
Abstract
Background:
Patients with lymphedema and lipedema share physical exam findings that may lead to misdiagnosis. Poor mobility is common in patients with obesity and patients with lymphedema and lipedema. This may constitute a risk factor for venous thromboembolism (VTE). Our objective was to evaluate the association of VTE in obese patients with lymphedema and lipedema.
Methods:
The National Inpatient Sample (NIS) was searched from 2016 to 2020 to identify hospital admissions of obese female patients with lymphedema and lipedema. Patients were analyzed in the context of presence or absence of VTE while adjusting for complex cluster sampling techniques. Predictors of VTE were accessed by multivariable regression.
Results:
Lymphedema was identified in 189,985 patients and lipedema in 50,645 patients. VTE was observed in 3.12% (n = 374,210) of patients with obesity. In patients with obesity, VTE was more common in patients with lymphedema than without (2.6% vs 1.6%; p < 0.01). Similarly, VTE was more common in patients with lipedema than without (0.6% vs 0.4%; p < 0.01). After multivariable logistic regression, VTE events in obese patients with lymphedema were higher versus without (OR 1.6; CI 1.08–2.43; p = 0.02). Similarly, VTE events were more common in obese patients with lipedema versus obese patients without lipedema (OR 1.20; CI 1.03–1.41; p = 0.02).
Conclusions:
In this hypothesis-generating study, lymphedema and lipedema show a positive association with VTE after adjusting for baseline patient characteristics such as obesity, which is a known independent risk factor for VTE. Mechanisms whereby lymphedema and lipedema are associated with VTE should be investigated.
See Commentary: Carroll B. Lymphedema and lipedema: More than a swollen limb? Vasc Med 2024; 29:48–49.
Background
Venous thromboembolism (VTE) is a driver of morbidity and mortality. 1 VTE has an estimated annual global incidence of one to two per 1000 persons with incremental direct medical costs reaching $12,000 to $15,000 per patient in the first year following diagnosis.2,3 Deep vein thrombosis (DVT) alone is observed in up to two-thirds of this population. 4 Signs and symptoms at presentation, although not diagnostic, play an important role in the suspicion and risk stratification of patients with VTE. Lower-extremity swelling and edema are common DVT symptoms in the acute medical setting. These physical exam findings also occur in a myriad of other conditions, including: heart failure, nephrotic syndrome, infections, lymphedema, chronic venous insufficiency, and lipedema. 5
In patients with lymphedema and lipedema, lower-extremity edema and a suboptimal quality of life are common findings.6,7 Limited mobility, common in lymphedema and lipedema, is also a risk factor for VTE. Elevated body mass index (BMI) is not only an independent predictor of VTE events in the general population but associated with increased risk of developing lymphedema.8,9 Clinical exam findings of lymphedema are commonly missed, even by trained medical professionals. 10 Distinguishing lymphedema from lipedema is even more challenging when both conditions co-exist in the same patient (lipo-lymphedema). 11 A consequence of a missed diagnosis of lipedema or lymphedema may be the impact on subsequent VTE events. Limited data exist for lymphedema as a potential risk factor for VTE in patients with obesity.
Lipedema is an orphan disease, frequently overlooked by medical professionals due to deficiencies in general medical education as well as a lack of understanding about its underlying etiology. As a progressive condition involving abnormal limb distribution of adipose tissue and increased capillary permeability leading to fluid accumulation, outcomes in patients with lipedema deserve careful attention. 12 Though not fully understood, microvasculature dysfunction in addition to tissue inflammation were proposed as underlying mechanisms for asymmetric adipocyte deposition in the limbs of patients with lipedema.13–15 The afore-mentioned data place the vascular internist in a strong position to further evaluate patients with lipedema for the purpose of risk factor modification, especially for VTE. As such, the primary goal of this investigation was to capitalize on a large clinical dataset to investigate independent predictors of VTE and adverse outcomes in lipedema and lymphedema in the context of BMI, comparing this to other independent predictors of VTE. We also explored clinical co-morbidities common to lipedema and lymphedema to provide more insight into these disorders.
Methods
Data for this study were obtained from the Agency for Healthcare Research in Quality (AHRQ) Nationwide Inpatient Sample (NIS) from January 2016 to December 2020. 16 Because AHRQ and NIS collect de-identified data, institutional review board approval was waived at the time of study design. IRB approvals there therefore not required. The NIS is an all-payer, administrative claims-based database containing information about patient discharges linked with unique nonfederal hospitals in the United States of America. The NIS approximates a 20% stratified sample of all discharges from US community hospitals, excluding rehabilitation and long-term acute care hospitals according to hospital types, patient volume, teaching status, location, and geographical region. NIS contains clinical and resource utilization information with safeguards to protect privacy and identity of the patients. Each author is responsible for study design, analysis of the data, and accuracy of the analysis presented.
Study population
Patients carrying a discharge diagnosis of obesity and BMI ⩾ 30 kg/m2 were identified using the International Classification of Disease (ICD) 10th revision, Clinical Modification (CM) (ICD-10-CM) coding in the NIS database for the years 2016, 2017, 2018, 2019, and 2020. ICD-10-CM codes utilized for Lymphedema (I89.0 or I89.9) and Lipedema (E88.2 or R60.9) were selected based on previously published studies and billing recommendations and specifically proposed by the Lipedema Foundation, an acknowledged group of experts in the care of patients with lipedema.17,18 The study population was identified by the presence of either one or both of the above-mentioned ICD codes in their categories. Patients were further stratified by the presence or absence of obesity with the help of ICD-10-CM codes (Supplemental Table 1, available online). A comparison among patients with obesity was based on the presence of VTE. Because lipedema is a medical condition identified almost exclusively in women, our investigation of large datasets in the NIS focused on female sex, given a secondary goal was to compare VTE outcomes directly with lymphedema. Patients under the age of 18 were excluded from the study as lipedema is more common in middle-aged women. 19
Statistical analysis
All analyses were conducted using complex survey analyses which account for hospital stratification, clustering, and discharge weights in the NIS domain. Independent sample t-tests were used to evaluate the continuous variables, which are expressed as means ± SD. Pearson’s chi-squared test was used to evaluate categorical variables, which are expressed as absolute values and their percentage of the study population. Patient groups were compared by baseline characteristics displayed in Table 1. Univariate logistic regression identified the potential predictor co-variates of VTE in lymphedema and lipedema patients with and without concomitant obesity. Statistically significant variables with a p-value less than 0.05 after univariate regression were finally included in the multivariate logistical regression model to evaluate lymphedema and lipedema as potential predictors of VTE. All statistical analyses were performed using a standard software package (Stata, version 17.0; StataCorp, College Station, TX, USA).
Baseline characteristics of the female population with obesity (weighted sample) based on the presence or absence of venous thromboembolism (VTE).
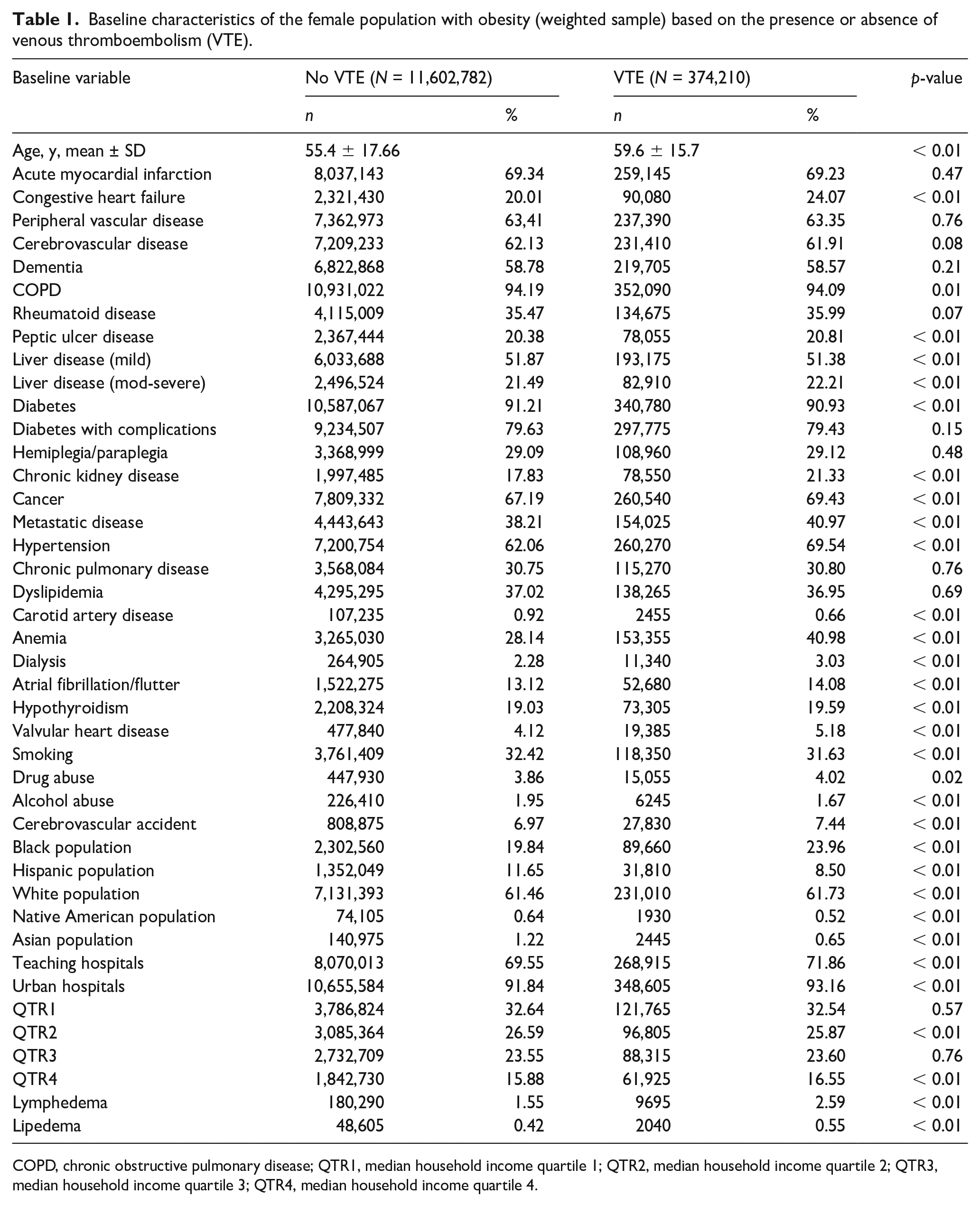
COPD, chronic obstructive pulmonary disease; QTR1, median household income quartile 1; QTR2, median household income quartile 2; QTR3, median household income quartile 3; QTR4, median household income quartile 4.
Results
A total of 11,976,992 hospital admissions with obesity were identified and included in the analysis. Lymphedema was observed in 1.6% (n = 189,985) of the population. Patients with lymphedema had a higher prevalence of congestive heart failure (3.2% vs 1.2%; p < 0.01), hypertension (79.7% vs 62%; p < 0.01), chronic kidney disease (CKD) (37.9% vs 30.6%; p < 0.01), dyslipidemia (40.7% vs 37%; p < 0.01), and hypothyroidism (27.5% vs 18%; p < 0.01). CKD occurred twice as frequently in patients with lymphedema with obesity (30.8% vs 17.1%; p < 0.01).
Lipedema was diagnosed in 0.4% (n = 50,645) of the patient population. CKD (20.29% vs 17.32%; p < 0.01), cancer (67.4% vs 68.5%; p = 0.02), hypothyroidism (23.3% vs 19%; p < 0.01), and rheumatoid disease (35.5% vs 36.7%; p = 0.02) were more common in patients with lipedema at baseline.
Overall, VTE was observed in 3.12% (n = 374,210) of patients with obesity. Patients with VTE had a higher prevalence of CKD, CHF, cancer, metastatic disease, and hypertension compared with obese patients without VTE. Lymphedema was nearly twice as prevalent in patients with VTE (2.6% vs 1.6%; p < 0.01). Similarly, lipedema was observed in 0.6% of the patients with VTE compared to only 0.4% in patients without VTE (p < 0.01) (Table 1).
By multivariable logistic regression analysis, the odds of VTE events in obese patients with lymphedema were 1.5-fold higher than in patients without lymphedema (OR 1.5; CI 1.4–1.6; p < 0.01). Similarly, patients with lipedema also had greater odds of VTE events (OR 1.2; CI 1.1–1.3; p < 0.01) (Table 2).
Univariate and multivariate logistic regression for predictors of venous thromboembolism.
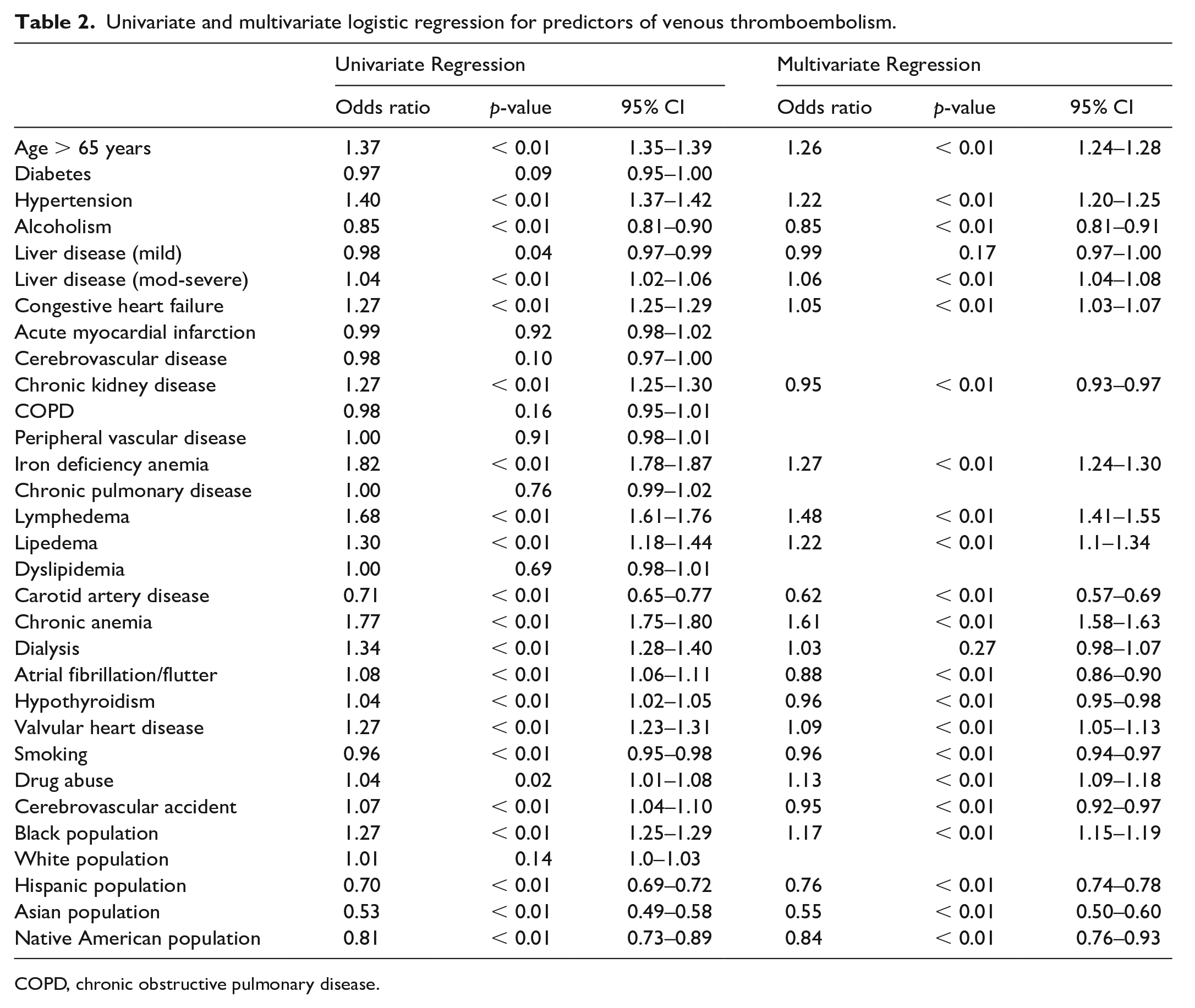
COPD, chronic obstructive pulmonary disease.
Patients with obesity > 65 years of age more commonly had VTE events (OR 1.26; CI 1.2–1.3; p < 0.01). Among other co-variates, hypertension (OR 1.22; CI 1.2–1.3; p < 0.01), iron deficiency anemia (OR 1.27; CI 1.2–1.3; p < 0.01), and drug abuse (OR 1.13; CI 1.1–1.2; p < 0.01) were independent predictors of VTE events. Black women also had higher odds of developing VTE (OR 1.17; CI 1.15–1.19; p < 0.01) (Table 2 and Figure 1).
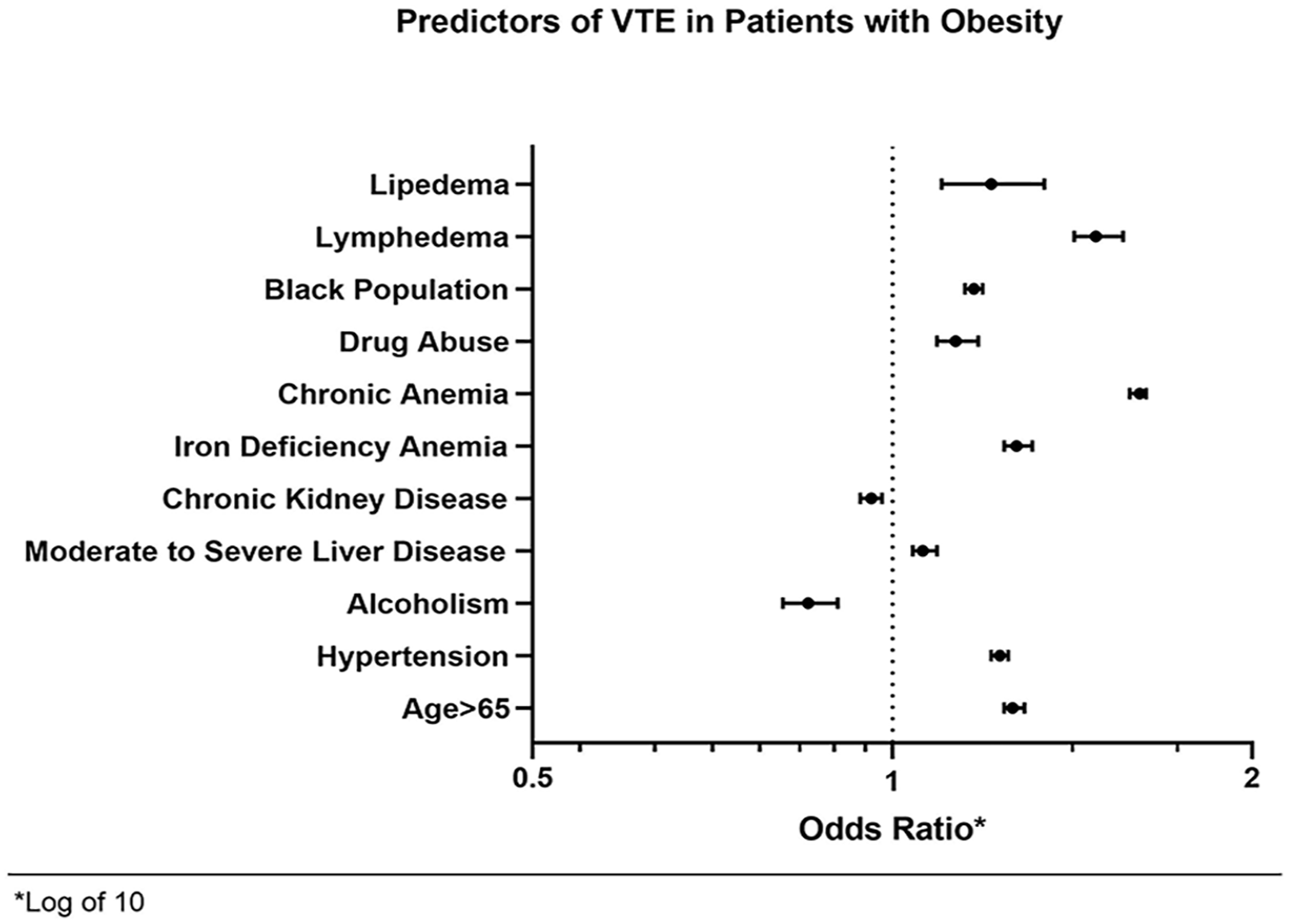
Independent predictors of venous thromboembolism in patients with obesity.
Discussion
This investigation revealed that lymphedema and lipedema are associated with a higher risk for VTE in the obese patient population. Limited mobility is common in the elderly and obese population and is therefore associated with an increased VTE risk.20–24 Similarly, in patients with lymphedema, limb volume reduction has demonstrated improvement in the mobility of patients with obesity. 25 This suggests the risk of VTE is higher in the elderly individuals with lymphedema and may also be observed in lipedema. Because limited mobility is common to lymphedema and lipedema and is more frequent in patients with obesity, this may potentiate the over-all combined risk of VTE.
Among other predictors of VTE, disorders associated with persistent inflammatory conditions including CKD, rheumatoid disease, and hypothyroidism increased the risk of VTE events. At baseline, female patients above 65 years old were at a higher risk of developing VTE. This finding was in concordance with other large studies suggesting a temporal relationship between advancing age and increased frequency of VTE events.26–28 An increased incidence of VTE in the elderly is also attributed to increased fibrinogen, factors VIII and IX, and other proteins of the coagulation cascade, without a proportional increase in circulating antithrombotic proteins.29–31 In addition, elevated interleukin 6 (IL-6) and C-reactive protein (CRP) in the elderly population may portend an imbalance toward a pro-inflammatory state, which contributes to thrombosis risk.32–34
Chronic vascular inflammation as a consequence of lymphatic dysfunction is common in lymphedema.35,36 Increased inflammatory markers including leukotriene B4 (LTB4) were reported in lymphedema, suggesting a mechanistic role in its pathogenesis. 37 Lipedema is regarded as a disorder with altered adipogenesis, microangiopathy, and dysregulated lymphatic function. Studies suggest an imbalance between pro-inflammatory and antiinflammatory cytokines in adipose tissue that may increase VTE risk.38–40 Lipedema and lymphedema are associated with substantial morbidity and decreased quality of life. All these factors can increase the risk of VTE, as noted in our analysis.
Study limitations
This is a retrospective analysis using an administrative claims-based database which raises multiple limitations. Being retrospective in nature, merely an association instead of a causal relationship between lymphedema or lipedema and VTE events can be established by our study. Furthermore, this database consists of estimates from the US population which is not representative of the global population. Hence, inferences cannot be generalized to other demographics and populations.
Identification of diseases in our study was based on ICD-10 codes. Lipedema, being an under-appreciated disease, is not well-characterized in the administrative coding system by a unique identifier. For the purposes of our study, surrogate diagnoses codes for lipedema were used based on recommendations from the Lipedema Foundation to identify the population of interest. Obesity is historically seen in up to 40% of the US population; however, our estimates suggest ~30% the population had either elevated BMI or obesity. Similarly, our study population underestimates the presence of lipedema as compared to previously published studies. This is due to a lack of disease-specific ICD-10-CM codes, underdiagnosis given that lipedema is under-recognized by clinicians, and loss of sample volume as a consequence of inadequate ICD coding during hospital encounters.41,42 Under-coding or mis-coding may have also led to decreased sample size in our study. The study population was selected based on ICD-10 codes for lymphedema, including ‘I89.0’ which includes patients with lymphedema not classified elsewhere. Inclusion of these patients may have also included patients with secondary upper-extremity lymphedema after mastectomy despite a dedicated code of ‘I97.2’. This could have led to underestimation of VTE risk in our patient population. Lastly, absence of data on the timing of these events makes it impossible to establish a tangential relationship between risk factors and subsequent VTE events.
Conclusion
Our observation that VTE remains prevalent in patients with lymphedema and lipedema even after adjusting for baseline characteristics, including obesity, suggests lymphedema and lipedema constitute a residual risk for VTE, and these patients should be carefully targeted for thrombotic risk factor reduction.
Supplemental Material
sj-docx-1-vmj-10.1177_1358863X231219006 – Supplemental material for Venous thromboembolic outcomes in patients with lymphedema and lipedema: An analysis from the National Inpatient Sample
Supplemental material, sj-docx-1-vmj-10.1177_1358863X231219006 for Venous thromboembolic outcomes in patients with lymphedema and lipedema: An analysis from the National Inpatient Sample by Muhammad Umar Khalid, Sameer Prasada, Courtney Jennings, John R Bartholomew, Meghann McCarthy, Deborah A Hornacek, Douglas Joseph, Wei Chen, Graham Schwarz, Rohan Bhandari, Ayman Elbadawi and Scott J Cameron in Vascular Medicine
Footnotes
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
This study is supported by grants from the Lipedema Foundation (#LF31 and R01HL158801) to Scott J. Cameron. The funder had no input in study design or manuscript preparation.
Supplementary material
The supplementary material is available online with the article.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.