
Abstract
Introduction:
Functional performance is impaired in patients with peripheral artery disease (PAD). The effects of a supervised exercise training (SET) program on functional performance have yet to be clearly determined. The aim was to investigate the time-course evolution of functional performance during a 3-month SET program.
Methods:
Patients with chronic symptomatic PAD participating in a 3-month SET program were investigated. Six-minute walking distance (6MWD), the stair climbing test (SCT), and the Short Physical Performance Battery (SPPB) were assessed before SET, after the first and second months of SET, and following the SET program. The ankle– and toe–brachial indices were measured before and after the SET program.
Results:
Ninety patients with PAD (age 65.4 ± 10.2 years) were analyzed. The 6MWD significantly improved after the first (+7%, p ⩽ 0.001) and second months (+13%, p ⩽ 0.001) and following SET (+14%, p ⩽ 0.001) compared to before the SET program. The 6MWD significantly improved after the 2nd month (+6%, p ⩽ 0.001) and following SET (+7%, p ⩽ 0.001) compared to after the first month of the SET program. The SPPB score and SCT performance significantly improved after the first (SPPB score: +9%, p ⩽ 0.001; SCT: +17%, p ⩽ 0.001) and second months (SPPB score: +11%, p ⩽ 0.001; SCT: +24%, p ⩽ 0.001) and following SET (SPPB score: +12%, p ⩽ 0.001; SCT: +25%, p ⩽ 0.001) compared to before the SET program. No significant differences were observed following SET compared to the second month of the SET program. Vascular parameters did not change significantly.
Conclusions:
A 3-month SET program improves several components of functional performance, and adaptations mainly occur during the 1st and 2nd months of the SET program.
Keywords
Introduction
Peripheral artery disease (PAD) affects over 236 million women and men worldwide. 1 Despite its high prevalence, PAD has been understudied compared to myocardial infarction and stroke. 2 Patients living with PAD have a high risk of death from cardiovascular causes.2,3 Intermittent claudication is a typical manifestation of PAD and is defined by reproducible pain/discomfort appearing in the legs during physical exertion and resolving within a few minutes of rest. 2 Notably, a large proportion of patients with PAD present with atypical claudication, characterized by difficulty walking with pain/discomfort that begins at rest and does not induce a stop during walking, or pain/discomfort that does not resolve with a few minutes of rest. 2 This may impair walking performance and daily life activities, leading to reductions in quality of life.
Patients with PAD have poor balance, muscle strength and power, and present a high prevalence of sarcopenia.4–6 This may lead to greater impairments in functional performance among patients with PAD than among non-PAD individuals.7 –9 Functional performance has been shown to predict further mobility loss and mortality in these patients.10,11 Functional performance is defined as the ability to perform a daily life task and is usually assessed with validated tests based on different components such as overground walking, standing balance, and muscle function.12 –14 Maintaining high levels of functional performance is therefore essential to preserve long-term independence, especially in older individuals.
A supervised exercise training (SET) program is the first-line therapy for patients with PAD and has been given a Class IA recommendation.15,16 A SET program has been shown to improve walking performance, quality of life, and cardiorespiratory fitness.17,18 Nevertheless, in PAD trials, the effects of a SET program on different components of functional performance have rarely been investigated. 19 Recently, we showed that a 3-month SET program improved overall functional performance in patients with PAD, and that larger increases in relative sit-to-stand muscle power following the SET program were associated with greater improvements in functional performance. 20 However, to the best of our knowledge, no study has investigated the monthly time-course evolution of functional performance during a 3-month SET program.
This study aimed to investigate the time-course evolution of functional performance during a 3-month SET program assessed by means of different functional tests focused on overground walking abilities, standing balance, and muscle function in patients with symptomatic PAD.
Methods
Participants
In this single-arm, prospective, nonrandomized study, symptomatic patients with chronic atherosclerotic PAD were investigated. As previously described,20 –23 patients were recruited during routine vascular visits to participate to our clinical multimodal SET program. The multimodal SET program includes patients with chronic uni- or bilateral lower-limb lifestyle-limiting claudication and resting ankle–brachial index (ABI) ⩽ 0.9 or > 20% decrement in posttreadmill ABI. 15 Patients with critical limb ischemia, patients who were not able to perform three training sessions per week, or who presented with cardiac contraindications to exercise were not included. For study purposes, we included all patients who had a monthly assessment (before SET, after the first and second months of SET, and following the SET program) of functional performance. All participants signed an informed consent. All procedures were conducted in accordance with the Declaration of Helsinki. The study was approved by the local ethics committee.
Multimodal SET program
The multimodal SET program had a 3-month duration with three sessions per week lasting 60 minutes.20 –23 During two of three sessions per week, patients performed outdoor Nordic walking. All patients were given information on correct pole use. In accordance with the guidelines,24,25 the claudication pain intensity during the walking bouts was moderate-to-severe. This was followed by a brief period of rest until complete (or almost complete) resolution of the pain. Although less reported in PAD trials, 17 the rate of perceived exertion (RPE) on Borg’s scale and/or heart rate (HR) throughout the exercise sessions were also used to monitor the training intensity. During walking sessions, the exercise intensity was mainly set between low and moderate intensity (RPE: 9–13; %HRmax ⩽ 76%). If well tolerated, patients also performed at vigorous intensity (RPE: 14–17; %HRmax 77–90%). In patients taking beta-blockers, only the Borg’s scale was used to monitor the training intensity. The duration of each walking bout depends on the targeted exercise intensity and the induced pain intensity. In general, low-to-moderate intensity walking bouts were 5–10 minutes in duration and allowed the induction of moderate-to-severe claudication pain intensity,24,25 whereas moderate-to-vigorous intensity walking bouts were 1–4 minutes in duration.17,26 When patients performed vigorous intensity training, the duration of walking bouts must be shortened to ensure feasibility. Indeed, during vigorous-intensity exercise (which may be induced by higher walking speed), the claudication pain may rapidly appear. Moreover, exercise tolerance during vigorous intensity is generally lower compared to low-to-moderate training. Bout durations of between 1 and 4 minutes are also generally well accepted when performing vigorous-intensity training in patients with cardiovascular diseases.27,28
During one of three sessions per week, patients performed lower-limb strengthening using a circuit training approach. The latter was composed of five to six exercise stations that mainly focused on functional walking and balance exercises or lower-limb resistance exercises using body weight, elastic bands, or dumbbells.20 –23 In general, each exercise was composed of 15–30 repetitions, interspersed with 30–60 seconds of passive recovery. All sessions started with a 5–10-minute warm-up period involving walking and proprioceptive activities, coordination, and balance and ended with a 5-minute cool down.
During the SET program, patients received information on nutrition, physical activity, tobacco use, and cardiovascular risk factors during a total of 6 hours of structured therapeutic education workshops.
The number of patients having sufficiently adhered to the treatment protocol, such as completing a minimum of 80% of sessions over 12 weeks (29 of 36), was also reported.
Assessments
Functional evaluation was performed before SET (before the first training session), after the first (between 10 and 14 completed sessions) and second (between 22 and 26 completed sessions) months of SET, and following the SET program (after the last training session). Patients were asked to avoid vigorous exercise 24 hours before the tests. Except for the before SET program condition, assessments were performed at least 48 hours following the last training session. Tests were performed on the same day and time and always in the following order: (1) 6-minute walk test (6MWT); (2) stair climbing test (SCT); (3) Short Physical Performance Battery (SPPB); (4) maximal walking speed test; and (5) unipedal stance time test. Patients were allowed to rest for 5 to 15 minutes between each functional test. The test administrator had 8 years of experience in exercise testing in these patients.
Six-minute walk test (6MWT)
Before the test, patients rested for 15 minutes. Subsequently, patients were asked to walk up and down an indoor 50-meter corridor after receiving instructions to cover as much distance as possible within 6 minutes to determine the 6-minute walking distance (6MWD). Patients were instructed to perform the test in accordance with the guidelines. 29 Standard phrases of encouragement were used during the test. 29
Stair climbing test
Patients were asked to climb a 12-stair flight of stairs as quickly as possible. 30 The stopwatch was stopped when both of the patient’s feet reached the 12th stair. For safety issues, the use of the handrail was allowed. The test was performed twice, and the average was considered for analyses. 30
Short Physical Performance Battery (SPPB)
The SPPB is composed of standing balance, habitual gait speed, and the sit-to-stand (STS) chair test. 14 First, patients were asked to hold three balance positions for 10 seconds each: side-by-side (feet together), semi-tandem (heel of one foot against side of big toe of the other), and tandem standing positions (feet aligned heel to toe). Second, patients performed a 4-meter walking test to assess their habitual gait speed. The stopwatch was stopped when one of the patient’s feet completely crossed the 4-meter line. The best time of two repetitions was considered. 14 Third, patients performed the STS chair test. From a sitting position, patients were asked to stand five times as quickly as possible on an armless chair. Each SPPB test has a score from 0 (worst) to 4 (best), with a maximal performance score of 12. 14 Relative STS muscle power was estimated from the STS time performance, as described elsewhere.20,31 Similar to the habitual gait speed test, patients also performed a 4-meter walking test to assess the maximal walking speed.
Unipedal stance time test
Patients performed a unipedal stance test. Patients were asked to hold this balance position for a maximum of 60 seconds on both legs. The unipedal stance time performance was recorded until the position could no longer be maintained.
Physical characteristics and vascular parameters
Prior to and following the SET program, a thorough medical history was assessed. Body mass index (BMI), resting ABI, and toe–brachial index (TBI) were also recorded. 32
Statistical analysis
First, statistical (Kolmogorov-Smirnov) and visual inspection of the normality of the distribution was performed. Thereafter, linear mixed models (LMMs) were used to investigate the time-course evolution (before SET, after the first and second months of SET, and following the SET program) of functional performance during the SET program. LMMs (group [low-to-moderate vs vigorous exercise intensity] × time [before SET, after the first and second months of SET, and following the SET program]) were also performed in a subanalysis aiming to compare the trajectory of functional performance during the SET program in patients performing low-to-moderate and vigorous exercise intensity. Using simple linear regressions, the influence of covariates, such as age, sex, and diabetes, was assessed. If linear regressions revealed significant influence, the covariate(s) were added in the LMMs. LMMs were also used to investigate the effects of the SET program on physical characteristics and vascular parameters. When LMMs showed a significant main time effect, multiple comparisons with Bonferroni adjustment were used to determine the difference.
The level of significance was set at p ⩽ 0.05.
All statistical analyses were performed with IBM SPSS Statistics 27 software (IBM Corp., Armonk, NY, USA).
Results
Participants
Ninety patients with chronic symptomatic PAD were included in the study (Table 1). Overall, the attendance rate of the SET program was 29.2 (range: 1–36) training sessions (81.2%). Twenty patients (22%) did not complete the SET program and have a mean number of training sessions completed of 9.6 (range: 1–23). Notably, 12 patients who dropped out performed between 1 and 12 sessions, four patients performed between 15 and 17 sessions, and four patients performed between 21 and 23 sessions. The reasons for an uncompleted SET program were endovascular revascularization during the SET program (n = 4), progression of symptoms (n = 3), incompatible schedule with work (n = 1), anxiety related to the pandemic period (n = 2), patient’s choice to withdraw (n = 5), and other comorbidities and other reasons not related to the SET program (n = 5). The remaining 70 patients had a training protocol adherence similar or greater than 80% over 12 weeks.
Baseline characteristics of the participants.
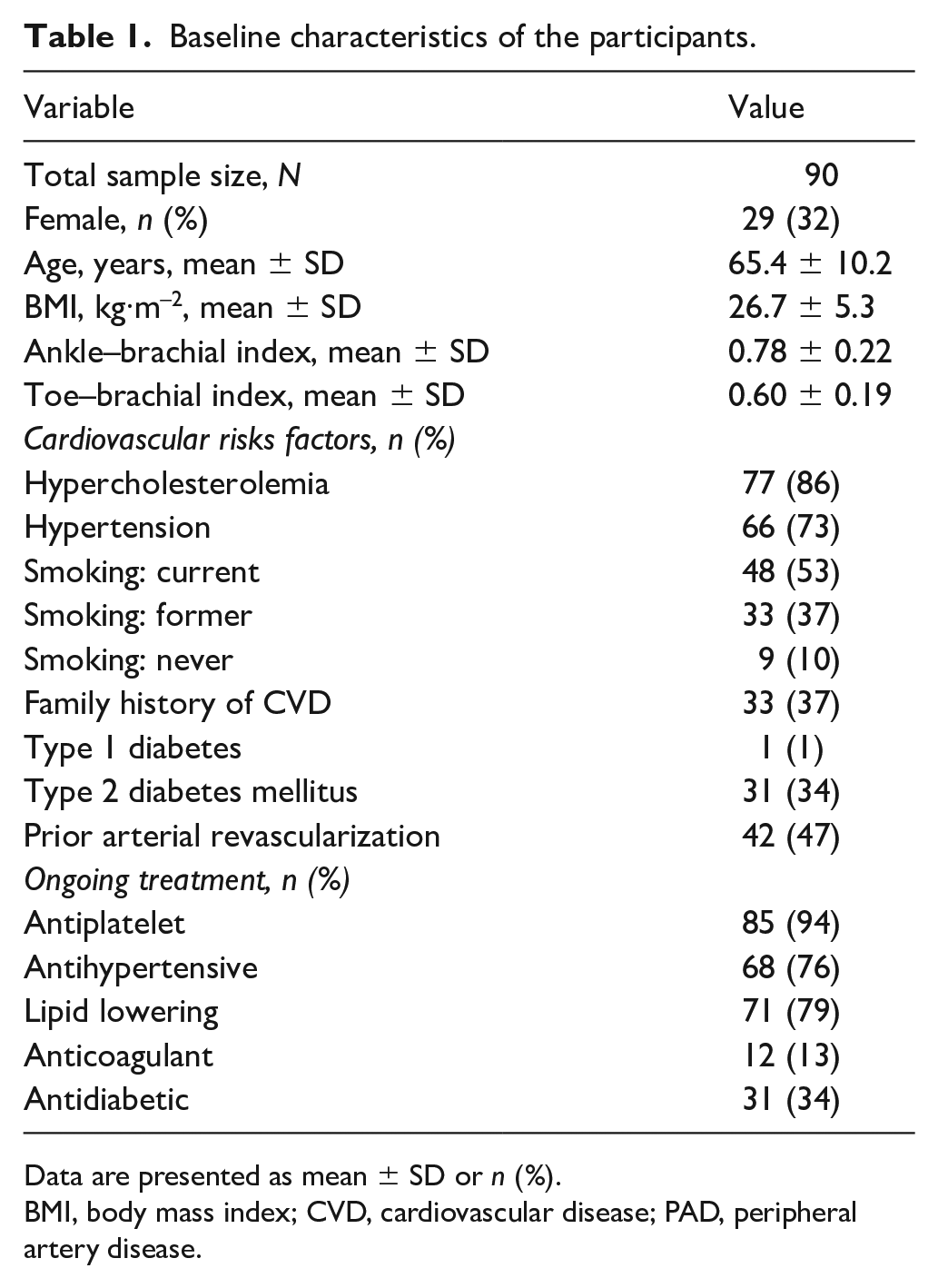
Data are presented as mean ± SD or n (%).
BMI, body mass index; CVD, cardiovascular disease; PAD, peripheral artery disease.
The pharmacological therapy provided before and after the SET program was similar for each patient, except four patients started statin therapy during the SET program; two patients stopped receiving antihypertensive therapy and one patient started antihypertensive therapy; and one patient stopped receiving antiplatelet therapy. During the SET program, three patients resumed smoking and two patients stopped smoking.
Seventy patients performed the SET program at a low-to-moderate exercise intensity, whereas only 20 patients (22%) were able to achieve vigorous exercise intensity during the second and/or 3rd month of the SET program. To note, vigorous-intensity exercise sessions were mainly performed once weekly.
Functional performance during the SET program
Six-minute walk test
There was a significant time effect for the 6MWD (Table 2). Multiple comparison analyses showed significant improvements after the first and second months and following SET when compared to before the SET program (Table 2). The 6MWD was significantly improved after the second month and following SET compared to the first month of the SET program (Table 2). No significant difference was observed following SET when compared to the second month of the SET program (Table 2).
Time-course evolution of functional performance during the supervised exercise training (SET) program.
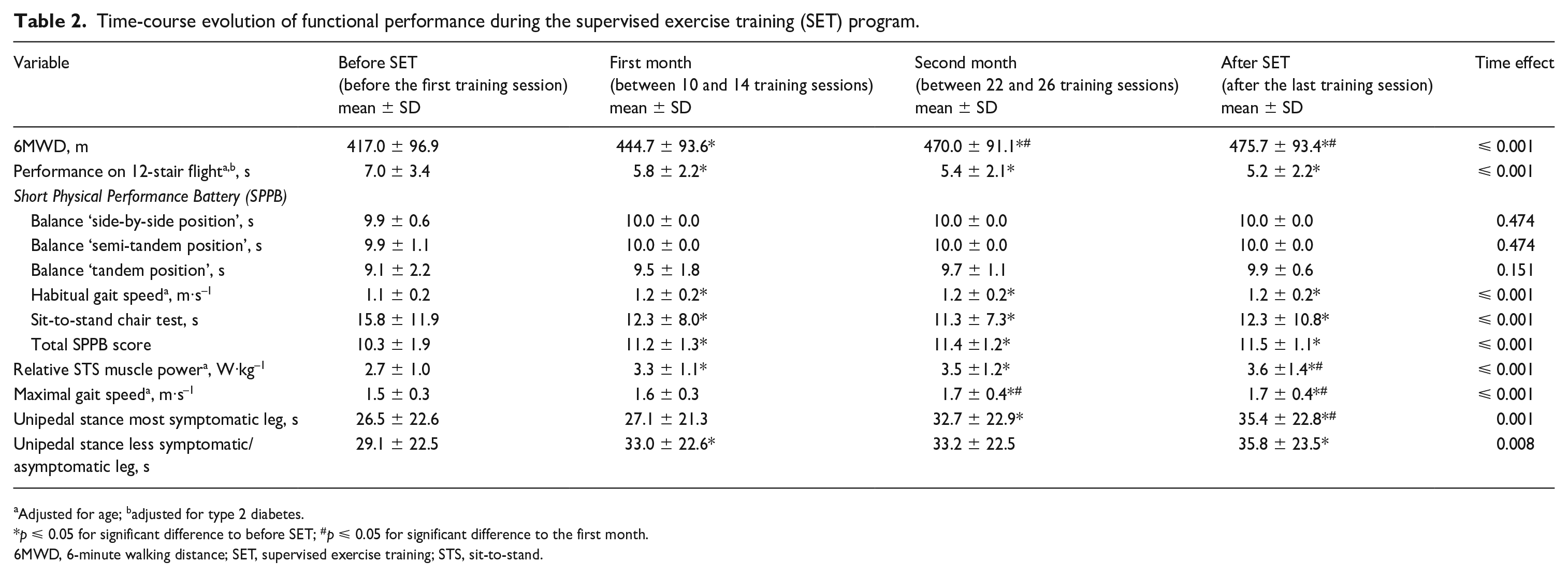
Adjusted for age; badjusted for type 2 diabetes.
p ⩽ 0.05 for significant difference to before SET; #p ⩽ 0.05 for significant difference to the first month.
6MWD, 6-minute walking distance; SET, supervised exercise training; STS, sit-to-stand.
Stair climbing test
There was a significant time effect on performance of the 12-stair flight (Table 2). Multiple comparison analyses showed a significantly improved performance after the first and second months and following SET when compared to before the SET program (Table 2). No significant differences were observed after the second month and following SET when compared to the first month of the SET program (Table 2). No significant difference was observed following SET when compared to the second month of the SET program (Table 2).
Short Physical Performance Battery (SPPB)
No significant changes were observed for the balance assessed in side-by-side, semi-tandem, and tandem positions (Table 2). There was a significant time effect for the habitual gait speed, STS chair test, and SPPB total score (Table 2). Multiple comparison analyses revealed significant improvements after the first and second months and following SET when compared to before the SET program (Table 2). No significant differences were observed after the second month and following SET when compared to the first month of the SET program (Table 2). No significant difference was observed following SET when compared to the second month of the SET program (Table 2). There was a significant time effect for the relative STS muscle power (Table 2). Multiple comparison analyses showed significantly improved muscle power after the first and second months and following SET compared to before the SET program (Table 2). Significantly greater muscle power was observed following SET when compared to the first month of the SET program (Table 2). No significant difference was observed following SET when compared to the second month of the SET program (Table 2).
Maximal walking speed test
There was a significant time effect for the maximal walking speed (Table 2). Multiple comparison analyses showed a significant improvement after the second month and following SET when compared to before SET and to the first month of the SET program (Table 2). No significant difference was observed following SET when compared to the second month of the SET program (Table 2).
Unipedal stance test
There was a significant time effect for unipedal stance performance (Table 2). Multiple comparison analyses in the most symptomatic leg showed a significantly improved performance after the second month and following SET when compared to before the SET program (Table 2). Additionally, a significantly improved performance was observed following SET when compared to the first month of the SET program (Table 2). Multiple comparison analyses in the less symptomatic/asymptomatic leg revealed a significantly improved performance after the first month and after SET when compared to before the SET program (Table 2). For both legs, no significant differences were observed following SET when compared to the second month of the SET program (Table 2).
Subanalysis of low-to-moderate versus vigorous exercise intensity
There was a significant group effect for all the different components of the functional performance, except for the balance in side-by-side and semi-tandem positions (online Supplemental Table). As expected, the group also performing vigorous exercise intensity presents greater functional performance (online Supplemental Table). There was a significant time effect for the 6MWD, performance on the 12-stair flight, habitual and maximal gait speed, sit-to-stand chair test, relative STS muscle power, and total SPPB score (online Supplemental Table). Multiple comparison analyses revealed that the improvements mainly occurred during the first and second months of the SET program (online Supplemental Table). However, there was no significant group × time interaction effect, indicating that both groups have similar changes in functional performance during the SET program (online Supplemental Table).
Physical characteristics and vascular parameters
BMI (before: 26.7 ± 5.3 kg·m–1; after: 27.1 ± 5.6 kg·m–1; p = 0.647), ABI (before: 0.78 ± 0.22; after: 0.79 ± 0.17; p = 0.989), and TBI (before: 0.60 ± 0.19; after: 0.61 ± 0.17; p = 0.451) remained unchanged following the SET program.
Discussion
The main findings of the present investigation showed that a 3-month multimodal SET program induces significant improvements in different components of functional performance, such as functional overground walking, standing balance, and muscle function, in patients with chronic symptomatic PAD. These improvements mainly occurred during the first and second months of the SET program, with no additional significant benefits in the 3rd month of intervention.
Exercise interventions in patients with PAD aim to improve walking performance (mostly assessed on a treadmill) and quality of life and to decrease symptoms and cardiovascular risk. However, very few PAD trials have focused on the effects of the SET program on several components of functional performance, and the results are inconsistent. 19 Indeed, some previous studies reported no differences in SPPB total score following traditional supervised treadmill or resistance training,33,34 yet others observed significant improvements following programs in which patients performed a wide spectrum of functional exercises.35,36 In the present investigation, patients performed a multimodal SET program focused on the main functional limitations previously observed in patients with PAD (such as overground walking, static and dynamic balance, and muscle strength/power), and the results showed that the multimodal SET program was effective in improving several components of functional performance. Although the present investigation cannot discern whether our multimodal SET program is superior to the traditional treadmill training generally used in patients with PAD, the exercises performed during the multimodal SET program (lower-limb strengthening and Nordic walking) are representative of daily-life activities and may therefore lead to better improvements in overall functional status. Our findings also showed that monthly adaptations of functional performance during a 3-month SET program mainly occur during the first and second months of the SET program. Interestingly, no further significant benefits were observed after the 3rd month of intervention. Additionally, changes in functional performance were similar in patients who performed low-to-moderate and vigorous exercise intensity. These results are in line with previous findings showing that during a SET program, improvements in treadmill performance occur rapidly after 2 months of the SET program and extend to different components of functional performance. 37 Notably, we observed a 28-meter increase (from 417.0 to 444.7 m) in the 6MWD after the first month of the SET program, which is larger than the minimal clinically important difference (MCID) for large improvements in patients with symptomatic PAD. 38 Additionally, a more than 50-meter increase (from 417.0 to 470.0 m) in the 6MWD was observed after the second month of the SET program, which is greater than the minimal detectable change (⩾ 46 m). 39 Similarly, the improvements in the habitual gait speed rapidly observed after the first month of the SET program (from 1.10 to 1.20 m·s–1) are larger than the MCID for substantial improvements observed after the SET program (+0.08 m·s–1). 40 Finally, the improvements in the SPPB total score after the first month of the SET program (from 10.3 to 11.2 points) are similar to the MCID for small to substantial changes observed in community-dwelling older adults. 41 Taken together, the results of the present investigation suggest that functional exercises should be implemented in training programs in patients with PAD with regard to optimizing functional performance and inducing rapid changes in these patients.
From a clinical standpoint, these results lead to interesting perspectives. First, performing a monthly assessment of functional performance during training programs could be useful not only in monitoring the timeline of training adaptations but also in improving training guidance and individualization during the SET program. Second, because we observed no significant additional benefits during the 3rd month of the SET program, changes in the training parameters in the last part of the SET program should be considered to further increase benefits, such as increasing the training frequency, volume (minutes per week), training load, or exercise intensity (e.g., high-intensity). It is possible that the lack of difference observed in the subanalysis was related to the relatively low dose of vigorous exercise intensity (i.e., once weekly). Therefore, this needs to be adequately investigated in the future. Also, refining the exercise training in the last part of the SET program may allow patients to explore different training approaches and, subsequently, may help them to achieve lifelong exercise. Therefore, the monthly assessment of functional performance during the SET program should be considered as a unique opportunity to teach tools aiming to promote and sustain high levels of physical activity following training interventions.
Study limitations
Some limitations exist. First, this study lacks a nonexercising control group. Second, the included patients presented moderately high levels of baseline functional performance, suggesting that these results may not be generalized to patients with severe PAD. Third, in the present investigation, patients performed a multimodal SET program combining the different training modalities. Therefore, these results may not be generalized to the most common treadmill programs usually performed by these patients. 25 Future investigations are needed to assess the time-course evolution of functional performance during a traditional treadmill exercise program. Fourth, although not significant, our results showed that after the 3rd month of the SET program some additional benefits were observed (Table 2). In this context, the time-course evolution of functional performance in longer (⩾ 6 months) training programs remains to be investigated. Fifth, 22% of the included patients failed to complete the training program, leading to missing data during and following the SET program. Notably, this high rate of noncompleters and the related reasons observed in this present investigation are similar to previous findings in patients with PAD. 42 Sixth, although the SET program used RPE and HR as a clinical tool to guide the exercise intensity during the training sessions, these data were not systematically recorded after each session. Therefore, it was not possible to fully evaluate treatment fidelity.
Conclusion
Results presented herein showed that a 3-month multimodal SET program improves different components of functional performance and that adaptations mainly occur during the first and second months of the SET program.
Supplemental Material
sj-pdf-1-vmj-10.1177_1358863X231191908 – Supplemental material for Time-course evolution of functional performance during a 3-month supervised exercise training program in patients with symptomatic peripheral artery disease
Supplemental material, sj-pdf-1-vmj-10.1177_1358863X231191908 for Time-course evolution of functional performance during a 3-month supervised exercise training program in patients with symptomatic peripheral artery disease by Stefano Lanzi, Anina Pousaz, Luca Calanca and Lucia Mazzolai in Vascular Medicine
Footnotes
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Supplementary material
The supplementary material is available online with the article.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.