
Abstract
Background:
D-dimer, a marker of ongoing procoagulant activity, has been widely used for the diagnosis of venous thromboembolism (VTE). The prognostic significance of D-dimer in stratifying VTE risk for acutely ill medical patients has not been well-established.
Methods:
A literature search was performed to collect studies that compared the incidence of short-term VTE between acutely ill medical patients with elevated or nonelevated D-dimer levels. The cutoff of D-dimer was 0.5 μg/mL or otherwise defined by included studies. The study endpoint was any occurrence of VTE (inclusive of deep vein thrombosis [DVT], pulmonary embolism, or VTE-related death) within 90 days of hospital presentation. A meta-analytic approach was employed to estimate the odds ratio (OR) with 95% CI by fitting random-effects models using the generic inverse variance weighted approach.
Results:
A total of 10 studies representing 31,119 acutely ill medical patients were included. Compared to those with nonelevated D-dimer levels, patients with elevated D-dimer had approximately threefold greater odds for short-term VTE within 90 days (OR, 3.28; 95% CI, 2.44 to 4.40; p < 0.0001). The association of elevated D-dimer with VTE composite (OR, 3.33; 95% CI, 2.20 to 5.02) and with DVT (OR, 3.26; 95% CI, 2.32 to 4.58) was comparable. The association was significant among patients who presented various acute medical illness (OR, 2.68; 95% CI, 2.01 to 3.58) and those who presented with acute stroke (OR, 3.25; 95% CI, 2.31 to 4.58).
Conclusion:
Elevation of D-dimer was predictive of the occurrence of VTE within 90 days among acutely ill medical patients.
Keywords
Introduction
Venous thromboembolism (VTE), including deep vein thrombosis (DVT) and pulmonary embolism (PE), is a key contributor to the global disease burden with an estimated incidence of three cases per 100 hospitalizations per year. 1 Current guidelines recommend VTE risk assessment for medical inpatients prior to thromboprophylaxis.2,3 Although several risk assessment models have been devised over the past decade, there has been no clear consensus on the optimal strategies of VTE risk assessment for this population. Furthermore, an overview of systematic reviews revealed that the discriminatory capacity of the existing models varied widely, with the concordance statistic ranging from 0.65 to 0.89. 4 Therefore, refinement of VTE risk assessment remains an ongoing challenge.
Measurement of D-dimer, a specific soluble degradation product of cross-linked fibrin clots, has been integrated into validated diagnostic algorithms of DVT and PE. 5 Although the clinical utility of D-dimer in the diagnosis of VTE has been established, its prognostic potential in risk-stratification of VTE has not undergone a thorough investigation. In a substudy of the MEDENOX trial, acutely ill medical patients who developed VTE within 10 days were found to have significantly higher D-dimer concentrations at presentation than those who did not develop VTE. 6 Further, all VTE events occurred in patients with D-dimer concentrations higher than normal levels (i.e., 0.5 μg/mL) both at presentation and on day 10. Subsequent cohort studies showed that D-dimer was associated with a greater risk of VTE occurrence among patients with various acute medical illnesses, including acute decompensated heart failure and acute stroke.7–9 In corroboration with these findings, the prognostic utility of D-dimer was confirmed in the secondary analysis of the MAGELLAN trial, 10 and was implemented as a part of the inclusion criteria in the APEX and MARINER trials to identify medical inpatients at an increased risk of VTE.11,12 However, a previous meta-analysis based on two studies indicated that there was only moderate certainty in the evidence regarding D-dimer as a prognostic factor for VTE. 13 To address the evidence gap, the present study aimed to comprehensively review the available studies that quantitatively assessed the association of elevated D-dimer with short-term VTE risk among acutely ill medical patients.
Methods
This study was conducted in accordance with the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) guidelines. 14 PROSPERO Registration ID: CRD42021264555.
Search strategies and selection criteria
A systematic literature search was performed in PubMed/MEDLINE and Embase supplemented by hand searches of references from relevant publications. Detailed queries are provided in online supplementary material in Table S1. The inclusion criteria were as follows: (1) original research articles, letters, or brief reports; (2) human participants presented with an acute medical illness (i.e., acute heart failure, acute respiratory failure, acute infectious disease, acute stroke, active cancer, acute inflammatory or rheumatic disease); (3) report of at least one of the clinical outcomes of interest (i.e., VTE, DVT, PE, or VTE-related death); and (4) accessible full text to allow for screening and data extraction. The exclusion criteria were as follows: (1) not original research (e.g., case report, case series, study protocol, narrative review, systematic review, and meta-analysis); (2) inclusion of human participants that did not present with an acute medical illness; (3) no report of any of the clinical outcomes of interest; and (4) publications without accessible full text. Search results were limited to the English language and the time from database inception to July 1, 2021. Two independent investigators screened and selected studies for inclusion based on the eligibility criteria. Disagreement in study selection was resolved by discussion and consensus. A flow diagram depicting the process of the study selection is shown in Figure S1 (online supplementary material).
Data extraction
Information about study design, study population, participant demographics and characteristics, use and duration of pharmacological thromboprophylaxis, duration of follow-up, measurement timing, analytical assay, and cutoff value of D-dimer, and the number of events and study participants or effect size estimates was extracted from the full text of publications. Two independent investigators extracted and tabulated data. Any discrepancy in data extraction or data entry was adjudicated by a third investigator.
Quality assessment
Quality assessment was performed by two independent investigators using the Newcastle–Ottawa Scale for cohort studies. 15 Quality assessment criteria for cohort studies are provided in Table S2 (online supplementary material). Disagreement in quality assessment was resolved by discussion and consensus. The results of quality assessment are provided in Table S3 (online supplementary material). Total scores of 0–3, 4–6, and 7–9 were considered as low, moderate, and high quality, respectively.
Study population, exposure, and endpoints
The study population comprised patients who presented to the emergency department or who were hospitalized with an acute medical illness, including acute heart failure, acute respiratory failure, acute infectious disease, acute stroke, active cancer, and acute inflammatory or rheumatic disease. These acute medical illnesses have been documented to be associated with an increased risk of VTE. Patients who presented with other acute medical illnesses irrelevant to VTE were not considered in the study.
The exposed group included patients who had elevated baseline D-dimer levels. The control group included patients who had normal baseline D-dimer levels. The cutoff of D-dimer was 0.5 μg/mL or otherwise defined by included studies.
The study endpoint was any occurrence of short-term VTE, inclusive of DVT, PE, or VTE-related death within 90 days of hospital presentation. DVT was detected by duplex ultrasound or based on clinical diagnosis. Table S4 (online supplementary material) provides detailed information on the diagnostic method and criteria applied by each study assessment of DVT.
Statistical analysis
The association between elevated D-dimer and the short-term risk of VTE was estimated using a meta-analytic approach. Odds ratio (OR) with 95% CI was calculated as the effect size, where an OR > 1 indicates a greater risk of VTE in the exposed group (patients with elevated D-dimer) than the control group (patients with normal D-dimer). For each study, the numbers of VTE events and individuals with or without elevated D-dimer or multivariable-adjusted ORs from the original studies were extracted for calculating the effect size (covariates for multivariable adjustment from the included studies are provided in Table S5 in the online supplementary material). The pooled effect size was summarized by fitting the random-effects models using the generic inverse variance weighted approach. Heterogeneity across the studies was assessed using Higgins’s I2 statistic, with cutoff values of ⩽ 30%, > 30% to ⩽ 50%, and > 50% indicating mild, moderate, and substantial heterogeneity, respectively. 16 Conventional funnel plots and Egger’s tests were employed to detect small-study effects. 17 A contour-enhanced funnel plot with contour lines corresponding to perceived milestones of statistical significance (p = 0.01, p = 0.05, and p = 0.10) was constructed to aid in determining whether asymmetry was more likely to be attributable to publication bias or other mechanisms. 18 The trim-and-fill approach was applied as a sensitivity analysis for the presence of funnel plot asymmetry. 19 In addition, to examine the robustness of association, five sets of subgroup analysis were performed: (1) stratification by the endpoint (VTE composite or DVT); (2) stratification by the type of acute medical illness; (3) stratification by whether or not the studies excluded patients with VTE at enrollment; (4) stratification by whether or not the patients received systematic chemoprophylaxis; and (5) stratification by whether or not systematic detection of DVT was performed. For each set of subgroup analysis, the difference between subgroups was tested in the random-effects model. All analyses were performed using the meta package in the R software (Version 4.0.5; the R Foundation for Statistical Computing). 20
Results
A total of 10 studies, comprising 31,119 acutely ill medical patients, were included.7–10,12,21–25 Results of quality assessment are shown in Table S3 (online supplementary material). The quality was high in nine (90.0%) studies and moderate in one (10.0%) study. Of note, two studies did not report whether VTE was excluded at enrollment or did not exclude VTE at enrollment,9,24 which may have introduced bias in the patient selection since the outcome of interest should not be present at the start of study. Specifically, in the study by Yi et al., 9 patients underwent VTE prophylaxis under the assumption that VTE was not present at baseline, whereas in the study by Nickel et al., 24 a small proportion (3.3%) of patients presented with VTE at baseline. Study characteristics are provided in Table 1. The duration of follow-up varied from less than 2 weeks to 90 days. With respect to the endpoint, six studies evaluated the VTE composite,7,8,10,12,23,24 and four studies evaluated DVT.9,21,22,25 With respect to the index hospitalization event, six studies enrolled patients with various types of acute medical illness,7,10,12,22–24 three studies enrolled patients with acute stroke,9,21,25 and one study enrolled patients with acute decompensated heart failure. 8 Eight studies excluded the presence of VTE at the time of enrollment.7,8,10,12,21–23,25 Patients received systematic chemoprophylaxis in four studies.8,10,12,23 Systematic detection of DVT was performed in seven studies.7,9,10,21–23,25 The cutoff value of D-dimer ranged from 0.5 to 1.5 μg/mL. Patient characteristics are described in Table 2. The mean age of study participants was ⩾ 65 years in all studies. The percentage of men ranged from 45.6% to 66.8%. The mean body mass index (BMI) ranged from 21.6 to 29.4 kg/m2. The distribution of acute medical illness varied widely across the studies.
Study characteristics.
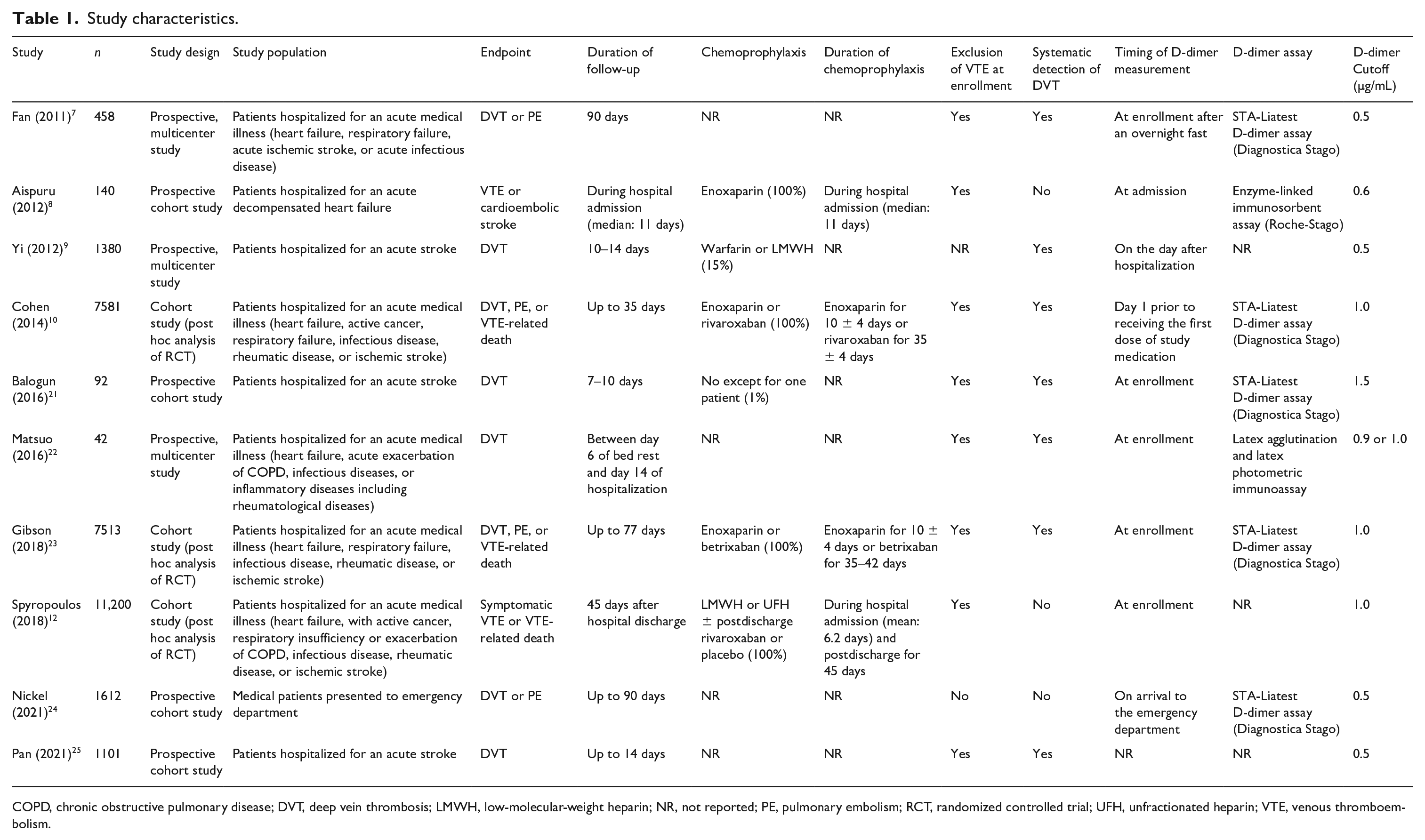
COPD, chronic obstructive pulmonary disease; DVT, deep vein thrombosis; LMWH, low-molecular-weight heparin; NR, not reported; PE, pulmonary embolism; RCT, randomized controlled trial; UFH, unfractionated heparin; VTE, venous thromboembolism.
Patient characteristics.
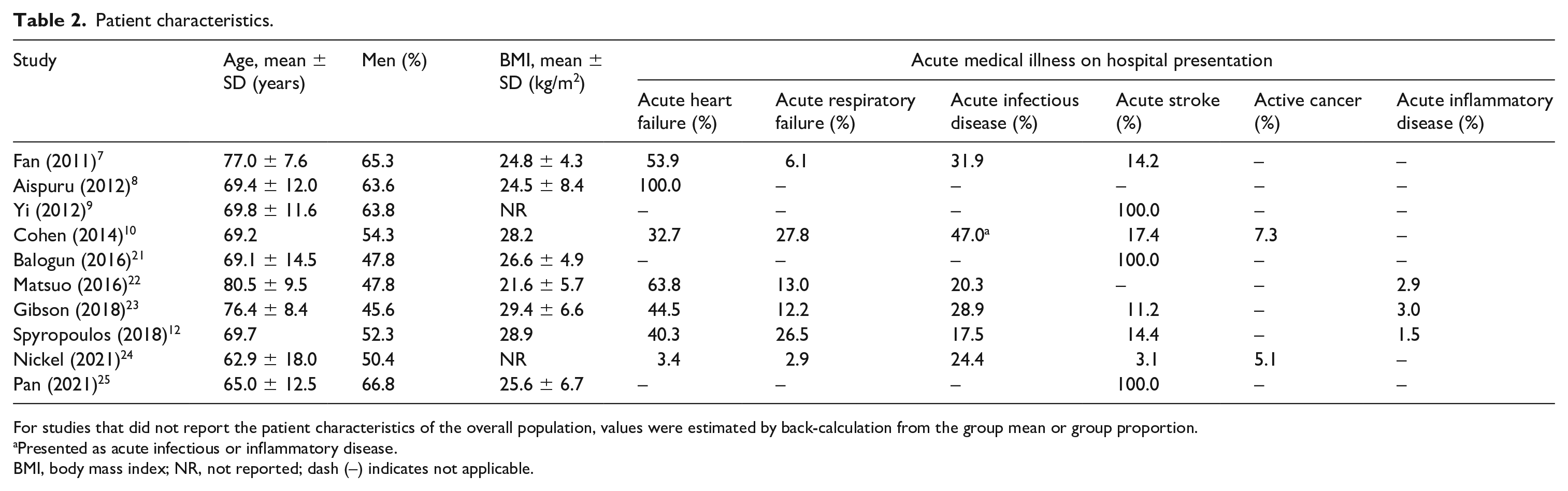
For studies that did not report the patient characteristics of the overall population, values were estimated by back-calculation from the group mean or group proportion.
Presented as acute infectious or inflammatory disease.
BMI, body mass index; NR, not reported; dash (–) indicates not applicable.
D-dimer and short-term VTE
The associations of D-dimer and occurrence of short-term VTE are summarized in Figure 1. Compared to patients with nonelevated D-dimer, patients with elevated D-dimer had approximately threefold greater odds of developing VTE within 90 days of hospital presentation (OR, 3.28; 95% CI, 2.44 to 4.40; p < 0.0001). Substantial heterogeneity was observed (I2 = 69.1%; 95% CI, 40.5% to 84.0%; p = 0.0006).
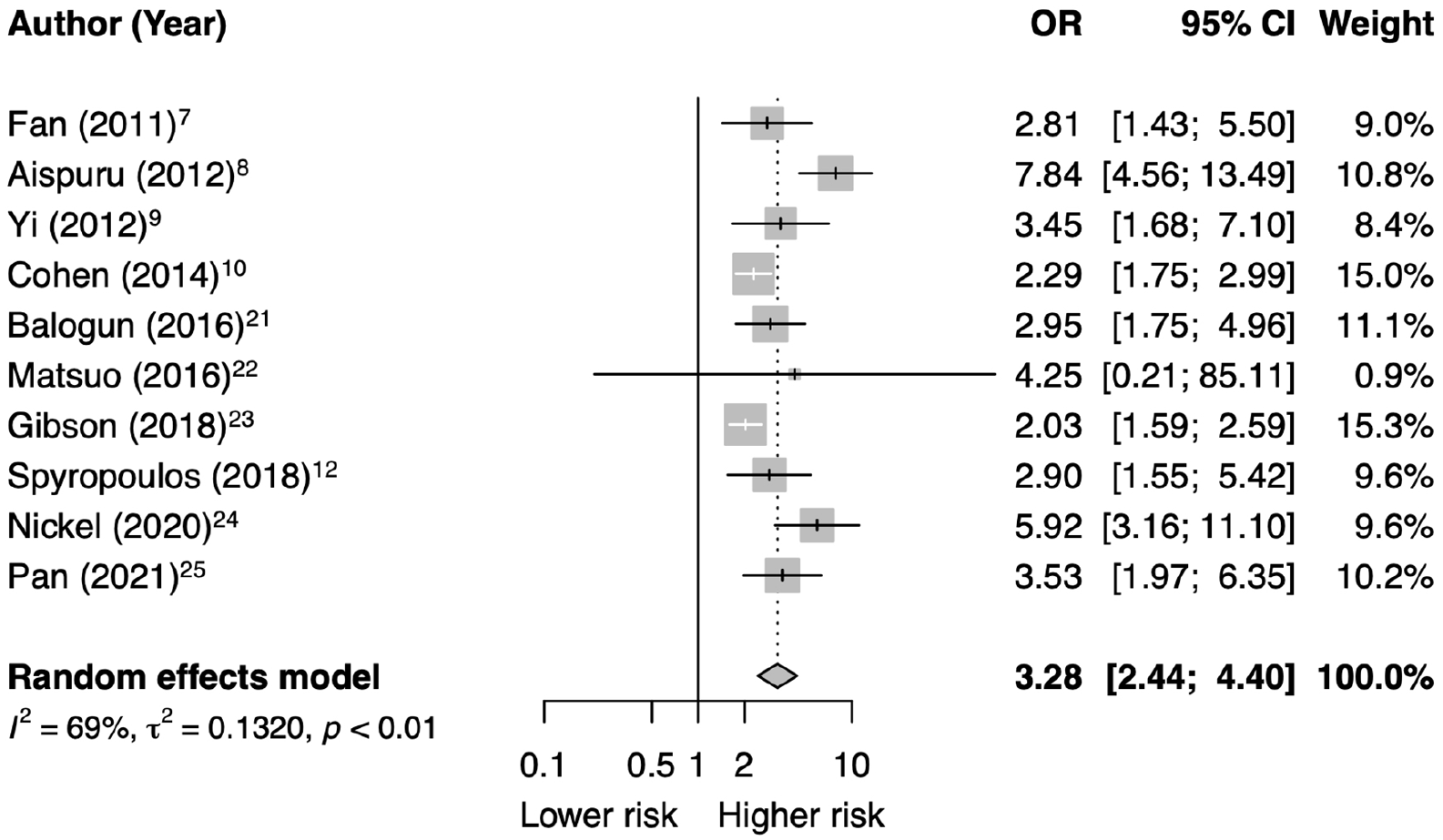
Association of D-dimer and short-term venous thromboembolism.
The funnel plot was modestly asymmetric (Figure S2; online supplementary material), as suggested by Egger’s test (p = 0.05). In the contour-enhanced funnel plot, there was a suggestion of four perceived missing studies on the top left side of the plot and one on the bottom left side of the plot. All five studies were within the white area of nonsignificance, suggesting that publication bias may be a plausible explanation of the asymmetry. The trim-and-fill approach included 15 studies (five studies imputed) and yielded a random-effects estimate (OR, 2.38; 95% CI, 1.73 to 3.27; p < 0.0001) consistent with the original analysis.
Subgroup analyses
As shown in Figure 2, among studies that evaluated VTE composite, patients with elevated D-dimer had threefold greater odds of developing composite VTE events than patients with nonelevated D-dimer (OR, 3.33; 95% CI, 2.20 to 5.02). Similarly, among studies that evaluated DVT, elevated D-dimer was associated with an increased risk for developing DVT events (OR, 3.26; 95% CI, 2.32 to 4.58). No significant subgroup difference was observed (p = 0.94).
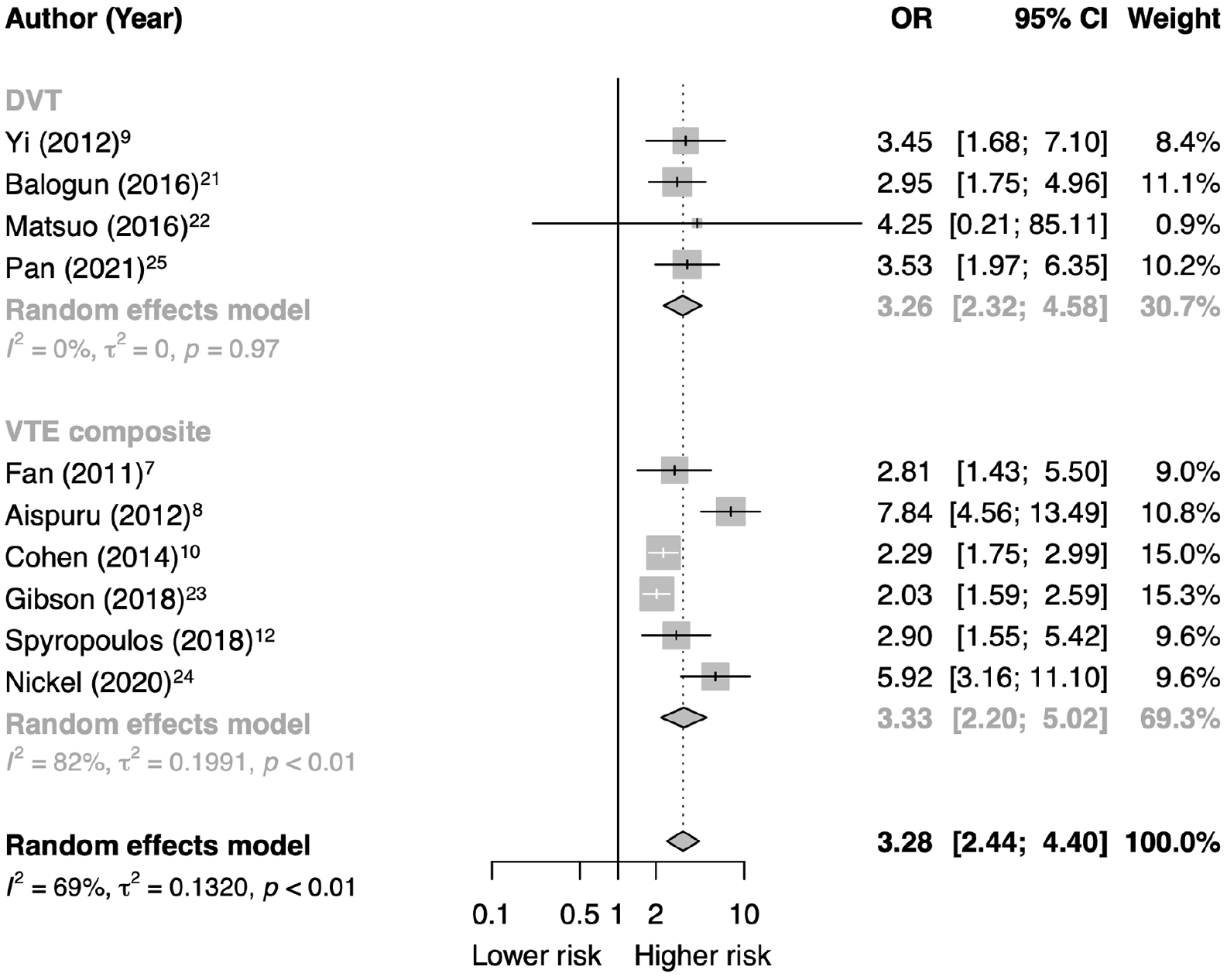
Subgroup analysis by the endpoint.
As shown in Figure 3, among studies that enrolled patients with various types of acute medical illness, elevated D-dimer was associated with an increased risk for developing VTE events (OR, 2.68; 95% CI, 2.01 to 3.58). The association of D-dimer with VTE was also significant among studies that enrolled patients presented with acute stroke (OR, 3.25; 95% CI, 2.31 to 4.58), as well as the study that enrolled patients with acute heart failure (OR, 7.84; 95% CI, 4.56 to 13.49). There was a significant subgroup difference in terms of the magnitude of association (p = 0.0028).
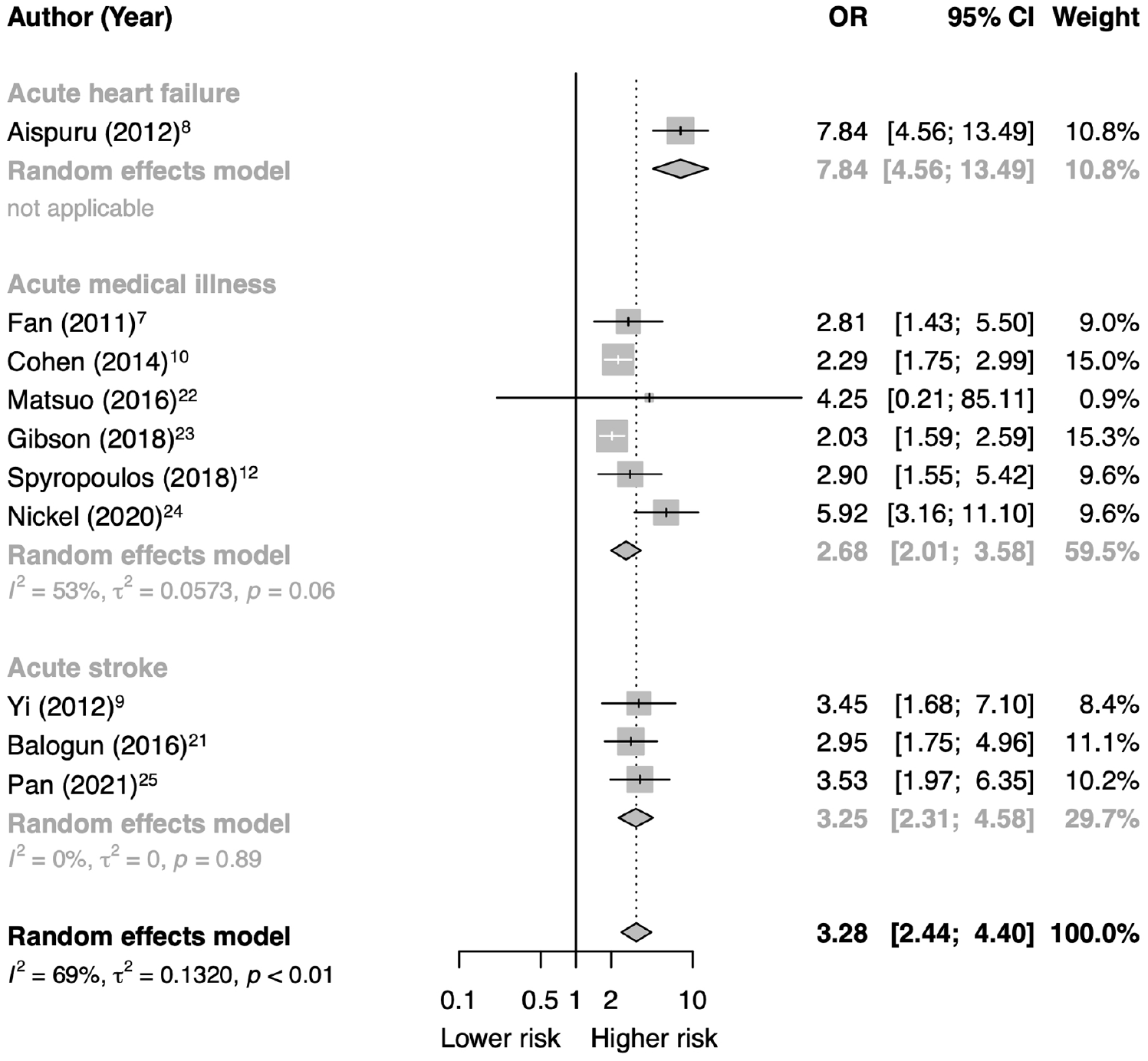
Subgroup analysis by the type of acute medical illness.
As shown in Figure S3 (online supplementary material), among studies that excluded the presence of VTE at enrollment, patients with elevated D-dimer had threefold greater odds for VTE occurrence than patients with nonelevated D-dimer (OR, 3.03; 95% CI, 2.22 to 4.13). Among studies that did not report whether VTE was excluded at enrollment or did not exclude VTE at enrollment, elevated D-dimer was associated with an increased VTE risk (OR, 4.66; 95% CI, 2.75 to 7.89). No significant subgroup difference was observed (p = 0.17).
As shown in Figure S4 (online supplementary material), among studies that utilized systematic chemoprophylaxis, patients with elevated D-dimer had threefold greater odds for VTE occurrence than patients with nonelevated D-dimer (OR, 3.56; 95% CI, 2.71 to 4.68). Among studies that did not utilize systematic chemoprophylaxis, elevated D-dimer was associated with an increased VTE risk (OR, 3.05; 95% CI, 1.89 to 4.94). No significant subgroup difference was observed (p = 0.59).
As shown in Figure S5 (online supplementary material), among studies that performed systematic detection of DVT, patients with elevated D-dimer had twofold greater odds for VTE occurrence than patients with nonelevated D-dimer (OR, 2.37; 95% CI, 2.03 to 2.77). Among studies that did not perform systematic detection of DVT, elevated D-dimer was associated with an increased VTE risk (OR, 5.20; 95% CI, 2.90 to 9.30). There was significant subgroup difference in terms of the magnitude of association (p = 0.0106).
Discussion
The results of meta-analysis are summarized in Table 3. Patients with elevated D-dimer on hospital presentation had threefold increased odds of developing VTE within 90 days compared to those who did not have D-dimer elevation. The association between D-dimer and VTE remained significant when stratified by endpoint definition, the type of acute medical illness, exclusion of VTE at enrollment, universal administration of chemoprophylaxis, or systematic detection of DVT.
Summary of results.
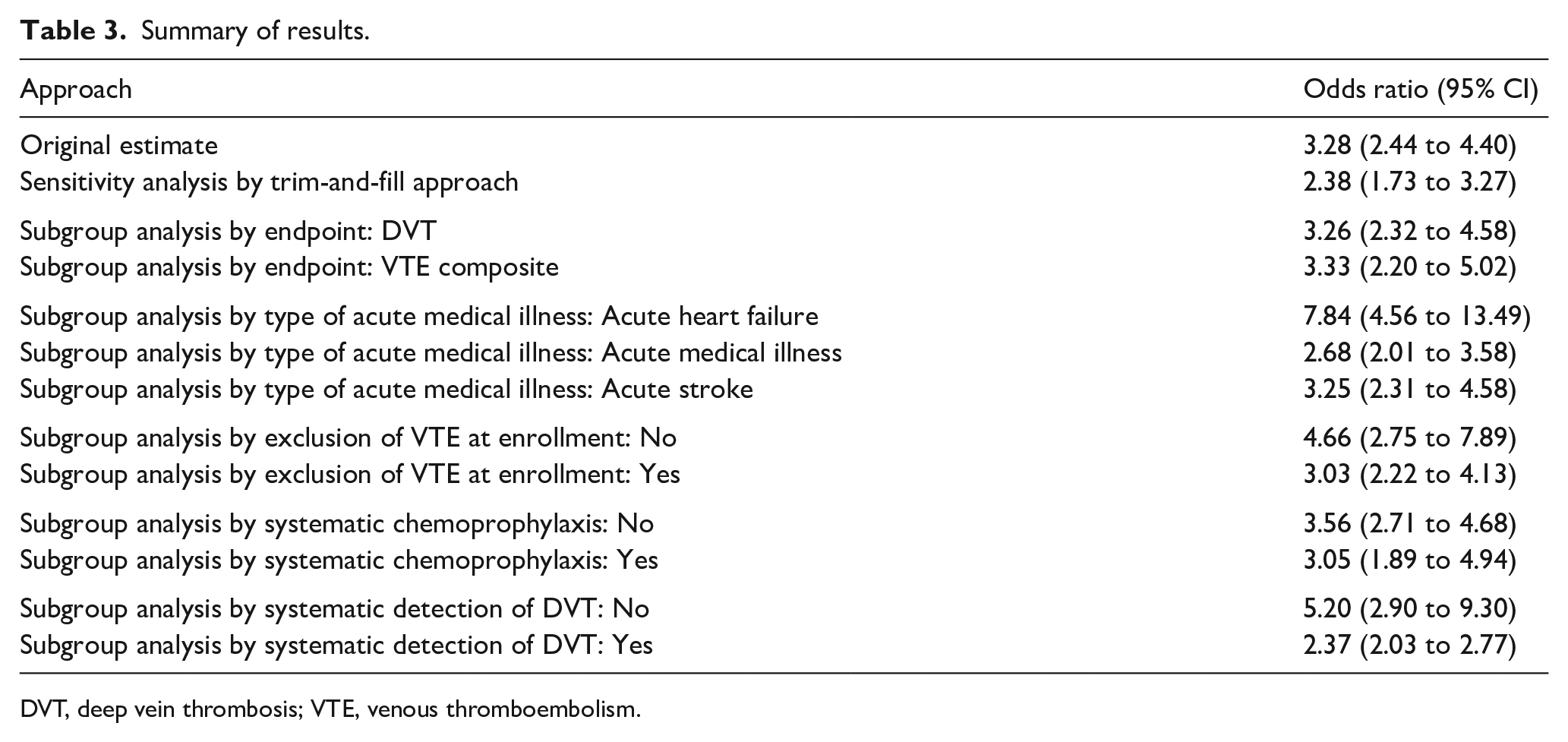
DVT, deep vein thrombosis; VTE, venous thromboembolism.
An interesting finding was that the magnitude of association between D-dimer and VTE was significantly greater in studies that did not perform systematic detection of DVT (OR = 5.20) than in the studies that screened for DVT (OR = 2.37; p = 0.0106 for subgroup difference). With study-mandated DVT screening, additional asymptomatic DVT events may have been identified among patients who did not experience symptoms suggestive of DVT. It was hypothesized that positive D-dimer would be more accurate in predicting symptomatic VTE than predicting asymptomatic DVT. Comparing patients with positive D-dimer to patients with normal D-dimer, the difference in symptomatic VTE risk may be greater than the difference in asymptomatic DVT risk. Consequently, the inclusion of asymptomatic DVT may have attenuated effect size among studies that performed systematic detection. This result suggests that the prognostic significance of D-dimer was more prominent for clinically overt VTE than asymptomatic DVT. Nevertheless, prediction of asymptomatic DVT events may be clinically important, as asymptomatic thrombosis was found to be associated with three- to eightfold increased mortality in the subanalyses of PREVENT and APEX trials.26,27 It is also noteworthy that the magnitude of association was greater among the study that enrolled patients with acute heart failure (OR = 7.84) or the studies that enrolled patients with acute stroke (OR = 3.25) than studies that enrolled patients with various acute medical illnesses (OR=2.68; p = 0.0028 for subgroup difference), suggesting that the acutely ill medical patients represent a population of heterogeneous predisposition to VTE, and the risk for short-term VTE may vary by the presenting acute medical illness. However, in view of the small number of studies within the subgroups, this finding needs to be validated in future studies.
Given that the D-dimer elevation is an independent predictor of VTE, recent studies have further examined the incremental prognostic value of D-dimer by incorporating D-dimer into the IMPROVE VTE risk assessment model (i.e., IMPROVEDD score). 28 The addition of D-dimer into the model was shown to improve VTE discrimination and reclassification significantly among acutely ill medical patients. Subsequently, the IMPROVEDD score was externally validated in a retrospective cohort study of patients hospitalized with coronavirus disease 2019 (COVID-19), which showed that the inclusion of elevated D-dimers enhanced VTE discrimination of the original model by 6.8%. 29 Results from the present analysis corroborated with previous meta-analyses of hospitalized COVID-19 patients.30,31 Specifically, hospitalized COVID-19 patients who developed VTE had a significantly higher D-dimer at baseline than those who did not develop VTE, with a mean difference of 2–3 μg/mL. In this context, the link between markedly elevated D-dimer and heightened risk of thromboembolic complications may be explained by upregulated fibrinolysis in the alveoli by urokinase-type plasminogen activator released from alveolar macrophages. 32 Taken together, these findings support the conjunctive use of D-dimer measurement with a validated risk assessment model for stratifying VTE risk in patients requiring hospital admission. Preliminary evidence also points to the potential value of D-dimer measurement in determining the candidacy of extended pharmacological thromboprophylaxis. A prior meta-analysis indicated that extended prophylaxis reduced VTE without excess major bleeding among medical inpatients with elevated D-dimer as compared to standard prophylaxis. 33 More research is required to assess the impact of D-dimer measurement on the decision of pharmacological thromboprophylaxis, health outcomes, and cost-effectiveness of care.
Impaired renal function and advanced age may potentially confound the association between D-dimer and VTE among acutely ill hospitalized medical patients. Patients with impaired renal function tend to have increased D-dimer values due to hyperactivity of the coagulation system and decreased elimination of D-dimer. 34 Additionally, chronic kidney disease is associated with elevated VTE risk, 35 possibly due to endothelial injury, increased activation of coagulation, platelet dysfunction, and decreased endogenous anticoagulants.36–38 Similarly, since both D-dimer level and VTE risk increase with age,39,40 the performance of D-dimer at the conventional cutoff in predicting VTE may vary by age. It should be noted that in the present meta-analysis, only one study reported the OR adjusted for creatinine clearance, and only five studies reported the OR adjusted for age (Table S5; online supplementary material). Further research is warranted to explore the impact of renal impairment and advanced age on the association of D-dimer with VTE risk.
Study limitations
Several limitations should be noted. First, the meta-analysis was conducted at the study-level. Accordingly, adjustment for patient-level characteristics could not be performed. Second, there were considerable variations in the follow-up duration across the studies (ranging from < 14 days to 90 days), which may have contributed to the heterogeneity. In addition, the follow-up duration varied across participants within most of the included studies. Therefore, the impact of the follow-up duration on the association between elevated D-dimer and VTE risk was not assessed in the present aggregate data meta-analysis. Third, different D-dimer assays and cutoff values were used in the studies. More studies are needed to harmonize D-dimer measurements from different analytical methods and explore the optimal D-dimer cutoff for predicting VTE risk. Fourth, the diagnostic criteria for DVT were slightly different across the studies. Although some studies included one criterion to establish the diagnosis of DVT, others included multiple criteria. Furthermore, the lack of defined chronic versus acute thrombus features on imaging may have led to overestimation of acute DVT. Fifth, the meta-analysis did not include non-English literature or gray literature (e.g., unpublished studies, graduate theses, company reports, conference abstracts, presentations, or proceedings) without accessible full text. Selection bias may have been introduced. Last, among the 10 included studies, three studies comprised 84.5% of the total study population. Results from these three larger studies may have influenced the summary estimate.
Conclusions
The meta-analysis demonstrated that elevation of D-dimer was associated with an increased VTE risk within 90 days among acutely ill medical patients. In light of its prognostic utility, D-dimer may be considered in constructing VTE risk assessment models.
Supplemental Material
sj-pdf-1-vmj-10.1177_1358863X221109855 – Supplemental material for Association of D-dimer with short-term risk of venous thromboembolism in acutely ill medical patients: A systematic review and meta-analysis
Supplemental material, sj-pdf-1-vmj-10.1177_1358863X221109855 for Association of D-dimer with short-term risk of venous thromboembolism in acutely ill medical patients: A systematic review and meta-analysis by Gerald Chi, Jane J Lee, Sahar Memar Montazerin and Jolanta Marszalek in Vascular Medicine
Footnotes
Data availability statement
Requests for access to the data reported and the code used in this article will be considered by the corresponding author.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Supplementary material
The supplementary material is available online with the article
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.