
Abstract
Published reports indicate low retrieval rates for retrievable inferior vena cava (IVC) filters. We performed a historic-controlled study of a 5-year intervention (March 2007 to February 2012) to improve IVC filter retrieval rates at a university medical center serving a rural area. All adults with a retrievable filter placed were included, except those with a life expectancy <6 months. The intervention included initial verbal counseling and printed educational materials, correspondence after discharge, and a hematology consultation. The control group included patients with retrievable filters placed in the 15 months preceding study initiation. In the control group, 116 filters were placed and 27 (23%) were removed, compared to 378 filters placed and 169 (45%) removed during the intervention. Adjusting for patient characteristics, the odds ratio of retrieval during the intervention was 3.03 (95% CI 1.85–4.27) compared to the control period. An intervention including patient education and hematology follow-up appeared to significantly improve IVC filter retrieval rates.
Keywords
Introduction
Inferior vena cava (IVC) filters are placed for a variety of indications, though the presence of pulmonary embolism (PE) or acute proximal lower extremity deep vein thrombosis (DVT) and absolute contraindication to anticoagulation is the only evidence-based and widely recognized indication for placement.1,2 Other settings where filters are placed in practice include recurrent PE despite therapeutic anticoagulation, acute proximal DVT with poor cardiopulmonary reserve, and prophylaxis for DVT in trauma patients and prior to bariatric surgery.3–6 The liberalization of IVC filter placement, ease of placement, and advent of retrievable filters has led to a sharp increase in filter use in recent years.7–9 In addition, there is wide variability in practice patterns among institutions and specialties, and disparate guidelines for filter use published by professional societies.2–6,10–13 Post-insertion complications are common and include recurrent venous thromboembolism (VTE), filter migration, filter fracture, IVC perforation, and infection.14–18
In August 2010, the Food and Drug Administration (FDA) reported 921 adverse event reports for IVC filters in the preceding 5 years (including 328 device migration, 146 embolization, 70 IVC perforation, 56 filter fracture). Based on this, the FDA recommended that the implanting physicians and clinicians responsible for the care of these patients consider removing the filter as soon as mechanical protection from PE is no longer needed. 19
Despite FDA recommendations and known complications of ongoing filter use, retrieval attempt rates as low as 10–33% have been reported.20–23 In response to the rising use of IVC filters, low retrieval rates, and FDA recommendations, we implemented a multidisciplinary quality improvement intervention to increase the IVC filter retrieval rate at our institution.
Methods
The study setting was the University of Vermont Medical Center, a 562-bed tertiary care teaching hospital with a level-1 trauma designation covering a population of 1 million persons residing in rural areas of Vermont and northern New York. The study was a historic-controlled study of the impact of an intervention program to increase IVC filter retrieval rates. All patients received retrievable IVC filters. The intervention took place from March 2007 to February 2012. The historical control group included patients with retrievable filters placed in the 15 months preceding the intervention, when there was no protocol in place for consideration of retrieval. During both periods, all IVC filters were placed by interventional radiology or trauma physicians. For both services, a database was used to record identifiers of all patients with filters placed. The historical control group included patients with retrievable IVC filters placed in the 15 months preceding the intervention, when there was no protocol in place for post-placement consideration of retrieval. Patients with a life expectancy <6 months, in a hospice, and <18 years of age at the time of filter placement were excluded from the control and intervention groups, as were patients who later transitioned to a hospice or died within 3 months of filter placement. We excluded those with a short life expectancy since it would not seem likely filter retrieval would be beneficial. The institutional review board of the University of Vermont approved the study.
A multidisciplinary team of interventional radiologists, trauma surgeons, hematologists, nurse practitioners, nurses, and clinic administrators planned and executed the intervention, which had four components: (1) early patient education regarding the importance of evaluation for filter retrieval; (2) referral by interventional radiology or trauma surgery to the Thrombosis and Hemostasis Program in the hematology clinic; (3) standard evaluation for decision making regarding the appropriateness and timing of filter retrieval; and (4) filter retrieval by interventional radiology when recommended.
During the intervention period, prior to placement of an IVC filter (or after if placed emergently), the implanting physician and nursing staff provided each patient with written information on IVC filters, education on the importance of evaluation to consider retrieval, and instruction that they would be contacted by phone to schedule an appointment for evaluation in the hematology clinic within 3 months. The clinic telephone number was given in case they had questions, or to call if they were not contacted. The document was prepared at a 5th grade reading level and was reinforced verbally when given to the patient. A referral to the hematology clinic was generated through the electronic health record immediately following IVC filter placement by the implanting team. The hematology scheduler tracked the patient until discharge, and then mailed an informational letter to the patient again detailing the reason for a visit. Telephone contact was used to schedule an appointment within 3 months. If the patient refused the visit or had questions, a thrombosis specialist nurse attempted to speak with the patient, and if still unsuccessful, an informational letter was sent to the primary care provider.
At the hematology appointment, a thrombosis specialist nurse practitioner (or occasionally a physician) in the Thrombosis and Hemostasis Program evaluated the patient. The evaluation included review of the indication for IVC filter placement, past thrombosis history, clinical course since placement, current clinical status, anticoagulation use, bleeding history, risk stratification for venous thrombosis recurrence, physical exam, and patient education regarding the risks and benefits of filter retrieval or retention. A decision was made to schedule filter retrieval by interventional radiology, leave the filter in place permanently, or defer the retrieval decision, in which case follow-up was arranged.
Data spreadsheets were prospectively maintained including indication for filter placement, the service placing the filter, hematology clinic recommendations, and date and outcome of filter retrieval attempts. A physician independently verified all data through medical chart review and collected additional information on medical history for calculation of the Charlson Comorbidity Index. 24 Travel distance from the patient’s home address to the University of Vermont Medical Center was estimated as the shortest driving distance using Google’s mapping function. Retrospective data on the above variables were collected by physician chart review in the historic control group.
Three primary outcomes were: (1) the proportion of patients who were evaluated in the hematology clinic; (2) the proportion who had filter retrieval attempted; and (3) the proportion who had successful filter retrieval. Secondary outcomes were the technical success rate of filter retrieval and mean filter dwell time.
Statistical analysis
Statistical analysis was done with SPSS version 22 (IBM Corp., Armonk, NY, USA). Patient characteristics were tabulated by control group or intervention group status. Including both the control and intervention group, univariable logistic regression was used to calculate unadjusted odds ratios (ORs) with 95% confidence intervals (CIs) for each primary outcome based on the potential confounding variables of age, service placing the filter, indication for filter placement, Charlson Comorbidity Index score, and travel distance to the University of Vermont Medical Center. Age, sex and covariates that were associated with each primary outcome (p<0.05) were included in a multivariable model to calculate an adjusted OR with 95% CI for that primary outcome in the intervention versus control group.
Results
During the 15-month control period, 116 IVC filters were placed while 378 were placed during the 5-year intervention period. There were 27 of 116 (23%) filters retrieved in the control group and 169 of 378 filters (45%) retrieved during the intervention period. During the intervention period, as shown in Figure 1, 196 (52%) patients attended a hematology clinic visit. Among these, retrieval was recommended at the first visit in 102 (52%) patients and 83 (81%) of these had their filter removed. Retrieval decision was deferred in 65 (33%) patients, of whom 28 (43%) eventually had a successful retrieval. The filter was recommended to remain in place for 29 (15%) patients, and four of these eventually had their filter removed. Overall, of the 196 patients seen in the hematology clinic, 115 (59%) had their filter retrieved, while 54 (30%) of the 182 patients not seen in the hematology clinic had their filter retrieved.
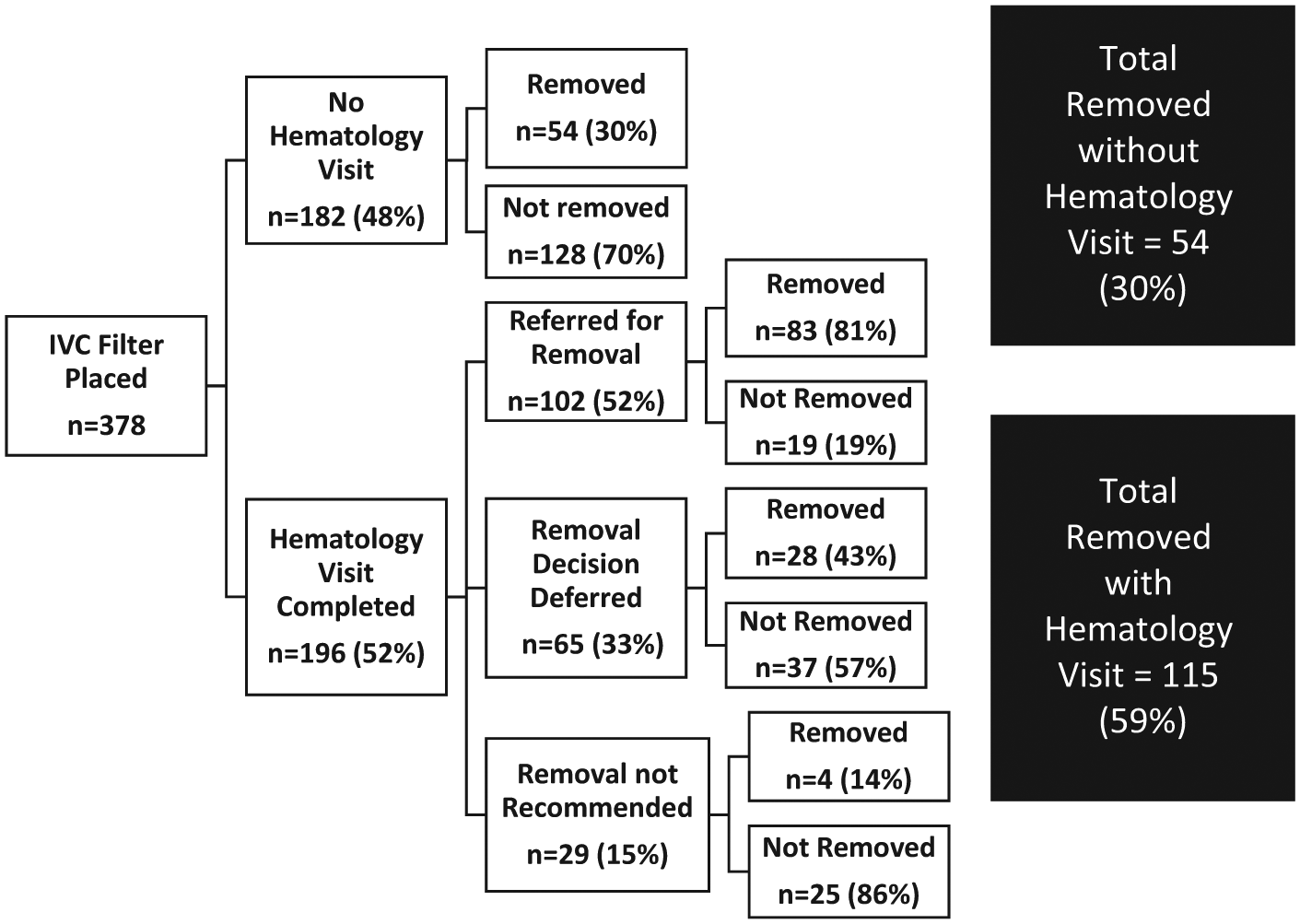
Flow chart of results of the intervention (IVC, inferior vena cava).
During the intervention period, placement of IVC filters declined with time principally due to a sharp decline in filters placed for prophylaxis among trauma patients (data not shown). Irrespective of this increasing complexity of decision making required for retrieval, the retrieval rate continuously improved across the 5 years of the intervention, with retrieval rates in each successive year of 43 of 106 (40%), 26 of 77 (34%), 44 of 89 (49%), 30 of 61 (49%), and 26 of 45 (58%), respectively (p for trend <0.001).
Table 1 shows the characteristics of control and intervention patients at the time of filter placement. On average, patients were in the sixth decade of age, and more than half were male. Characteristics were similar in the two groups, though patients in the intervention group were less likely to have the filter placed for prophylactic indications than treatment of VTE (34% vs 46%), less likely to have the filter placed by a trauma surgeon (15% vs 63%), and lived closer to the hospital.
Patient characteristics.
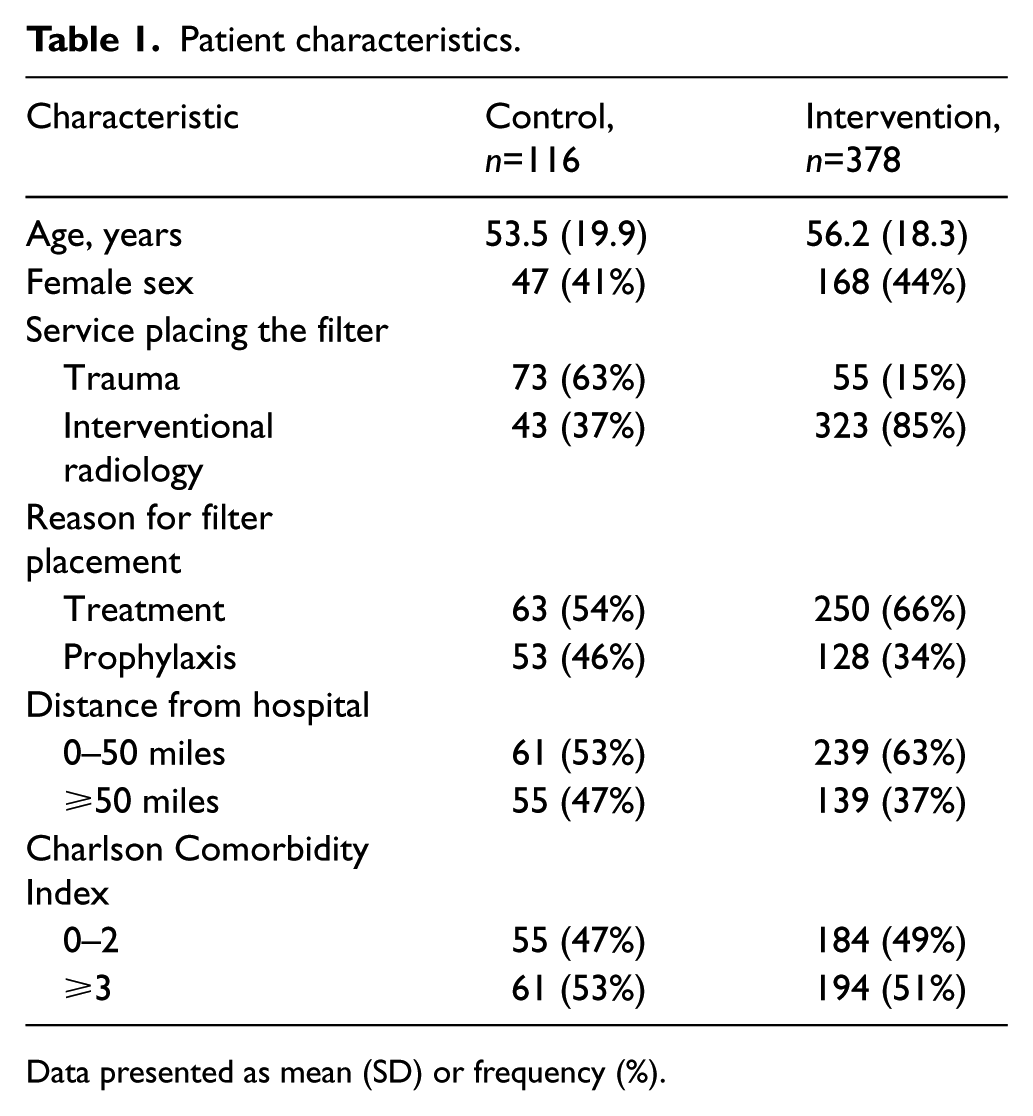
Data presented as mean (SD) or frequency (%).
Associations of patient characteristics with the primary outcomes in the control plus intervention groups are shown in Table 2. Eight percent of patients in the control group attended a hematology visit whereas 52% in the intervention group did. Factors associated with attending a hematology visit included placement of the filter by interventional radiology, placement for treatment of VTE rather than prophylaxis, travel distance <50 miles, and increasing time since the intervention began. Age, sex, and comorbidities were not associated with attending a hematology visit. Since nearly all retrieval attempts were successful, patterns of association between the filter retrieval attempt and success were similar. As shown in Table 2, a low Charlson Comorbidity Index score had the strongest association with having a retrieval attempted and a successful retrieval. Other factors associated with both outcomes included younger age, travel distance <50 miles, and later study year. Sex, the service placing the filter, and indication for filter placement were not associated with either attempting a retrieval or successful retrieval.
Factors associated with primary outcomes in univariable analysis in control plus intervention groups.
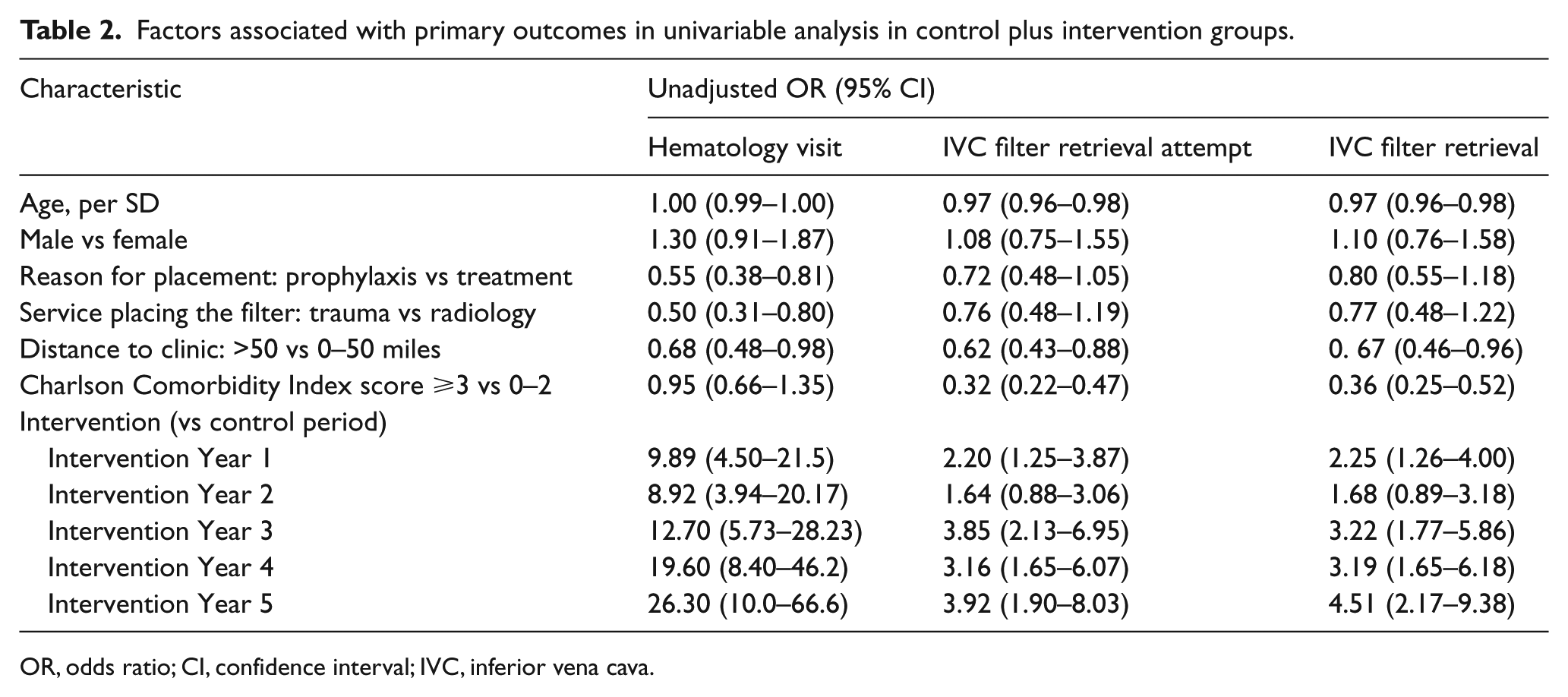
OR, odds ratio; CI, confidence interval; IVC, inferior vena cava.
As shown in Table 3, after adjusting for potential confounding variables, attending a hematology clinic visit was nearly 13-fold more likely during the intervention than control period. An IVC filter retrieval attempt was threefold more likely during the intervention, as was successful filter retrieval. The technical success rate of filter retrieval was high (92%) and did not differ between groups. Median filter dwell time in the intervention group was 203 (interquartile range 132–276) days.
Multivariable-adjusted association of intervention with primary outcomes.
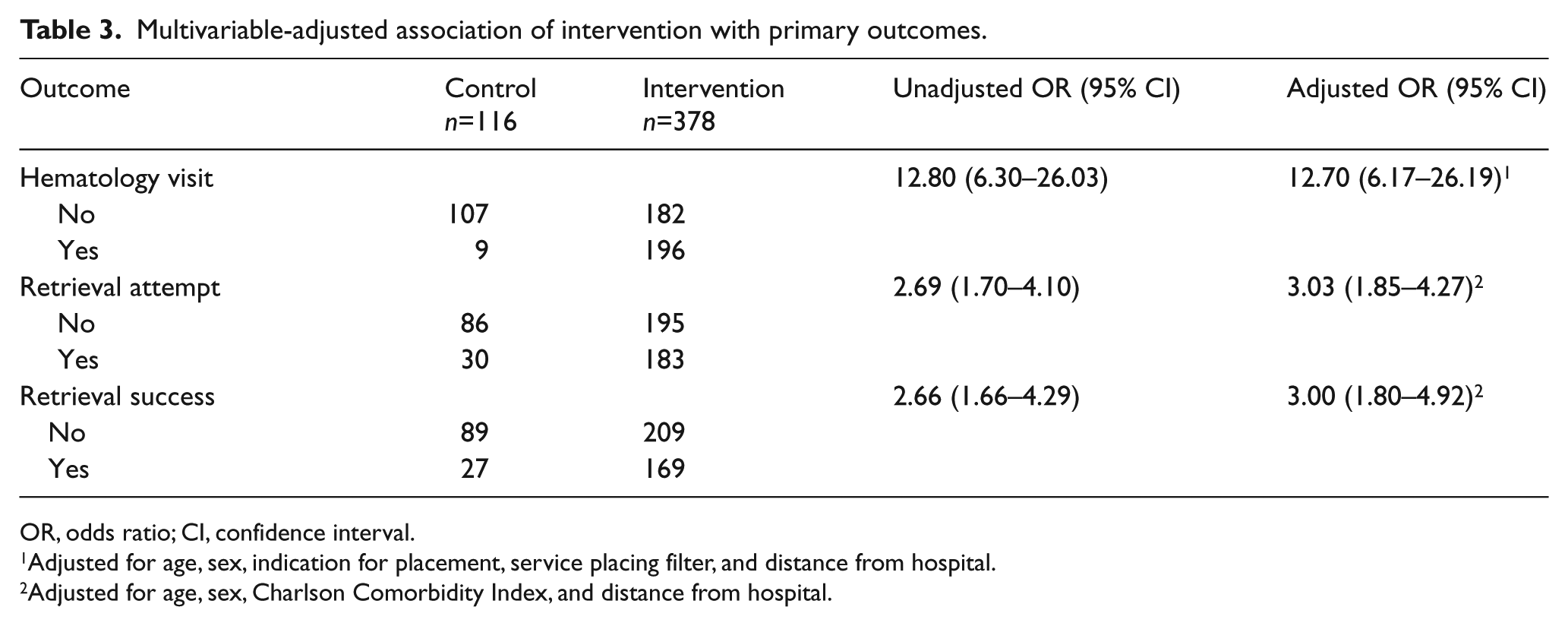
OR, odds ratio; CI, confidence interval.
Adjusted for age, sex, indication for placement, service placing filter, and distance from hospital.
Adjusted for age, sex, Charlson Comorbidity Index, and distance from hospital.
Discussion
This study demonstrated that IVC filter retrieval rates improved by threefold after implementing a multidisciplinary coordinated approach to post-procedure care that included patient education, post-discharge patient communication, and a visit to a thrombosis specialist to assess the ongoing need for the filter and to coordinate retrieval. The low retrieval rate (23%) prior to implementation of the intervention was similar to experience reported at other institutions.20–23 We hypothesized that barriers to filter removal in routine care might include a lack of patient understanding of the need for device retrieval, lack of consistent clinical follow-up, and lack of a coordinated approach to scheduling retrieval. By addressing these barriers using a quality improvement intervention, our institution tripled the IVC filter retrieval rate during the 5 years of the study.
We are aware of three other reports of institutions addressing the problem of low retrieval rates of IVC filters using systems-based approaches to improve patient follow-up. These institutions achieved retrieval rates of 58–75%.25–27 Two studies compared data from a post-intervention period to a pre-intervention control period, and all three studies used databases to track patients along with various methods of communication, including mail and telephone contact.25,26 Three approaches were used in these studies to determine a recommendation for filter removal: (1) physician review of electronic medical record data; 25 (2) a clinic visit with the interventional radiologist after communicating with the referring physician; 26 and (3) telephone evaluation by a case manager for ongoing VTE risk 60 days after discharge, with subsequent evaluation by a radiologist and retrieval in low- risk patients. 27 There are strengths and weaknesses of these approaches. Our approach may have advantages over these approaches since the appropriateness of filter retrieval may change over time in a patient, and not all data required to make a decision regarding retrieval may be accessible through review of the medical record or decision making at the time of discharge after filter placement. Our approach involved a thrombosis specialist integrating clinical information from the medical history and the status of the patient at the time of consideration of filter retrieval. Over and above the filter retrieval decision, the thrombosis specialist could also address topics related to patient care for thrombosis.
Factors independently associated with lower filter retrieval rate in this study included older age, advanced comorbidity, and residence more than 50 miles from the hospital. Lower retrieval rates in patients with advanced age and higher comorbidity may be due to decisions to leave the filter in place based on poor prognosis or patient preference, but data were not available to allow determination of this. Concerning patients living far from the hospital, future efforts to improve IVC filter retrieval rates might include more involvement by their primary care providers in decision making, provision of transportation to appointments, formal telephone or telemedicine consultation, or coordination with interventional radiologists at hospitals closer to the patients’ residence (although in rural areas these services are not usually available).
Our retrieval success rate during the intervention was 92%, which may seem low. We believe this is likely explained by the definition of retrieval success employed. Each procedure encounter after referral for IVC filter removal was considered an attempt, even if the procedure was terminated due to thrombus in the filter seen on a pre-procedure inferior venacavogram (which was routinely done).
Strengths and limitations
The strengths of our study included the prospective collection of patient data from a large number of patients with retrievable filters in place and the consistency of application of care in a specialty thrombosis clinic over time. We also studied a rural population. Limitations should also be considered. The study was conducted in a single institution and results may not be generalizable to health care systems with different patient characteristics, physician and administrative resources, practice patterns, or technical experience. Use of a historic control group may be problematic as some data were collected retrospectively from chart review, and patient characteristics and practice patterns related to filter placement changed over time. However, the historic control group was prospectively ascertained with a database so patients were fully captured, and multivariable modeling was used to account for factors that differed in the two periods. Moreover, a randomized trial of a retrieval coordination intervention compared to standard care would not be possible for ethical reasons given the likely benefits of filter retrieval, and would be impractical due to the inability to blind patients and providers. Retrieval rates may have been underestimated as patients lost to follow-up may have had filters retrieved at outside institutions, particularly if they lived in a distant community with available capability. Clinically relevant outcomes such as IVC filter complications, recurrent VTE, and post-thrombotic syndrome were not ascertained.
Conclusion
A multidisciplinary team-based intervention including patient education, outpatient follow-up with a thrombosis specialist to assess the ongoing need for the IVC filter, and initiation of the filter removal protocol at the time of IVC filter placement significantly improved IVC filter retrieval rates in a rural population. To comply with FDA recommendations to provide high-quality care in this patient population, these findings support wide implementation of similar protocols.
Footnotes
Acknowledgements
The authors acknowledge the key roles of Lisa Smith RN, Emily Parenteau APRN, Karen Libby RN and Richard Watts PhD for their contributions to the project.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: this work was supported by the Department of Radiology, University of Vermont Medical Center.