
Abstract
Black patients have a higher prevalence of peripheral artery disease (PAD) than white patients, and also tend to have a greater extent and severity of disease, and poorer outcomes. The association of race with quality of health (QOH) after peripheral vascular intervention (PVI), however, is less well-known. In our study, we hypothesized that after PVI, black patients experience worse QOH than white patients. We retrospectively assessed racial differences in health status using responses to the Peripheral Arterial Questionnaire (PAQ) at baseline (pre-PVI) and up to 6 months following PVI among 387 patients. We used the PAQ summary score (which includes physical limitation, symptoms, social function and quality of life) as a measure of QOH. We compared QOH scores at baseline and at follow-up after PVI between black (n=132, 34.1%) and white (n=255, 65.9%) patients. We then computed the change in score from baseline to follow-up for each patient (the delta) and compared the median delta between the two groups. Multivariable regression was used to model the delta QOH after controlling for factors associated with race or with the delta QOH. There was no significant difference in mean QOH by race either at baseline (p=0.09) or at follow-up (p=0.45). There was no significant difference in the unadjusted median delta by race (white 25.3 vs black 21.5, p=0.28) and QOH scores improved significantly at follow-up in both groups, albeit the improvement was marginally lower in black compared with white patients after adjustment for baseline confounders (b = −6.6, p=0.05, 95% CI −13.2, −0.11).
Keywords
Introduction
Patients with peripheral artery disease (PAD) generally present with a spectrum of symptoms, ranging from intermittent claudication and leg pain at rest to non-healing ulcers and gangrene. These symptoms are not only associated with significant potential for limb loss but are also associated with decreased functional capacity and poor quality of life (QOL) with significant psychological impact. Thus, the management of PAD aims to decrease the cardiovascular risk, alleviate the symptoms and prevent limb loss with the hope of improving QOL in these patients. The initial treatment options include medical therapy, smoking cessation and supervised exercise programs. 1 Revascularization, either percutaneously or surgically, is recommended for patients who fail conservative treatment or have critical limb ischemia. These therapies are associated with increased maximum walking distance, reduced limb loss and improved QOL.2–6
The prevalence and severity of PAD varies with race, with black patients having the highest prevalence and greater severity of PAD compared with white patients.7–9 Prior studies have shown that given their increased severity of PAD, black patients are more likely to have amputations after peripheral vascular intervention (PVI) and to undergo repeat peripheral intervention compared with white patients.9–12 Thus far, no study has evaluated whether changes in symptoms, physical limitation, social functioning and perceived QOL differ by race after PVI. We hypothesize that post-PVI, black patients were more likely to have higher baseline comorbid conditions and thus worse PAD-related health status than white patients. Accordingly, the goal of this study is to examine the differences in PAD-related health status at baseline and follow-up as well as change in this parameter in both black and white patients undergoing PVI.
Methods
Study population and data collection
The study population consisted of consecutive patients who underwent PVI between 1 January 2012 and 31 December 2012 at St John Hospital and Medical Center in Detroit, Michigan, USA. These data are collected on an ongoing basis as a result of our participation in the multicenter quality improvement registry, BMC2 VIC, which involves 47 hospitals in Michigan. Details of the BMC2 VIC registry have been described elsewhere.13,14 For this analysis, all patients who underwent lower extremity PVI, and whose data were collected in the registry at our single center, were included in this analysis. An on-site registered nurse coordinator collected data on demographic and clinical characteristics, procedural details, treatments and outcomes of patients undergoing PVI procedures. The data were submitted electronically to the registry and a copy of these data was maintained at our institution. Our research nurse coordinators collected data on health status prior to PVI and at follow-up (up to 6 months post-intervention) using the Peripheral Arterial Questionnaire (PAQ). 15 The data on health status were collected for a total of 502 patients. Of those, 115 patients had acute limb ischemia and were excluded from the current analysis. Race was self-reported by patients. Thus, the study population consisted of 387 consecutive patients with PAD who underwent PVI in the time period noted above. A local electronic database was created and PAQ data were entered manually by two physicians (AZ, TM). As a part of participation in the BMC2 VIC registry, data quality and the inclusion of consecutive procedures were ensured by ad hoc queries, random chart reviews and a series of diagnostic routines included in the database. This study was approved by the St John Hospital and Medical Center Institutional Review Board.
Data definitions and endpoints
PVI was defined as endovascular intervention on an artery in the aorto-iliac, femoro-popliteal and below-knee arterial trees using a wide range of interventional devices including stents used at the discretion of the operator.
The PAQ is a PAD-specific tool that assesses the health status of PAD patients over 4 weeks’ duration prior to completing the questionnaire. The PAQ is composed of six domains (symptoms, symptoms stability, treatment satisfaction, physical limitation, social limitation and quality of life). The summary score, as defined by Spertus et al., reflects the average scores of the following domains: physical limitation, symptoms, social limitation and quality of life. 15 For the purpose of our study, the PAQ summary score was used to represent the QOH in our patients. The PAQ is structured to globally evaluate and monitor the health status of PAD patients. The PAQ has been validated against different health status questionnaires in patients with PAD who underwent PVI.4,15 Overall, the PAQ scores range from 0 to 100; higher scores suggest better functional status, better QOL and decreased frequency of symptoms. 15
The primary end point of this study was the change in QOH following PVI between black and white patients (the delta). The change in QOH was described as the difference between the baseline PAQ summary score pre-PVI and up to 6 months post-PVI.
Statistical analysis
Descriptive statistics were calculated to characterize the study group. Continuous variables were described as the mean with standard deviation (SD) or median with range. Categorical variables were described as frequency distributions. Differences in demographic and clinical characteristics by race were assessed using Student’s t-test, the Mann–Whitney U-test and the chi-squared test. Mean and median domain and overall PAQ scores were computed. The differences in scores at each time period (baseline and post-PVI) between white and black patients were assessed using Student’s t-test or the Mann–Whitney U-test (if the data were skewed). The difference in the change in scores (the delta) over time was compared between black and white patients using the Mann–Whitney U-test. Multivariable regression with a stepwise algorithm was used to predict the delta, after controlling for variables that were associated with the delta or with race, on univariate analysis. All data were analyzed using IBM SPSS Statistics for Windows v. 24.0 (IBM Corp., Armonk, NY, USA) and a p-value of 0.05 or less was considered to indicate statistical significance.
Results
Demographics and clinical history
We studied 387 patients: 34.1% (132) were black and 65.9% were white (255). Table 1 shows the differences in demographic and clinical characteristics by race. Black patients were younger than white patients (p=0.001). A greater proportion of black patients were women compared to white patients (62.6% vs 43.1%, p<0.0001). Black patients were more likely to have diabetes mellitus and renal failure requiring dialysis; however, the prevalence of atrial fibrillation was higher in white patients. There was no difference in Rutherford classification between groups. There were also no significant differences in the findings of the ankle–brachial index (ABI), or the anatomic distribution of PAD lesions (above knee, popliteal and below-knee, or above and below-knee) requiring PVI between white and black patients. Of note, data on the ABI were available only in 51.5% of our study population as most patients were referred to our tertiary center for planned PVI after having an ABI performed at an outside facility. Other comorbidities did not differ significantly between the two study groups, including rates of previous vascular procedures (surgical and percutaneous interventions).
Baseline characteristics of the study population.
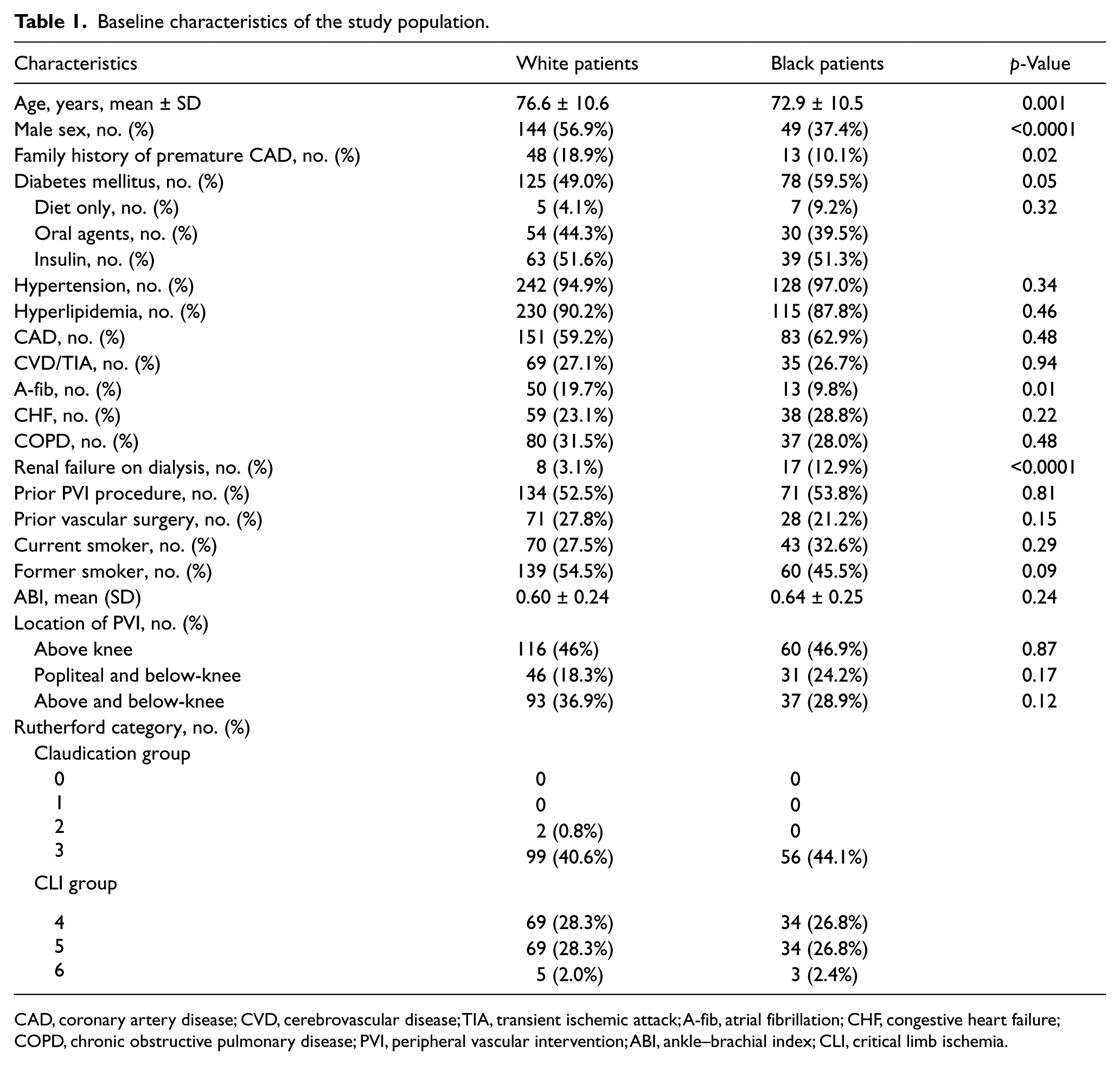
CAD, coronary artery disease; CVD, cerebrovascular disease; TIA, transient ischemic attack; A-fib, atrial fibrillation; CHF, congestive heart failure; COPD, chronic obstructive pulmonary disease; PVI, peripheral vascular intervention; ABI, ankle–brachial index; CLI, critical limb ischemia.
Post-PVI care and medications
Education on the importance of lifestyle modification, such as regular exercise and smoking cessation, was imparted equally in both groups. There was no significant difference in the use of discharged dual anti-platelet therapy, statins, beta-blockers, angiotensin converting enzyme (ACE) inhibitors and angiotensin receptor blockers (ARBs) among groups, as shown in Table 2. Black patients, however, were more likely to receive additional vasodilator medications, including cilostazol, calcium channel blockers (CCBs) and nitrate.
Prescribed medications and education upon discharge.
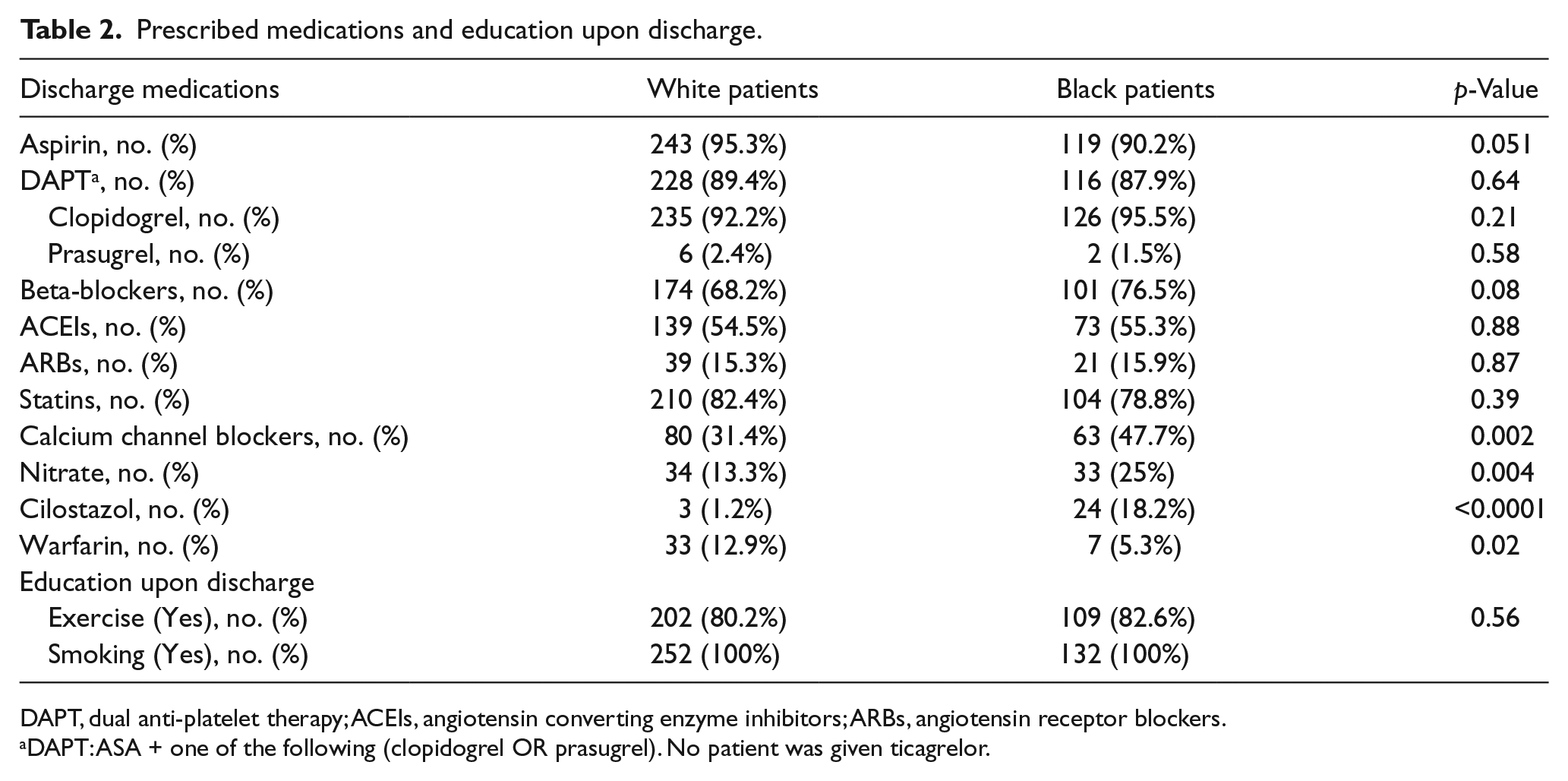
DAPT, dual anti-platelet therapy; ACEIs, angiotensin converting enzyme inhibitors; ARBs, angiotensin receptor blockers.
DAPT: ASA + one of the following (clopidogrel OR prasugrel). No patient was given ticagrelor.
Quality of health following PVI
As shown in Tables 3–5 and Figures 1 and 2, the analyses of PAQ scores showed that both groups had similar baseline scores in all PAQ domains with the exception of a higher mean QOL score in black patients, while white patients had a higher mean satisfaction treatment score. Following PVI, both groups achieved significant improvement in PAQ scores in all domains with similar unadjusted change in scores from baseline (pre-PVI) to follow-up (up to 6 months post-PVI).
PAQ domains and summary score in both groups at baseline.
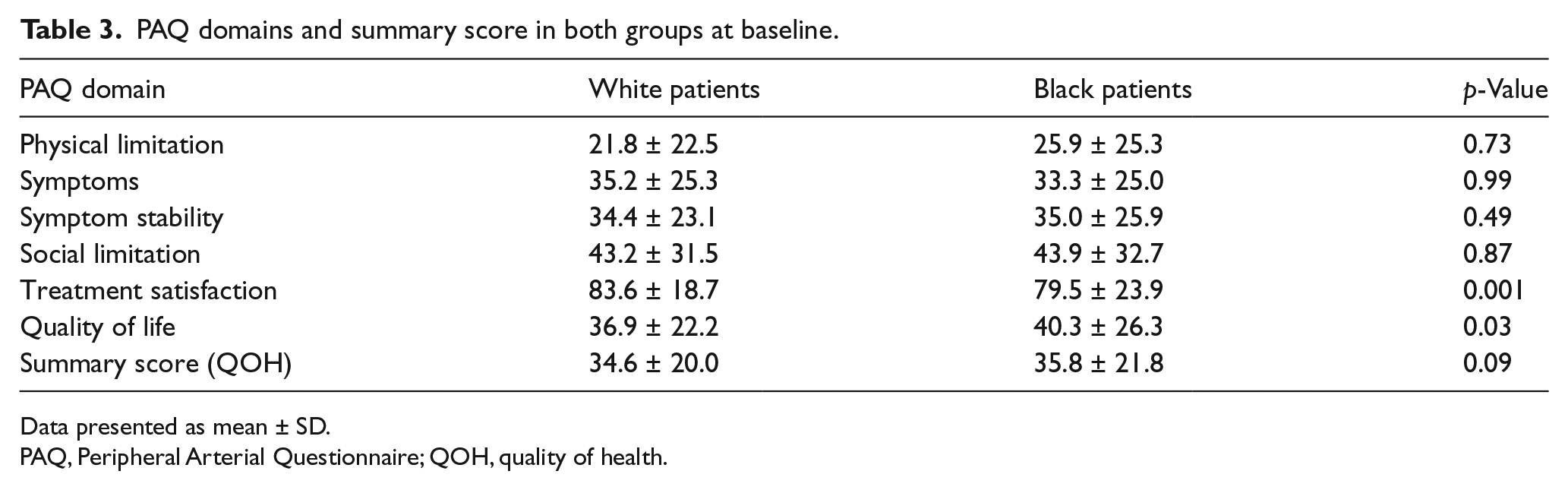
Data presented as mean ± SD.
PAQ, Peripheral Arterial Questionnaire; QOH, quality of health.
PAQ domains and summary score in both groups post-PVI.
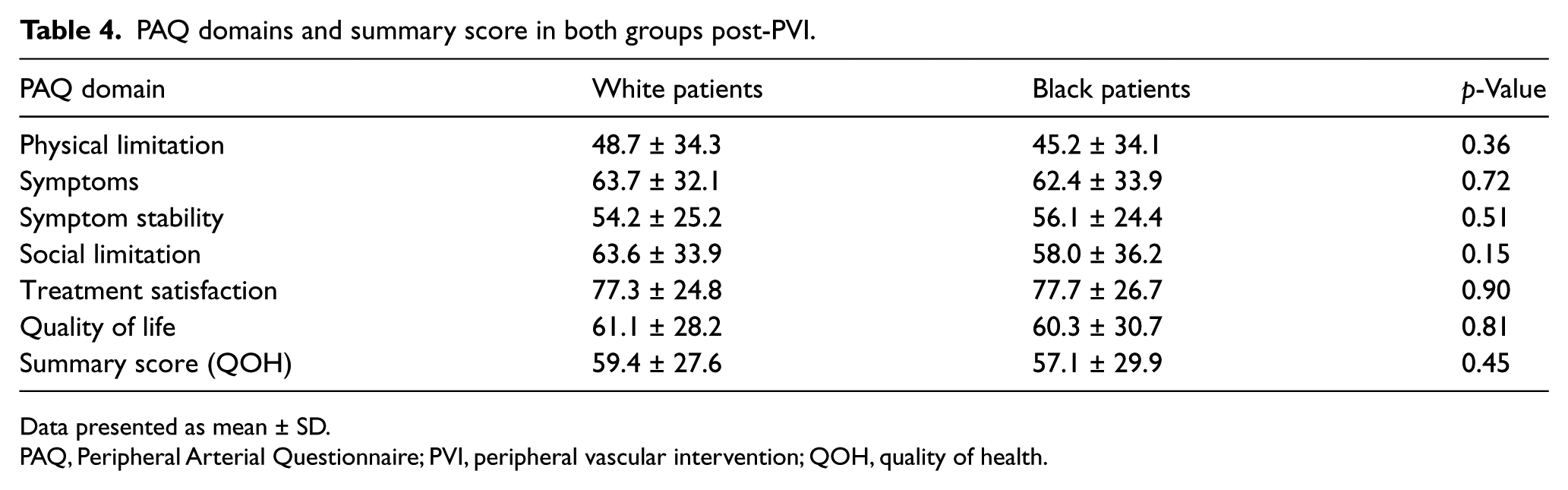
Data presented as mean ± SD.
PAQ, Peripheral Arterial Questionnaire; PVI, peripheral vascular intervention; QOH, quality of health.
Change in PAQ domains and summary scores a .
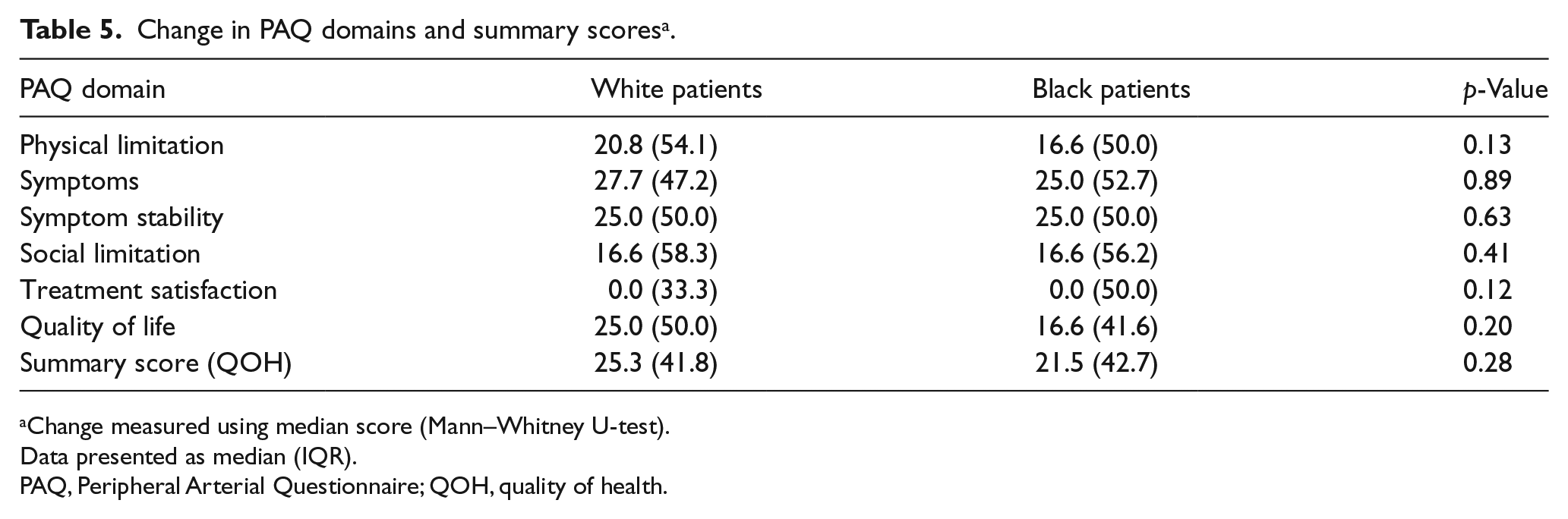
Change measured using median score (Mann–Whitney U-test).
Data presented as median (IQR).
PAQ, Peripheral Arterial Questionnaire; QOH, quality of health.
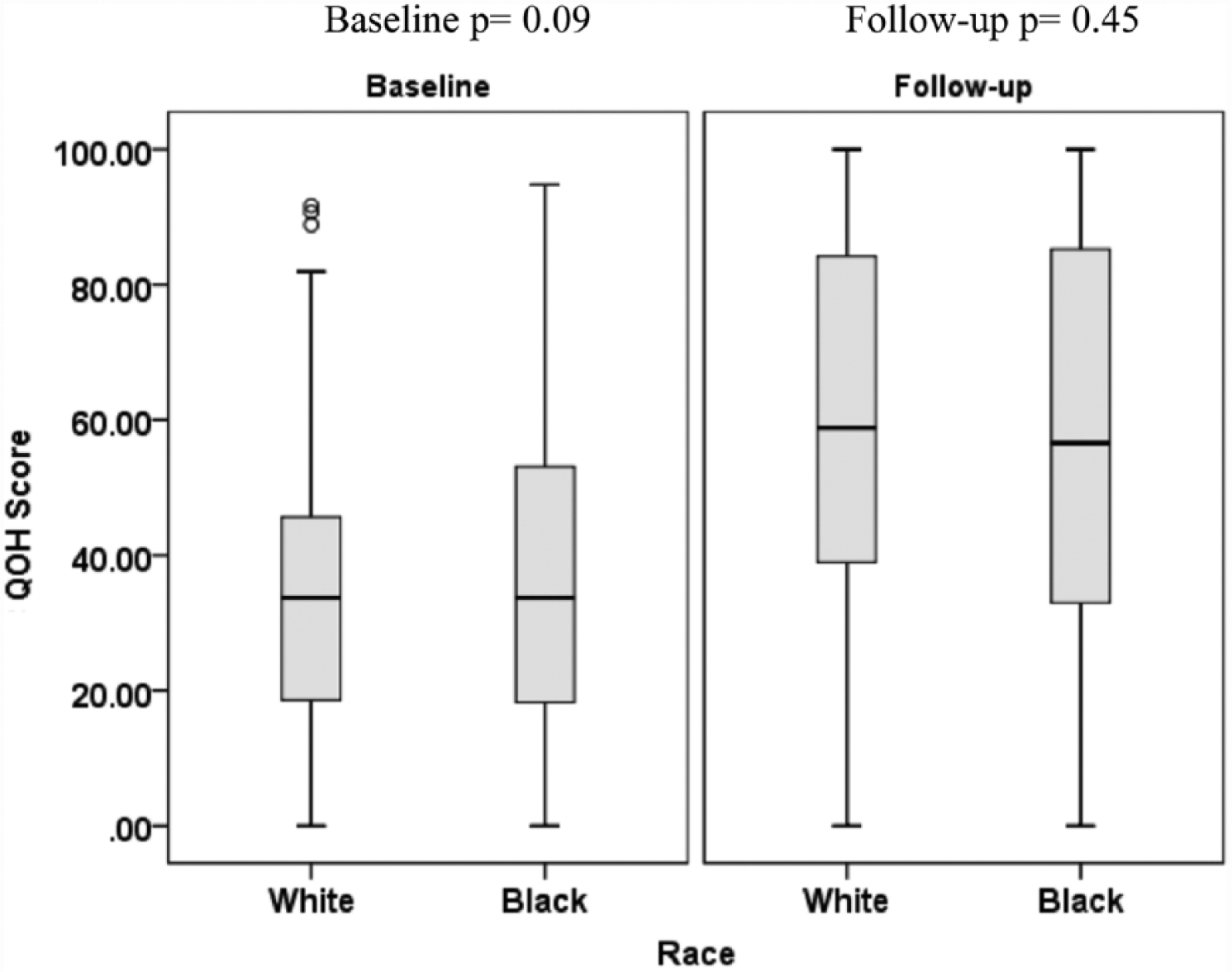
Quality of health (QOH) scores in both groups at baseline and at follow-up.
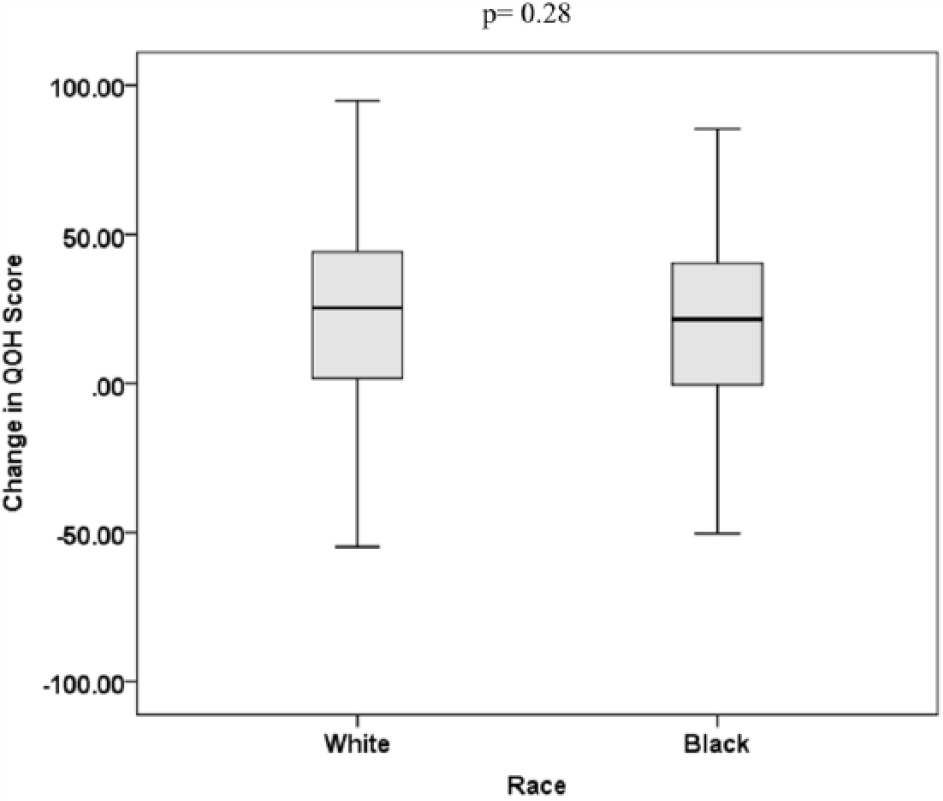
Change in quality of health (QOH) score (unadjusted delta).
Stepwise multivariable regression was used to model the change in QOH from baseline to follow-up, after controlling for variables that were associated with race (age, sex, family history, diabetes mellitus, atrial fibrillation, end-stage renal disease, use of aspirin, CCB, nitrate, cilostazol and warfarin) or associated with the change in QOH (age, current smoker, diabetes, chronic obstructive pulmonary disease, prior PVI, ARBs, Rutherford category including claudication and critical limb ischemia) in univariate analysis. The only factors independently related to change in QOH were age (b = −0.50, p=0.001, 95% confidence interval (CI) −0.78, −0.21) and race (b = −6.6, p=0.05, 95% CI −13.2, −0.11).
Discussion
Our study aimed to assess the differences in the health status (QOH) between black and white patients undergoing PVI using a PAD-specific questionnaire (PAQ). While numerous studies have focused on racial disparities in mortality and morbidity in PAD after revascularization, to our knowledge we are unaware of any prior study that has assessed the racial disparities in health status following PVI.9,16,17 Although in our study cohort black patients undergoing PVI were younger and more likely to be women compared with white patients, they were more likely to have significant comorbid conditions, particularly diabetes and end-stage renal disease requiring dialysis. Prior studies have shown that QOH is likely to be worse among women with PAD compared to men.18,19 Renal disease and dialysis are associated with increased mortality and higher risk for major amputations in patients who underwent PVI. 20 In addition, there was higher use of vasodilators such as cilostazol, nitrates and CCBs in black patients undergoing PVI. Cilostazol, nitrates and CCBs are therapies that have been shown to increase maximal walking and pain-free walking distances in patients with claudication.21–25 Yet, despite this, black patients with PAD undergoing PVI had significant improvement in QOH scores from baseline to follow-up. Given baseline differences in black and white patients, risk adjustment was performed to account for these differences. This analysis revealed that while improvements were seen in both racial groups, the degree of improvement in QOH from baseline to follow-up (delta) was marginally less in black than white patients (b = −6.6, p=0.05, 95% CI −13.2, −0.11). We are unable to provide any definitive explanation of why the QOH scores increased similarly in the two groups despite higher comorbidities in black patients. However, this might be simply due to the fact that both study cohorts had a similar severity of clinical PAD, and, possibly due to that, improved blood flow to an ischemic limb outweighed all other risk factors influencing QOH in the short-term following PVI.
Understanding racial differences in management and outcomes in healthcare is a priority of the US Department of Health and Human Services, as stated in its Healthy People 2010 agenda. 26 These race-related disparities in management and outcomes have been a focus of many studies that have permitted understanding of the ‘gaps’ in the disease, treatment and outcomes between black and white patients with cardiovascular diseases and allowed the application of strategies to minimize these variations. Evaluations of the race-related discrepancies in cardiovascular disease outcomes have focused predominantly on adverse cardiovascular events. 27 Recently, however, assessment of QOL as an important outcome domain has been gaining considerable attention in healthcare outcome evaluation. The assessment of QOL has become a key quality tool in evaluating the efficacy/effectiveness of therapeutic interventions in cardiovascular diseases and has been a routine assessment in many clinical trials and prospective cardiovascular registries designed to understand contemporary practices.28–30 The use of QOL has also been a focus of evaluating inequalities in this outcome domain when studying racial disparities. For example, in patients with coronary artery disease, differences in QOL between black and white patients following percutaneous coronary intervention (PCI) have been studied; these investigations have suggested that after such an intervention black patients have more frequent angina pectoris and worse QOL compared to white patients. 17 There is also growing evidence that invasive treatment is significantly associated with sustained improvement in QOL in patients with PAD.3,4
Our preliminary findings may have some implications. Recent studies have supported PVI procedures, in addition to conservative medical strategies, to improve QOH in patients with persistent intermittent claudication. 3 The current data indicate that despite higher comorbidities, QOH following PVI did improve significantly in black patients, albeit to a marginally lesser degree when compared with white patients. Thus, the presence of higher comorbidities in black patients should not dissuade physicians from offering PVI to them when deemed appropriate. More importantly, the QOH summary scores were in the range of approximately 60%, and even lower in some QOH domains, indicating that there remains significant room for improvement in both groups. Future research should be directed at testing existing and novel strategies to improve not only other outcome domains but also QOH in both groups.
Study limitations
This is a retrospective, observational, single-center study and inference regarding causation should be made with caution. We are unable to account for the influence of missing and unmeasured confounders. Our study findings are applicable to black patients compared with white patients undergoing PVI and should not be extrapolated to other race and ethnic groups, or those managed medically without PVI. We only had intermediate-term data on QOH following PVI. Longer follow-up data may provide a better understanding of the sustainability of these results in both racial groups. No anatomic characteristics of arterial lesions were described or compared between the study groups as these data were not collected as part of the BMC2 VIC database. We only reported and compared the location of PVIs between the study groups. However, anatomic characteristics have not been shown to be predictive of sustained QOH after PVI. 4
Conclusions
Despite the increased comorbidities of diabetes mellitus and renal failure requiring dialysis among black compared to white patients, QOH improved significantly in both groups after PVI. This improvement in QOH was marginally less in black than in white patients. This study highlights the need for strict risk factor controls as early as possible in PAD patients, especially black patients. More importantly, our data identified a significant opportunity irrespective of race for better risk factor controls and to evaluate strategies for improving QOH in patients with PAD. This calls for larger studies in future to test and refine current treatment options and to evaluate novel strategies for improving QOH in different racial and ethnic groups with PAD.
Footnotes
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.