To analyze the current pattern of IVC filter insertion and the reasons for the low retrieval rate, we aimed to identify the common indications for IVC filter insertion, the filter retrieval rate, and the factors associated with retrieval attempts.
Methods
Study design and subjects
We performed a retrospective cohort study of patients with PE at Asan Medical Center, a 2700-bed tertiary care center in South Korea, between January 2010 and May 2016. Patients aged 18 years or older and with a consultation record for IVC filter insertion were screened for the study. The diagnosis of PE and DVT was made by each attending physician based on the imaging findings from pulmonary computed tomography (CT) angiography, a ventilation/perfusion scan, lower extremity venographic CT, and lower extremity venous Doppler ultrasound. All images were initially read by radiologists at our institution, and each CT and ultrasound image was checked once more by the authors.
Filter placement and retrieval
Interventional radiologists placed all IVC filters. IVC filter insertions were performed in an angiography suite with venographic and fluoroscopic guidance. Filters were placed infrarenally unless otherwise indicated. Celect filters (Cook Medical, Bloomington, IN, USA) and OPTEASE filters (Cordis, Milpitas, CA, USA) were used in 415 and 24 patients, respectively.
Retrieval of the IVC filter was considered in patients who could undergo anticoagulation and were considered to have a low risk for venous thromboembolism (VTE) at the time of retrieval. There was no defined protocol for the retrieval of filters or the timing of retrieval; the decision to remove the filter depended on each case. Filter retrieval was performed via the Günther Tulip vena cava filter retrieval set (Cook Medical).
Data collection
Clinical characteristics were collected from the medical charts, including electronic medical records and the Asan Biomedical Research Environment. The electronic medical records of 445 cases were manually reviewed for age, sex, body mass index, admitting services, risk factors for VTE, medical comorbidities, date of filter insertion and removal, filter complications, presence of DVT, and severity of PE. The severity of PE was calculated by using the simplified Pulmonary Embolism Severity Index. 13
The study was approved by the institutional review board (IRB) of Asan Medical Center (IRB no. 2015-0516). The need for informed consent was waived owing to the retrospective nature of the study. Moreover, we used encoded numbers for patient identification to maintain confidentiality.
Statistical analysis
Descriptive statistics are provided for patient demographics. The data are presented as means and standard deviations for continuous variables, whereas the indwelling time of IVC filters is presented as median and range. Categorical variables are presented as numbers (%). Variables were chosen as candidates for multivariable analyses with binary logistic regression if they were statistically significant in the univariate analysis using the chi-squared test. P-values < 0.05 were considered statistically significant. Data were analyzed by using SPSS version 21 (IBM Corp., Armonk, NY, USA).
Results
Clinical characteristics of patients
A total of 445 cases were reviewed for the analysis, and four cases were excluded because IVC filter insertion was not performed. Another two cases without evidence of PE were excluded because of possible heterogeneity in clinical characteristics and the small number (two); thus, 439 cases were eventually included in the analysis. Two patients underwent IVC filter placement twice. One patient experienced bleeding during anticoagulation after filter removal and required reinsertion of the IVC filter. Another patient was scheduled for surgery after the first filter had been removed, and decided to undergo filter insertion for the second time.
The clinical characteristics of the patients are described in Table 1. The mean patient age was 60.3 years, and 255 patients (58.1%) were women. A total of 220 IVC filter insertions (50.1%) were ordered from the medical department and 219 cases (49.9%) were ordered from the surgical department. More than half of the patients had an active malignancy at the time of PE diagnosis. The most common malignancy was lung cancer (38 cases, not shown in the table). In 359 cases (81.8%), DVT was found concurrently with PE. Right ventricular dysfunction was also present in 98 patients (22.3%).
Clinical characteristics of patients.
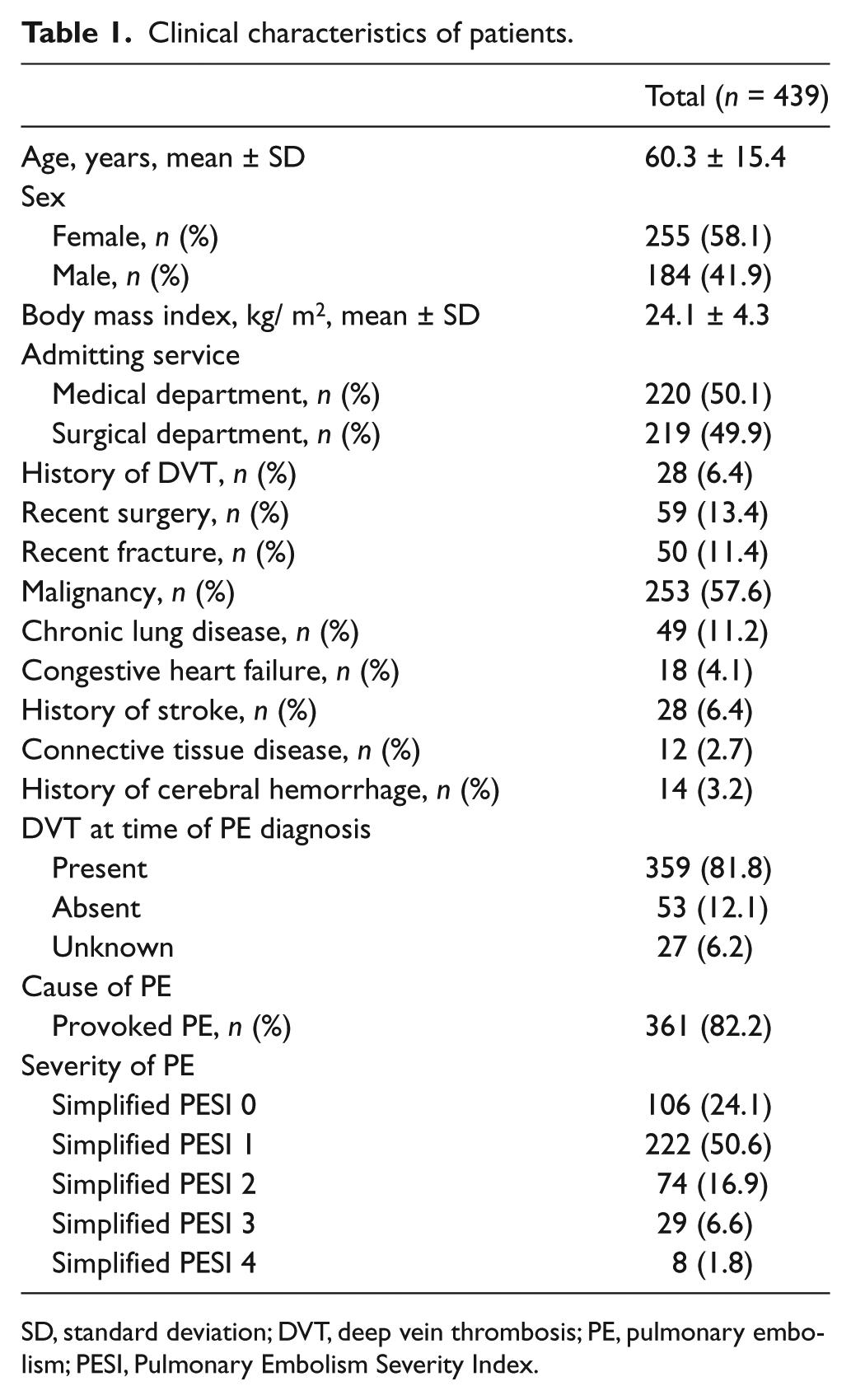
SD, standard deviation; DVT, deep vein thrombosis; PE, pulmonary embolism; PESI, Pulmonary Embolism Severity Index.
Indications for filter insertion
We found six common indications for IVC filter insertion (Table 2). The most frequent indication was preoperative/procedural insertion in 136 cases (31.0%), followed by extensive iliofemoral DVT in 105 patients (23.9%). In 71 patients (16.2%) and 30 patients (6.8%), an IVC filter was implanted because of a contraindication to anticoagulation and complication of anticoagulation, respectively. Medical therapy had failed in 19 patients (4.3%). Nine IVC filters (2.1%) were inserted in patients with poor cardiopulmonary reserve. For 69 cases (15.7%), the reason for filter insertion was unclear, despite a thorough review of the medical charts.
Indications for IVC filter insertion.
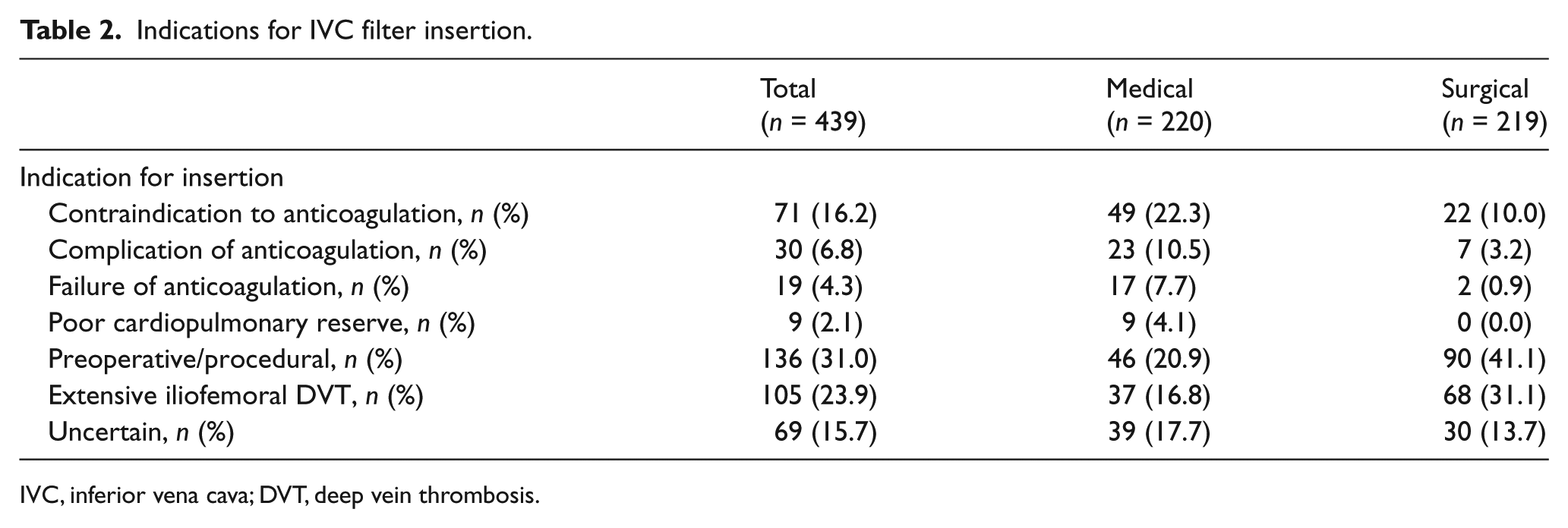
IVC, inferior vena cava; DVT, deep vein thrombosis.
Rates of filter retrieval
A total of 197 trials (44.9%) of filter retrieval were made, and 185 filters were successfully removed (42.1%) (Table 3). The success rate was 93.9%. Among 12 patients in whom filter removal failed, IVC thrombus was found in seven patients when filter retrieval was attempted. Anticoagulation therapy was maintained in these patients and a second trial was not attempted in four of these patients. Meanwhile, in another two patients, thrombus was resolved, but removal was not possible because the filter was embedded in the IVC. In the remaining patient, an IVC thrombus was still noticed when the second trial was made after 2 weeks and the filter was retained.
Rates of filter retrieval.
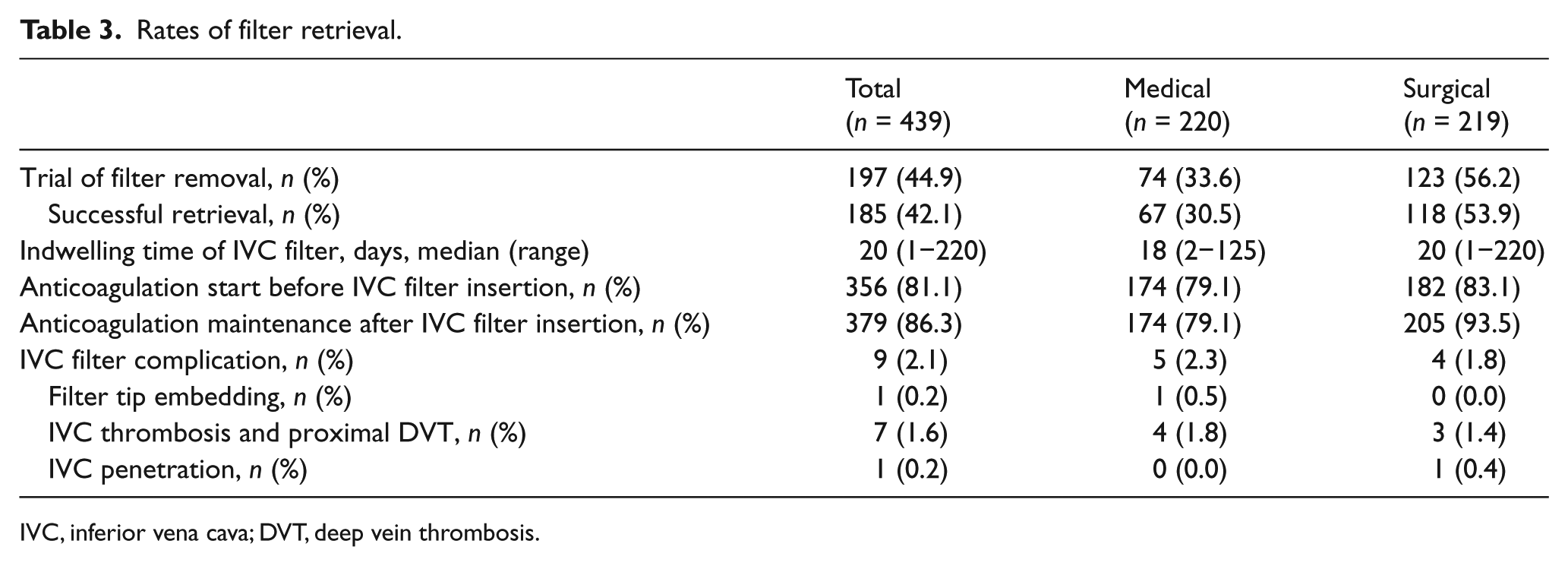
IVC, inferior vena cava; DVT, deep vein thrombosis.
The median time of filter indwelling was 20 days. There was no significant difference in the filter indwelling time between cases referred from the medical department and those from the surgical department (18 and 20 days, respectively; p=0.965; p-value not shown in the table).
Among 439 patients, 379 (86.3%) were able to receive therapeutic anticoagulation after IVC filter insertion. This means that 86.3% of patients were able to maintain anticoagulant therapy at discharge and should have been considered for the removal of the IVC filter.
Overall, nine cases (2.1%) were found to have complications from IVC filters. IVC penetration was found in one case; however, there was no evidence of bleeding. The most common complication was newly developed thrombosis, including IVC thrombus and proximal DVT.
Predictors of attempts at IVC filter retrieval
Some variables were chosen a priori for the analysis. Ten clinical variables were analyzed, including demographic factors, such as old age, female sex, and obesity, as well as risk factors for VTE, such as malignancy (Table 4). A history of cerebral hemorrhage, malignancy, and admittance to the surgical department were statistically significant variables in multivariate analysis (Table 5). Body mass index > 25 kg/m2, recent surgery, and recent fracture were statistically significant variables in univariate analysis; however, they were no longer significant in multivariate analysis.
Univariate analysis for predictors of IVC filter removal.
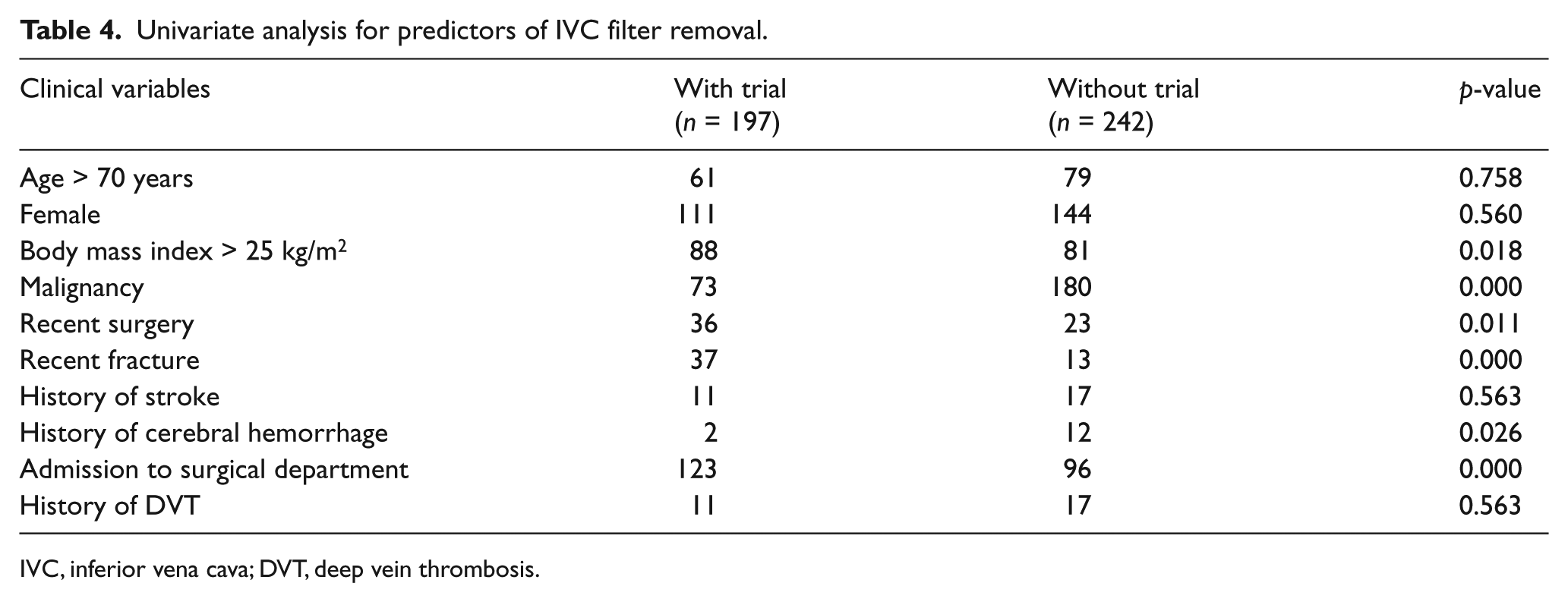
IVC, inferior vena cava; DVT, deep vein thrombosis.
Multivariate analysis for predictors of IVC filter removal.
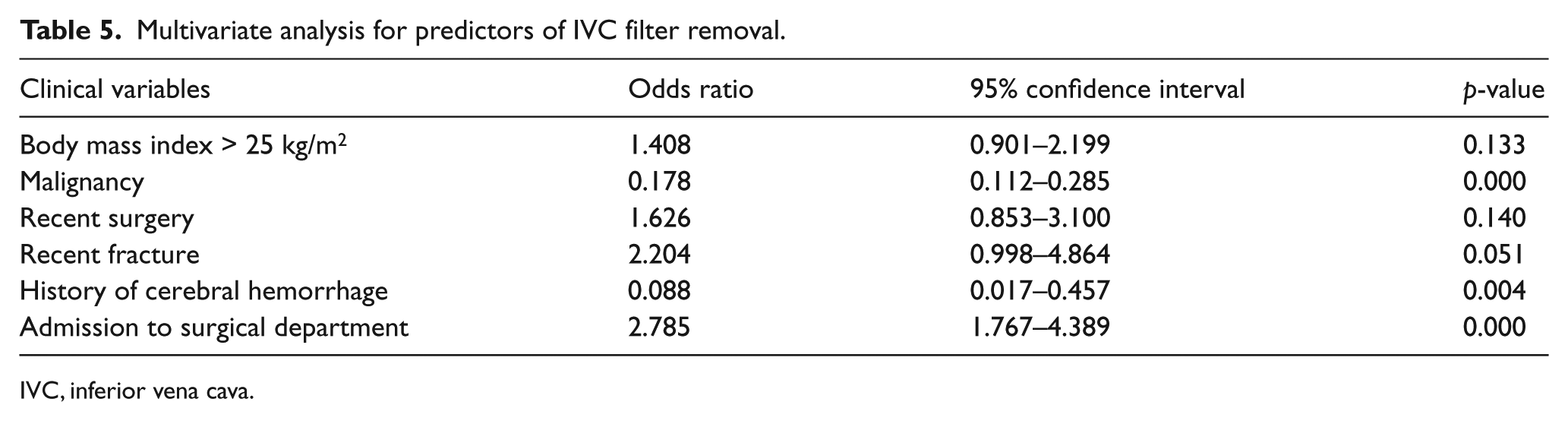
IVC, inferior vena cava.
Discussion
This study is the first report from Asia to investigate the indications of IVC filter insertion, filter retrieval rate, and predictors of filter retrieval. We found that attempts at filter retrieval were made in 44.9% of the cases, a rate that is slightly higher than those previously reported elsewhere,7,14–16 but that remains lower than desirable. Many of the patients with retained filters seemed to be eligible for filter retrieval, as they were receiving anticoagulant therapy. Once retrieval was attempted, the success rate was > 90%. Three significant factors were associated with fewer retrieval attempts in multivariate analysis: a history of cerebral hemorrhage, malignancy, and admittance to the medical department.
The indications for filter insertion are somewhat controversial, creating confusion among physicians. In contrast to the American College of Chest Physicians (ACCP) guidelines, 17 which advocate the use of IVC filters only in patients with contraindications to anticoagulant therapy, other societies accept broader indications. For example, the American Heart Association guidelines state that an IVC filter is used in patients with acute PE and very poor cardiopulmonary reserve, including those with massive PE. 18 The Society of Interventional Radiology provided more liberal indications, including free-floating iliofemoral or IVC thrombus, recurrent PE in spite of adequate therapy, and prophylactic indications. 19 This variability in indications for IVC filters among different societal guidelines causes confusion. For example, we encountered different opinions among vascular surgeons and pulmonologists at our institution about when to insert IVC filters. Moreover, the second most common indication found in this study was extensive iliofemoral DVT, which is not an indication according to the ACCP guidelines. The recently updated 2016 ACCP guidelines 20 strongly emphasize that an IVC filter should be inserted only in patients with contraindications to anticoagulation therapy. The discrepancy between the guidelines from various societies needs to be resolved.
A retrospective study in 2002 revealed no clinical benefit of IVC filters in patients with malignancy, in terms of overall survival rates. 21 However, in this study, physicians tended to retain the filters 5.6 times more frequently in patients with malignancy. Previous studies observed the same trend.9,12,22 This is because the patients are at a risk of developing VTE unless the underlying cancer is cured. The short life expectancy and overall poor condition of these patients also explain the low rate of retrieval attempts. However, it is striking that a significant proportion of these patients were discharged with anticoagulation therapy in our study (211 of 253 patients). Thus, active malignancy itself should not be the reason for filter retention.
If the patient had been admitted to the surgical department, the IVC filter was 2.8 times more likely to be retrieved. Among the patients admitted to the surgical department, 41.1% of IVC filters were inserted preoperatively. In contrast, only 20.9% of patients admitted to the medical department had preoperative indications. There may be a possibility that more filters were retrieved if they had been inserted preoperatively, explaining the higher retrieval rate in the surgical department.
In this study, the success rate of filter retrieval was high (93.9%) despite the low rate of retrieval attempts. The longest indwelling time of the filters that were successfully retrieved was 220 days. It is recommended that filters should be removed as soon as anticoagulation is initiated because longer indwelling times are associated with retrieval failure. The success rate of filter retrieval was 99% at 1 month after placement; however, the rate was as low as 37% at 12 months, according to a pooled analysis in a systematic review. 5 However, with advances in retrieval techniques, IVC filters can now be retrieved more often, as shown in recent studies.23,24 Given the overall high retrieval success rate and recent advances in technology, more effort should be made to retrieve filters whenever they are no longer needed.
Although, in this study, we did not evaluate the impact of follow-up care after discharge on the retrieval rate, previous studies have pointed out the importance of a retrieval plan and a dedicated filter clinic. One study suggested that ambiguities about which service was responsible for the decision on filter removal might have contributed to the high rate of filter retention. 12 Another study found that patients with discharge summaries of filter management instructions had significantly higher filter retrieval rates. 8 Thus, physicians who deal with VTE (e.g. pulmonologists, vascular surgeons, oncologists, and interventional radiologists) should pay more attention to having an IVC filter retrieval plan. Furthermore, a recent study showed that IVC filter retrieval rates improved threefold with a multidisciplinary approach, including patient education and a visit to a thrombosis specialist. 25 In this regard, the establishment of an interdepartmental follow-up protocol may decrease the avoidable complications resulting from unnecessary filter retention.
Limitations
This study has several limitations. First, owing to the retrospective nature of the study, biases may be present. Second, our institution deals with a high volume of patients with cancer. In other institutions with different compositions of patients, the result may not be the same. Third, the complication rate of IVC filters seems lower than that reported in previous studies, 26 and it may have been underestimated because not all patients underwent follow-up imaging evaluations. Fourth, all the filters were inserted by radiologists in our institution, according to the decision of each attending physician; this practice pattern may differ from those in hospitals where other specialists, such as those in the departments of cardiology and vascular surgery, not only make the decision to place IVC filters, but also perform the filter insertion.
Conclusion
We analyzed the common indications for IVC filter insertion, the filter retrieval rates, and factors influencing the rate of retrieval attempts in this study. History of cerebral hemorrhage, malignancy, and admission to a nonsurgical department were the significant predictive factors of a lower retrieval attempt rate in multivariate analysis. With the increased use of IVC filters, more considerations should be addressed before placing a filter, and physicians should attempt to avoid unnecessary IVC filter placement and improve the retrieval rate.
Footnotes
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: this study was supported by University of Ulsan College of Medicine.