
Abstract

What is lipedema?
Lipedema is a painful swollen leg condition that almost exclusively affects women. It involves both legs equally, sparing the feet. Edema, or swelling, is commonly due to fluid retention. Lipedema is different. It begins as abnormal depositions of body fat in the buttocks and hips and progresses gradually to include the thighs and calves but stops at the ankles. Many patients are overweight or obese. In those who are not overweight, their lower body shape is disproportionately larger than their upper body, producing a pear-shaped appearance (Figure 1).

Lipedema in a young woman. She has an abnormal distribution of fat tissue in her buttocks, hips and thighs compared to her slim upper body and waist. In addition her legs are quite painful. Published with permission from the patient.
Who is at risk for lipedema?
The cause of lipedema is unknown. Some patients have affected female family members (a grandmother, mother, sister or daughter). Lipedema usually starts after puberty, pregnancy or menopause and is aggravated by weight gain.
What are the symptoms and signs of lipedema?
Symptoms include painful legs and symmetrical leg swelling ending abruptly just above the ankles, known as the ‘cut-off sign’, as seen in Figure 1. This swelling does not typically indent with pressure (‘non-pitting’), unless the patient also has other reasons for the edema. Swelling persists despite leg elevation. Easy bruising and the presence of varicose or small spider veins near the skin surface are commonly reported.
The feet are not involved, and the arms are less commonly affected. The swelling does not improve with elevation or weight loss.
There is substantial variability in the severity and progression of lipedema. Some patients develop mild symptoms that do not progress at all; however, others experience gradual or accelerated progression. In stage I lipedema, fat deposition is increased, but the skin is smooth and soft (Figure 1). Over time, the skin may develop an irregular appearance (sometimes referred to as the ‘mattress phenomenon’) and small masses of fat (subcutaneous nodules) may develop (stage II). Patients with stage III lipedema develop tender bulging protrusions of fat which may make walking difficult.
What are the potential complications of lipedema?
Complications are both medical and psychological. Medical complications include joint problems involving the hips and knees that can lead to difficult and painful walking. Complications of obesity (diabetes, hypertension, cardiovascular) often co-exist. Psychological problems include low self-esteem, anxiety and depression, which coupled with mobility issues frequently make weight loss hugely challenging.
How is lipedema diagnosed?
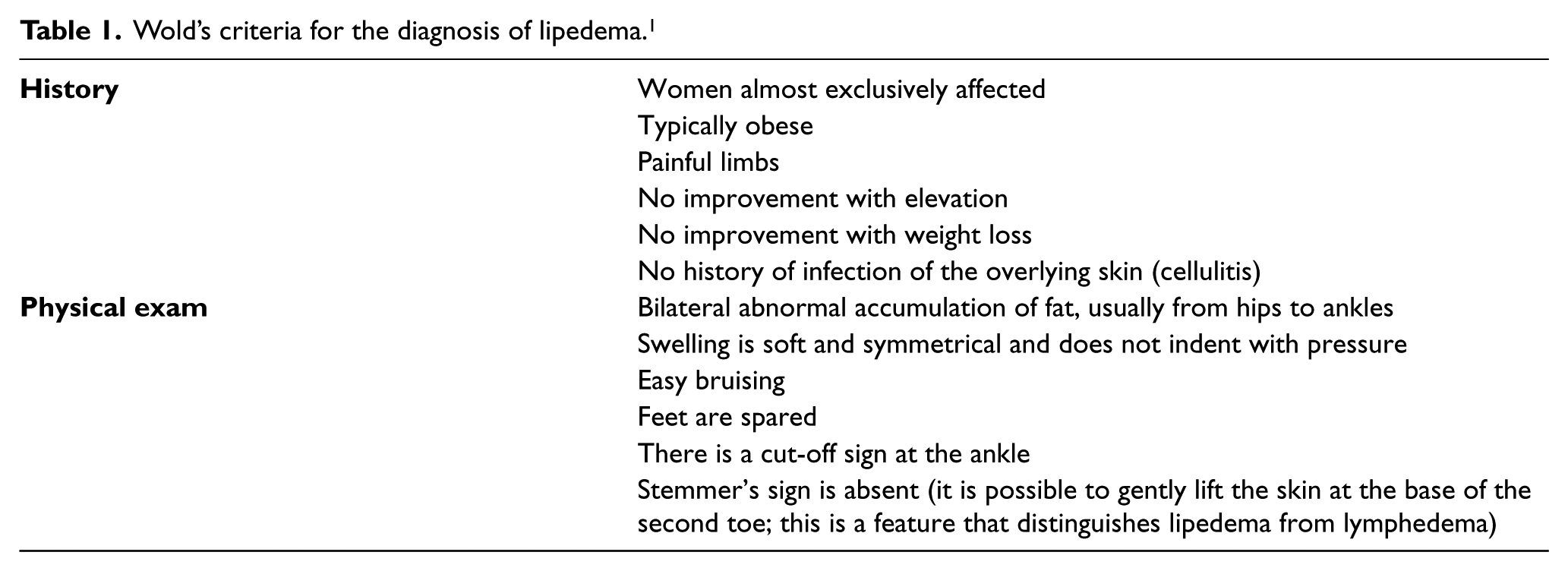
The diagnosis of lipedema depends on the clinical experience of the physician and is confirmed by a thorough history and comprehensive physical exam. Criteria listed by Wold and colleagues in 1951 help confirm the diagnosis (Table 1). 1 Special laboratory studies or scans are not required.
Wold’s criteria for the diagnosis of lipedema. 1
What other conditions may be confused with lipedema?
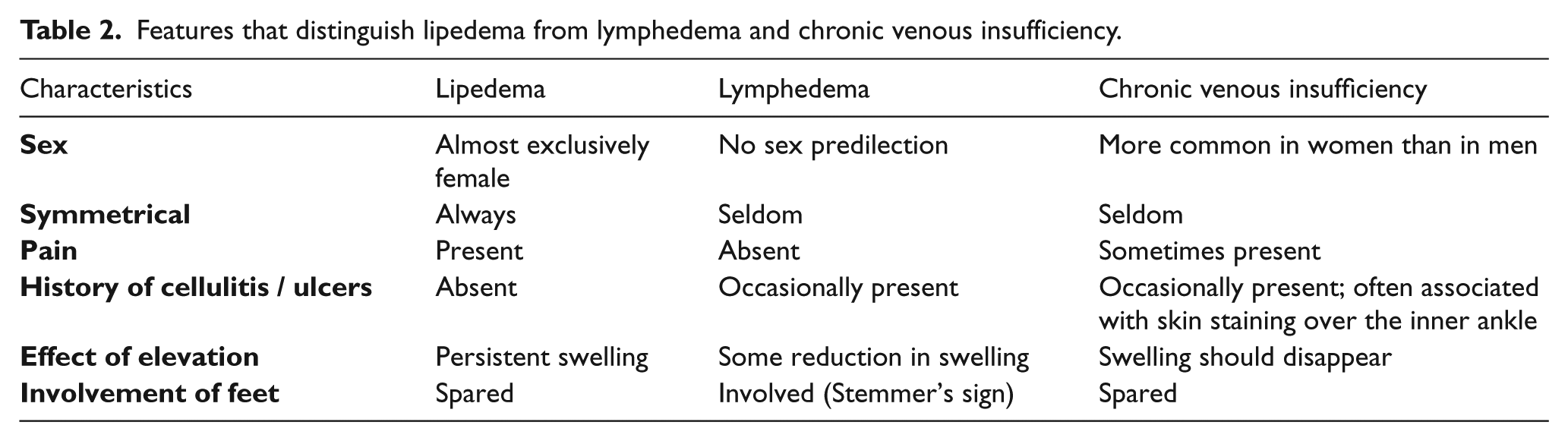
In some patients it may be difficult to distinguish lipedema from other more common diseases that cause swollen legs, including lymphedema, chronic venous insufficiency, or obesity (Table 2). More information about lymphedema is available in the ‘Lymphedema’ Vascular Disease Patient Information Page. 2 Many other causes of leg swelling exist, including dependent edema, organ failure, medications, deep venous thrombosis and the post-thrombotic syndrome. These are summarized in ‘The swollen leg’ Vascular Disease Patient Information Page. 3 These other conditions causing leg swelling may co-exist with lipedema.
Features that distinguish lipedema from lymphedema and chronic venous insufficiency.
Advanced lipedema may progress into lymphedema, a condition known as ‘lipolymphedema’. In the early stages, patients with this condition have swelling that indents with pressure (‘pitting edema’), and their feet and toes are involved.
Signs of chronic venous insufficiency are present in 20% of patients with lipedema (‘phlebolipedema’). Swelling in patients with chronic venous insufficiency is not symmetrical and indents with pressure. In addition, patients’ legs develop a rust-like stain on their inner ankles, as well as dry skin and a rash known as eczema. The combination of lipedema, chronic venous insufficiency and lymphedema is known as ‘phlebolipolymphedema’.
How is lipedema treated?
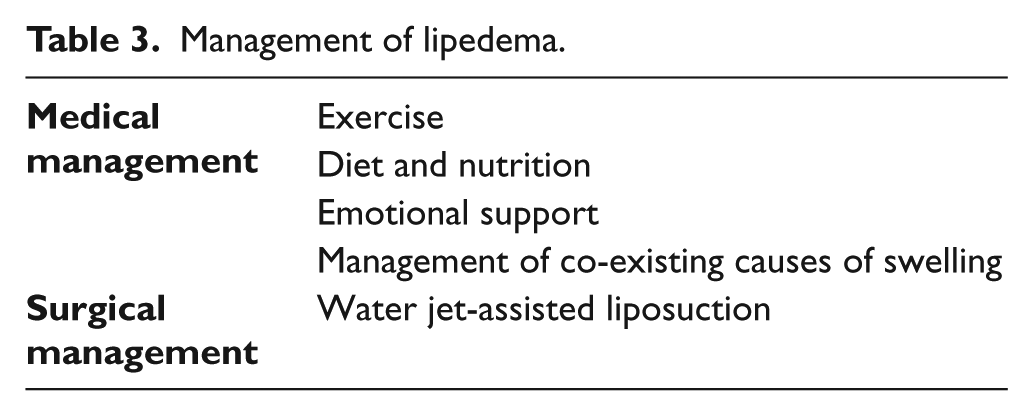
The management of lipedema is multi-faceted. It involves exercise, diet and nutrition, emotional support and management of other co-existing causes of lower extremity swelling. Water jet-assisted liposuction may be an option if conservative treatment fails.
Exercise (particularly walking, swimming, cycling, Pilates or body vibration) and a healthy diet are recommended to prevent progression of lipedema. Although weight loss may not help, prevention of additional weight gain is important, as any weight gain to the affected body areas becomes difficult to treat.
Emotional support is often overlooked. Information about patient support groups is available on www.fatdisorders.org. Counselling may also be appropriate.
Other causes of leg swelling may co-exist with lipedema and should not be overlooked during treatment. Skin care is important for patients with lipedema complicated by lymphedema or chronic venous insufficiency. Regular application of moisture creams avoids dry skin, thus reducing the risk of infection (cellulitis).
Compression stockings are useful when edema is present and may help prevent the progression of lipedema into lipolymphedema. Manual lymph drainage (MLD) and intermittent pneumatic compression therapy can be tried with varying degrees of success. Herbal medications such as horse chestnut or diosmin are often tried with varying results and are usually more effective when there is a venous component to the swelling.
Water jet-assisted liposuction is a lymph-sparing procedure that removes excess fat and is useful for patients who have not improved with conservative measures. This procedure is generally performed under local anesthesia and is less likely to damage lymphatic vessels when compared to standard liposuction procedures. Many patients report improved walking ability, less pain, and a better quality of life; the results appear to be durable over time. Unfortunately, these procedures are not widely available and are not covered by most insurance providers. It is important that the patient be assessed by a physician with experience in this type of liposuction as complications resulting in damage to the lymph vessels can result in more swelling. Many patients need to continue usual care for the long term, even after intervention.
Summary
Lipedema is a painful swollen leg condition caused by an abnormal distribution of body fat that affects both legs equally and spares the feet. Women are predominantly affected and many are overweight. Leg swelling is resistant to elevation and weight loss. Complications are medical (joint problems and difficulty walking) and psychological (anxiety and depression). Lipedema is often confused with lymphedema, chronic venous insufficiency and obesity. Management of lipedema is multifaceted and primarily medical (Table 3). Water jet-assisted liposuction is a surgical option that can remove excess fat but is expensive, time consuming and not widely available.
Management of lipedema.
Footnotes
Correction (July 2025):
Article updated online to correct the article type to “Other”.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.