
Abstract
Background:
It is not yet known whether lipedema is a progressive chronic disease or not. The aim of this paper is to describe the long-term changes in the volume of the lower limbs.
Methods:
The primary endpoint of this prospective cohort study of patients with lipedema was the percentage of volume change (PVC) during follow up. Progression was defined as when the PVC was > 10% from the baseline, whereas improvement was defined as when the PVC was < –10%, and stability as PVC −10% to 10%.
Results:
A cohort of 100 patients with lipedema were included in the study. The average follow-up period from the start of this study was 4.6 years. The average PVC was 2.8%. Stability was observed in 62% of the patients, progression in 28%, and improvement in 10%. In the univariate analysis, a significant positive association was observed between PVC and both BMI-change and waist-to-height ratio (WHtR)-change. The more the BMI increased, the more the lipedema progressed (p < 0.0001), as did the WHtR (p < 0.0001). In the adjusted regression analysis, age was not seen to be an influencing factor for PVC. Regarding maintenance therapies, no associations were observed.
Conclusion:
Lipedema was seen to be stable in two-thirds of the patients. Age was not related to progression. Progression was related to WHtR increase, which is an indicator of abdominal fat gain. This demonstrates the relationship between fat gain and lipedema progression.
Background
Lipedema is a chronic disease that affects many women worldwide, causing them swelling and an abnormal fat deposition in the lower limbs (LL), bruising, and pain. 1 There is an evident disproportion in the distribution of fat, involving the LL, and sometimes upper limbs.2,3 Owing to the lack of awareness and knowledge among professionals, the real prevalence is underestimated due to misdiagnosis or failure to refer patients.2,4 –7
Despite etiopathogenic mechanisms having not yet been fully described, lipedema has been associated with lymphatic dysfunction, with a genetic background and hormonal changes. 8 Patients’ main complaint is the enlargement of the LL with pain or discomfort. As the disease progresses, leg heaviness may increase and impair mobility 9 and global capacity, but it can reduce quality of life, even in the early stages.9,10
Biomedical research on lipedema has increased in the last few years, but there is a significant knowledge gap regarding progression of the disease. Few patient cohorts have been published; however, it has already been observed that lipedema tends to be more severe in older patients. This would suggest that lipedema worsens with age (Figure 1). 11 Discussion continues today regarding whether this disease really is a progressive condition. The aim of our study was to describe long-term changes in volume of the LL in a prospective cohort of patients with lipedema.
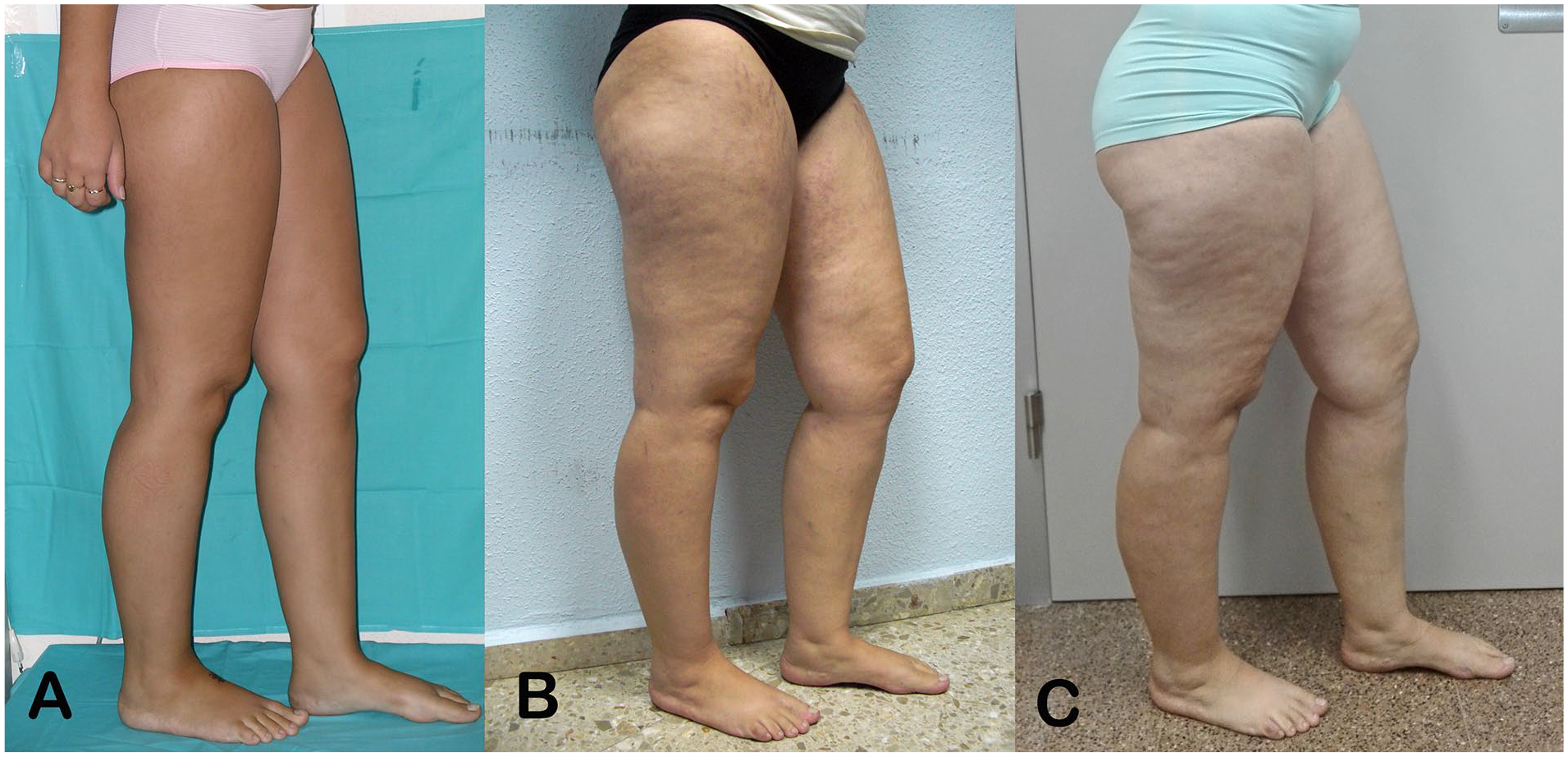
Evolution of lipedema in a 15-year-old girl with Type III lipedema over 10 years.
Methods
Study design
This is an ongoing, prospective, noninterventional cohort study in patients with lipedema, which aims to analyze the characteristics of lipedema for the purposes of biomedical research. The study was approved by the Research Ethics Committee of the La Fe University and Polytechnic Hospital, and written informed consent was obtained from all participants. All procedures followed were in accordance with the ethical standards of the committee in charge of human experimentation (institutional and national) and with the Helsinki Declaration of 1964 and later versions. Lipedema was defined as patients with LL enlargement with fat deposition, and as disproportion between the upper and lower parts of the body, associated with pain or discomfort in LL. Cases are recruited prospectively and consecutively to avoid selection bias. The recruitment period and follow up is still in progress, so the study will stay active as long as the research team is able to continue.
Study population
Female patients at the Lymphedema Unit of the La Fe University and Polytechnic Hospital were screened by the investigators and checked for eligibility. Eligibility criteria include age > 18 years with bilateral LL enlargement, disproportion between the upper and lower part of the body, and at least three of the following symptoms of lipedema: spontaneous or provoked pain or tenderness, easy bruising, family history of lipedema, absence of LL injuries, absent Stemmer sign, symmetrical LL involvement, and no swollen feet. The selected patients had their LL volume measured at baseline and at least once, 1 year after. The measurements were performed by IFC in all the cases. The data included in this paper were from the first follow up with volumetry. Pregnancy, renal, hepatic or heart failure, thrombosis, infection, active cancer, corticosteroid treatment, traumatic history in LL, and liposuction history are criteria for exclusion. Lack or withdrawal of consent was a criterion for exclusion. Patients were advised to wear their compression garments during waking hours and to do physical exercise as part of their daily care.
Objectives and study variables
The primary endpoint was the percentage of volume change (PVC) during follow up, calculated with the following formula: PVC = (volume at follow up – volume at baseline) × 100/volume at baseline. The LL volume was calculated with perimeter measurements using a tape measure (C). Measurements were taken from the dorsum of the foot (C1) and repeated every 4 cm proximally as far as the root of the limb (Cn). The calculation was made using the Kuhnke formula: 12 [Volume = (C12 + C22 + Cn2)/π].
Although water displacement or perometer are the gold-standard for volumetry, these methods are not available in our center. The indirect volumetry with tape measurements has shown excellent inter- and intra-observer reproducibility in comparison to water displacement and in terms of low cost, simplicity, and reliability it has been recommended as the method of choice in clinical practice.13 –15 A recent study that compares different methods to measure volume concludes that circumferential volumetry is accurate with an error < 2%. 16 As intra-rater reliability was always better than inter-rater reliability, patients were evaluated by the same examiner (IFC).
Progression of disease was defined as PVC > 10% from baseline; improvement: PVC < –10%; and stability: PVC −10% to 10%. The secondary aims of this paper include analyzing the influence of clinical features, maintenance therapies, and compliance with PVC.
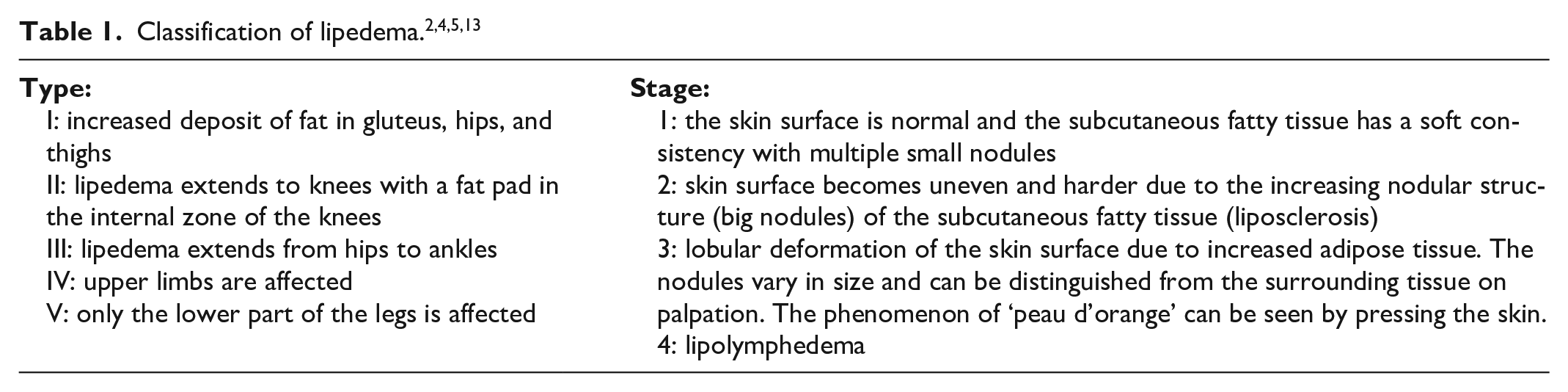
Currently, lipedema can be classified according to the localization of the fat accumulation and the severity of clinical manifestations. Based on inspection and palpation, lipedema can be classified into four clinical stages of severity (Table 1).4,6,17 However, stage 4, lipolymphedema, is controversial. The clinical classification of lipedema into stages does not reflect the complete severity of symptoms and has limited relevance in management of the disease. 14
Chronicity was defined as the duration of the disease, calculated as the time between the onset of the symptoms reported by the patient and the date of recruitment, in years.
Statistical methods
Descriptive statistics were obtained for all variables. For continuous variables, the mean, the SD, and the median were calculated, and absolute and relative frequencies were obtained for categorical variables. Qualitative variables were compared with the chi-squared test and continuous variables with the analysis of variance (ANOVA). All statistical analyses are performed with IBM SPSS, Version 22 (IBM Corp., Armonk, NY, USA).
Ethical issues and authorization
All procedures followed were in accordance with the ethical standards of the committee in charge of human experimentation (institutional and national) and with the Helsinki Declaration of 1964 and later versions.
All participants had to provide written, signed, informed consent to be included. The study was approved by the Research Ethics Committee of the La Fe University and Polytechnic Hospital, with the number 2014/0099.
Results
Sample characteristics
From the 195 patients with lipedema recruited in our prospective cohort from September 2012 to September 2023, those who had at least two volume measurements at baseline and more than a year after were included (100 cases) in this study. The median follow up was 4.6 years (SD: 2.9), and 25% of patients had a follow up of more than 7 years. The first follow up had a median of 3.1 years (SD: 1.9) after baseline. The average patient age was 47.6 years. The demographic and clinical characteristics of the patients are shown in Table 2.
Demographic and clinical characteristics.
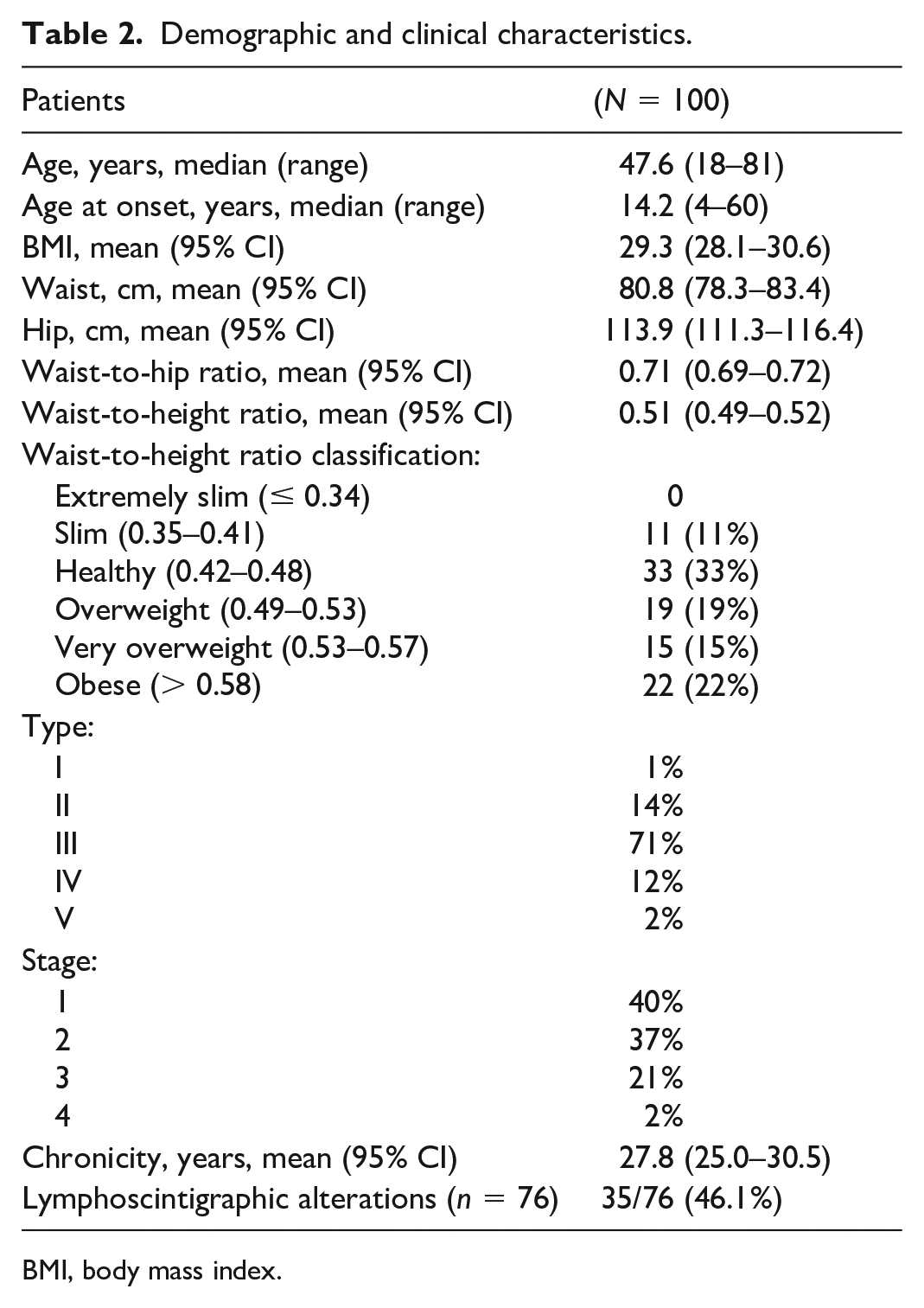
BMI, body mass index.
The most frequent type of lipedema was Type III, which affects patients from the ankles to the hips, and present in two-thirds of the patients. Furthermore, most patients were in stages 1 and 2. Taking into account the waist-to-height ratio (WHtR), 44% of the patients were slightly underweight or of a normal weight, 19% were overweight, and 37% were obese or morbidly obese (Table 2).
Relationships between clinical features
The greater the patient’s age, the more advanced the stage of lipedema: stage 1 (mean of WHtR [95% CI]): 39.1 (35.2–43.0); stage 2: 49.6 (45.5–53.6); stage 3: 57.1 (50.9–63.2); stage 4: 55.7 (22.1–89.3); p < 0.0001. WHtR was greater in older patients (β: 0.570; p < 0.0001). The greater the WHtR, the more advanced the stage of lipedema: stage 1 (mean of WHtR [95% CI]): 0.46 (0.44–0.48); stage 2: 0.52 (0.49–0.55); stage 3: 0.56 (0.52–0.60); stage 4: 0.59 (0.59–0.60); p < 0.0001.
Maintenance therapies
The maintenance therapies followed by the patients are shown in Table 3. A total of 76% of the patients wore the compression garments prescribed by the doctor and 66% carried out physical exercise several days per week. Few patients underwent other physical therapies (Table 3).
Maintenance therapies for patients with lipedema (N = 100).
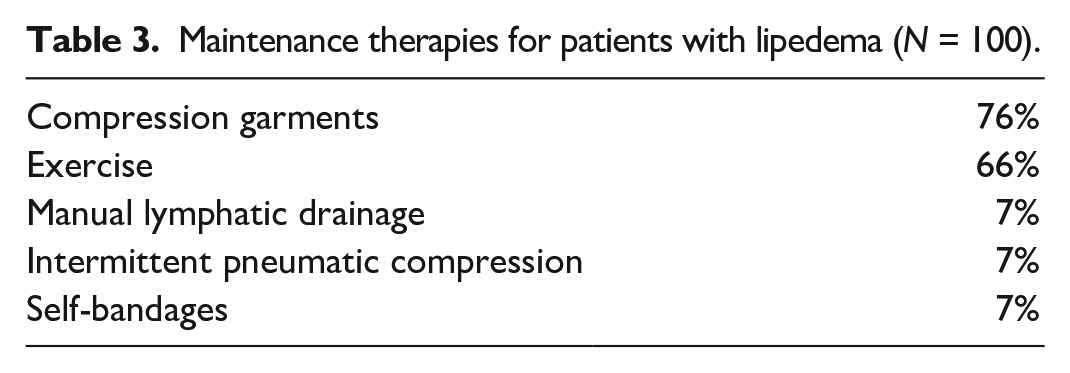
Patients who complied regarding the compression garments wore them for an average of 10.9 hours per day (95% CI: 10.2–11.3) and 6.0 days per week (95% CI: 5.7–6.3). The most frequent prescription was for pantyhose (75.6%), with circular tissue (60.3%) and CCL 2 (95%). Patients who followed the doctor’s advice regarding physical exercise, did so for a mean of 5.1 hours per week (95% CI: 4.3–5.8). The most frequent exercises were walking (34%) and gym training (20%).
Volume change at follow up
The mean PVC was 2.8% (95% CI: 0.6–5.0). Stability of the volume was observed in 62% of the patients, progression in 28%, and improvement in 10%.
The mean of BMI-change at follow up was 2.8% (± SD: 11.2) and the mean of WHtR-change was 2.8% (± SD: 7.7). Patients who showed progression presented with a higher increase in BMI and WHtR (Table 4).
Evolution of percentage of volume change and change in nutritional status for patients with lipedema (N = 100).
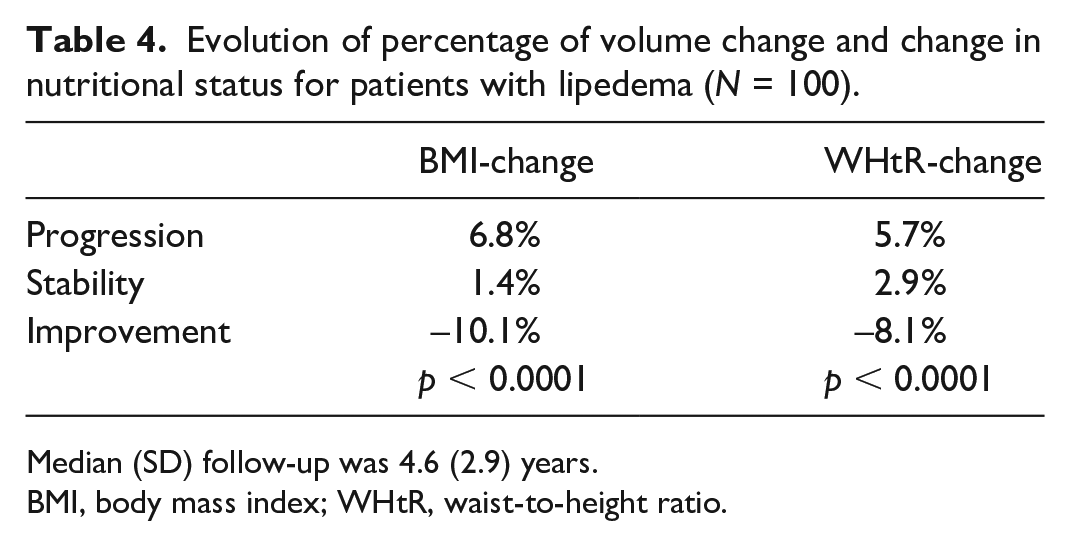
Median (SD) follow-up was 4.6 (2.9) years.
BMI, body mass index; WHtR, waist-to-height ratio.
In the univariate analysis, a significant positive association was observed between PVC and both BMI-change and WHtR-change (Table 5). The more the BMI increased, the more the lipedema progressed (β: 0.78; p < 0.0001). Likewise, a notable positive correlation was identified between PVC and the change in WHtR. With an increase in WHtR, lipedema showed a corresponding progression (β: 0.68; p < 0.0001) (Table 5, Figure 2).
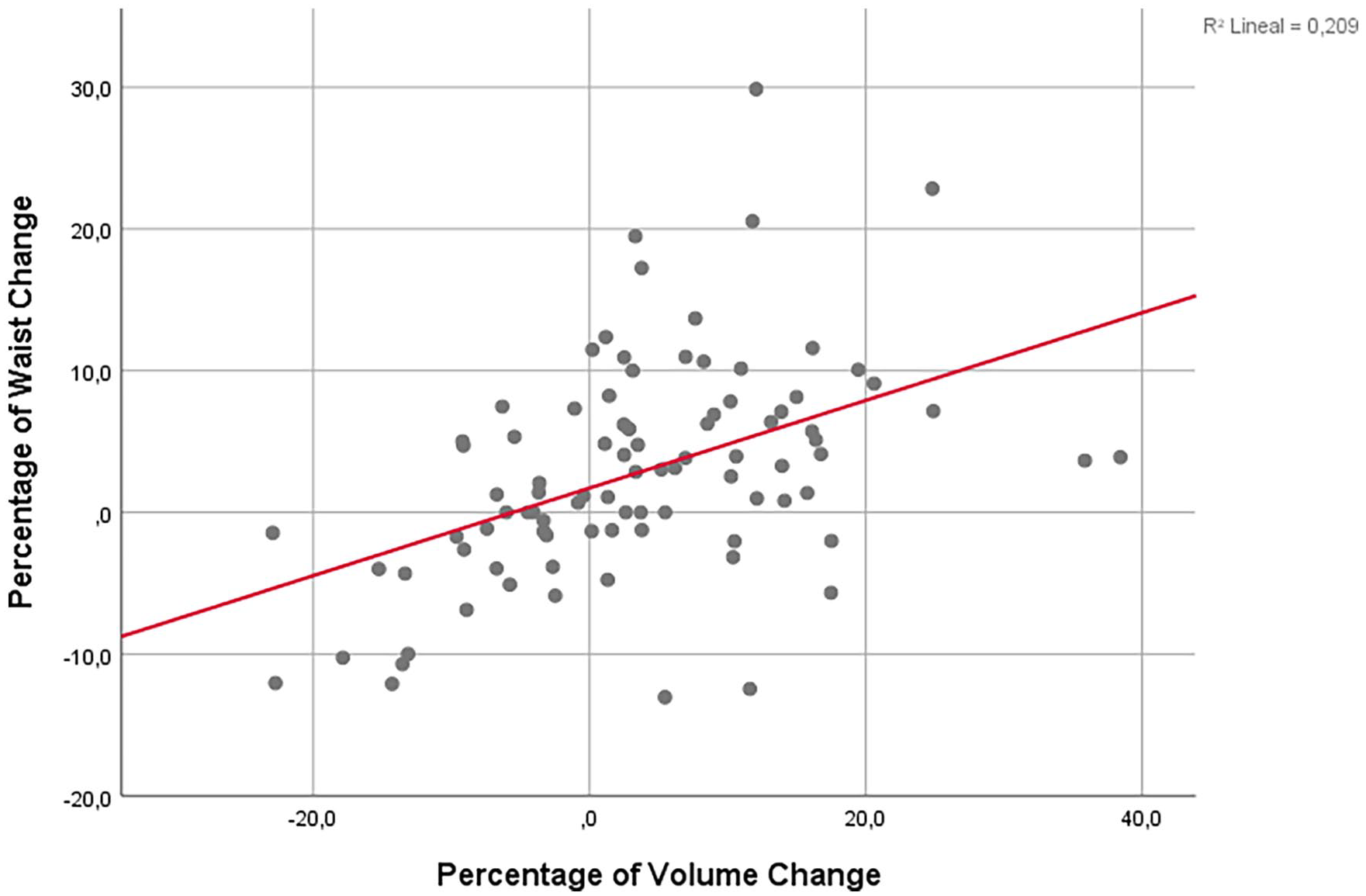
Analysis of the relationship between waist-to-height ratio-change and percentage of volume-change (β: 0.677; p < 0.0001).
Factors related to percentage of volume change (univariate and multivariate analysis) in patients with lipedema (N = 100).

Values in parentheses are 95% CIs.
BMI, body mass index; WHtR, waist-to-height ratio.
Age correlated with BMI (Pearson: 0.48; p < 0.0001) and WHtR (Pearson: 0.57; p < 0.0001), which means that a higher BMI and a higher WHtR were found in older patients. But age was not associated with a higher PVC (Pearson: –0.087; p = 0.39); so progression was not related to age. In the adjusted regression analysis, age did not influence as a confounding or interaction factor regarding volume change (PVC) (Table 5).
No significant differences were found between the age groups in pre-, peri-, and postmenopausal women and the PVC (p = 0.595). Although there was a trend of greater volume increase in premenopausal women, this did not reach statistical significance.
No relation was observed between chronicity, type, and stage of lipedema, or lymphoscintigraphic findings (Table 5).
Lymphoscintigraphic alterations were seen in 35 patients (n = 76): 46.1%. The degree of these findings were scored by a nuclear medicine specialist as: absent (55.4%), low grade (20%), low–moderate grade (18.5%), and moderate (6.2%). 18 No relation was observed between the presence of lymphoscintigraphic findings and BMI (p = 0.21), nor with the grade of these findings (p = 0.405).
Regarding maintenance therapies, no associations were observed between manual lymphatic drainage, intermittent pneumatic compression, bandages, exercise, or compliance with compression garments (Table 5). Although it was not statistically significant, patients who showed improvement wore their compression garments longer than those who remained stable or whose lipedema worsened (progression: 47.1 hours/week [h/w], 95% CI: 33.2–61.0; stability: 51.4 h/w, 95% CI: 42.2–60.6; improvement: 60.1 h/w, 95% CI: 28.1–92.1), p = 0.63.
Discussion
This is the first study to analyze the natural history of lipedema in a cohort of patients.
In this prospective cohort of 100 patients with lipedema, the follow up of the LL volume showed that lipedema was stable in two-thirds of patients. Progression was related to a central fat increase, evaluated with WHtR, and was not associated with age or maintenance therapies.
Is lipedema a progressive disease?
Many authors have defined lipedema as a progressive condition; however, up to the present day no studies have been carried out regarding this issue.
Though more severe stages of lipedema associated with lymphedema are probably related to obesity and have been considered as the natural evolution of the disease, our observations show that not all the patients in these advanced stages were elderly. On the contrary, there were also younger patients who showed advanced stages of lipedema.
As far as LL volume is concerned, our results show that lipedema was a stable disease in two-thirds of our patients; some showed progression but 10% improved.
Regarding pathophysiology, the progression of lipedema defined by stages has been associated with adipocyte hypertrophy, progressive fibrosis, and inflammatory processes in the affected areas. 19 It is worth noting that these processes were not linked to age. The current classification of lipedema in stages is now under debate in the Lipedema World Alliance 20 and other scientific forums, as it does not describe the real evolution of patients. Even in the early stages, it is associated with several health problems and a lower quality of life. 9
Body fat and percentage of volume change (PVC)
The most important factor related to volume progression was the increase in body fat.
The association of an increase in BMI and the increase in LL volume was an observation that can be interpreted in two ways. Is the increase in LL volume the cause of the weight increase and therefore the BMI, or is it the increase in body fat which causes the disease to progress? Are more obese patients going to progress, or is lipedema progression the cause of obesity? Given that WHtR is a more accurate diagnostic tool for lipedema patients than BMI, and that the BMI can increase in the same way as LL volume, we used this ratio to compare the results. Waist circumference is not influenced by LL volume, and is an indicator of central fat. 21 WHtR classification is shown in Table 2. We found that when WHtR increased, the volume of LL increased too. Thus, the progression of lipedema is linked to the increase in body fat.
Age and PVC
Even though in older patients more advanced stages were more frequent, our study showed age was not related to the progression of volume in the long term. According to literature in this field, the onset and evolution of lipedema is linked to hormonal changes.1,4 –6,11 In retrospect, the cohort of patients should have had a more homogeneous age range to avoid heterogeneity in hormonal conditions. 22
Age was also related to a higher WHtR. If the patient gains abdominal fat, the amount of total body fat is also increased, and this causes a progression in LL volume. A possible explanation of this could be the influence of inflammation on the pathophysiology of lipedema. Inflammation as the cause or the consequence of obesity may be related to the progression of lipedema volume. This hypothesis is important because it confronts the established idea that lipedema is a progressive disease and has a clear implication for daily practice. The focus of attention in the management of lipedema patients must be on maintaining an adequate nutritional status.
Maintenance therapies and PVC
The patients’ adherence to maintenance therapies was not related to the progression of the lipedema. In our sample, the number of patients undergoing manual lymphatic drainage, intermittent pneumatic compression, or self-bandaging was very low, so this was an expected result. However, a significant number of patients complied with advice on compression and exercise. Regarding compression garments, the prescription aimed to reduce the edema component (if present), to improve circulation, to reduce pain, and to produce the antiinflammatory effect of compression. Patients reported significant benefits in alleviation of pain and discomfort,23,24 as well as a reduction in volume and thickness of subcutaneous adipose tissue. 25 However, more research is still necessary. Clinical trials are needed to demonstrate the effectiveness of compression in lipedema. 26 The significant edema reduction with compression in lymphedema and venous insufficiency may be explained by a reduction in the amount of lymphatic fluid in the tissue rather than an improvement in lymphatic transport. 23 Therefore, as the edema in lipedema is minor, this effect was not so significant, and this can explain our results.
Recent guidelines state that the use of compression aims to reduce symptoms (pain, sensation of heaviness), reduce edema, and optimize the contours of the extremities. 27 Compression is known to have an antiinflammatory and oxygenating effect on tissues, and they can prevent fluid buildup to prevent swelling and possible progression to lymphatic insufficiency. Patients should be informed that compression is not appropriate for adipose tissue reduction. 24
Compliance was reported by the patients and not objectively measured, so this result should be interpreted with caution. A holistic strategy for managing lipedema, encompassing a comprehensive approach rather than focusing solely on basic pathophysiological treatment, is more advantageous for patients. 28 It is crucial to tackle key active epigenetic sociobiological factors linked to lipedema, including obesity, a pro-inflammatory diet, hyperactivation of the stress axis, and prolonged periods of sitting. Addressing these factors is essential, as they exert a substantial impact on the development and progression of chronic degenerative venolymphatic disease. 29
Limitations
One of the limitations of the study is that progression was linked to the increase in volume, when there are other parameters that could evaluate the evolution of the disease. Stage is not considered a valid measure today. According to Ernst, each lipedema stage should be seen as a complex entity because it represents the sum of several conditions, such as the presence of comorbidities, nutritional status, and family history. 22 The symptoms could be important, although as subjective variables they are influenced by many other factors. Histopathology would be an effective method, although due to technical difficulties and discomfort for the patient it is not routinely used. Other limitations of this study include the small sample size and heterogeneity in the age range and follow-up; however, the study is ongoing.
Conclusion
Lipedema in two-thirds of the patients remained stable in this study. Age was not related to progression. Progression was related to abdominal fat increase, evaluated as waist-to-height ratio (WHtR). When the patient gained abdominal fat, the volume of their lower limb also increased. This demonstrates the relationship of fat gain with worsening lipedema and highlights the importance of addressing this issue as a key approach in treating lipedema. Further research is warranted to detect those patients in whom the disease will progress despite treatment.
Footnotes
Acknowledgements
We thank Carmen Román-Ribes (Nursing Assistant, Hospital Universitari i Politècnic La Fe, Valencia, Spain) for her contribution with the measurements for volumetry.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.