
Abstract

Keywords
What is a popliteal vein aneurysm?
An aneurysm refers to a weakening of the blood vessel wall, causing it to bulge or dilate to ⩾ 1.5 times its normal diameter. Aneurysms may occur in arteries, which carry oxygen-rich blood away from the heart, or in veins, which return the blood back to the heart. A popliteal vein aneurysm involves dilation of the popliteal vein. The popliteal vein is a deep vein of the leg, formed where the veins that drain the calf come together behind the knee joint and before entering the thigh.
Vein aneurysms are rare but can occur in any vein, and the popliteal vein is the most common location. A popliteal vein aneurysm is a ‘true’ aneurysm involving all three layers of the blood vessel wall, which are called the intima, media, and adventitia. 1 The exact size to define a popliteal vein aneurysm remains controversial, 2 but generally is around 1.5 cm or larger. Experts classify aneurysms according to their shape: either fusiform (vessel expands from all sides) or saccular (vessel wall protrudes from one side), as shown in Figure 1.
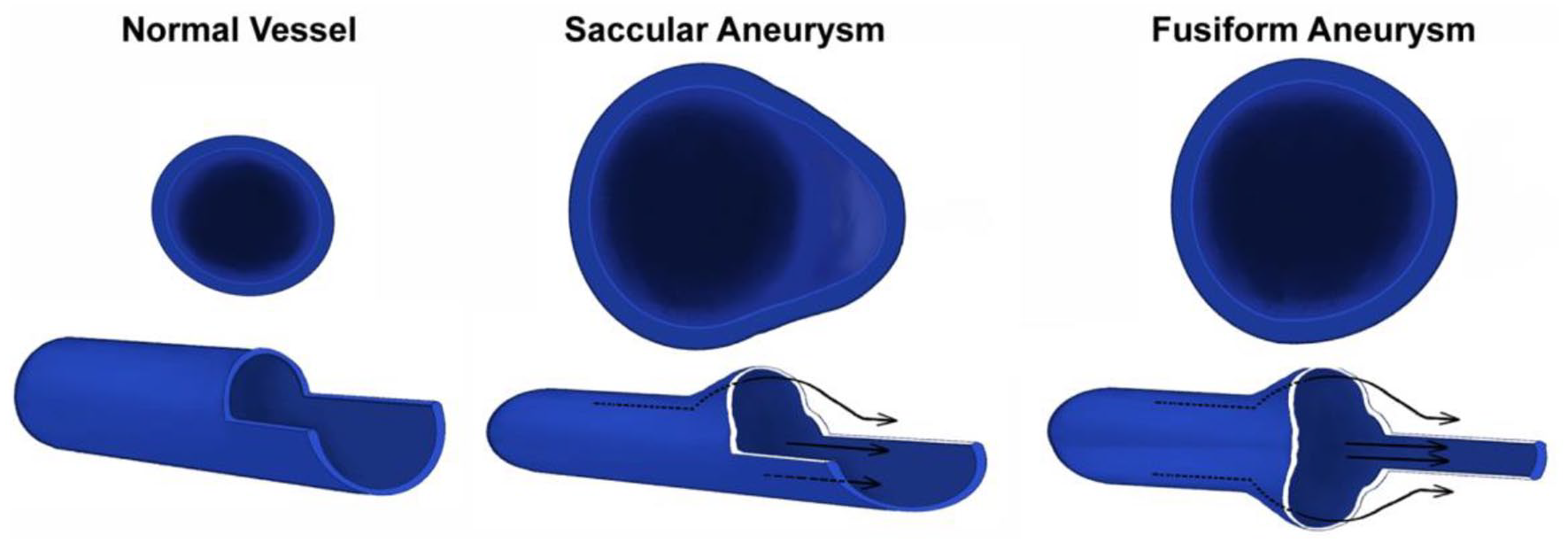
Saccular and fusiform aneurysms compared to a normal vessel. A saccular aneurysm protrudes on one side of the vessel. A fusiform aneurysm expands uniformly from all sides.
What causes popliteal vein aneurysms?
The exact cause is unclear. Contributing factors include inflammation, inherent weakness of the vein wall, venous hypertension (increased pressure in the venous system), mechanical trauma, or degenerative changes. 3 In patients with popliteal vein aneurysm, the fibers in the media layer are chaotic and disorganized and the outer adventitial layer is intact. Future research into these alterations in the vein wall structure will help improve understanding of this entity.
What are the symptoms and complications of a popliteal vein aneurysm?
Popliteal vein aneurysms cause no symptoms in their early stages and have no specific signs, which can lead to underdiagnosis or misdiagnosis. Most serious symptoms are due to blood clots, as explained below. Lumps behind the knee, pain, swelling, skin ulcers, or varicose veins can also occur.
The most important complication of an untreated popliteal vein aneurysm is a blood clot, which may be a deep vein thrombosis (DVT) and/or a pulmonary embolism (PE). Slow venous blood flow, increased blood viscosity (stickiness or thickness), venous valves, thin vein walls, and vulnerability to mechanical damage make veins four times more likely to develop blood clots than arteries. Blood flows slowly through a dilated blood vessel and is especially slow within an aneurysm sac. Furthermore, the blood in an aneurysm tends to swirl like a whirlpool. These unique features lead to abnormal blood flow, with a popliteal vein aneurysm, blood clotting, and potential blockage of the vessel (Figure 2A). Age, smoking, and obesity are additional factors that can increase clotting risk. Unlike arterial aneurysms, risk of rupture of a popliteal vein aneurysm is rare, although some cases have been reported.
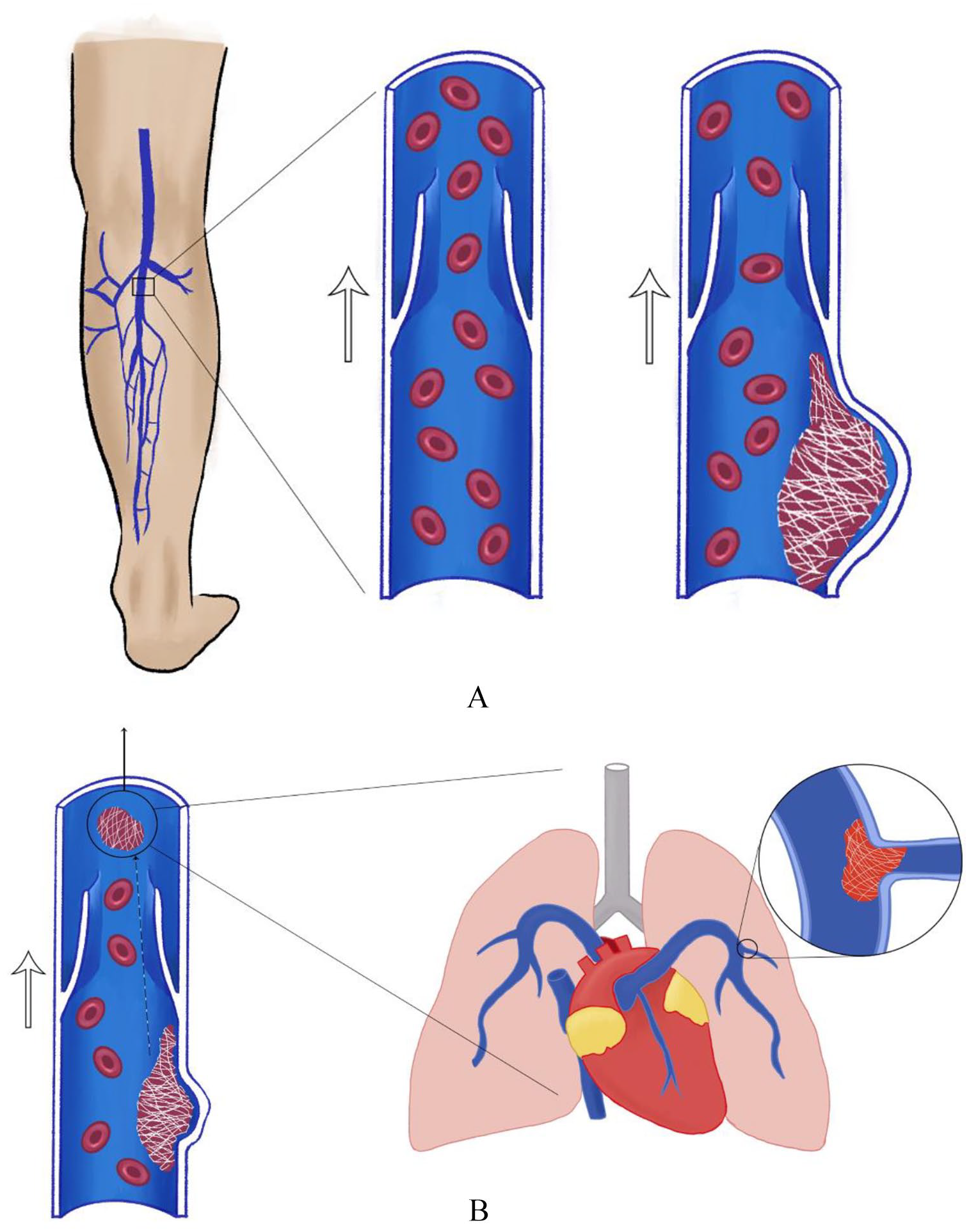
Symptoms of a DVT include swelling, tightness, redness, warmth, and/or pain in the leg(s). If the blood clot migrates to the lungs, it is called a PE, which is the major danger of a popliteal vein aneurysm. Most PEs originate from the deep veins of the legs, particularly from the popliteal veins behind the knee. As the ankle and knee joints move, the walls of the veins are squeezed, which can dislodge a DVT. As shown in Figure 2B, the clot travels in the venous circulatory system, leading to PE. The symptoms of PE depend on the size and number of clots that have traveled to the lungs. Symptoms include shortness of breath, heart palpitations, irregular heartbeat, or chest discomfort, which may be worse while taking a deep breath. If the clots are large, a massive PE may result in low blood pressure, loss of consciousness, or cardiac arrest. For more information on DVT and PE, see the Patient Information Page on venous thromboembolism. 4
How is a popliteal vein aneurysm diagnosed?
Vein aneurysms are rare and may be discovered inadvertently. The popliteal veins are typically difficult to feel on physical examination due to low venous pressure and their location deep behind the knee. Thus, the diagnosis is primarily made by imaging studies.
Vascular (or duplex) ultrasound is noninvasive, convenient, and inexpensive, so it is the test of choice for the initial diagnosis and monitoring of popliteal vein aneurysms. Ultrasound can show the size of the vein aneurysm and whether or not a blood clot has formed. The ultrasound technologist and interpreting physician must correctly identify the popliteal vein aneurysm, which may be confused with a hematoma (collection of blood outside the blood vessel), an arteriovenous fistula (an abnormal connection between an artery and a vein), or a popliteal cyst (fluid-filled lump behind the knee, also called a Baker’s cyst). To diagnose popliteal vein aneurysm, the key distinctive feature is continuity of the vein wall in the area of dilation (enlargement). These aneurysms can occur on both sides, so the veins of both legs should be imaged.
If needed, an angiogram can confirm the diagnosis. In an angiogram, a small tube (catheter) is inserted into the blood vessel, and then contrast (dye) is injected through the catheter while X-ray images are taken. As the ‘gold standard’ for vascular diagnosis, angiography provides a clear and precise visual picture (Figure 3) of the circulation, but it is invasive and carries more risk than an ultrasound.
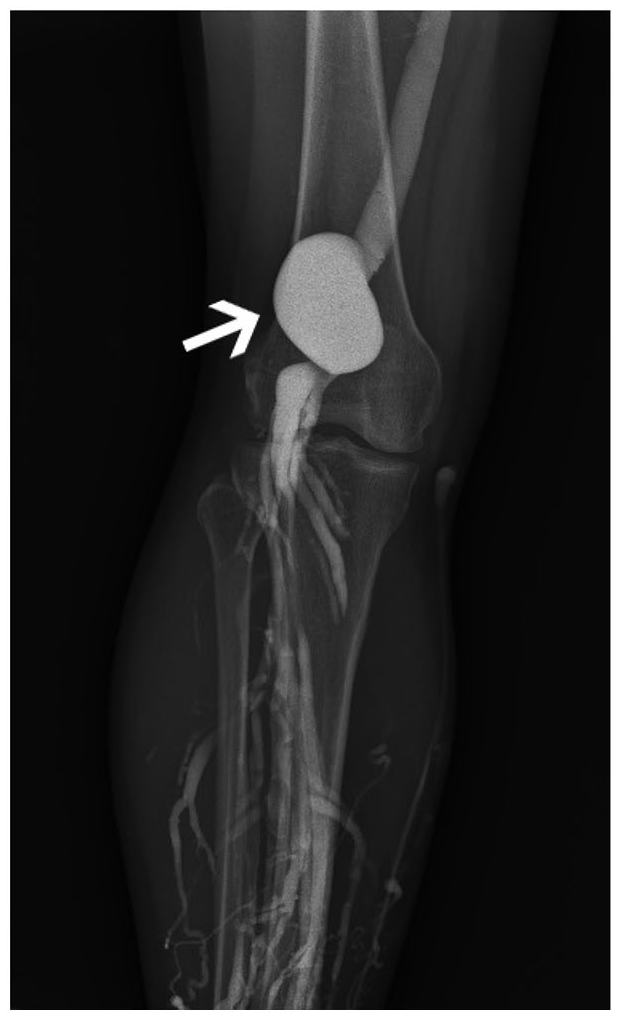
A catheter-directed angiogram shows a large popliteal vein aneurysm (arrow) near the knee joint.
What is the treatment for a popliteal vein aneurysm?
With advances in medical imaging, popliteal vein aneurysms are increasingly being detected inadvertently during evaluation for other medical problems. The treatment approach depends on whether the patient has symptoms, the aneurysm size, and if a blood clot is present within the aneurysm. Surgical treatment may not be necessary for patients with aneurysms smaller than 20 mm with no clot or symptoms; regular follow-up imaging is recommended. 3 Larger aneurysms require surgical intervention due to the high risk of blood clots.
Whereas blood thinners are used to treat blood clots (DVTs) if present, medical treatment alone is often not sufficient in patients with symptoms from a popliteal vein aneurysm. Thus, surgery is the primary treatment for this condition. In general, endovascular (catheter-based) therapies, such as stents, are not used to treat popliteal vein aneurysms due to the location behind the knee joint. The main aim of surgery is to maintain the continuity of the popliteal vein with the other veins of the leg and to restore the normal vein diameter. However, since popliteal vein aneurysms are rare, no consensus exists on the standard surgical approach and there is little clinical research available. Clinicians will develop a personalized treatment plan according to the aneurysm size and other co-existing medical conditions. Postoperative follow-up is important to monitor for any subsequent problems.
Can popliteal vein aneurysms be prevented?
Early diagnosis and treatment of a popliteal vein aneurysm are key to prevent complications. Because it is uncommon, no specific measures have been developed to prevent the aneurysm itself. In the event of leg discomfort (suspected DVT) or unexplained PE, the popliteal veins should be evaluated for aneurysm using vascular (duplex) ultrasound.
Summary
Popliteal vein aneurysm is a rare disorder involving dilation of the popliteal vein behind the knee. The location of the aneurysm behind the knee increases the risk of blood clots (DVT and PE). Vascular ultrasound is often used to diagnose popliteal vein aneurysm, and surgery provides definitive treatment of large aneurysms (⩾ 20 mm) to avoid complications.
The Vascular Disease Patient Information Page is a regular feature of Vascular Medicine. All articles in the collection are available for free online at http://journals.sagepub.com/vmjpatientpage.
The Vascular Disease Patient Information Page is provided for educational purposes only and is not a substitute for medical advice.
Footnotes
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
Dr Elizabeth Ratchford’s work was supported in part by the generosity of David Kotick (1926–2021). Dr Chuanqi Cai’s research was supported by National Natural Science Foundation of China (no. 82000729).