
Abstract
Introduction:
This study investigated disparities in health care access for Hispanic adults with diabetes and peripheral artery disease (PAD) who are at risk of lower-extremity amputation and other cardiovascular morbidities and mortalities.
Methods:
We utilized the health care access survey data from the All of Us research program to examine adults (⩾ 18 years) with either diabetes and/or PAD. The primary associations evaluated were: could not afford medical care and delayed getting medical care in the past 12 months. Multivariable logistic regression models were used to assess the association of Hispanic ethnicity and survey responses, adjusting for age, sex, income, health insurance, and employment status.
Results:
Among 24,104 participants, the mean age was 54.9 years and 67% were women. Of these, 8.2% were Hispanic adults. In multivariable analysis, Hispanic adults were more likely to be unable to afford seeing a health care provider, and receiving emergency care, follow-up care, and prescription medications (p < 0.05) than non-Hispanic adults. Furthermore, Hispanic adults were more likely to report being unable to afford medical care due to cost (odds ratios [OR] 1.72, 95% CI 1.50–1.99), more likely to purchase prescription drugs from another country (OR 2.20, 95% CI 1.69–2.86), and more likely to delay getting medical care due to work (OR 1.46, 95% CI 1.22–1.74) and child care (OR 1.80, 95% CI 1.35–2.39) issues than non-Hispanic White adults.
Conclusion:
The Hispanic population with diabetes and PAD faces substantial barriers in health care access, including a higher likelihood of delaying medical care and being unable to afford it.
Keywords
Introduction
Diabetes and peripheral artery disease (PAD) are significant contributors to health burdens globally.1,2 In addition to cardiovascular disease, these two conditions are also major risk factors for lower-limb amputations,3,4 with diabetes alone accounting for 60–70% of the 150,000 nontraumatic minor and major amputations performed annually in the United States (US).5 –7 Recent data suggest that, after a prolonged decline, the rates of lower-extremity amputations are rising among adults with diabetes, with the greatest increase observed in young and middle-aged adults and minority populations.6,8 This highlights the urgent need to identify and address the underlying factors driving this trend, including access to high-quality care, diabetes management, and preventive measures for individuals at risk of developing diabetes-related foot complications and amputations. 9
Disproportionate rates of diabetes and PAD are observed among ethnic minority groups, with extensive research consistently showing an inequitable relationship between these groups and diabetes-related limb loss and cardiovascular disease.10–13 Hispanic adults have 50% higher prevalence of concurrent diabetes and PAD than White adults. 14 A recent study by our group found that individuals identifying as Hispanic with diabetes-related foot problems faced a 33% higher risk of major amputation and a 10% higher risk of minor amputation than White individuals. 13 These disparities are compounded by other health care disparities, including socioeconomic factors and insurance status.15,16 According to the United States Census, individuals identifying as Hispanic comprised 18% of the population in 2017 and they are projected to increase to 26% by 2050. 17 To ensure equitable care for this rapidly growing ethnic group, it is essential to understand the determinants that contribute to disparities in the prevalence and severity of diabetic foot disease, such as severe PAD and foot infection.13,18 These findings indicate potential barriers to early identification and timely medical care to prevent limb loss and cardiovascular morbidity and mortality.
In this study, we aimed to examine the determinants that contribute to delays in accessing medical care and the inability to afford medical care among adults identifying as Hispanics with diabetes and/or PAD and at risk of lower-extremity amputations.
Methods
Data sources
This retrospective cohort study involved participants in the All of Us research program, which is National Institutes of Health (NIH)-sponsored and aims to collect biopsychosocial information from a diverse range of participants in the United States, particularly those from historically underrepresented backgrounds in biomedical research (allofus.nih.gov). As of March 2023, 347,500 participants have completed the initial steps to participate in the program. Over half of the participants come from racial and ethnic minority groups based on self-reported surveys. Available data include participant-provided information, electronic health record data, physical measurements, and biospecimens. Detailed information about the protocol can be found elsewhere. 19
The institutional review board (IRB) at the University of Arizona has approved the use of de-identified data for this study (protocol number: 1907814019). The study followed the Strengthening the Reporting of Observational studies in Epidemiology (STROBE) reporting guidelines. 20
Study populations
We included individuals who were ⩾ 18 years old and had completed the Healthcare Access and Utilization Survey between 2017 to 2023 as part of the All of Us research program. Participants with type 1 or 2 diabetes and/or PAD were identified through the cloud-based environment of the Researcher Workbench. Individuals without information on their race and ethnicity were excluded from the study.
Variables and covariates
Participants were categorized based on their self-reported race (White, Black, Asian, and other) and ethnicity (Hispanic or non-Hispanic) information available in the All of Us database. In addition, sociodemographic, education level, employment, income, housing, and insurance information were also evaluated.
Survey responses
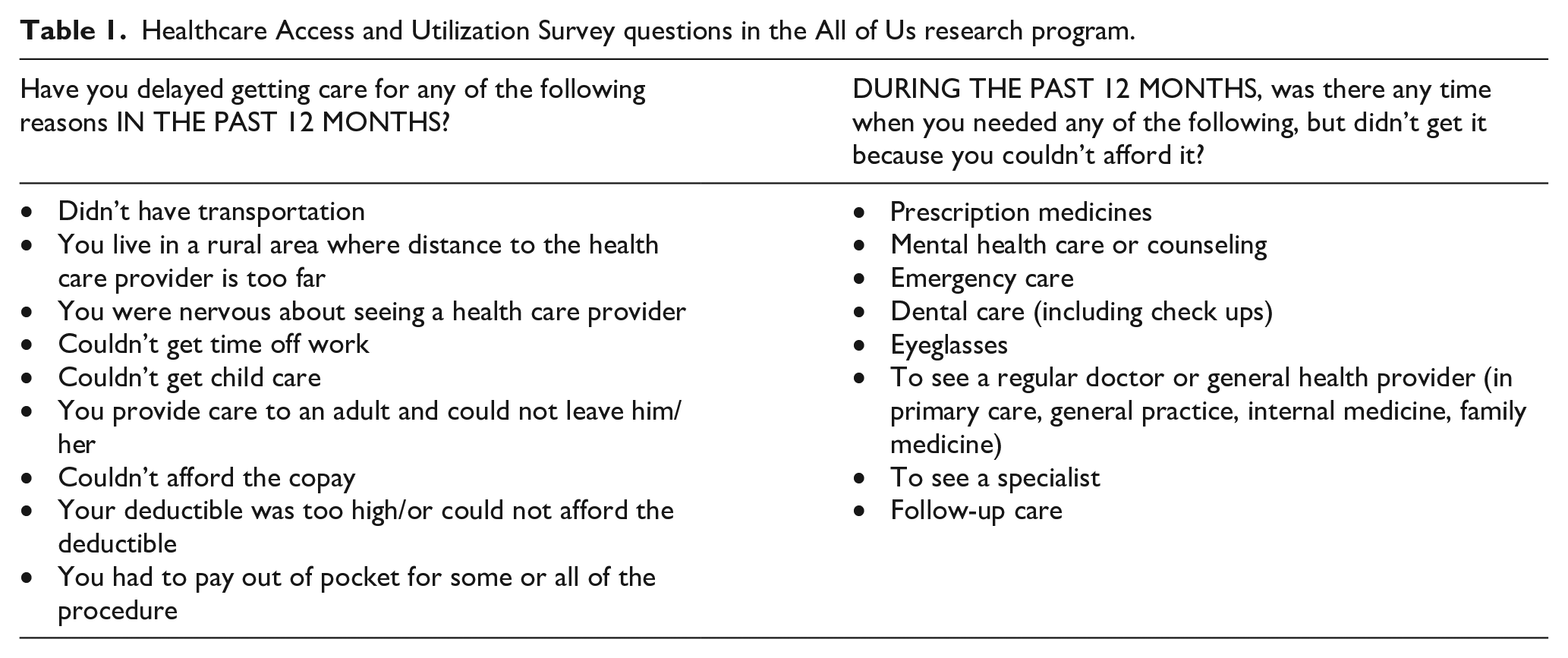
The study evaluated associations based on responses to the Healthcare Access and Utilization Survey, which included two parts (Table 1). The responses were organized into financial versus logistic barriers.
Healthcare Access and Utilization Survey questions in the All of Us research program.
Statistical analysis
Continuous variables were evaluated using Wilcoxon rank sum tests and reported using means and SD, with categorical variables evaluated using chi-squared tests and expressed as counts and percentages. Multivariable logistic regression models were utilized to explore the association with adjustment for age, sex, income, education level, health insurance, and employment status. Odds ratio (OR) and 95% CI were reported to describe the association between ethnicity and survey responses. Adjusted p-values based on the Holm–Bonferroni method were derived to account for multiple comparisons. A multiple-comparison adjusted p-value less than 0.05 was considered statistically significant. The statistical analyses were performed using R (R Foundation for Statistical Computing) and Python (Python Software Foundation) in the cloud-based environment of the Researcher Workbench of the All of Us research program. The initial analysis was performed in June 2022. Updated analyses were conducted in March and June 2023.
Results
Of the 24,104 participants analyzed in the study, 8.2% (n = 1968) identified as Hispanic (17.5% White and 79.8% other) and 22,136 were those identified as non-Hispanic (84.7% White). The mean age of the participants was 54.9 years and 67.1% were women. Of the participants, 52.4% were employed for wages or self-employed and 46.8% (n = 11,293) were not employed. More than 50% (n = 7622) had health insurance sponsored by their employer or union, whereas 25.6% and 10.8% were beneficiaries of Medicare and Medicaid, respectively (Table 2).
Comparison of demographic characteristics between adults who identified as Hispanic and non-Hispanic with diabetes and peripheral artery disease.
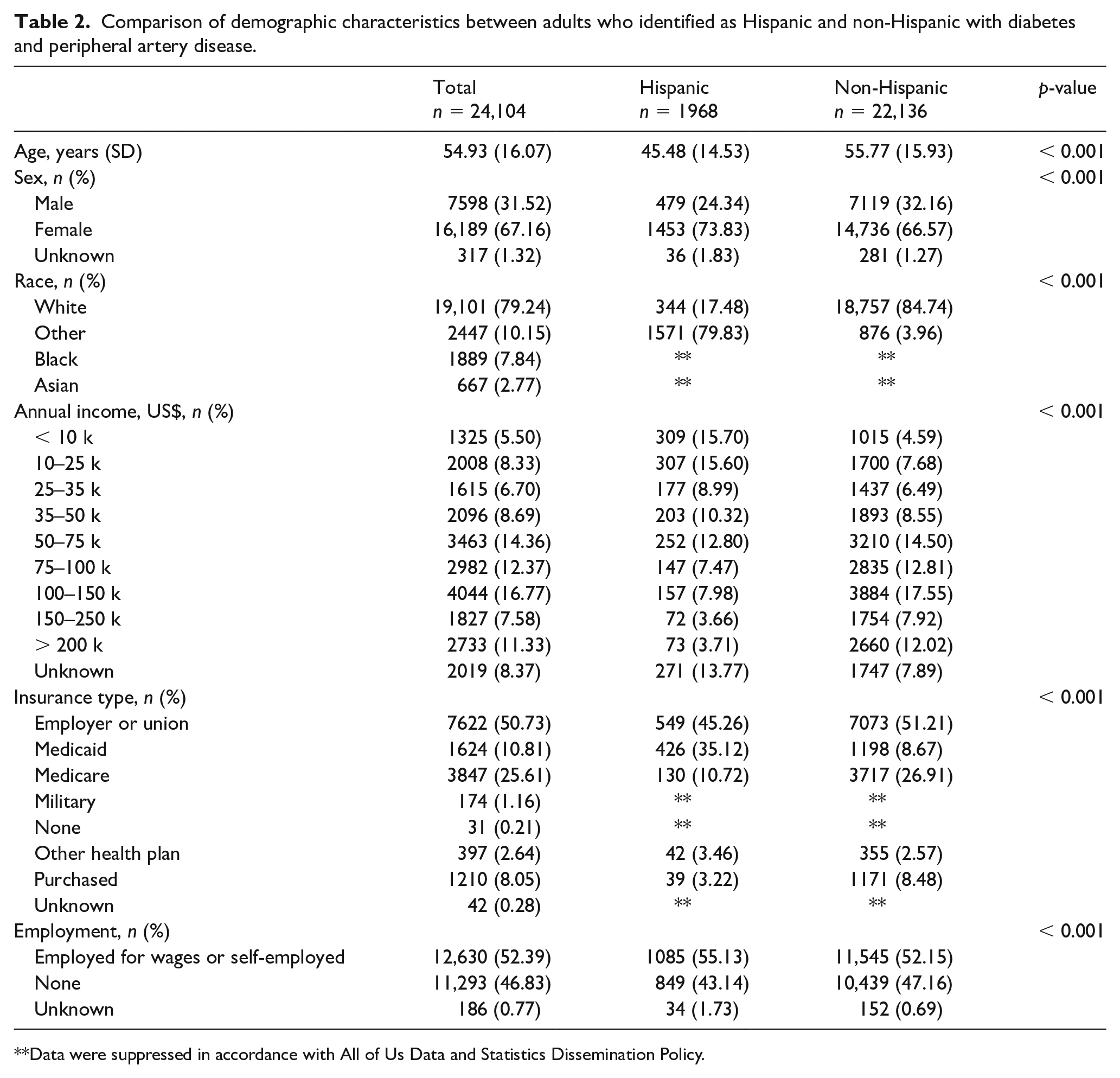
Data were suppressed in accordance with All of Us Data and Statistics Dissemination Policy.
Reasons to delay medical care among Hispanic populations
The result for the univariable analysis is listed in Table 3. The multivariable analysis revealed that Hispanic ethnicity was independently associated with delayed medical care due to issues related to time off work (OR 1.46, 95% CI 1.22–1.74) and child care (OR 1.80, 95% CI 1.35–2.39) when compared to participants who identified as non-Hispanic White (Table 4).
Comparison of reasons to delay medical care and financial barriers to timely medical care among adults with diabetes and peripheral artery disease, categorized by race and ethnicity.
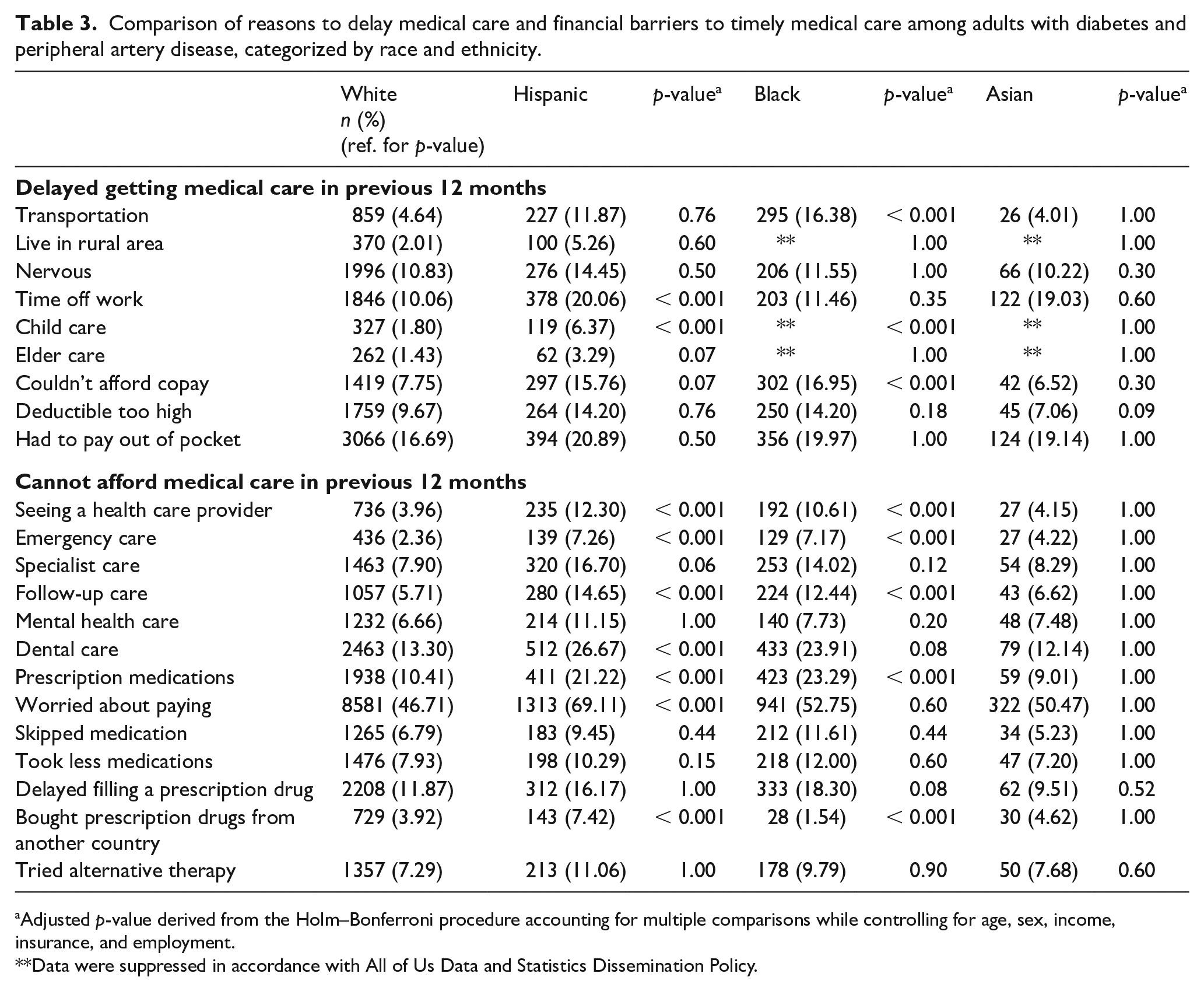
Adjusted p-value derived from the Holm–Bonferroni procedure accounting for multiple comparisons while controlling for age, sex, income, insurance, and employment.
Data were suppressed in accordance with All of Us Data and Statistics Dissemination Policy.
Multivariable analysis examining reasons to delay medical care and financial barriers to timely medical care among adults who identified as Hispanic and non-Hispanic White with diabetes and peripheral artery disease.
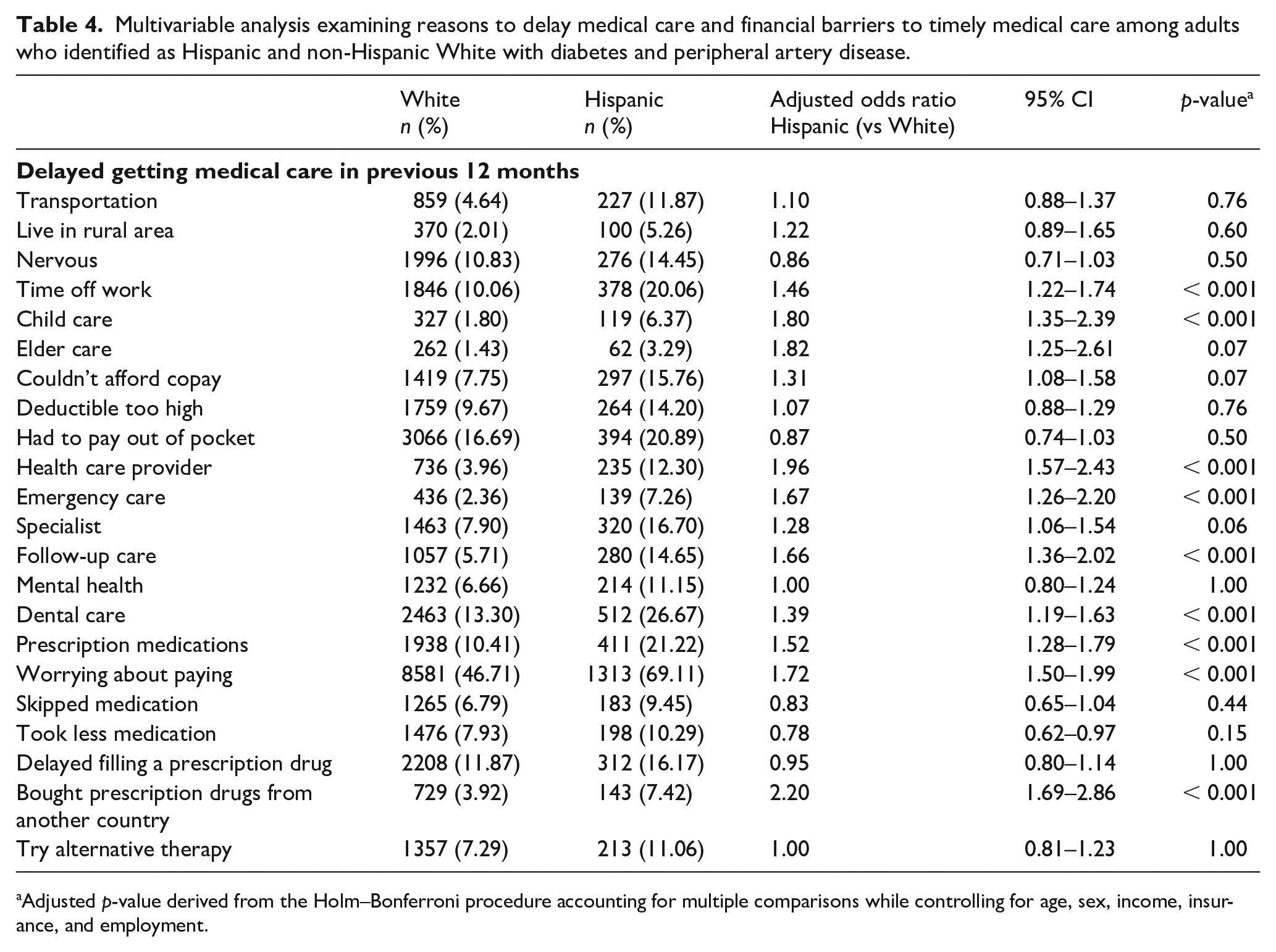
Adjusted p-value derived from the Holm–Bonferroni procedure accounting for multiple comparisons while controlling for age, sex, income, insurance, and employment.
Financial barriers to timely medical care among Hispanic populations
The results for the univariable analysis are listed in Table 3. In the multivariable analysis, participants who identified as Hispanic were significantly less likely to be able to afford to see a health care provider (OR 1.96, 95% CI 1.57–2.43), to receive emergency care (OR 1.67, 95% CI 1.26–2.20), to receive follow-up care (OR 1.66, 95% CI 1.36–2.02), to receive dental care (OR 1.39, 95% CI 1.19–1.63), prescription medications (OR 1.52, 95% CI 1.28–1.79). Those who identified as Hispanic were 1.72 times more likely to report being unable to afford medical care due to cost (OR 1.72, 95% CI 1.50–1.99) and 2.2 times more likely to buy medications from another country (OR 2.20, 95% CI 1.69–2.86) than those who identified as non-Hispanic White (Table 4).
Discussion
Our retrospective study showed that adults identifying as Hispanic with diabetes and/or PAD, the two primary risk factors for lower-extremity amputation and other cardiovascular morbidity and mortality, encounter significant financial challenges, as well as nonfinancial barriers such as transportation, when needing medical care, compared to the non-Hispanic White population. Hispanic individuals were more likely to delay medical care and be unable to afford necessary medical care, even after controlling for health insurance and socioeconomic factors. Early diagnosis, routine follow-up, and access to specialized care are essential for preserving cardiovascular and limb health. The disparities in health care access faced by minority individuals with diabetes and PAD can have significant impacts on health outcomes and increase their risk of limb loss. Interventions and policies must be implemented that focus on the specific needs and barriers of minority populations.
Participants who identified as Hispanic reported a higher likelihood of being unable to afford medical care, including primary care visits, emergency care, follow-up care, dental care, and prescription medications. One of the main contributing issues is inadequate health insurance coverage within Hispanic communities. Despite the implementation of the Affordable Care Act, which aimed to increase health care access for all Americans, individuals identifying as Hispanic continue to have the highest uninsured rates in the US. 21 They are also more likely to have suboptimal insurance with high deductibles, copays, and out-of-pocket costs.22–24 As a result, those identifying as Hispanic with diabetes are significantly less likely to receive indicated foot examinations and undergo revascularization for PAD, elements crucial to limb preservation care.18,25 These inequalities in care extend beyond diabetes and PAD management. Door-to-drug and door-to-balloon times were significantly longer for Hispanic patients than White patients receiving percutaneous coronary interventions for myocardial infarct. 26 Individuals identifying as Hispanic are also more likely to present with more advanced disease and seek care at safety-net facilities.18,27 However, even after adjusting for health insurance status, our study suggests that Hispanic adults are more likely than non-Hispanic White adults to worry about paying for their medical care. In addition to health insurance, other factors related to social determinants of health can also act as a significant barrier to necessary healthcare services.
Our findings regarding individuals identifying as Hispanic delaying necessary care and facing financial barriers to health care access are consistent with previous studies. For example, a large-scale study reported that individuals identifying as Hispanic faced delays in medical care due to various reasons, such as transportation, long wait times, or inconvenient office or clinic hours. 28 The finding that Hispanic participants were more likely to buy prescription medications from other countries outside the US is also supported by other studies, which found that those identifying as Hispanic were more likely to engage in cross-border pharmaceutical purchases.29,30 This behavior can be attributed to several factors, including lower drug prices, limited access to health care providers, and a preference for familiar medications from their country of origin. Furthermore, the financial barriers that individuals identifying as Hispanic face have been well documented by various studies.31,32 These findings have important implications for healthcare policy and practice, as they underscore the need for targeted interventions to address the unique barriers Hispanic communities face in accessing timely and affordable medical care.
Furthermore, the study findings showed that the Hispanic population encountered significant challenges in accessing timely medical care due to various social, economic, and cultural factors. Specifically, individuals who identified as Hispanic were more likely to defer their medical care because of time off work and family caregiving obligations such as child care. This tendency could be partially explained by the Hispanic cultural value of familismo, which emphasizes dedication, commitment, and loyalty to one’s family. 33 Prioritizing the needs of family members over one’s own health needs due to familismo may lead to postponed medical care and subsequent health complications. These results emphasize the significance of taking into account cultural factors when providing and accessing limb preservation care.
The findings of the study provide valuable insight into reducing disparities among minority individuals and at risk of amputation and other cardiovascular disease. The disparities in health care access among individuals with diabetes and PAD in the study can be classified into proximal, intermediate, and distal determinants.9,34 Proximal determinants refer to individual behaviors and decisions that affect health care choices, such as delaying prescription refills and purchasing medications from other countries. One approach is to increase the number of Spanish-speaking health care providers, which can improve patient–provider relationships, chronic disease management, patient satisfaction, and treatment adherence.35,36 Intermediate determinants relate to the immediate social and physical environment that impact health care access, including transportation, work schedules, and caregiving responsibilities. Addressing intermediate determinants, such as transportation difficulties, could help alleviate amputation disparities. 37 Mobile clinics in disadvantaged areas and telemedicine for managing lower-extremity wounds, especially among those with caregiving responsibilities and difficulty taking time off work, can be valuable.37,38 Distal determinants encompass economic barriers and the broader healthcare system, such as affordability issues, copays, deductibles, and out-of-pocket expenses. Addressing distal determinants through health policy is crucial to tackling medical care costs, including prescription medications and preventive services. Expanding insurance coverage and implementing programs to alleviate financial burdens on at-risk individuals could yield significant benefits, as seen with the Affordable Care Act and Medicaid expansion. 39
Study limitations
This study has several limitations that should be taken into consideration. Although we were able to include a large sample size, the data used in this study were self-reported, which could potentially lead to recall and reporting biases. In addition, as our study relied on a convenience sample (the All of Us dataset), it may not represent the broader US population, limiting the generalizability of the findings. Second, a further potential limitation stems from the heterogeneity within the ‘Hispanic’ categorization. The term ‘Hispanic’ encompasses a diverse range of ethnicities, including but not limited to Cubans, Mexicans, and Puerto Ricans, each with unique histories and social determinants of health. This diversity may obscure certain nuanced disparities in health care access and outcomes. In addition, although we are planning on additional analysis (for a future study), we did not account for the interactions between Hispanic ethnicity and income level in this study. Lastly, the study is based on cross-sectional data, which provide a snapshot of the study population at a specific point in time, which complicates the establishment of temporal relationships or causality between variables.
Conclusion
This study highlights significant health care access barriers faced by individuals identifying as Hispanic with diabetes and PAD. These disparities, resulting from financial, behavioral, healthcare system, and policy factors, lead to delays in medical care and difficulties affording necessary care to preserve limb health. Therefore, targeted interventions are needed to address these issues and reduce disparities in limb preservation and cardiovascular care among racial and ethnic minority groups.
Footnotes
Acknowledgements
We gratefully acknowledge All of Us participants for their contributions, without whom this research would not have been possible. We also thank the National Institutes of Health’s All of Us Research Program for making available the participant data examined in this study. Part of this research was presented at the 2021 Vascular Annual Meeting in San Diego, CA, USA.
Correction (June 2024):
This article has been corrected in accordance with the All of Us Data and Statistics Dissemination Policy.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
Tze-Woei Tan is supported by the National Institutes of Health, National Institute of Diabetes and Kidney Disease (NIDDK) Career Development Award (1K23DK122126), and Society for Vascular Surgery (SVS) Foundation Mentored Research Career Development Award.