
Abstract

What is cervical artery dissection (CeAD)?
Cervical artery dissection (CeAD) has been recognized as a common cause of stroke in younger adults, such as those less than 50 years of age. A CeAD occurs when there is a tear in the inner layer of one of the major arteries of the neck that supplies blood flow to the brain. When this tear occurs, a blood clot forms within the artery wall, called an ‘intramural hematoma’. Pieces of blood clot that form where the artery tears can break off and travel up to the brain (known as an embolism) or the blood clot can expand and narrow the artery, which restricts blood flow to the brain. When this happens the patient with CeAD can experience symptoms (see below). In some cases, CeAD can lead to complete blockage of an artery to the brain (known as an artery occlusion). CeAD may also damage the nerves around the arteries, which can cause face or neck pain, drooping of an eyelid, or differences in the size of the pupils in the eyes.
CeAD may involve the carotid or vertebral arteries, which are the main vessels in the neck that supply blood from the heart to the brain. The body has two common carotid arteries that run along both sides of the neck. These common arteries branch into the internal and external carotid arteries (Figure 1). The internal carotid arteries, one on each side of the neck, deliver blood up to the brain, whereas the external carotid arteries deliver blood to the muscles of the head, neck, and face through a network of branches. The two vertebral arteries run along the back of the neck within the bones of the cervical spine to deliver blood from the heart to the brain. CeAD more commonly involves in the internal carotid arteries than the vertebral arteries. 1 However, dissection may occur in any of these four major arteries (two internal carotid and two vertebral arteries), and multiple arteries can have dissections at or around the same time.
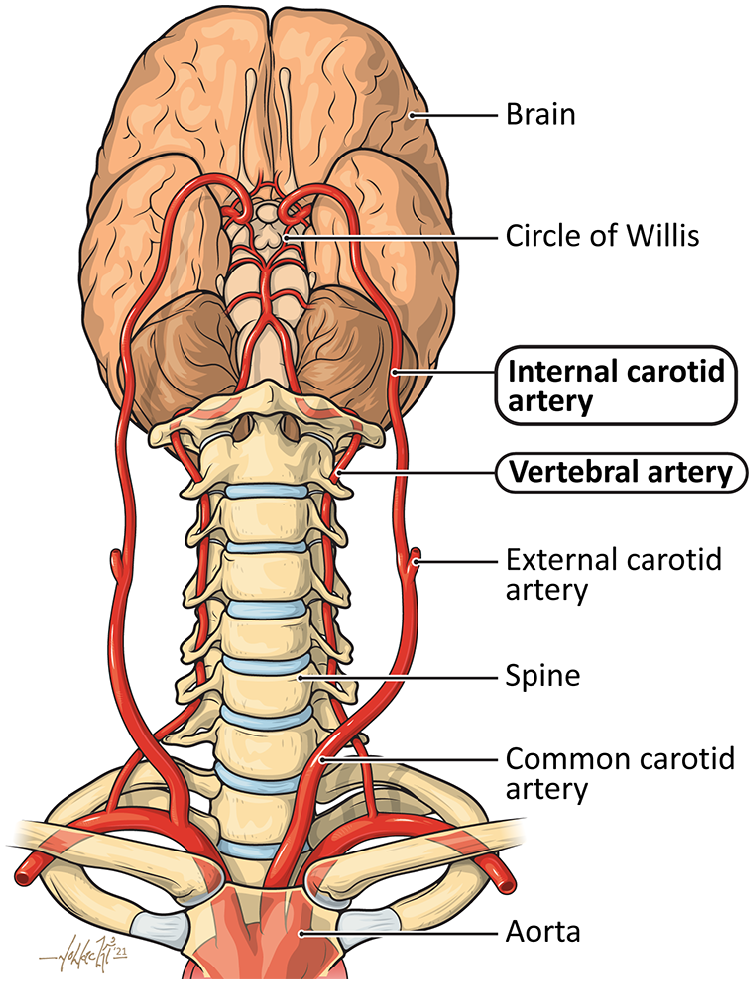
Anatomy of the cervical arteries. The two internal carotid arteries and two vertebral arteries supply blood flow to the brain and are the vessels involved in cervical artery dissection.
What are the symptoms of a CeAD?
The most common symptoms associated with CeAD are:
Headache
Neck and/or ear pain, sometimes with tenderness to touch
Whooshing sound in one or both ears that times with the heartbeat (pulsatile tinnitus)
Drooping of the lid of one of the eyes and uneven pupils (Horner’s syndrome)
Symptoms of stroke (sudden deficit in neurologic function caused by an injury to the brain related to lack of blood flow) or TIA (transient ischemic attack; stroke symptoms that only last a short period of time and resolve suddenly). Symptoms of stroke or TIA can include:
– Weakness or numbness of the face, arm, or leg on one side
– Slurred speech or difficulty getting words out
– Double vision or visual loss
– Problems with coordination or difficulty walking.
Symptoms of CeAD vary depending on which artery is involved and which side of the brain it is supplying, whether an embolism has occurred, and the severity of narrowing of the artery.
What causes CeAD?
CeAD can occur due to trauma, such as after a car accident or neck injury, but more often occur spontaneously or with minor neck exertion. When CeAD occurs spontaneously, an inherited or underlying medical condition may have led to weakening of the arteries, making them more susceptible to a dissection. These conditions include vascular connective tissue disorders such as Ehlers–Danlos, Loeys–Dietz, or Marfan syndromes, as well as other vascular diseases that may weaken the artery wall, such as fibromuscular dysplasia (FMD). 2 Recent research has shown that up to 40% of patients with CeAD have underlying FMD. 3 Other genetic factors may be associated with risk of CeAD, such as a variant in a common gene called PHACTR1. 4 Understanding the genetics of CeAD is an ongoing area of international research collaborations, including the CADISP-Plus consortium (www.cadisp.com).
Patients with CeAD often report having done a specific activity that may have put pressure or mechanical strain on the blood vessels of the neck in the hours or days prior to the onset of symptoms. These activities may include turning the neck to the side too quickly or hyperextending the neck by leaning the neck back too far or too quickly. These motions may happen with lifting heavy objects, in violent fits of coughing or with vomiting. Jerking head motions may also occur during chiropractic neck adjustments or on waterslides or rollercoaster rides. 5 Some patients with CeAD have reported a recent illness, such as a virus. 1 High blood pressure, especially if uncontrolled, is also a risk factor for CeAD.1,6
How is CeAD diagnosed?
When CeAD is suspected, the first step in diagnosis is noninvasive imaging. Computed tomographic angiography (CTA) or magnetic resonance angiography (MRA) is typically used to establish the diagnosis. CTA is more frequently used as it is widely available at most medical facilities and provides the best detailed imaging of the blood vessels. During CTA, a special iodine-containing contrast dye is injected into the patient’s blood vessels through an intravenous (IV) line while multiple X-ray type images are taken during the CTA. CTA images allow physicians to visualize blood vessels in detail in three-dimensions and can show dissection flaps (tears) in the internal carotid or vertebral arteries, thickening of the artery walls due to the intramural hematoma (blood clot), and irregular narrowing or occlusion of the blood vessels. MRA may also be used to diagnose CeAD. MRA is performed with or without a special IV contrast agent and uses a magnetic field to image the blood vessels. Magnetic resonance imaging (MRI) of the brain can be done at the time of the MRA to evaluate the brain in detail and assess for areas of stroke due to CeAD. Duplex ultrasound, which is another noninvasive test to assess the carotid arteries, is generally not adequate to diagnose CeAD as it has limited ability to image the internal carotid arteries high in the neck or the vertebral arteries which run along the spine. To learn more about imaging studies for the diagnosis of vascular disease, read the Vascular Disease Patient Information Page on Advanced Vascular Imaging. 7
In some cases, catheter angiography is required to confirm the diagnosis of CeAD, but generally only when the diagnosis is uncertain after CTA and/or MRA and when further intervention is required for severe symptoms (see below). Catheter angiography is a minimally invasive procedure during which X-ray pictures are taken while contrast dye is directly injected into arteries from a catheter inserted in the groin or arm (Figure 2).
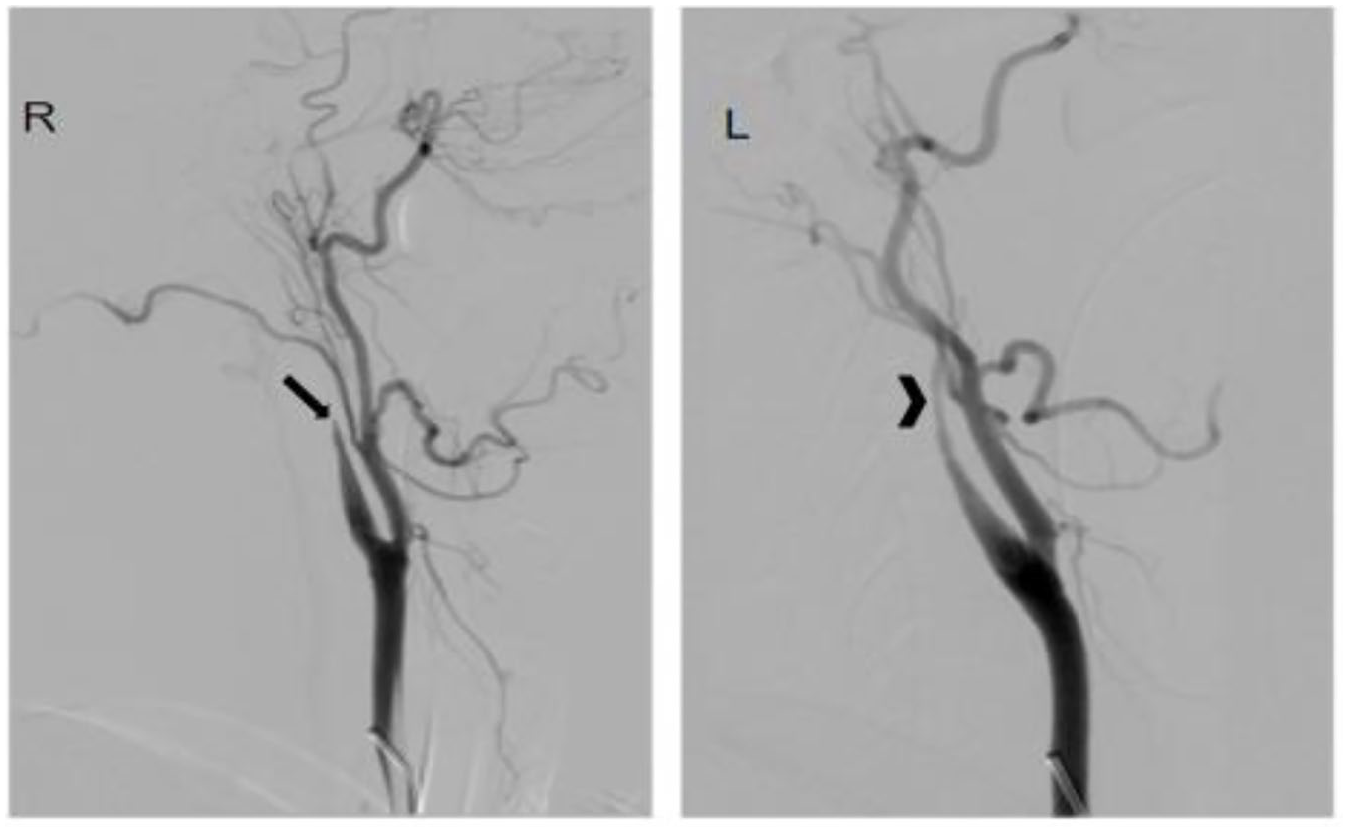
Catheter angiogram of cervical artery dissection. This patient had a severe headache, confusion, and personality changes. She was found to have had a stroke and two internal carotid artery dissections with right internal carotid artery occlusion (arrow) and severe left internal carotid artery stenosis (arrowhead).
How is CeAD treated?
Initial treatment
When a patient is diagnosed with CeAD, the primary goals of treatment are to prevent stroke and to manage symptoms. Antiplatelet and anticoagulant blood-thinning medications are the initial treatment for CeAD to minimize blood clot formation and embolization. Antiplatelet blood-thinning medications may be prescribed as single agents (aspirin or clopidogrel alone) or in combination. Some patients with CeAD may need an anticoagulant blood thinner, such as heparin (either IV or in an injection form called low molecular weight heparin). For some patients, an oral blood thinner, such as warfarin, or a direct oral anticoagulant (DOAC), may be prescribed. 8 Recent research studies comparing antiplatelet versus anticoagulant blood thinners for CeAD have been inconclusive. 9 Thus, the choice of antiplatelet or anticoagulant medication is made on a case-by-case basis depending on the nature and location of the dissection(s), associated medical conditions, and the risk of bleeding.
Most patients with CeAD do well when treated with medications only. However, if a patient with CeAD has a stroke or TIA despite being on blood thinners, or if blood flow to the brain is not sufficient due to severe artery narrowing, then additional procedures may be necessary. These procedures use catheter-based techniques, such as balloon angioplasty, to restore blood flow to severely blocked arteries. After blood flow is restored, a metallic stent may be placed to hold the artery open and maintain blood flow. In cases of CeAD causing disabling acute ischemic stroke, clot busting medications, such as tissue plasminogen activator (tPA) or tenecteplase (TNK), or a clot removal procedure (thrombectomy) may be used to break up or take out blood clots to restore blood flow to the brain.
Patients with CeAD also often need medications to control high blood pressure, headaches, or neck pain, especially after the initial event.
Long-term treatment
Once the patient recovers from the initial CeAD, the goals of treatment are to prevent a stroke, prevent recurrent dissection(s), and manage symptoms. Patients with CeAD will be discharged from the hospital on a blood-thinning medication (antiplatelet or anticoagulant) and will have scheduled follow-up with a neurologist or other vascular specialist who has experience caring for patients with CeAD. Patients who have had a stroke due to CeAD may require referral for physical and occupational therapy to help with recovery of function. Good control of blood pressure is important, and patients may be discharged with blood pressure medications and a cuff for home blood pressure monitoring.
Following CeAD, the arteries to the brain are generally monitored with repeated imaging studies (CTA or MRA) over time for healing of the vessel(s). In many cases, the artery heals almost completely back to normal, yet in other cases the artery may have residual (leftover) dissection that does not go away. Some patients with CeAD develop a ‘bulge’ in the artery at the site of the initial dissection, which is called a pseudoaneurysm (Figure 3). These pseudoaneurysms are usually located in the neck (not inside the brain) and they rarely grow or rupture, though they may require periodic monitoring.

CTA of cervical artery dissection (CeAD). This patient had a history of CeAD of both the right and left internal carotid arteries and had a left internal carotid artery pseudoaneurysm (arrow).
The neurologist or other vascular specialist will determine the frequency of follow-up imaging studies and the duration and type of blood-thinning medications. For most patients with CeAD, follow-up monitoring occurs over a period of years, although with much less frequent imaging studies beyond the first year after the event.
Residual headache and neck pain are common after CeAD, especially during the initial weeks and months after the event. Since another dissection may occur, patients with CeAD should report any new or worsening symptoms to their neurologist or vascular specialist. Many patients with CeAD also have migraine headaches, sometimes with associated neurological symptoms such as cognitive fogging, blurry vision, numbness and tingling, and dizziness. Medications can help alleviate neck pain, headaches, and sensory disturbances related to CeAD. Fortunately, the pain usually improves and often resolves over time. Some patients with Horner’s syndrome due to CeAD have unequal pupils or drooping of an eyelid that does not resolve.
Is additional testing needed to figure out the cause of CeAD?
Many factors can increase the risk of CeAD, including the vascular disease FMD and genetic vascular connective tissue disorders, as well as controllable risk factors such as high blood pressure and tobacco smoking.2,3,6
For some patients with no clear cause or risk factors for CeAD, a medical genetics evaluation may be recommended to test for known vascular connective tissue disorders and help counsel about the risk for family members. Genetic testing may not be necessary for all patients but may be recommended for those with certain traits or physical characteristics, those who have a strong family history of aneurysms or dissections, and those with multiple dissections. Noninvasive imaging of the arteries of the body below the neck may be recommended, such as a CTA of the chest, abdomen, and pelvis, to evaluate for FMD and aneurysms and dissections in other areas.2,3
How can another CeAD be prevented?
Patients with CeAD may be at risk for another event, particularly in the first few days or weeks after the initial CeAD. 10 Therefore, patients must be aware of the signs and symptoms of stroke and CeAD and seek emergency medical care for any new or recurrent neurological symptoms or worsening headaches or neck pain. Active monitoring and control of high blood pressure is also particularly important for this reason.
After CeAD, patients should avoid high-risk activities such as heavy lifting, contact sports or martial arts, high-intensity exercise, rollercoasters, and chiropractic neck adjustments or other neck manipulation. 5 Taking medications as prescribed, controlling blood pressure, and remaining tobacco-free will also help prevent recurrence in the long-term. Patients should have a discussion with their neurologist or other vascular specialist before engaging in high-intensity exercise or activities, although most patients are able to resume normal daily activities once their dissection has healed. Fortunately, longitudinal studies of patients with CeAD suggest the long-term risk of recurrent dissection is low. 10 Women considering pregnancy should discuss family plans in detail with their health care team.
Conclusion
Cervical artery dissection (CeAD) involving the carotid and/or vertebral arteries is a cause of stroke in younger patients but can also cause less severe symptoms, such as headache and neck pain. CeAD is diagnosed with noninvasive imaging studies and is generally treated with medication and time to allow the artery to heal, although in rare instances patients may require catheter-based procedures including stenting. Patients are at the highest risk for stroke and recurrent dissection early after the initial CeAD, but this risk decreases over time. CeAD patients should be evaluated for signs of a genetic vascular connective tissue disorder or other vascular disorders, such as FMD. Management of risk factors, especially high blood pressure, and moderating certain physical activities that involve heavy lifting or put strain on the neck, are important to prevent recurrent CeAD.
Footnotes
Declaration of conflicting interests
The authors declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: Dr Gornik is a member of the Medical Advisory Board of the FMD Society of America, a nonprofit organization. Dr Sharma has received research funding from Vascular Medcure and serves as a consultant to Boston Scientific Corporation for creation of education content for chronic deep vein disease. Dr Southerland is an expert legal consultant for cases related to cervical artery dissection and stroke. Ms Stimach has nothing to disclose.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.