
Abstract
Background:
National survey data exploring the patient experience with lipedema are lacking.
Methods:
We conducted national surveys from 2016 to 2022 of women with lipedema as well as female controls. Surveys collected information on symptomatology, pain, and therapies. We performed logistic regression comparing symptoms among those with lipedema versus controls adjusting for age and BMI.
Results:
A total of 707 women with lipedema and 216 controls completed the surveys. Those with lipedema had a mean age of 48.6 years and mean BMI of 40.9 kg/m2. Lipedema symptom onset occurred frequently at puberty (48.0%) or pregnancy (41.2%). Compared to controls, women with lipedema were more likely to report leg swelling in heat (odds ratio [OR], 66.82; 95% CI, 33.04–135.12; p < 0.0001), easy bruising (OR, 26.23; 95% CI, 15.58–44.17; p < 0.0001), altered gait (OR, 15.54; 95% CI, 7.58–31.96; p < 0.0001), flu-like symptoms (OR, 12.99; 95% CI, 4.27–39.49; p < 0.0001), joint hypermobility (OR, 12.88; 95% CI, 6.68–24.81; p < 0.0001), cool skin (OR, 12.21; 95% CI, 5.20–28.69; p < 0.0001), varicose veins (OR, 11.29; 95% CI, 6.71–18.99; p < 0.0001), and fatigue (OR, 9.59; 95% CI, 6.10–15.09; p < 0.0001). Additionally, 70.3% had upper arm involvement, 21.2% reported foot swelling, and 16.6% reported foot pain. Most (52.2%) reported no symptom improvement with diet or exercise. Common therapies used included compression therapy (45.0%), gastric bypass (15.7%), and lower-extremity liposuction (14.0%).
Conclusion:
In a large, national, symptom survey, women with lipedema reported excess pain, swelling, and fat in the legs along with numerous symptoms beyond those classically described. Symptom responses to common therapies remain understudied.
See Commentary: Carroll B. Lymphedema and lipedema: More than a swollen limb? Vasc Med 2024; 29:48–49.
Background
Lipedema is characterized by the disproportionate accumulation of nodular, fibrotic adipose tissue primarily in the lower limbs with sparing of the upper torso, hands, and feet.1,2 Lipedema almost exclusively affects women, and these limb changes are reported to often begin during puberty, pregnancy, menopause, or following surgery. Because it is often confused with obesity or lymphedema, lipedema is chronically misdiagnosed and undertreated. 3 Symptoms frequently reported in lipedema include pain with light touch or pressure, 4 easy bruising, 5 and joint hypermobility. 6 These symptoms may impact physical function and quality of life.7–9 Prior surveys regarding symptom onset, symptom description, and therapies utilized by patients with lipedema are limited by small sample size,10,11 narrow focus of survey questions,10,11 and lack of peer review of survey findings. 12
Characterizing the symptomatology of those living with lipedema in a large population may improve the understanding of this disorder, provide targets for therapeutic trials, and assist in the development of patient-centered treatment plans. Thus, a comprehensive survey in a large population that collects patients’ reported symptomatology and treatment experience with lipedema remains a critical unmet need.
To address this, we collected detailed survey data on symptom description and distribution as well as common treatments among the largest cohort of patients with lipedema in the United States reported to date. Additionally, we compared symptomatology to a control cohort without lipedema.
Methods
Patient identification and recruitment
All participants provided written informed consent. This study was conducted according to the World Medical Association Declaration of Helsinki and was approved by the Vanderbilt University Medical Center (VUMC) institutional review board (IRB). We recruited patients with lipedema using IRB-approved research advertisements on social media, in-person recruitment at a Fat Disorders Resource Society annual conference, ResearchMatch.org, VUMC research e-mail advertisements, and through VUMC clinics. We recruited control participants without lipedema within a decade of life through ResearchMatch.org, VUMC research e-mail advertisements, social media outreach, and outreach through both the Fat Disorders Resource Society and the Lipedema Foundation.
Survey instrument
We collected data between 2016 and 2022 using four survey instruments from 2016 to 2022 (Table 1). We distributed all surveys as electronic instruments in Research Electronic Data Capture (REDCap)13,14 either remotely or in person. Participants had access to study personnel to address questions. To determine survey content, we used lipedema characterizations reported in the literature or shared during patient interactions at the Fat Disorders Resource Society Annual Conference in 2016. Survey questions used in the present analysis were identical across all four surveys. If a subject completed multiple surveys, only the first was used for this analysis. In addition to baseline demographic information, the surveys collected information on symptom onset timing, symptom type (online Supplemental Figure 1), sign and symptom distribution (online Supplemental Figure 2), and therapies used for lipedema (online Supplemental Figure 3). Controls without lipedema completed the same surveys except for lipedema-specific sections. We assessed leg pain using the visual analogue scale (VAS) presented as a user-controlled sliding bar from 0 to 100 (online Supplemental Figure 4). Survey data were collected and managed using REDCap electronic data capture tools hosted at VUMC.
Survey details for study respondents.

Statistical analysis
We included all respondents who provided complete information on age, weight, and height and who self-identified as women. We used descriptive statistics to summarize demographic and survey outcome by group. The lipedema group consisted of individuals with a reported diagnosis of lipedema (i.e., case), and the control group consisted of those without a reported diagnosis of lipedema (i.e., control). We reported means and SDs for continuous variables and frequency (counts) and percentages for categorical variables. To control for confounding variables, we used multivariable logistic regression adjusted for age and body mass index (BMI) to compare symptoms in cases versus controls and reported adjusted odds ratios (OR) and 95% CI. To explore the impact of varicose veins on these symptoms, we added a history of varicose veins to the above multivariable logistic regression models for additional analyses. In exploratory analyses, we compared symptoms among either cases with physician-diagnosed lipedema or cases with self-reported lipedema to controls using multivariable logistic regression adjusted for age and BMI. Similarly, we reported adjusted ORs and 95% CIs for these exploratory analyses. We analyzed BMI on a natural log scale to reduce variation. We used the penalization of the likelihood by Jeffreys’ prior to reduce biased estimation for solving the low number of events for some survey responses in binomial-response generalized linear models. To account for multiple testing, we adjusted p-values using the Benjamini–Hochberg method and considered a two-sided p-value less than 0.05 statistically significant. We did not impute missing data, and used SAS software, version 9.4 (SAS Institute Inc., Cary, NC, USA) and R 4.1.2 (R Foundation for Statistical Computing, Vienna, Austria) for all analyses.
Results
The sample included 707 women with a lipedema phenotype and 216 controls. The mean age of those with lipedema was 48.6 years with a mean BMI of 40.9 kg/m2 (Table 2). At the time of survey, 46.3% of respondents with lipedema reported receiving a diagnosis by a physician. An additional 6.6% were identified by a physical therapist. Worsening symptoms were most commonly reported at puberty (48.0%) or pregnancy (41.2%) followed by menopause (33.2%) and abdominal surgery (31.0%). Using the 0–100 VAS sliding scale for pain, the mean severity of leg pain typically experienced by women with lipedema was 53.9 (SD, 23.8) compared to 6.9 (SD, 12.7) by controls.
Baseline characteristics of survey respondents.
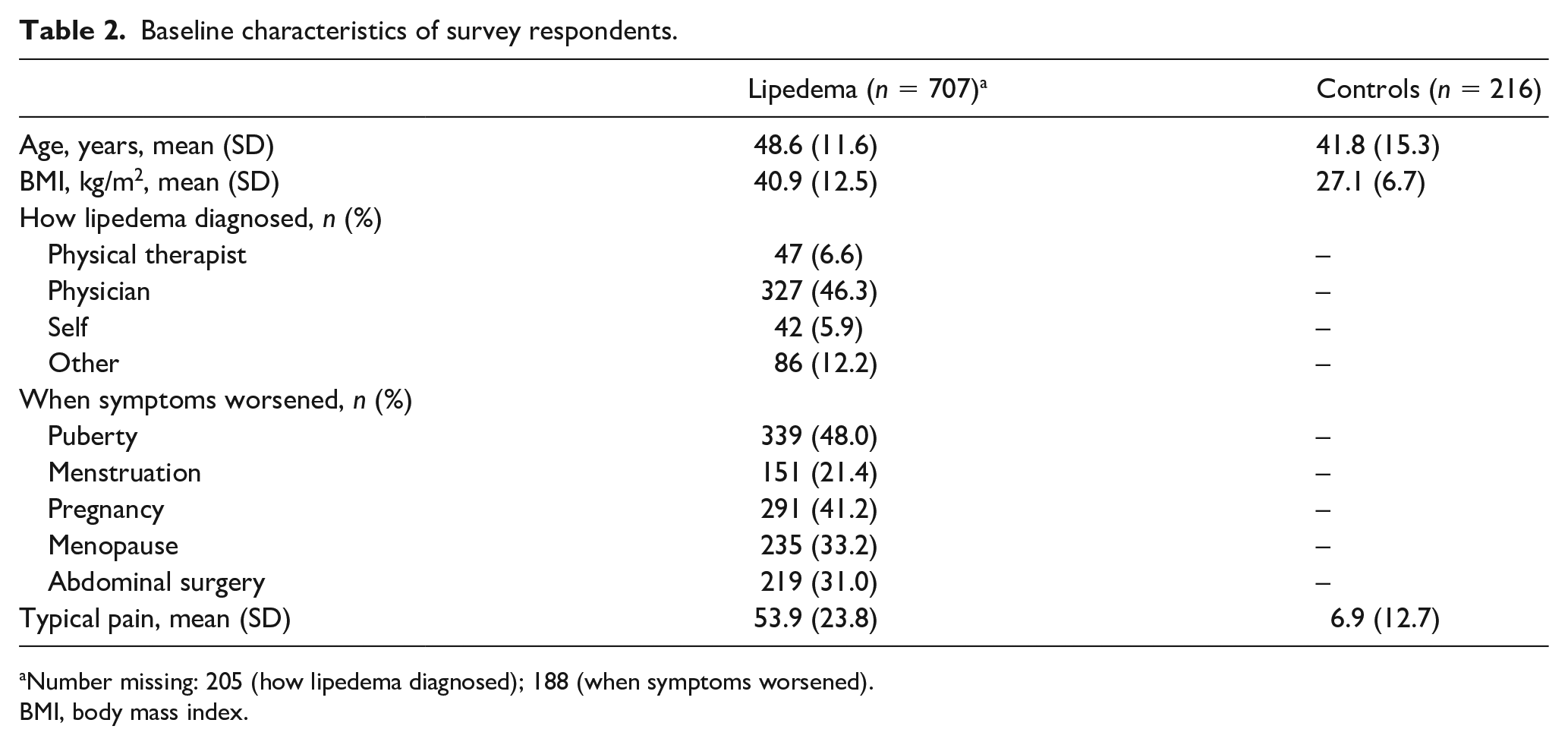
Number missing: 205 (how lipedema diagnosed); 188 (when symptoms worsened).
BMI, body mass index.
In logistic regression models adjusting for age and BMI, participants with lipedema were more likely to experience swelling in hot weather (OR, 66.82; 95% CI, 33.04–135.12; p < 0.0001), easy bruising (OR, 26.23; 95% CI, 15.58–44.17; p < 0.0001), and altered gait (OR, 15.54; 95% CI, 7.58–31.96; p < 0.0001) compared to controls (Figure 1). Other signs and symptoms more common in those with lipedema compared to controls were flu-like symptoms (OR, 12.99; 95% CI, 4.27–39.49; p < 0.0001), joint hypermobility (OR, 12.88; 95% CI, 6.68–24.81; p < 0.0001), skin that was cool to the touch (OR, 12.21; 95% CI, 5.20–28.69; p < 0.0001), varicose veins (OR, 11.29; 95% CI, 6.71–18.99; p < 0.0001), and fatigue (OR, 9.59; 95% CI, 6.10–15.09; p < 0.0001). Participants with lipedema were also more likely to report lipomas than controls (OR, 5.34; 95% CI, 2.84–10.04; p < 0.0001). Additionally adjusting for the presence of varicose veins only partially attenuated these associations (online Supplemental Table 1). In exploratory analyses, participants with either physician-diagnosed lipedema or self-reported lipedema were more likely than controls to experience all symptoms surveyed, although this did not reach statistical significance for hyperactive behavior or distractibility among those with self-reported lipedema (OR, 4.45; 95% CI, 0.85–23.37; p = 0.08) (online Supplemental Table 2).
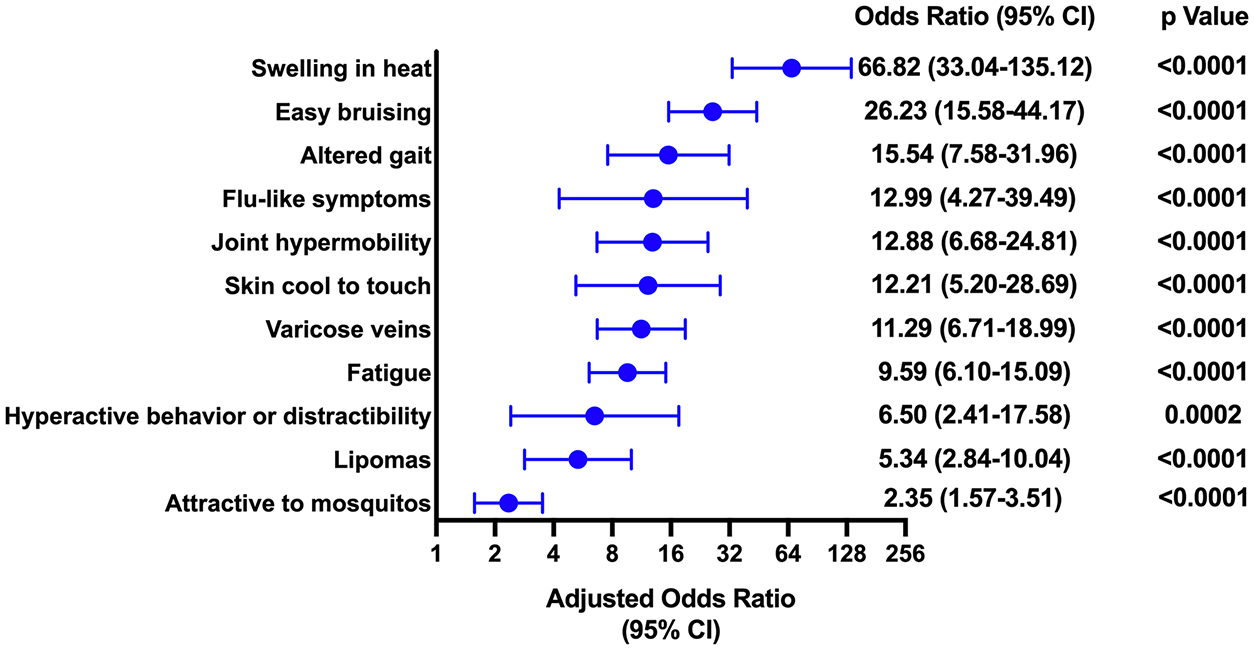
Symptoms surveyed in respondents with lipedema versus controls.
Regarding the distribution of symptoms, respondents with lipedema frequently reported excessive fat in the thighs (85.3%), followed by knees (76.1%), hips (75.5%), upper arms (70.3%), calves (66.3%), and forearms (30.1%), whereas the hands and feet were typically spared from fat (< 5%) (Figure 2A). Of the 213 women with excess forearm fat deposition, 202 (94.8%) also had excess upper arm fat deposition. Swelling in the calves was common (68.5%), followed by thigh and knee swelling in more than 50% of respondents (Figure 2B). Pain was similarly distributed, with the calves most commonly affected (62.0%), followed by thighs and knees (Figure 2C). Fewer women reported swelling (21.2%) or pain (16.6%) in their feet. Respondents with lipedema also reported an asymmetric appearance of the calves (23.8%), thighs (20.7%), knees (18.0%), and hips (13.3%) (online Supplemental Table 3). The distribution of symptoms was numerically similar in women with physician-diagnosed lipedema and those with self-reported lipedema (online Supplemental Table 4).
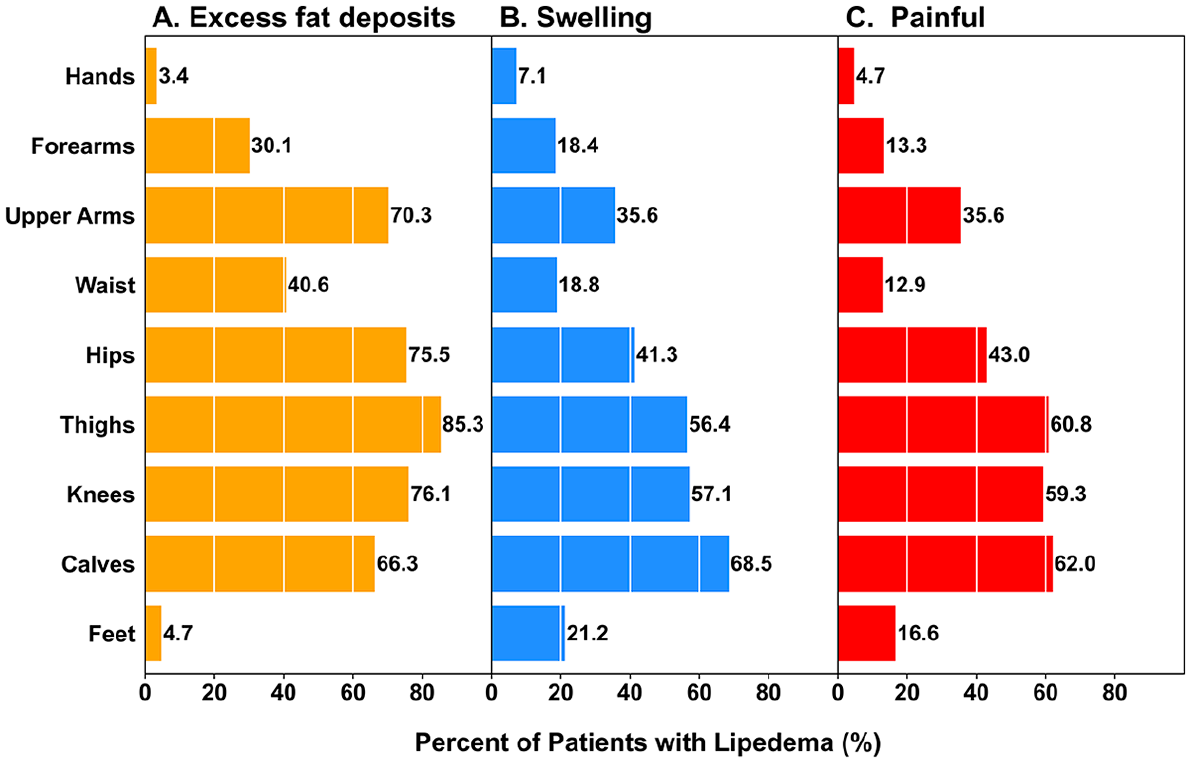
Distribution of signs and symptoms among respondents with lipedema.
Prior treatments for lipedema were commonly tried among surveyed participants (Table 3). More than 90% of participants had tried dieting or exercise, although 52% of these reported this therapy was not helpful in reducing symptoms. Fewer than half had used compression therapy (45%) or manual lymphatic drainage therapy (43%), and 59% trialed nutritional supplements. A small proportion of respondents had undergone surgical treatment, either with gastric bypass (15.7%) or liposuction (14.0%).
Lipedema treatments utilized by survey respondents.
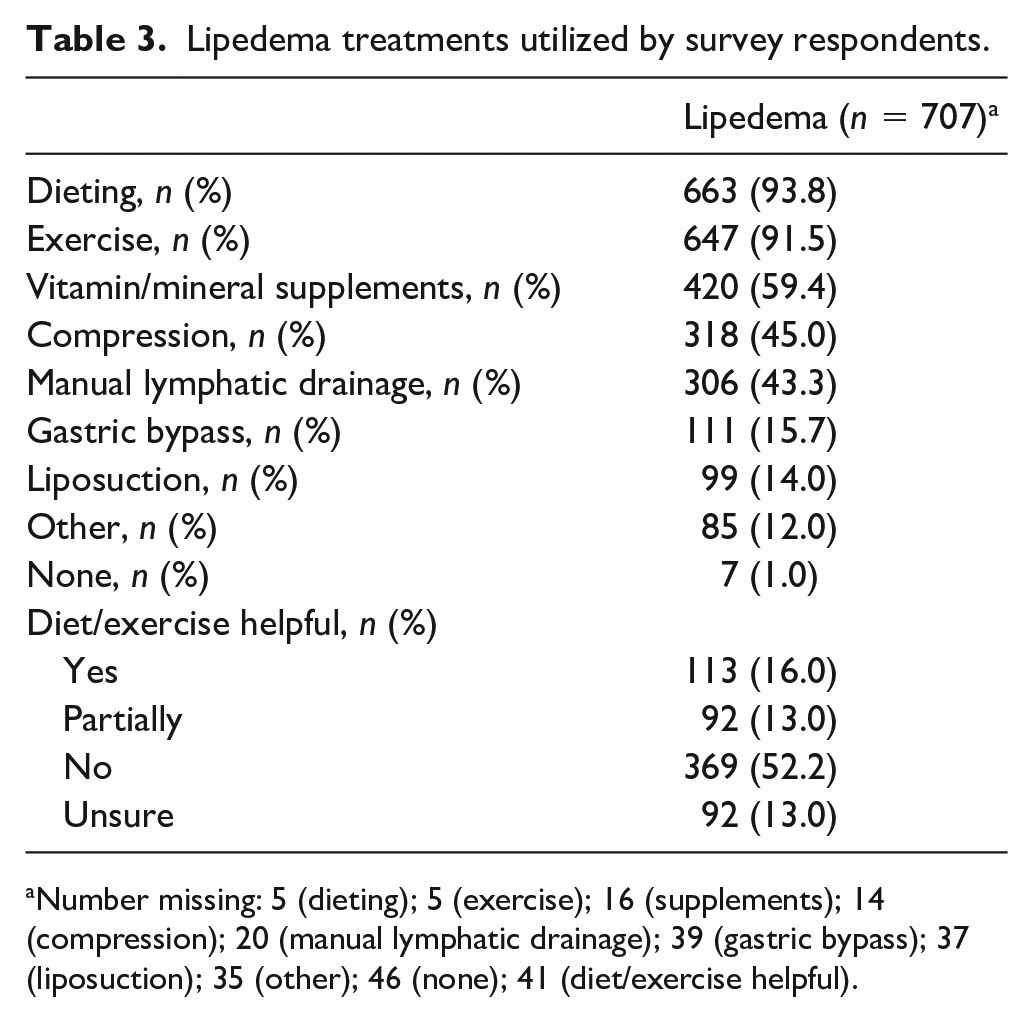
Number missing: 5 (dieting); 5 (exercise); 16 (supplements); 14 (compression); 20 (manual lymphatic drainage); 39 (gastric bypass); 37 (liposuction); 35 (other); 46 (none); 41 (diet/exercise helpful).
Discussion
In this national survey of more than 700 women with lipedema, participants reported experiencing a wide range of symptoms not accounted for by age or BMI. Beyond involvement of the hips, thighs, and calves, upper arm fatty deposits were common, and the feet were frequently affected by swelling and pain. Asymmetric signs and symptoms were also common. The experience of leg pain in those with lipedema was significantly greater than in control subjects. Fewer than half of respondents had tried compression or manual lymphatic drainage to address pain and swelling, and even fewer tried liposuction. To our knowledge, this is the largest survey of women with lipedema to date that includes comparisons to control subjects and assesses symptoms across a nonsurgical and surgical cohort of women.
Beyond classically reported symptoms of easy bruising and presence of subcutaneous nodules, both the present study and a prior online survey by the Lipedema Foundation 12 make clear the presence of systemic symptoms, including fatigue, pain, diffuse swelling, altered gate, joint hypermobility, pain, and fatigue. Edema, in particular, has emerged as a controversial topic in the field. For example, the recent International Consensus Document reports that edema is not a feature of lipedema. 15 The present data, in which patients frequently reported dynamic changes in swelling in response to heat as well as involvement of the feet, suggest that further study of edema in women with lipedema is needed. Prior data demonstrated greater capillary density within lipedema tissue, 16 as well as increased endothelial permeability, 17 which may in part relate to symptoms of edema. Notably, after adjusting for the high prevalence of varicose veins in our cohort, swelling remained the most likely symptom of those with lipedema, suggesting other contributors to their edema beyond chronic venous insufficiency. Finally, a growing body of literature demonstrates direct visualization of edema in the limbs of women with lipedema,18,19 as well as improved imaging parameters related to disease burden following manual lymphatic drainage, 20 suggesting this paradigm should be revisited.
The survey findings also call into question the notion that lipedema is primarily a disease of the lower legs that spares the feet. We found that 70% of respondents had upper arm excess fat deposits, and 30% had forearm involvement that nearly always occurred along with upper arm involvement (i.e., full arm excess fat deposition). These findings are consistent with a prior survey that reported arm involvement in 52% of respondents in 148 women undergoing surgery for lipedema. 11 Both a recent UK survey as well as the Lipedema Foundation survey reported upper-extremity involvement (70% and 71%, respectively).10,12 Symptoms of fat deposition may be less pronounced in the arms than legs or may develop later in the disease process, but it should be noted that pain in both the upper arms and the forearms was common among our survey respondents. Similarly, although few women reported excess fat in their feet, we found that pain and edema were common in the feet. Here, too, these survey data challenge the classic understanding of lipedema and emphasize the need for reliable, quantifiable diagnostic tests reflecting this distribution of symptoms in lipedema. These data also suggest a need to further investigate the influences lipedema has on the veno-lymphatic and neurological systems.
Most of our survey respondents had tried conservative therapy, primarily diet and exercise, and found these therapies ineffective at improving their symptoms. However, we did not capture data on whether respondents were successful at losing weight, and it is possible more effective nonsurgical or surgical interventions may be effective options for some patients.21,22 The efficacy of weight loss on improving lipedema symptoms should be researched further. Numerous studies have shown that liposuction is an effective therapy to reduce symptoms and improve functional status in women with liped-ema.1,11,23–27 Despite the significant symptomatic burden of our respondents, very few had undergone liposuction. Cost and inconsistent insurance coverage for these procedures persist. These data highlight the ongoing treatment gap for patients with lipedema.
Study limitations
There are several limitations to our analysis. Questionnaires did not fully capture patient demographics, such as race, geographic location, or medical comorbidities, which could be important factors to understand in future questionnaires. Although most respondents had been formally diagnosed with lipedema by a clinician, central adjudication of the diagnosis was not possible. As a result, it is possible some respondents had obesity or other disorders without lipedema. Additionally, we did not capture data on other conservative therapies, including soft tissue mobilization techniques beyond manual lymphatic drainage. It is possible other important symptoms of lipedema may also be present but were not captured by this set of questionnaires. Because respondents were recruited based on the presence of lipedema, our results may have been impacted by selection bias, and the experiences of individuals with less severe symptoms may be underrepresented in our data. Future studies should emphasize the inclusion of patients with a wide range of symptom severity and disability. The control population had a lower mean BMI than those with lipedema, and it is possible a control population with a more similar BMI would have yielded additional insights. Finally, survey responses may have been influenced by recall bias.
Conclusion
Among a large, national cohort of patients with lipedema, nearly half of whom were formally diagnosed by a physician, women with lipedema experience a wide range of symptoms. Furthermore, signs and symptoms frequently affect areas outside the lower body, suggesting that the classical description of lipedema may be incomplete, at least among patients with more severe symptoms and disability. Despite numerous advances in lipedema awareness in recent years, 28 survey data presented here also highlight an ongoing treatment gap for this patient population. Without further efforts to deeply phenotype patients, fully characterize the patient experience, and ultimately develop reliable diagnostic criteria for lipedema, these treatment gaps will likely persist. National research efforts, such as those presented here, are intended to help guide further collaborations between patients, clinicians, researchers, and funding partners.
Supplemental Material
sj-pdf-1-vmj-10.1177_1358863X231202769 – Supplemental material for National survey of patient symptoms and therapies among 707 women with a lipedema phenotype in the United States
Supplemental material, sj-pdf-1-vmj-10.1177_1358863X231202769 for National survey of patient symptoms and therapies among 707 women with a lipedema phenotype in the United States by Aaron W Aday, Paula MC Donahue, Maria Garza, Vanessa N Crain, Niral J Patel, John A Beasley, Karen L Herbst, Joshua A Beckman, Shannon L Taylor, Michael Pridmore, Sheau-Chiann Chen, Manus J Donahue and Rachelle Crescenzi in Vascular Medicine
Footnotes
Acknowledgements
The authors would also like to recognize the Fat Disorders Resource Society (FDRS) for their support during their 2016–2019 FDRS Conferences in connecting people living with lipedema and researchers.
Data availability statement
Data used in the present analysis are available upon reasonable request from the corresponding author.
Declaration of conflicting interests
Aaron W Aday reports receiving consulting fees from Aeglea outside of the current work. Paula MC Donahue is a paid consultant for PureTech Health and Tactile Medical, and has received clinical and imaging grants from LymphaTouch. Manus J Donahue is a paid consultant or advisory board member for Pfizer, Inc., Alterity, bluebird bio, Novartis, LymphaTouch, and Graphite Bio, and he is the chief executive officer for Biosight, LLC, which operates as an imaging vendor and clinical research organization: there is no actual or perceived conflict of interest with these agreements and the scope of this work. John A Beasley reports consulting fees from JanOne, Janssen, and Novartis and he has received grant funding from Bristol Myers Squibb. All other authors report no conflicts.
Funding
This work was supported by the National Institutes of Health (NIH) National Heart, Lung, and Blood Institute (NHLBI) K23 HL151871 (Aaron W Aday), R01 HL157378 (Rachelle Crescenzi), and the Lipedema Foundation (LF) Postdoctoral Research Fellowship (Rachelle Crescenzi), LF Award LF30-B (Rachelle Crescenzi and Aaron W Aday), and LF Award 12 (Manus J Donahue). REDCap and recruitment through ![]() are supported by the National Center for Advancing Translational Sciences (NCATS) Clinical Translational Science Award (CTSA) Program, award number 5UL1TR002243-03. The content is solely the responsibility of the authors and does not necessarily represent the official views of the NIH.
are supported by the National Center for Advancing Translational Sciences (NCATS) Clinical Translational Science Award (CTSA) Program, award number 5UL1TR002243-03. The content is solely the responsibility of the authors and does not necessarily represent the official views of the NIH.
Supplementary material
The supplementary material is available online with the article.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.