
Abstract
Socio-economic determinants of health (SDoH) include various nonmedical factors in the socio-economic sphere with a potentially significant impact on health outcomes. Their effects manifest through several mediators/moderators (behavioral characteristics, physical environment, psychosocial circumstances, access to care, and biological factors). Various critical covariates (age, gender/sex, race/ethnicity, culture/acculturation, and disability status) also interact. Analyzing the effects of these factors is challenging due to their enormous complexity. Although the significance of SDoH for cardiovascular diseases is well documented, research regarding their impact on peripheral artery disease (PAD) occurrence and care is less well documented. This narrative review explores to what extent SDoH are multifaceted in PAD and how they are associated with its occurrence and care. Additionally, methodological issues that may hamper this effort are addressed. Finally, the most important question, whether this association may contribute to reasonable interventions aimed at SDoH, is analyzed. This endeavor requires attention to the social context, a whole systems approach, multilevel-thinking, and a broader alliance that reaches out to more stakeholders outside the medical sphere. More research is needed to justify the power in this concept to improve PAD-related outcomes like lower extremity amputations. At the present time, some evidence, reasonable consideration, and intuitive reasoning support the implementation of various interventions in SDoH in this field.
Keywords
Introduction
According to the World Health Organization, health is an individual’s physical, mental, and social well-being and ability to pursue different life paths. 1 Consequently, its determinants are not only medical in nature but include nonmedical elements, known as the socio-economic determinants of health (SDoH). These are factors in the places where people live, learn, work, and play that affect a wide range of risks and outcomes related to health and quality of life. In this sense, the socio-economic status (SES) may refer to a construct of income, educational attainment, and employment for either the individual (iSES) or the neighborhood community (nSES). SDoH exert their effect through various mediators/moderators that include behavioral aspects, the physical/built-up environment, access to care, and biological factors.2–5
All these factors can be conceptualized on an individual, interpersonal (family, caregiver), community, and societal level. Critical covariates may show a significant modifying effect on this framework. Age, sex/gender, race/ethnicity, culture/acculturation, and disability status are examples of this.6–10
SDoH represent a unique set of cardiovascular disease (CVD) risks. The association of the risk related to SDoH with different manifestations of coronary and cerebrovascular diseases has been studied extensively.11,12 However, fewer reports exist on this association with peripheral artery disease (PAD).13,14 Nevertheless, as PAD increases worldwide, 15 its consequences will likely raise demand for public health research and service. As an example, the need to reduce lower-limb amputations is worth highlighting. 16
This narrative review aims to explore the role of SDoH in PAD occurrence and care and elucidate how interventions can be implemented to improve PAD care. Methodological challenges are also addressed.
A conceptual framework for the relationship between socio-economic status (SES) and health outcomes
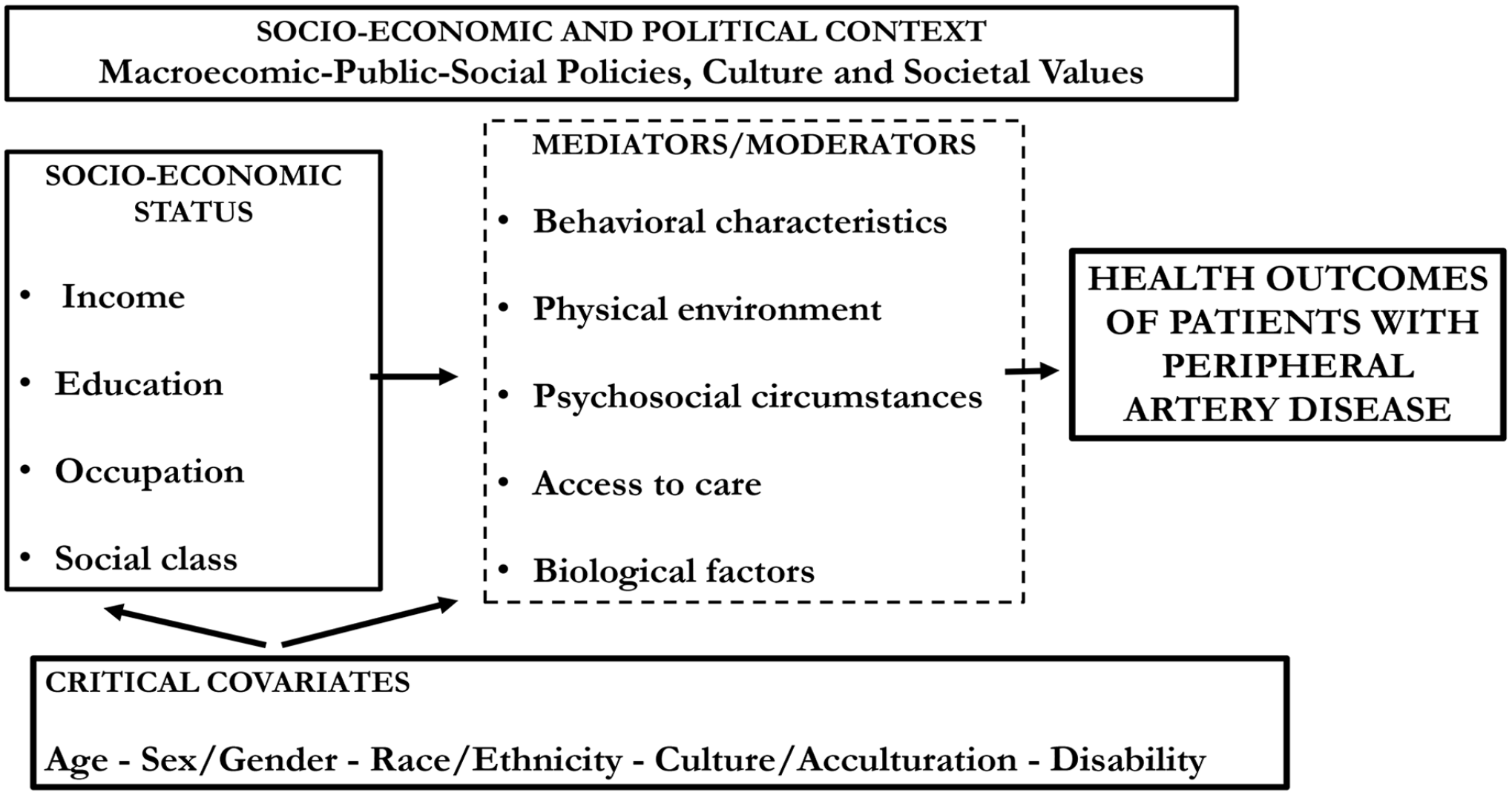
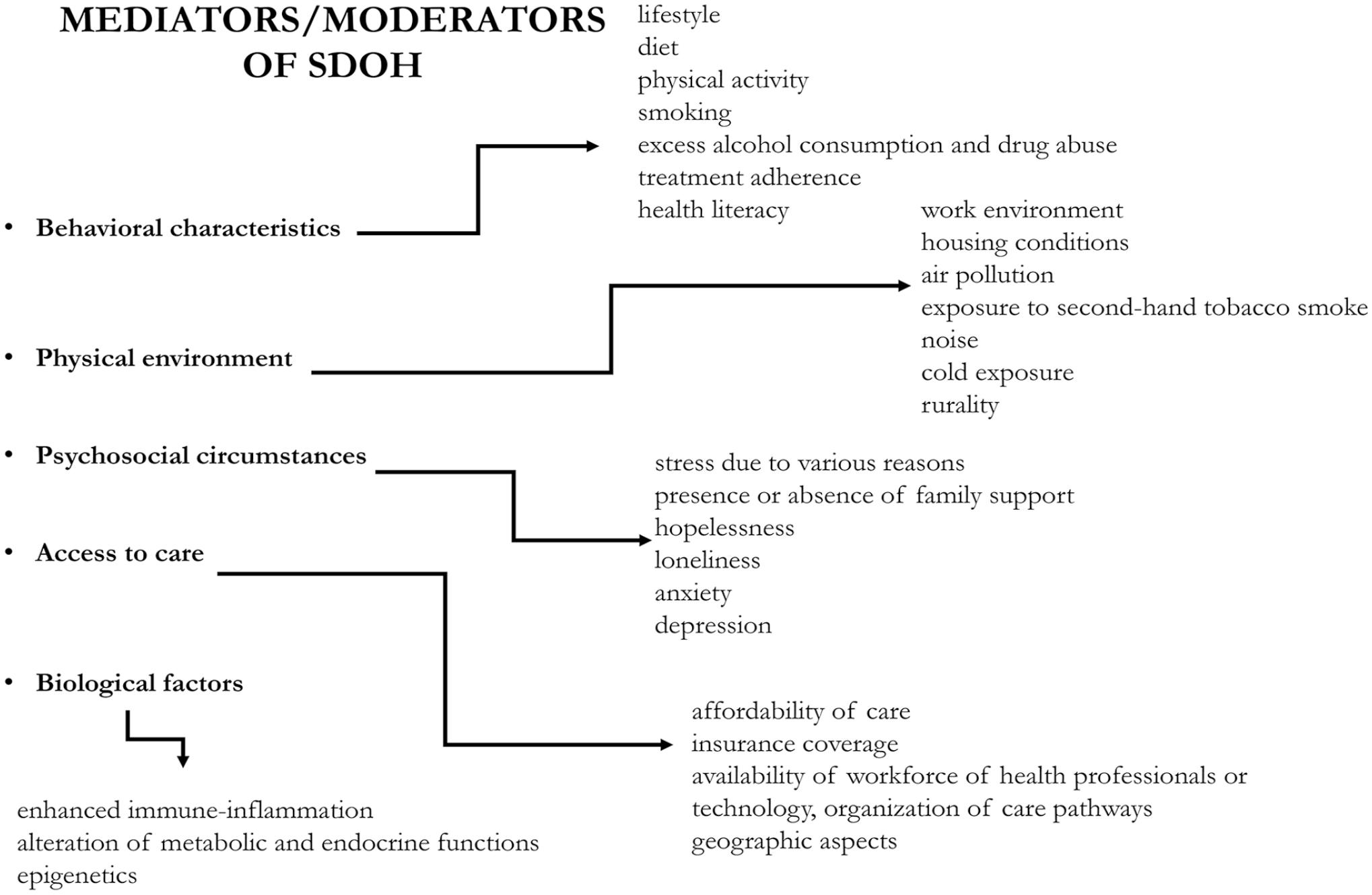
Although several elements of SDoH have been shown to be associated with the occurrence, care, and outcomes of PAD, conceptualizing them in a framework is challenging. The concept is imprecise and not uniformly defined.17–19 In a framework, different social, economic, and political mechanisms representing a socio-economic and political context set the individual’s SES. This latter is stratified according to income, education, occupation, and social class. These elements illustrate the structure of SDoH. These structural determinants are linked to health outcomes by various intermediary determinants (mediators and moderators).9,20,21 Among them, behavioral characteristics (lifestyle, diet, physical activity, smoking, excess alcohol consumption, drug abuse, treatment adherence, health literacy, loneliness, anxiety, and depression) represent the first group.6 –8 The next group is related to the physical environment (work environment, housing conditions, air pollution, exposure to second-hand tobacco smoke, noise, cold exposure, rurality, etc.) to which people are exposed during their life.2 –4 Psychosocial circumstances (stress due to various reasons, presence or absence of family support, hopelessness, loneliness, anxiety, depression) also represent a unique set of factors highly influential on health outcomes. 22 The role of access to care (affordability of care, insurance coverage, availability of a workforce of health professionals or technology, organization of care pathways, geographic aspects, etc.) is of the utmost importance to how SDoH are linked to health outcomes. 23 Additionally, factors mediating between SES and health are not limited to the former aspects. Biological factors (enhanced immune-inflammation, alteration of metabolic and endocrine functions, and epigenetics) may also be involved and may explain how socio-economic exposures affect health.24,25
Critical covariates have a very important impact on health by interacting with SDoH. These are age, race (physical characteristics), and ethnicity (shared common national or cultural backgrounds), 21 gender/sex, 26 culture/acculturation, 27 and disability status. 28 The influence of these factors may be recognized in various forms of structural and intermediary determinants. The complexity of this framework becomes even more complicated if one recognizes that all these elements affect the individuals and the family, the caregiver, the community, and the general population. This concept is illustrated in Figures 1 and 2.
All these elements may also be conceptualized in discrimination, which is considered a socially structured action that is unfair or unjustified and harms individuals and groups. 29 In this sense, structural and individual discrimination incorporates various simultaneous exposure to SDoH and covariates. This view puts a marked emphasis on the societal responsibility to mitigate health disparities. 29
In this framework, which tries to explore SDoH and the health of patients with PAD, several challenges are worth highlighting.
Challenges in studying the role of socio-economic determinants of health (SDoH) on patients with PAD
In contrast to other traditional and nontraditional (primarily biological) risk factors for CVD, SDoH and their critical covariates represent a highly complex set of variables. Lower-limb amputations, as the most feared consequence of PAD, may exemplify the multiple methodological challenges that research will face exploring SDoH.
Difficulties in data acquisition
There is uncertainty about how SDoH data can be ascertained and measured, and the varying definitions of these factors lead to difficulties in comprehension. Research on SDoH needs a multisource data acquisition (administrative databases, surveys, censuses, and registers). The cross-data linkage of disparate data sets (taxation, education, pensions, health, housing, workforce) across time, space, and sources may lead to a new evolutionary schema.30,31 Measuring SDoH based on datasets from different origins is a prerequisite for research. It requires the transformation of data and the formation of different indices. 32 In the case of amputations, which is considered a distal outcome measure of PAD care, the required data compel the researcher to reach out to databases beyond healthcare. 30
Emergency problems in analysis
In the analytic phase, researchers will face several methodological problems. The variables reflecting SDoH are numerous, and, additionally, they are intertwined and interdependent. Consequently, multicollinearity will presumably be present, which represents a severe disadvantage in different regression models that would serve to explore an association between SDoH and health outcomes. As a result, these models may become highly unpredictable and unstable. A remedy for this problem might be to transform multiple explanatory variables into a single construct (e.g., deprivation indexes). However, in doing so—by performing principal component analysis, for example—it becomes difficult and nonintuitive to interpret the single complex construct. Another way to exclude most collinear variables from the analysis (residualization) is to omit all factors but one (e.g., income) that is thought to be most representative. However, this manner of data reduction raises concerns about the robustness of the analysis. 33 Considering amputations, for example, procedure rates are highly associated with the socio-economic parameters; however, these (income, education, employment) show a high degree of multicollinearity. Covariates (e.g., race/ethnicity) are also significant. In this sense, the researcher is forced to work out this problem, as delineated above. 34
The next analytical problem is how to tackle the various interactions between the different SDoH, not forgetting about critical covariates (Figure 1). As an example, SDoH may be interpreted at the level of the individuals at risk (the individual SES, or iSES) and the neighborhood (the neighborhood SES, or nSES) where affected people live. 35 People living in more advantaged neighborhoods show better results regarding many components in the health domain (better subjective health, fewer risk factors, and lower morbidity and mortality rates) compared to those residing in less advantaged neighborhoods. 36 The association of nSES with health metrics is independent of those associated with iSES, but their association is often weaker than for iSES. Factors affecting health in the living environment may include the following: differences and inequalities in access to material resources, the cost burden of available resources, the availability and quality of services, access to medical care, environmental exposures (e.g., air pollution, noise), safety, crowding, and recreational resources. 37 On the one hand, a higher nSES seems associated with better health, but on the other hand, it is not known how iSES strengthens or weakens this association. Several theoretical models (double-jeopardy hypothesis, collective resources model, fundamental cause theory, and relative deprivation hypothesis) were developed to support the comprehension of this complexity. They differ in the particular emphasis placed on understanding the complexity of the relationship between iSES and nSES. 38 When critical covariates are also allowed to interact, the complexity of the analysis becomes even higher. Race/ethnicity/sex/gender/acculturation in a minority community illustrates this situation. 39 Presumably, interactions of these factors determining amputation practice are numerous, and this presents a considerable challenge when trying to untangle them. 16
Additionally, the temporal dependency of the SDoH impact on the risk of developing or worsening PAD also represents an inevitable challenge. A life-course risk is considered as a framework that attends to the way in which a health risk begins and changes over time and how this contributes to the development of diseases. It may relate to a specific period during which exposures shape outcomes that may not manifest for years (the latency/sensitive period model). Examples of this are the ‘transition shock’ in postsocialist Central and Eastern European countries in the early 1990s, 40 or the transgenerational consequences of structural racial discrimination for African American health. 41 Additionally, harmful exposure may exert its influence throughout the whole lifespan (the cumulative exposure model), or early exposure may lead to detrimental exposures in later life (the social trajectory model).42,43 Amputation risk is an excellent example of life-course risk, especially when SDoH and covariates’ impact is analyzed. 16
Trying to interpret the results following analysis, the complexity of SDoH also becomes very clear. The high number of mediators/moderators and the pathways through which SDoH contribute to health represent difficulties in themselves, but proving causality is also challenging. The influence of SES on health is referred to as social causation 44 ; however, the impact of health on SES (health selection or reverse causal pathway) 40 is sometimes not easily separable. Also, an indirect selection—an unknown third factor affecting SES and health 44 —can be part of the interpretation. Although randomization is an essential tool in biomedical research to explore causality, few randomized experiments evaluate the broader interventions and policies that address the SDoH. A range of political, ethical, and practical concerns (lack of feasibility, low generalizability) limit the use of randomized designs to evaluate SDoH interventions. Many times, only quasi-experimental econometric methods remain available to estimate causal impacts. 44 Considering amputations, while in a clinical situation, the unavailability of revascularization procedures seems to be the primary cause of limb loss; at the population level, this association was shown to be much more complicated. Numerous factors may also play a role in amputation rates and spatial patterns. 34
Challenges in actionability
In spite of all these concerns, the primary test of the value of focusing on SDoH is whether it may be efficiently used to improve outcomes by implementing different SDoH-targeted interventions. The evidence base of SDoH is predominantly descriptive, highlighting an association that is only implicitly able to suggest interventions. Solid evidence demonstrating the efficacy of interventions in the socio-economic domain (housing, work environment, education, employment, transport, and access to care) is scarce. 45
Whereas medical interventions act directly ‘downstream’, their impacts are strongly influenced by SDoH determined by the community or societal levels. Thus, looking ‘upstream’ is crucial to identify factors outside the health system and implement specific measures to mitigate the detrimental effect of SDoH.19,46 However, research aiming to collect scientific evidence to prove the contribution of SDoH-targeted interventions to better health will, once more, encounter several methodological difficulties. How to select a realistic and plausible effect size that, together with the sample size, will determine the power of a study? At the same time, even if the effect size of the intervention seems achievable, the question remains of whether it will provide actionable evidence for decision-makers and stakeholders outside healthcare. 47 Implementing interventions in SDoH may entail additional costs and also a potential benefit. However, there are few available data about this aspect.48,49 Additionally, it should be emphasized that many of the SDoH correspond to the core responsibilities of the local authorities, whose budget is limited. Considering how much to spend and how to distribute spending requires a complex economic approach. It may include a sensitivity analysis to provide a sense of the range of costs and benefits over time that could result, an assessment of the economic value of health, and a cost–benefit analysis that also considers benefits from cost reduction, productivity gains, long-term health gains (measured in terms of their monetary value), equity gains (where assessed), and impacts on other sectors, to name just a few. In a broader sense, the social return on investment (SROI), a measure of an intervention’s financial and social impact, plays a decisive role in this context. 49
With the complexity of interventions based on SDoH aimed at decreasing amputation rates, legislative/regulatory and organizational/health system policy change is needed. This effort entails various recommendations. First, however, further research is needed to assess their efficacy. 50
Finally, frequently, the external validity of conclusions drawn from a specific study is questionable. It is often unclear how interventions that were proven effective in a particular environment can be transferred to other conditions. 51 Considering the complex interplay of determinants of amputation practice, they are likely different in high-income and low or middle-income countries. 52
The sources of the methodological challenges in research about SDoH are summarized in Table 1.
Sources of methodological challenges in research about socio-economic determinants of health (SDoH).
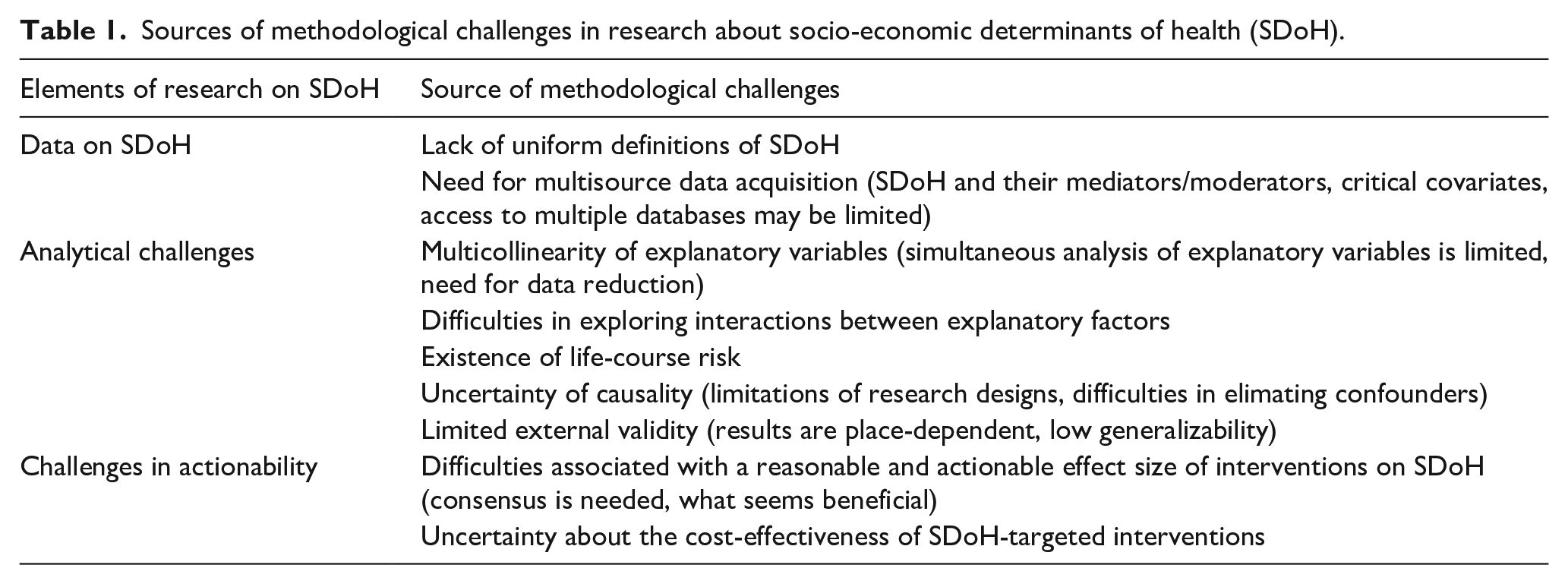
All these methodological difficulties should be considered when exploring how SDoH and critical covariates influence the risk for patients with PAD, including the odds for lower-limb amputations.
Impact of SDoHs on patients with PAD
SES and PAD occurrence
Increasing evidence signals that lower SES is associated with PAD occurrence. Based on data from the National Health and Nutrition Examination Survey (NHANES), using a representative sample of adults in the US from 1999 to 2004, a low individual poverty-to-income ratio (PIR), which compares income to a poverty threshold, entailed higher PAD incidence. The difference in risk between the lowest and the highest category of PIR was significant (OR 2.69, 95% CI 1.8–4.0) and remained so even after adjustment for demographics, education level, and cardiovascular risk factors (OR 1.64, 95% CI 1.04–2.6). Attained education level was also associated with PAD occurrence, and this finding remained significant after adjustment for demographics (OR 1.87, 95% CI 1.26–2.78). However, in a fully adjusted multivariate model, this association was no longer significant. Similar results were shown in the Heinz Nixdorf Recall Study from Germany, which demonstrated higher PAD occurrence in individuals with a low iSES. 53 The Atherosclerosis Risk in Communities Study attempted to explore the association between the iSES (defined by income and educational attainment), the nSES (area deprivation index), and the incidence of hospitalization with PAD. In a study of more than 12,000 middle-aged US adults with a median follow-up of 23.6 years, the risk for hospitalization with PAD was assessed using a Cox proportional hazards regression model. The demographically adjusted hazard ratio was 2.42 (1.81–3.23) for low household income, 2.08 (1.60–2.69) for low educational attainment, and 2.18 (1.35–3.53) for the most deprived neighborhoods compared to their high-SES counterparts. After adjustment for traditional cardiovascular risk factors and healthcare access, the associations were attenuated but remained significant, particularly for income and education. Results were consistent when stratified by race. 54
The association between PAD occurrence and SES was also demonstrated in subgroups at the highest risk for PAD, like patients with diabetes and chronic renal failure.55,56 PAD presentation had the highest association with SES, compared with other cardiovascular diseases (5.5 median years’ follow-up of 114,859 people). 57 In addition to PAD occurrence, the association of SES with a more advanced presentation of PAD was also demonstrated. Unemployment, socio-economic disadvantage, and rurality entailed disease presentation with gangrenous ulcers or a need for emergency surgery, in contrast to elective procedures. 58 This is evidently related to the fact that low SES entails late recognition of PAD, even when other cardiovascular conditions have been identified and are being treated. 59 The onset time of PAD was also related to SES (high unemployment rate, low education, small cities area). 60 Another aspect of SES, environmental pollution, was also associated with higher PAD prevalence. Specifically, particulate matter 10 (PM10) in the air was proven to be related worldwide. 61
Considering the critical covariates, race/ethnicity was proven to be influential in PAD prevalence. The disproportionate affection of Black Americans with PAD exemplifies this. 39 This multifactorial phenomenon is highlighted in research that revealed PAD occurrence is different in ethnic minorities living in a foreign environment compared to the same ethnic group in the motherland. 62 Though ageing is strongly associated with a higher occurrence of PAD, women and men are similarly affected. 63
SES and PAD care
SES is also related to disparities in the care of PAD (lifestyle modifications, medical treatment, invasive procedures, rehabilitation).
Lifestyle
Smoking represents one of the most important modifiable risk factors for PAD. Low SES is associated with a higher prevalence of smoking and more pronounced exposure to tobacco. According to the results of studies that attempted to assess tobacco exposure objectively (via measurement of nicotine concentration), cigarette smoking affects the poor twice as hard. They are not only more likely to smoke (and, if they do, to smoke more cigarettes per day), but they also appear to smoke each cigarette more heavily and extract more nicotine (and therefore tar) per cigarette. 64 Smoking uptake is also highly dependent on SES (via parental modeling, peer pressure, access to tobacco, lower awareness and underestimation of tobacco’s harm, behavior problems, and poorer educational performance). 64 Evidence supports the observation that smoking cessation is less likely to succeed in patients with lower SES, even with access to cessation programs. Markers associated with poor success in quitting include low educational attainment, financial disadvantage, early habit uptake, preference for cheaper cigarette brands and hand-rolled tobacco, greater exposure to stress, psychological differences, and tobacco company targeting. The social gradient in quitting was also demonstrated during pregnancy.
An abundance of evidence can be found about the role of nutrition in the development/progression of PAD. Additionally, it was shown that dietary patterns and eating habits are associated with SDoH. Low SES may hamper the access and adherence to a healthy diet (Mediterranean diet). Although data on PAD and eating disorders (emotional eating and binge eating) is lacking, its association with PAD occurrence may also be assumed. 65
The regular and supervised training programs that have been highly effective in many PAD patients 66 show limited value with low SES individuals. Low awareness of their benefits, low educational levels, and logistical obstacles are the main reasons for failure.67,68
Race/ethnicity, as an important covariate, is also shown to interact with lifestyle. The lower rate of successful smoking cessation in Black Americans was thought to be associated with the lack of home ownership, lower income, and more neighborhood problems. 69 A similar association (smoking habit and SES) was detected in the Roma population in Europe. 70
Medical treatment
Regarding medical treatment, it has been demonstrated that the lower rate of utilization of drug therapy was impacted by uninsurance 71 and low nSES. 72 Patients with PAD from the lowest versus the highest income quintiles were less likely to be on statin (72.5% vs 85.8%; relative risk [RR] 0.84, 95% CI 0.83–0.86; p < 0.001) or antiplatelet (79.0% vs 84.6%; RR 0.93, 95% CI 0.91–0.94; p < 0.001) therapy. This relationship was attenuated when adjusted for the practice site. This suggests that, as regards access to care, the quality of the local service has a decisive influence on PAD care. It may also lead to a paradoxical situation, as was shown in Germany. Though PAD occurrence was higher in low-income areas, the proportion of patients on guideline-recommended pharmacotherapy was also higher in these areas compared to high-income areas. This was because, in high-income areas, vascular surgery outpatient clinics provided the care, whereas in lower-income areas, angiology outpatient clinics predominated. 73 This kind of disparity in access to care, leading to a lack of optimized medication, was also reported in Canada. 13 SES also influences medication adherence. Based on the results of nine studies, low SES was associated with lower adherence to statin therapy. 74 Presumably, these findings may be applied to the PAD population as well.
Critical covariates like race/ethnicity are also influential. Hispanic/Latino individuals with PAD were proven to underuse cardiovascular medications that were recommended in the guidelines. 75 Women also seem more vulnerable in this regard. They were less likely to receive guideline-recommended high-intensity statins or any statin prescription compared with men. In addition, the female sex was associated with lower adherence to statin therapy. 14
Lower extremity revascularization
A social gradient is also discernible when examining the different outcomes of vascular procedures in patients with PAD. Following lower-limb endovascular procedures, low SES was associated with worse postoperative cardiac problems, postoperative limb ischemia, and unplanned admission to higher levels of care, even after adjustment for demographics, comorbidity, Fontaine stages, and medication. The risk of adverse outcomes was twofold in patients from the most deprived areas. 76
The most comprehensive summary of this issue was a recent meta analysis, based on 11 observational studies and randomized controlled trials evaluating the impact of SES on presentation severity or outcomes for patients undergoing lower extremity bypass or angioplasty. The data from 1,470,381 patients demonstrated that lower SES is associated with more severe disease presentation in the form of critical limb ischemia and higher rates of postoperative amputation after revascularization. 77
Similarly, patients with low nSES showed higher rates of major adverse limb events (revisions, thrombectomy) and hospital readmissions following lower-limb bypass surgery.78,79 This association was also shown for surgical site infection in poorer households. 80 In addition to SDoH, the critical covariates also influenced the outcomes of vascular procedures. This was demonstrated for race/ethnicity 81 and sex/gender 82 across various vascular surgery presentations.
Lower extremity amputations/rehabilitation
The most intensively studied aspect of PAD care and its relation to SES was an estimation of the odds for a given patient to undergo lower extremity amputation instead of treatment to prevent limb loss (such as revascularization). Amputation represents a complex distal outcome measure of PAD care. However, in addition to aspects of the medical service, amputation is also determined by the demographics, comorbidity patterns, and socio-economic characteristics of patients and their living environment. 16 Low iSES was associated with a more unfavorable vascular risk profile in lower-limb amputees and a higher predisposition for major amputation.83–85 Low nSES also increased the odds of having major lower-limb amputations.34,86 Although iSES seems to play the more decisive role, a geostatistical model considering only the neighborhood revealed that nSES represented the predominant impact on amputation rate; the effect of healthcare service disparities was less influential, and 37% of the variability in amputation practice could be attributed to the living environment of amputees. 34 The socio-economic gradients in amputation rates may also exist when comparing different countries. A striking difference in amputation rates across Europe is an example of the East/West divide in health 87 that may be partly accounted for by the complex disparities found in socio-economic characteristics of Western European and Central and Eastern European countries. 88
Critical covariates were also shown to interact with amputation risk. In a metanalysis, men and non-Caucasians showed higher risk. 85 Black and Hispanic patients undergoing infrainguinal revascularization for chronic limb-threatening ischemia and claudication had worse limb outcomes (amputation) compared with White patients, even with similar disease severity at presentation. 89
Following amputation, affected patients will face diminished community reintegration with reduced self-perceived health and well-being. 90 Adaptation to prostheses was related to educational attainment. 91 Financial difficulty was a significant predictor for diminished work or daily activity participation due to physical and emotional stress. Consequently, a low iSES may hamper the complex course of rehabilitation. 90 Minorities, defined by race/ethnicity, were again shown to be disadvantaged. Higher-level amputations entail increased energy costs for mobility, increased rehabilitation needs, decreased use of and satisfaction with a prosthesis, biomechanical disadvantage, and a greater financial burden. Amputation level was a particular disadvantage for Black individuals and women.92,93
Potential interventions targeting SES in patients with PAD
Although evidence for the association between SES and PAD is accumulating, it seems less available than for other cardiovascular diseases, and there are very few data on the potential benefits of tailored interventions. The lack of data is likely related to the methodological challenges that were highlighted before (Table 1). The difficulty in demonstrating a reasonable and actionable effect size, determination of cost-effectiveness, limited, population-dependent effectiveness, and a need for a more extended period to assess impacts are some of the obstacles that are to be overcome by any research on interventions in SDoH.
The very first question is: what are the relevant items that may serve as a target for interventions aimed at SDoH in PAD? This means that we have to focus on the mediators/moderators that connect SDoH with PAD outcomes. Some research data are available; however, more often, opinions are based on reasonable consideration.
The first group of potential items corresponds to behavioral characteristics. The individual’s values and preferences are unquestionably crucial in treatment decisions. It has been demonstrated that a great majority of patients prefer a shared or autonomous role in the treatment process. However, decision-support tools can also be used to meet the needs of patients who want to be engaged, and to educate and invite patients to transition from a more passive role to a more engaged one.94,95 Social support by family members, close relatives, nurses, and caregivers may have an impact on disease acceptance and cooperation; it may give individuals the sense that they are cared for. 96 For example, good social support may contribute to better recovery following bypass surgery in PAD patients. 97 In addition, social support can help mitigate the depressive symptoms that are prevalent in patients with PAD. 98 Socially isolated, lonely patients following amputation are especially vulnerable. In these cases, social network support or psychotherapy may be pivotal in the adaption process. 99
In addition to social support, increased understanding of PAD may also have benefits at the individual or community level. The deficit in awareness and the lack of information on PAD in the general public, compared to stroke and myocardial infarction, represents a significant barrier to care. Enhancing PAD awareness by implementing community campaigns bears consideration. 100 Although there is agreement about the importance of patient education, the limited studies on the value of structured education for increasing physical activity are inconclusive. Social support can foster information-seeking behavior and effective educational programs for PAD.101,102 There is a need for more rigorous scientific research with better criteria for structured programs and consideration of patients’ experiences and perceptions. 103
Health literacy, defined as an individual’s capacity to access and use health-related information to promote and maintain good health, represents an important challenge in educating and communicating with patients with PAD. 104 As a mediator between education and healthcare utilization, health literacy is a highly complex characteristic. For example, it does not reflect overall literacy in every case and may also involve the role of patients’ relatives and caregivers. 105 Low health literacy related to higher age and low educational attainment has been demonstrated in the PAD population. 106 Some research claimed benefits from interventions to improve PAD knowledge among the public; however, this educational program had only a marginal effect compared to no intervention. 107
Healthy eating, another behavioral characteristic, was addressed in a multilevel, community-engaged food environment intervention that was intended to improve access to healthy food in two neighborhoods, both of which were food swamps (i.e., places where there are a disproportionate amount of unhealthy food venues and choices). The project involved multiple stakeholders and intervention targets, including neighborhood residents, business owners, local politicians, high-school students, community clinics, community-based organizations, and law enforcement officials. However, the effect of all these interventions was weak. 108
Similar multilevel, community-based interventions (community mobilization, structural change, health education, and social marketing) were used against smoking, resulting in a significant beneficial change. 109 Additionally, preventive interventions, such as increased cost of tobacco products, may be more effective for people with lower SES. 64
Beyond the behavioral aspects, the physical environment also represents a source of potential adverse outcomes in PAD. In this regard, regional air pollution (especially particulate matter) seems to matter. Second-hand smoke (passive smoking) was also proven to influence PAD occurrence. 110 Changing the physical environment may be an option for improving PAD outcomes; however, no specific scientific results are available in this regard.
Access to care likely represents an important area in which benefits from interventions can be expected. However, affected patients have to be detected. A crucial element for reaching out to patients with PAD is screening 111 in the community. An appropriate step in this scheme is to find the most vulnerable subgroup of patients at risk of late detection of PAD. For this, critical covariates are very important. Homeless and older people face several unique challenges (social isolation, loneliness, physical inactivity/overstrain by walking, inappropriate footwear, poor foot hygiene, masked PAD, etc.) that influence PAD risk and late recognition.112,113 Racial/ethnic minorities also represent a special subgroup of patients who are exposed to marked risks in PAD occurrence, presentation, management, and outcomes. 39 In addition to identifying these vulnerable subgroups, a tailored approach to planning interventions in SDoH would be beneficial.
Another aspect that influences access to care is rurality, which may be solved by tailored patient transportation support. 114 A crucial element of regional care organization is to plan and design patient referral pathways to multidisciplinary teams. In this process, there may be an opportunity for community services to become more proactive; for example, the creation of a PAD screening service run by a nurse leader with a group of trained healthcare assistants, 115 or the development of a podiatry-led integrated pathway for patients with leg symptoms. 116 In general, social prescribing, as a way of linking patients with sources of support within the community, is a promising approach; however, studies exploring its efficiency fail to provide sufficient detail to judge either success or financial efficiency. The potential of nonmedical referral options that can operate alongside existing treatments to improve health and well-being needs further research. 117
Although scientific data, reasonable considerations, and intuitive reasoning support the potential benefit of interventions in SDoH and their set of moderator/mediators, the quality of the evidence to date falls far short of the scientific criteria that we would expect in evidence-based medical interventions. 41 However, there are some principles of interventions that can be highlighted.
Principles to consider when planning interventions in SDoH to improve PAD outcomes
Accepting the difficulties, for efficient interventions in SDoH to improve PAD-related outcomes, a systems approach is needed. Focus on the whole system rather than focusing exclusively on individual components is required. 118 ‘Swimming upstream’ means returning to the root of a health problem. Upstream determinants of health reside at the economic and political levels, where decisions are made that influence public health. 119 This endeavor entails the implementation of complex regulatory and legislative health system policies to address SDoH. 120
An enormous array of SDoH may potentially influence PAD outcomes. Interventions may be achieved by increasing expenditure on health, assuring medical insurance coverage, diminishing gradients in income and wealth, providing high-quality education to a wider population, improving work conditions, and decreasing the detrimental effects of the physical environment. Policy changes can focus on different targets, such as regulating smoking, promoting health literacy and awareness of PAD (media coverage, inclusion in school curricula), developing and supporting PAD-specific health services, facilitating the accessibility of PAD-specific health technology, and supporting research and development related to PAD. However, tailored solutions or interventions are of utmost importance. In jurisdictions where basic healthcare is unavailable for most of the population, the most appropriate intervention is to raise awareness and elevate care provision. Where the care exists, but access to it is a barrier, low SES (poverty, social exclusion), many times combined with race/ethnicity, become the major drivers of inequality. In this case, structural changes are needed to overcome these barriers. Finally, in jurisdictions where access to healthcare is available to all, health literacy and education may become a high priority. For this, the social history of patients and family and a better understanding of the broader context of the socio-economic environment of the patient is imperative. 13
In order to intervene more efficiently, it is reasonable to propose bundled policies instead of separating the ones that are politically acceptable. In this sense, multilevel interventions are more beneficial, even if the research methodology for this kind of study is underdeveloped. 108 Many times, SDoH fall under the remit of different ministries, which seriously hinders the possibility of coordinated actions. Involvement of more institutional systems, that entails the constraints of previous paths in decision making (path dependency), institutional inertia, and the rigidity of the structure of political decision-making, represents a challenge for implementing SDoH-based interventions.121,122
This complexity requires action that is not limited to the treating physicians or patients but that involves much broader societal collaboration. Success assumes a wide collaboration of stakeholders who are not exclusively engaged in health or the social sphere. They are politicians, government people, industry representatives, media workers, scientists, etc.
Though there is a potential to influence politics more broadly to improve PAD outcomes, this effort compels the representatives of the medical profession and science to communicate with policy makers, media representatives, lay audience, and other public stakeholders. This communication is fundamentally different from discussions among medical professionals. Communicating ‘politicized’ science, especially when the mass media have an overwhelming role in determining which issues come to public attention, represents a dilemma for scientists who are engaged in research. They must be conscious of factors that influence the success or failure of incorporating socio-economic aspects. Some of the challenges that may affect the effort to address SDoH at this level include the varying roles scientists can play in providing scientific inputs, the different levels of information and perceptions of risk among the public, and countervailing forces of other stakeholders. 123
These principles represent the basis of the VAS International PAD Strategic Network with its campaign ‘No More Vascular Amputations!’, 16 which is in harmony with the effort that was summarized in the recent American Heart Association Statement on its amputation reduction policy. 50
The ‘Health in All Policies’ approach in Finland, implemented in the 1970s, exemplifies how public health can be supported by interventions through acting on determinants beyond the health sector. Significant improvements in outcomes highlight the importance of this effort. 124 A similar policy against PAD would be beneficial.
However, the very first step that would be beneficial here is to conduct more research that aims to explore the different aspects of the role of SDoH, their mediators/moderators, and the critical covariates in the care of PAD. The potential and principles of interventions of this kind are illustrated in Figure 3.
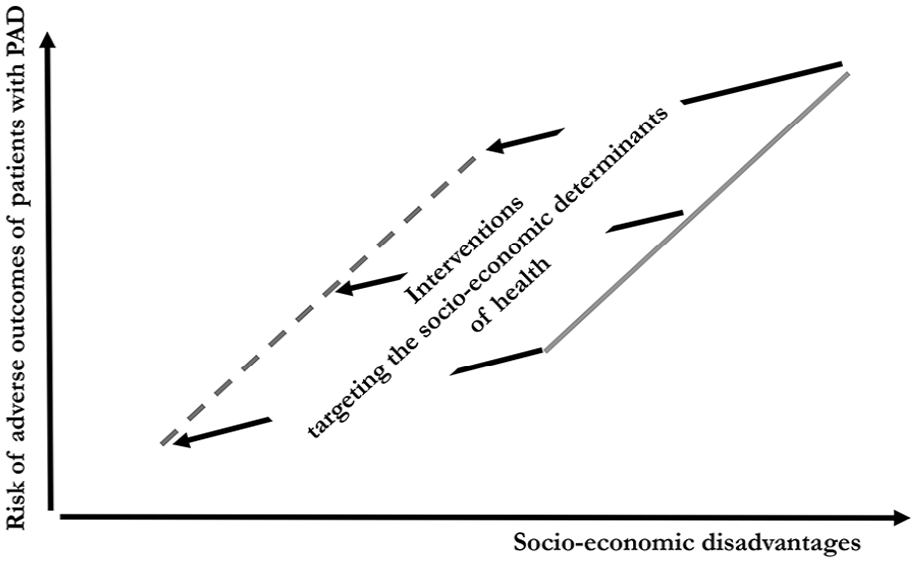
Illustration of the potentials of interventions on socio-economic determinants of health.
Conclusion
According to the available evidence, the impact of SDoH on health is indisputable. This effect is exerted through various mediators/moderators and is influenced by several critical covariates. However, this association shows extraordinary complexity related to the multiplicity of potential factors and their interrelations, difficulties in disentangling their links to health, and complex temporal dynamics (life-course exposure). Demonstrating causality is not straightforward. Some evidence, reasonable consideration and intuitive reasoning support the implementation of various interventions in SDoH to improve health outcomes. The association between socio-economic context and cardiovascular diseases is well documented. However, specific data about PAD is less available. Based on the present data, the relevance of socio-economic determinants in PAD occurrence and different aspects of care was clearly demonstrated. The potential benefits of targeting SDoH with complex interventions can be assumed. However, before an agenda can be built, several challenges in methodology need to be tackled. Further research is recommended, not only at the downstream level of care but also at the upstream level, for which the social context should inevitably be taken into account.
Footnotes
Acknowledgements
The body of this material reflects the discussion among international experts at the 18th European Angiology Day, organized by the VAS-European Independent Foundation in Angiology/Vascular Medicine (26–28 November 2021) and the subsequent developments. 125
We thank Peggy Maguire, Karina Mocanu, Vanessa Moore, Lucy Auad, Chris Manu, Isabelle Durand-Zaleski, and Aaron Liew, who gave useful suggestions and comments and shared their ideas in the community of VAS-International Consortium – International PAD Strategic Network.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.