
Abstract
This article is a comprehensive document on the diagnosis and management of fibromuscular dysplasia (FMD), which was commissioned by the working group ‘Hypertension and the Kidney’ of the European Society of Hypertension (ESH) and the Society for Vascular Medicine (SVM). This document updates previous consensus documents/scientific statements on FMD published in 2014 with full harmonization of the position of European and US experts. In addition to practical consensus-based clinical recommendations, including a consensus protocol for catheter-based angiography and percutaneous angioplasty for renal FMD, the document also includes the first analysis of the European/International FMD Registry and provides updated data from the US Registry for FMD. Finally, it provides insights on ongoing research programs and proposes future research directions for understanding this multifaceted arterial disease.
Keywords
Introduction
Fibromuscular dysplasia (FMD) is a non-atherosclerotic arterial disease that is characterized by abnormal cellular proliferation and distorted architecture of the arterial wall. FMD primarily manifests as beaded (multifocal) or focal lesions in medium or small-sized arteries, though the clinical phenotype of FMD has recently been expanded to include arterial dissection, aneurysm, and tortuosity.1,2 FMD most commonly affects the renal and extracranial carotid and vertebral arteries, but nearly all arterial beds may be affected, and multivessel involvement is common. Approximately 80–90% of patients with FMD are women.2,3 Though less common, men also develop FMD and may have a more aggressive course with a higher frequency of aneurysms and dissections. 3 Though initially described in 1938 and classified according to angiographic and histopathological findings in the 1960s and 1970s, the greatest advances in the understanding of the pathophysiology and natural history of FMD have come in the past decade and have been driven by data from international patient registries and multicenter research collaborations.2,4 In 2014, multispecialty groups from Europe and the United States published consensus statements regarding FMD.5,6 Although these documents were developed independently, there were many similarities in interpretation of the medical literature and state of the clinical science – both documents representing initial attempts to develop a multispecialty consensus on a standardized approach to this disease.
Building upon the prior European and US documents, as well as international symposia held in Cleveland, Ohio, USA (May 18–19, 2017) and Brussels, Belgium (February 22–24, 2018), a writing committee was commissioned by the Society for Vascular Medicine (SVM) and the working group ‘Hypertension and the Kidney’ of the European Society for Hypertension (ESH) to create a single expert consensus document regarding FMD. The focus of this document will be review of new medical literature since the 2014 statements, summary of current international research efforts, and coordination of expert opinion into a single international expert consensus regarding the etiology, diagnostic approach, and management of FMD. A summary of consensus points, discussed throughout the document, is provided in Supplemental Table 1. Although there has been a recent expansion of published research in this field, including data from observational registries of patients with FMD, the authors acknowledge that level I data in this field are limited and the majority of points are based upon the expert consensus of the international panel of writing committee members. It is the intent of the writing committee that this international consensus document, including identification of research priorities, will lead to future high-quality research efforts, additional observational studies, and randomized controlled trials, and that these data will be incorporated into a future international guideline document.
Although the writing committee recognizes the importance of FMD as a cause of renovascular hypertension in children, the scope of this document is focused on FMD in adult patients. Writing committee members were selected by each society based upon extensive experience in the care of patients with FMD and/or research contributions to the field, including participation in international FMD registries. This document has been peer reviewed by members of both the ESH and SVM, and this final expert consensus has been endorsed by both the working group ‘Hypertension and the Kidney’ of the ESH and the Board of Trustees of the SVM.
Definition, classification, and differential diagnosis
Definition of FMD
The European consensus definition of FMD provides a baseline description of what constitutes FMD: An idiopathic, segmental, non-atherosclerotic and non-inflammatory disease of the musculature of arterial walls, leading to stenosis of small and medium-sized arteries. 6 Lesions of FMD can be either symptomatic or clinically silent and can be either hemodynamically significant or not. The diagnosis of FMD requires evaluation for other disease states on the differential diagnosis, such as arterial spasm, standing waves, atherosclerosis, and monogenic and inflammatory arterial diseases, among other entities which are discussed in detail below.
Classification of FMD
Although previously used, the consensus of this writing committee is that the histopathological classification of FMD is no longer applicable in modern clinical practice.7–9 FMD may result in two types of angiographic appearance (Figure 1): (1) focal FMD, which may occur in any part of the artery; or (2) multifocal FMD, alternating areas of stenosis and dilation (the so-called ‘string of beads’), which usually occurs in the mid and distal portions of the artery.5,10 This morphology most often occurs in the renal and carotid arteries but may occur in any artery in the body. 2 This classification of FMD does not refer to histology as tissue is rarely available since the advent of endovascular therapy. The 2014 AHA classification of FMD is similar to the 2014 European consensus document, though the two documents differ with respect to the use of the terms ‘focal FMD’ (AHA) or ‘unifocal FMD’ (European).5,6 This international consensus now recommends angiographic classification of FMD using the terms ‘focal FMD’ and ‘multifocal FMD’.
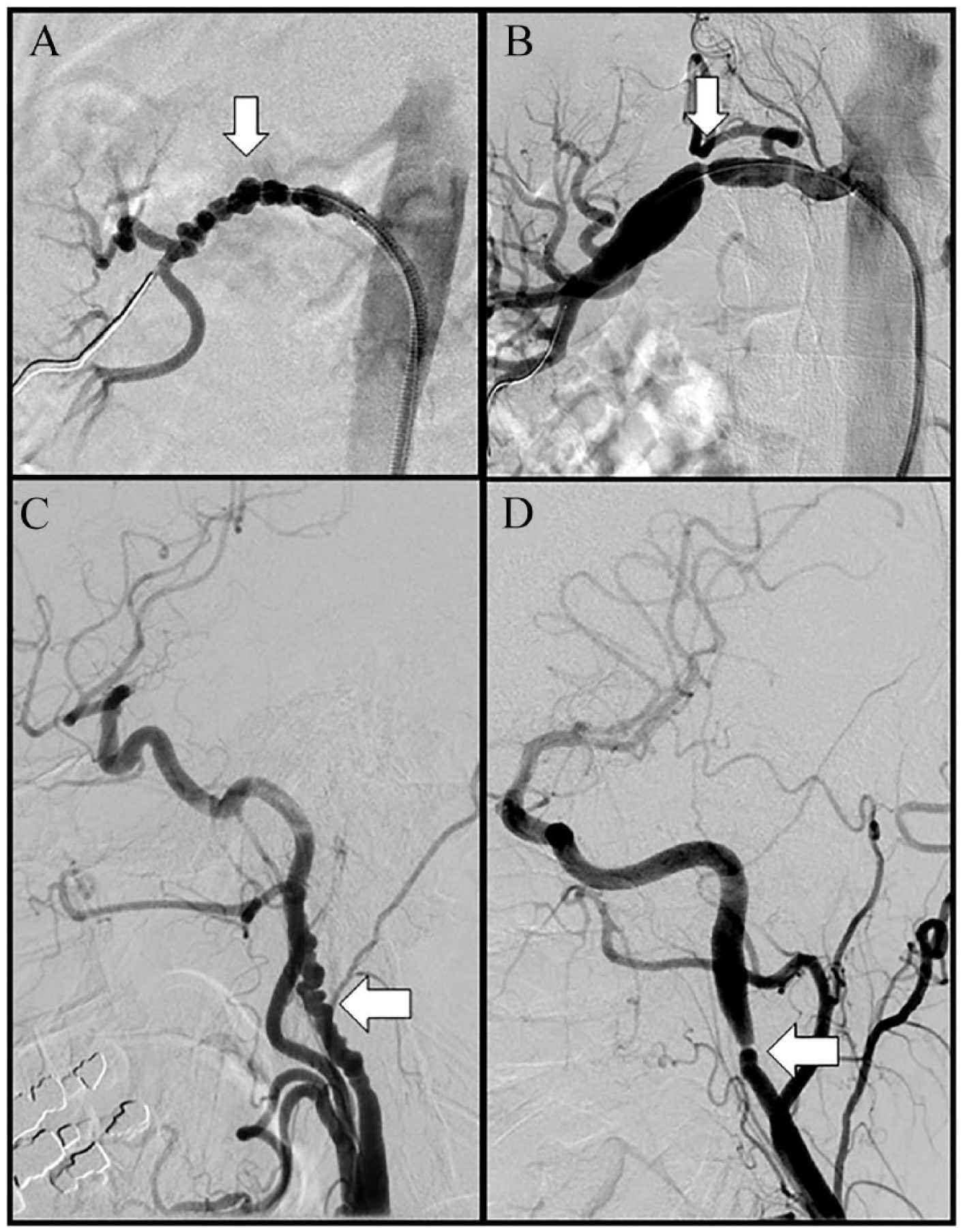
Angiographic images of multifocal and focal FMD of the renal and internal carotid arteries (arrows). (A) Multifocal FMD of the renal artery; (B) severe FMD-related focal stenosis of the renal artery with post-stenotic dilatation; (C) multifocal FMD of the internal carotid artery; (D) focal FMD of the internal carotid artery.
Stenosis, aneurysm, dissection, arterial tortuosity
FMD is primarily a stenotic disease (with lesions classified by angiographic appearance as above). It is also increasingly recognized that aneurysm, dissection, and arterial tortuosity occur with increased frequency in affected patients.1,11 Recent literature has suggested that arterial tortuosity occurs frequently among patients with FMD. 12 Tortuosity of the internal carotid artery (ICA) leading to an S-curve has been described among patients with FMD as a distinct morphological entity of the mid to distal portion of the ICA formed by an elongation causing two markedly tortuous turns in the shape of the letter ‘S’. 12 In one study, the S-curve was identified on carotid duplex ultrasound in 32% of patients with FMD of the renal, carotid, and/or vertebral arteries. 12 In addition to the S-curve, other manifestations of carotid and vertebral artery tortuosity have been described, though not specifically among patients with FMD.13–15 Tortuosity has also been reported in other arterial beds, including the coronary arteries. In a study from the Mayo Clinic, coronary tortuosity was defined by the presence of three or more consecutive curvatures of 90° to 180° measured at end-diastole in a major epicardial coronary artery ⩾ 2 mm in diameter. 16 Severe tortuosity was defined as two or more consecutive curvatures of ⩾ 180° in a major epicardial coronary artery ⩾ 2 mm in diameter. It was shown that there was a higher rate of recurrence of spontaneous coronary artery dissection (SCAD) among those patients with a high coronary tortuosity score. Other definitions of coronary artery tortuosity have been proposed.17,18
Nevertheless, it is important to recognize that the presence of aneurysms, dissections, or tortuosity in the absence of a focal or multifocal FMD stenotic lesion does not suffice to establish a diagnosis of FMD. Arterial aneurysm, dissection, and tortuosity are not unique to FMD and have been reported in multiple other vascular diseases.19,20 However, if the patient has a focal or multifocal FMD lesion in one vascular bed and a documented aneurysm, dissection, or tortuosity in another vascular bed, it is the consensus of the writing committee that the patient be considered to have FMD in the vascular bed with the focal or multifocal lesion, as well as FMD involvement of the vascular bed with aneurysm, dissection, or tortuosity (i.e. multivessel FMD).1,5 This point is of importance to allow for standardization of taxonomy in current FMD patient registries and future research studies.
Etiological factors and genetics of FMD
Although a variety of genetic, mechanical, and hormonal factors have been proposed, the cause of FMD remains poorly understood. The development of FMD is likely related to a combination of genetic and environmental factors. 21
Genetics of FMD
FMD appears to be both sporadic and familial in a subset of patients, with autosomal dominant inheritance suggested in some families.21,22 However, it is important to note that in modern Registry studies, only a minority of patients (1.9–7.3%) with FMD report an affected family member.2,4 Traditional family-based analyses have been hampered by the relatively low frequency of well-characterized multiplex pedigrees, incomplete penetrance (~0.5) and underdiagnosis of FMD, particularly of subclinical disease.22–25 Previous studies which assessed genes associated with other known arteriopathies, such as those underlying aortic aneurysm and dissection, have not identified any clear association patterns between these genes and FMD.26,27 Along with the high prevalence of asymptomatic FMD (~3–6%) and the influence of environmental modifiers (e.g. female hormones, lifetime mechanical stress, tobacco use), a complex genetic basis for FMD is suspected and provides a rationale for genetic association studies.4,28,29 A genome-wide association study identified a common genetic risk variant: a single nucleotide polymorphism (SNP) rs9349379-A, in the PHACTR1 locus (6p24), conferring an odds ratio (OR) of ~1.4 for FMD. 30 The risk variant resides within an intron of the PHACTR1 gene that is associated with PHACTR1 transcript expression levels in dermal fibroblasts and may have direct effects on vascular development when tested in a zebrafish model of gene expression knock-down. 30 Further data suggest that the same SNP is located at the site of an enhancer in aortic tissue and that it regulates endothelin-1 expression. 31 Endothelin-1 has pleiotropic vascular effects on vascular tone and arterial remodeling. Interestingly, the PHACTR1 FMD rs9349379-A risk-allele is associated with cervical artery dissection (CeAD), hypertension, and migraine headache, which belong to the spectrum of FMD-associated abnormalities but confers protection against atherosclerotic coronary artery disease, suggesting common underlying biology.32–37
Further genetic studies are needed in order to understand the role of genetic variation in the pathogenesis of FMD, and are underway. Knowledge of the genes underlying FMD will be needed for insight into the biology of FMD and to ultimately develop targeted therapeutic approaches. Further, knowing which genes are involved in FMD may be clinically useful to predict the risk of FMD in individuals, particularly in affected families. Ongoing research efforts are underway, including studies utilizing genome-wide association study methods (which will be best suited to identify common variants conferring risk to FMD under a model of complex genetic architecture) as well as whole exome sequencing and whole genome sequencing (which has the potential to identify rare and low frequency genetic variants with high impact).
Clinical signs of renal artery FMD.
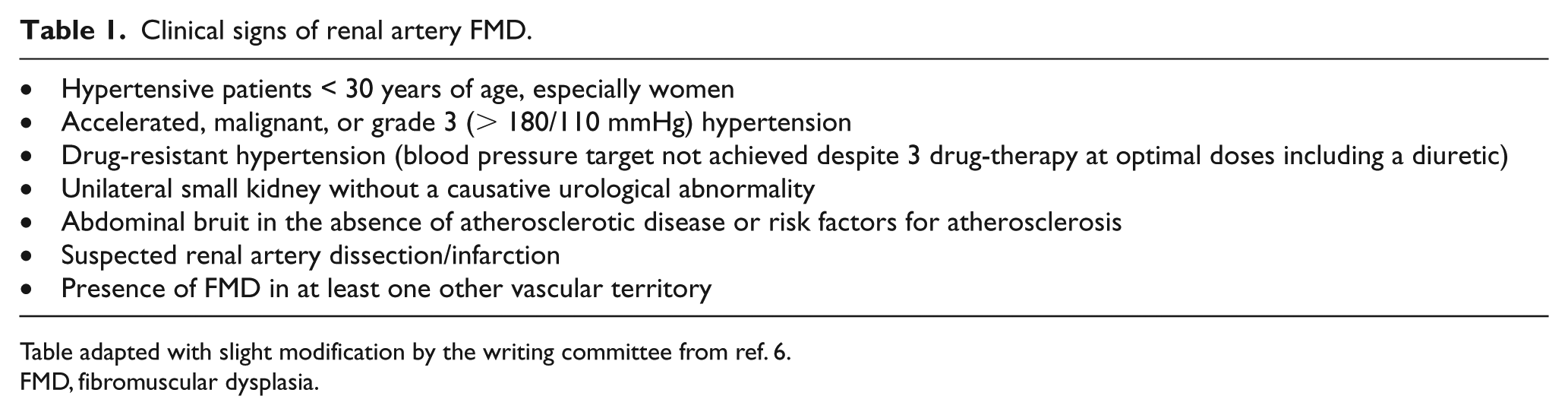
Table adapted with slight modification by the writing committee from ref. 6.
FMD, fibromuscular dysplasia.
Clinical signs/symptoms of cerebrovascular FMD.
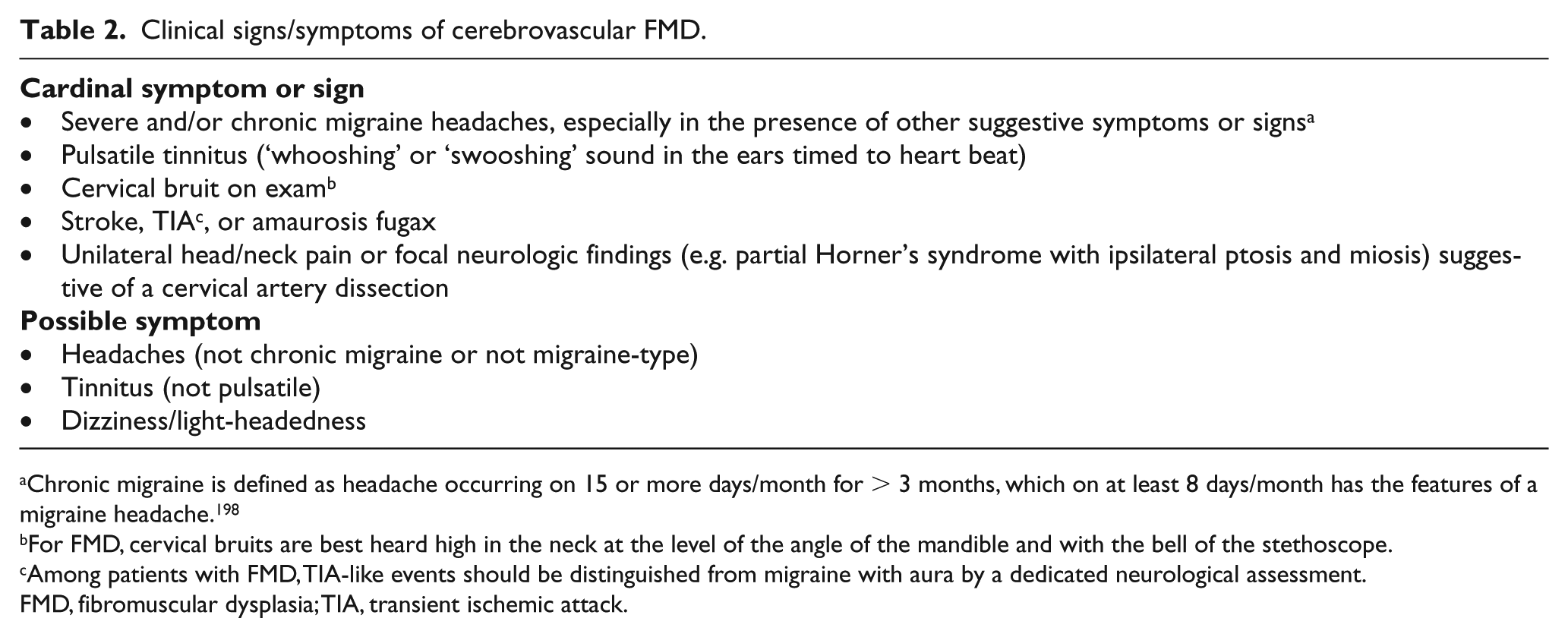
Chronic migraine is defined as headache occurring on 15 or more days/month for > 3 months, which on at least 8 days/month has the features of a migraine headache. 198
For FMD, cervical bruits are best heard high in the neck at the level of the angle of the mandible and with the bell of the stethoscope.
Among patients with FMD, TIA-like events should be distinguished from migraine with aura by a dedicated neurological assessment.
FMD, fibromuscular dysplasia; TIA, transient ischemic attack.
Environmental factors
Tobacco smoking has been identified as a potential pathogenic factor associated with FMD. Case–control studies have demonstrated an association of both current smoking (OR, 2.5–4.05) and ever smoking (OR, 1.8–4.1) and renal FMD.38–40 Among patients with multifocal FMD, current smokers experienced an earlier diagnosis of hypertension and FMD than non-smoking patients, and a greater likelihood of kidney asymmetry and further renal artery interventions. 40 In the US Registry for FMD, it was reported that patients with FMD with a history of smoking had a significantly higher rate of aneurysms than those who had never smoked and there was a trend toward increased prevalence of major vascular events in smokers. 41 Despite these data, smoking cannot be considered as a prerequisite for the development of FMD.5,41
Additional environmental factors, such as exposure to endogenous or exogenous female hormones, have also been associated with FMD, but the exact association remains unclear. Indeed, though the disease is far more prevalent in women than in men, no clear-cut causative link has been identified in those who have used oral contraceptives or other exogenous female hormones.3,39,42 A recent case–control histology study suggested abnormal balance between estrogen and progesterone receptors in renal artery samples of patients who underwent surgery for renal FMD, characterized by intense progesterone receptor expression in the nuclei of smooth muscle cells which was not found in the samples of control patients. 43 These preliminary findings suggests that progesterone may also play a role in the pathogenesis of FMD, but this needs to be replicated in other studies.
Repeated stretching of the renal artery due to kidney mobility (‘nephroptosis’) has also been associated with FMD, but the exact nature of this relationship remains unclear. 44 However, available data do not support a major contribution of renal mobility as an important exposure for the development of FMD. 39 Mechanical factors may contribute to the formation of FMD in certain arterial locations, including the right more than left renal, mid to distal internal carotid, and external iliac arteries, but specific mechanisms are currently unknown.
Other potential pathogenic factors
In a small cohort of patients with multifocal FMD, secretion of transforming growth factor (TGF)-β1 and TGF-β2 by dermal fibroblast cell lines was increased compared with matched controls. 27 In this study, FMD patients also had elevated plasma levels of circulating TGF-β1 and TGF-β2 relative to matched controls. The potential involvement of TGF-β pathways in the pathogenesis of FMD is an area for future investigation.
It has recently been suggested that accumulation of lysophosphatidylcholine (lysoPC), a pro-inflammatory and pro-apoptotic lipid mediator, in the visceral arteries may reflect predisposition for the development of aneurysms among patients with FMD. 45 Differences in the distribution patterns of lipid molecules, including cholesterol esters and lysoPC, between FMD-associated and atherosclerotic visceral artery aneurysms have been reported. 45
Differential diagnosis of FMD and overlapping entities
An understanding of the unique clinical and imaging findings in patients with FMD is paramount to distinguishing FMD from other arterial diseases. The differential diagnosis of FMD is broad, and includes many other arterial pathologies as well as imaging artifacts.46–58 The imaging diagnosis depends upon the finding of typical patterns of FMD (focal or multifocal lesions) as well as the presence of associated arterial findings (dissection, aneurysm, and tortuosity). Table 3 reviews key elements of the differential diagnosis of FMD.
Differential diagnosis of FMD.
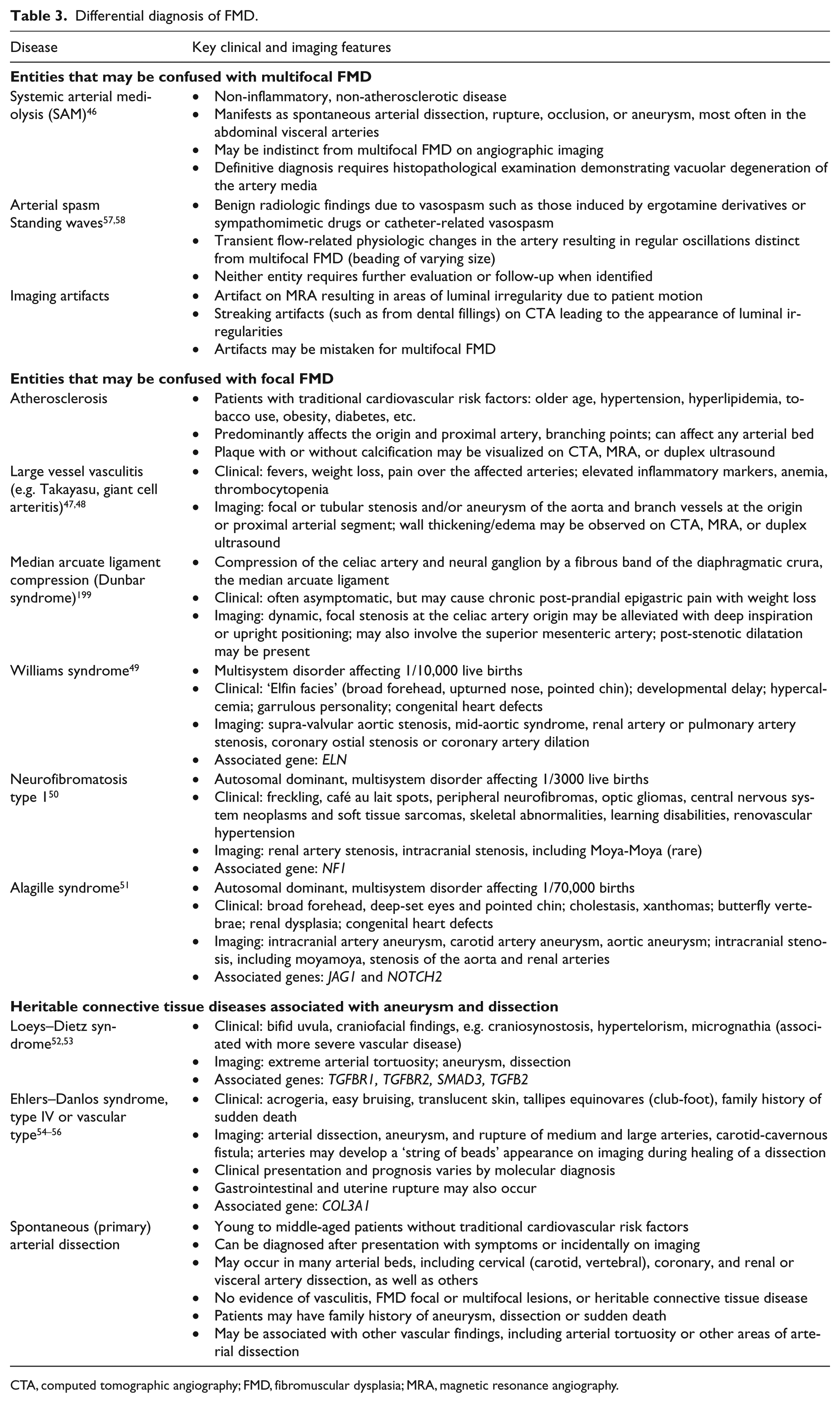
CTA, computed tomographic angiography; FMD, fibromuscular dysplasia; MRA, magnetic resonance angiography.
Current status of US and European/International FMD registries
United States Registry for FMD
The US Registry for FMD began enrolling patients in January 2009 at seven clinical centers in the continental United States and has subsequently expanded to 13 actively enrolling clinical centers. The US Registry is funded by the FMD Society of America (FMDSA) with centralized data coordination in a secure online platform by the University of Michigan Cardiovascular Outcomes Research and Reporting Program (www.med.umich.edu/mcorrp/). As of February 2018, the US Registry has enrolled nearly 2000 patients and has had seven publications in peer-reviewed journals.1,3,4,11,41,59,60 Some clinical centers in the US Registry enroll pediatric as well as adult FMD patients.
European/International FMD Registry
The European FMD Registry was launched on the occasion of the First National Meeting on FMD in Belgium (December 12, 2015), in parallel with the Belgian FMD initiative. Although no funding is currently available, the European Registry has been subsequently endorsed by the European Society of Hypertension (http://www.eshonline.org/). It has been adapted from the French FMD Registry (coordinator: P-F Plouin), created in 2010 to merge existing local FMD databases. It includes over 50 items covering demographic and clinical characteristics of FMD, family history, type, localization, associated complications, and interventions selected from the larger dataset used in the French ARCADIA Registry.2,61 A flexible, secure online platform has been developed, which will allow for the addition of an indefinite number of new visits, imaging or vascular interventions.62,63
Since enrollment of the first patient in December 2015, the Registry includes 675 patients with FMD recruited in 30 centers from 17 different countries. Some clinical centers also enroll patients with SCAD. The Registry has become more international, with extensions using the same or similar datasets to national initiatives in Argentina (Sociedad Argentina de Hipertensión Arterial-República Argentina-Displasia Fibromuscular, SAHARA-DF), Japan, China (Chinese FMD initiative), and Tunisia. Besides new initiatives launched in the wake of the European initiative, the European FMD Registry also benefits from the contribution of pre-existing registries, such as ARCADIA-POL, currently including 220 patients from 32 centers in Poland, and initially inspired by the ARCADIA Registry but with its own specific objectives and research aims. 64 The latter are progressively incorporated in the European FMD Registry.
Comparison of US and European registries and objectives for the future
As can be seen in Tables 4 and 5, the US and European/International FMD registries share many similarities in structure and in clinical characteristics of patients enrolled. Although the assets of the newer European Registry include, among others, image archiving for systematic characterization of FMD subtype (multifocal/focal), inclusion of prevalent cases from smaller centers mostly focused on renal arteries or, less frequently, cerebrovascular arteries, probably accounts for the relatively low proportion of multivessel FMD compared to the US and ARCADIA registries. 2 Notably, in the subset of incident patients diagnosed after the creation of the European FMD Registry, differences with the US Registry and ARCADIA (e.g. in terms of age at diagnosis, estimated glomerular filtration rate, or proportion of patients undergoing interventions) tends to be much smaller (A Persu, personal communication, February 21, 2018). The writing committee anticipates that the current international consensus will be instrumental in harmonizing screening and imaging strategies within Europe and between Europe and the US.
Study design and overall characteristics of adult patients enrolled in the United States and European/International FMD registries.
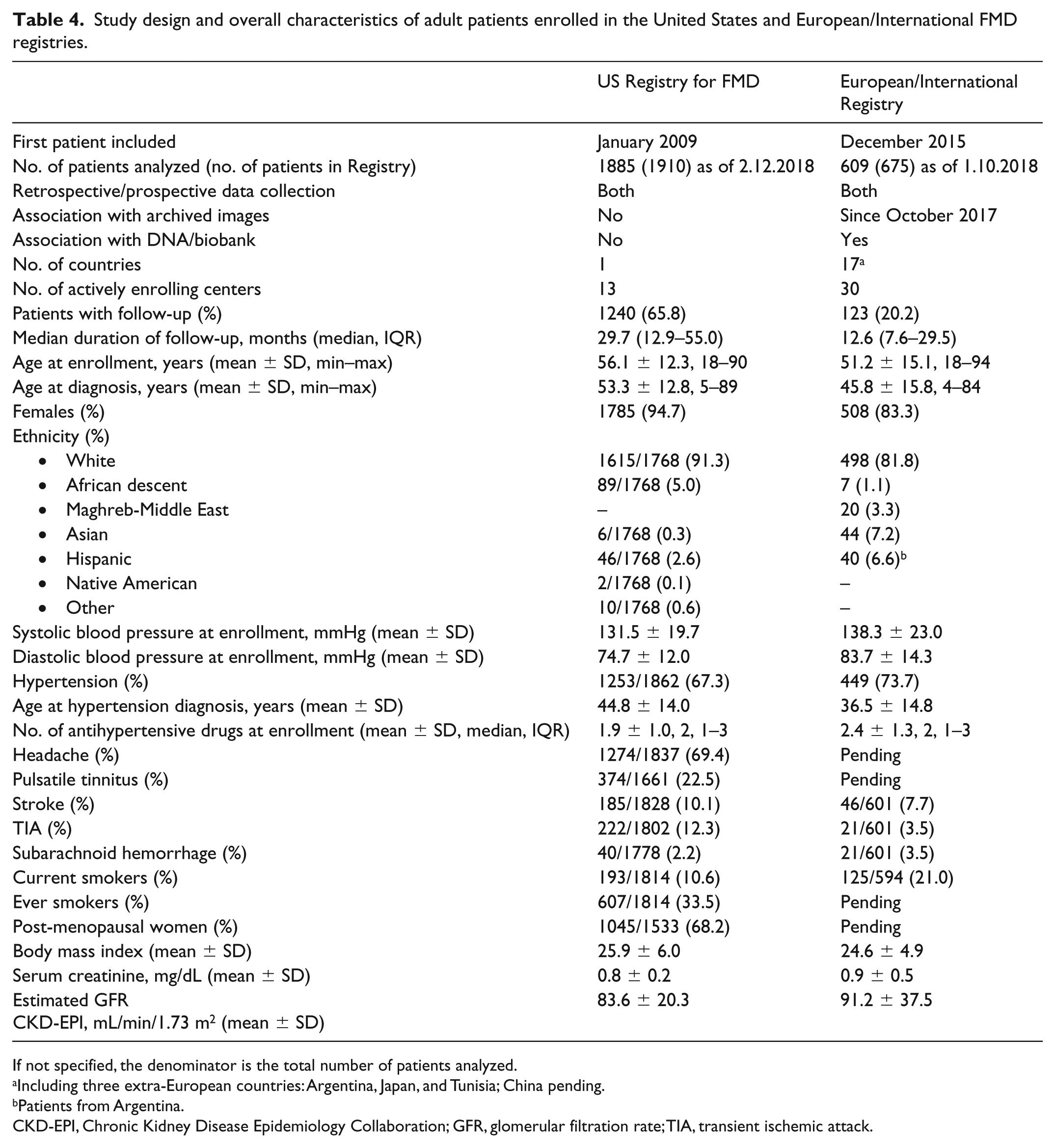
If not specified, the denominator is the total number of patients analyzed.
Including three extra-European countries: Argentina, Japan, and Tunisia; China pending.
Patients from Argentina.
CKD-EPI, Chronic Kidney Disease Epidemiology Collaboration; GFR, glomerular filtration rate; TIA, transient ischemic attack.
Vascular manifestations and type of FMD of adult patients enrolled in the United States and European/International registries.
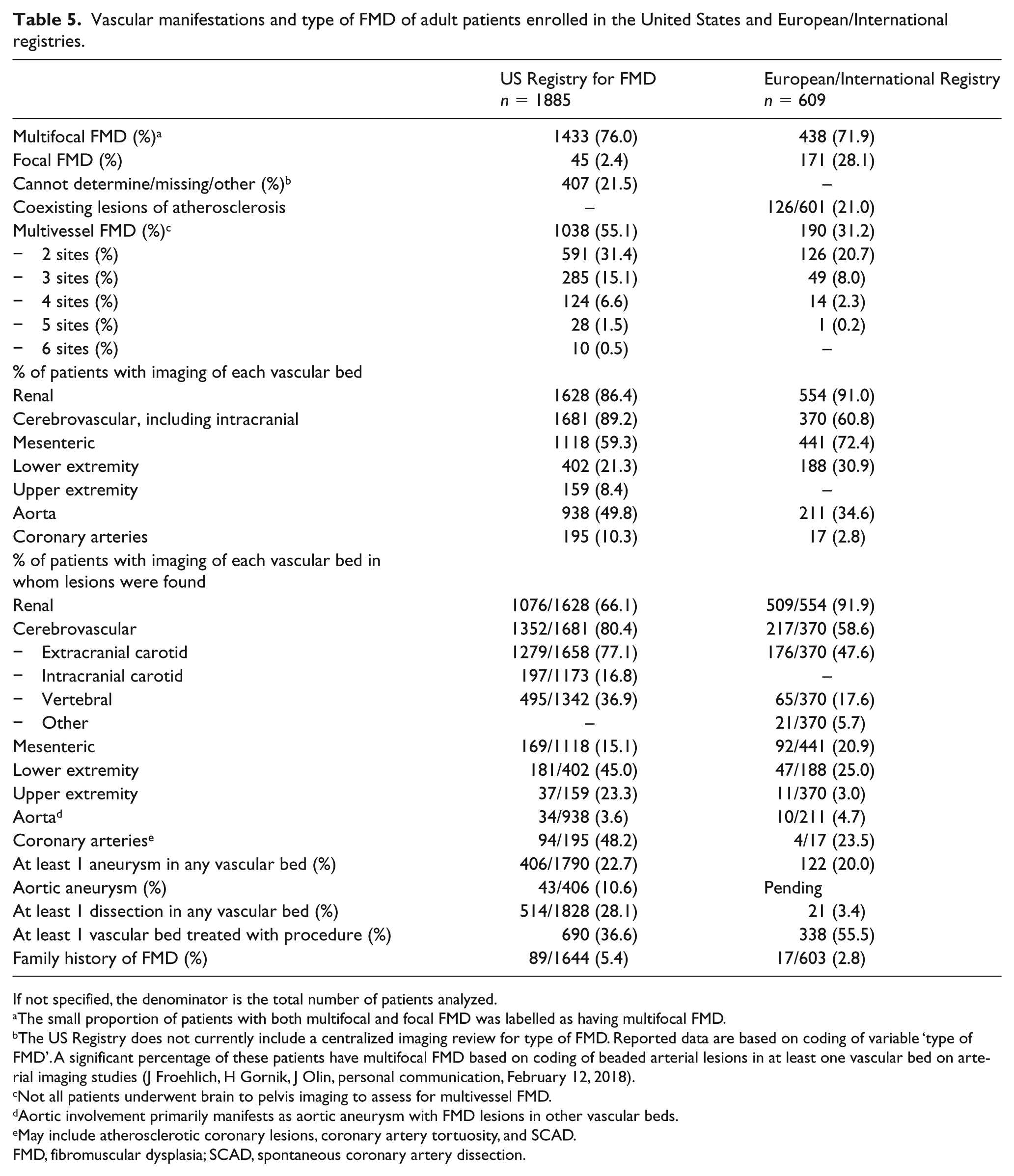
If not specified, the denominator is the total number of patients analyzed.
The small proportion of patients with both multifocal and focal FMD was labelled as having multifocal FMD.
The US Registry does not currently include a centralized imaging review for type of FMD. Reported data are based on coding of variable ‘type of FMD’. A significant percentage of these patients have multifocal FMD based on coding of beaded arterial lesions in at least one vascular bed on arterial imaging studies (J Froehlich, H Gornik, J Olin, personal communication, February 12, 2018).
Not all patients underwent brain to pelvis imaging to assess for multivessel FMD.
Aortic involvement primarily manifests as aortic aneurysm with FMD lesions in other vascular beds.
May include atherosclerotic coronary lesions, coronary artery tortuosity, and SCAD.
FMD, fibromuscular dysplasia; SCAD, spontaneous coronary artery dissection.
The leadership of both registries are committed to make them even more compatible in the future in order to facilitate collaboration and merging of data on specific topics, to disseminate the current consensus in order to harmonize screening and management strategies within and between both registries, and to make efforts to expand the registries to more diverse populations of patients with FMD, including populations of non-white ethnicity, which are currently underrepresented in both registries.
Example of another initiative: the Australian FMD Registry
The Australian FMD Registry (ROKD-FMD) was established in 2015. This Registry is nested within the Australian Registry of Kidney Diseases (ROKD-FMD – http://rokd.org.au/), designed as a patient data aggregation platform to facilitate research, monitor clinical progression, and capture quality-of-care indices to assess patterns of care for Australian patients. Data are held in a secure platform at the Department of Epidemiology at Monash University in Melbourne, Australia. With the support of the FMD Association of Australasia, a very active patient advocacy group (http://www.fmdaa.org.au/), 41 patients have been enrolled as of February 2018.
Imaging and diagnosis of FMD
Renal FMD
The prevalence of renal FMD in the general population is unknown because this disease is often clinically silent or discovered incidentally. However, studies from living kidney donor candidates and other clinical series indicate a prevalence of renal FMD of 3–4%, and the prevalence of incidental renal FMD among patients with renovascular hypertension enrolled in the Cardiovascular Outcomes in Renal Atherosclerotic Lesions (CORAL) trial was 5.8%.29,65 Among subjects with FMD in the US and ARCADIA registries, the renal arteries were involved in approximately 75% of patients.2,4 Based upon Registry data, the typical clinical phenotype of renal FMD is a middle-aged, white woman with hypertension, as well as a family history of hypertension, and up to 90% of these women have a multifocal type of FMD.2,4 Focal FMD is usually discovered before 30 years of age and often with blood pressure values on average higher than those observed among patients with the multifocal form. 10 There is a more balanced sex distribution among patients with focal compared to multifocal FMD.10,60 Hypertension is, by far, the most frequent presenting symptom among patients with renal FMD, whereas headache (especially migraine), pulsatile tinnitus, transient ischemic attack (TIA) or stroke may be the hallmark of cerebrovascular FMD (see below).
The proposed criteria to proceed to imaging assessment for renal FMD (Table 1) have been adapted with slight modification from the 2014 European FMD consensus.
Diagnostic approach to renal FMD
When a clinical suspicion of renal FMD has arisen, as outlined above (Table 1), the first step to confirm (or exclude) the diagnosis should be to perform a non-invasive imaging study. It is the consensus of the writing committee that computed tomographic angiography (CTA) is the initial test of choice for suspected FMD, but contrast-enhanced magnetic resonance angiography (MRA) is an option if CTA is contraindicated. CTA is preferable to MRA for diagnosis of FMD because of better spatial resolution. Moreover, CTA better visualizes small calcifications, thereby providing a more accurate discrimination of FMD from atherosclerotic renal artery stenosis. Although there are small cases series that have explored the diagnostic accuracy of CTA or MRA compared to angiography for FMD, it should be stressed that most studies of the diagnostic accuracy of various imaging techniques have been done in patients with atherosclerotic renal artery stenosis.66–68 It is the consensus of the writing committee that duplex ultrasound as the first diagnostic test for renal FMD should only be considered in specialized centers with extensive experience in duplex ultrasound for evaluation of FMD.
When the results of CTA or MRA confirm the diagnosis of FMD, or when a high clinical suspicion persists despite negative findings on CTA or MRA, proceeding to catheter-based angiography may be considered. Although catheter-based angiography is the gold standard for imaging the location and morphology of FMD, it is indicated only when its findings are expected to impact patient management. In patients with renal artery FMD, particularly of the multifocal type, imaging alone does not allow for determining the severity and hemodynamic significance of renal artery stenosis (Figure 2). Renal blood flow and renin secretion are often normal, and because FMD is often bilateral, there may be no lateralization on renal vein renin sampling. Therefore, translesional pressure gradient measurement is recommended in order to assess the hemodynamic significance of stenosis, particularly in multifocal FMD, as well as post-angioplasty in both focal and multifocal FMD to ensure the pressure gradient has been obliterated. In experienced centers, the procedure may be combined with intravascular ultrasound (IVUS) or optical coherence tomography (OCT). A proposed consensus protocol for catheter-based angiography in renal FMD is detailed in Table 6 and discussed below.
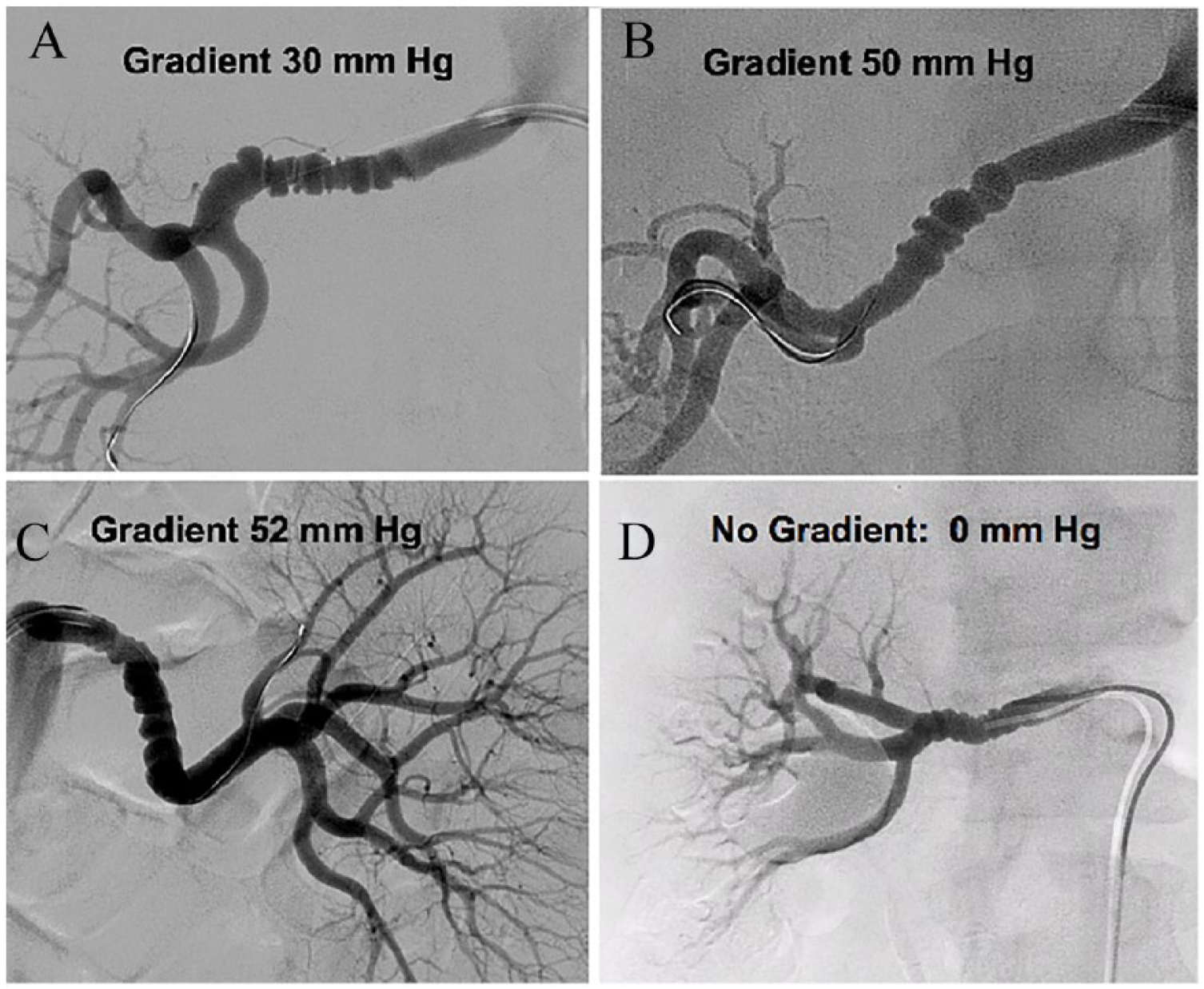
Measurement of translesional pressure gradients in renal artery FMD (A–D). Despite the appearance of multifocal FMD in all renal arteries, pressure gradients were highly variable, supporting the consensus that visual inspection alone is not adequate to determine the hemodynamic significance of multifocal renal FMD.
Consensus protocol for catheter-based angiography and PTA in patients with renal artery FMD.
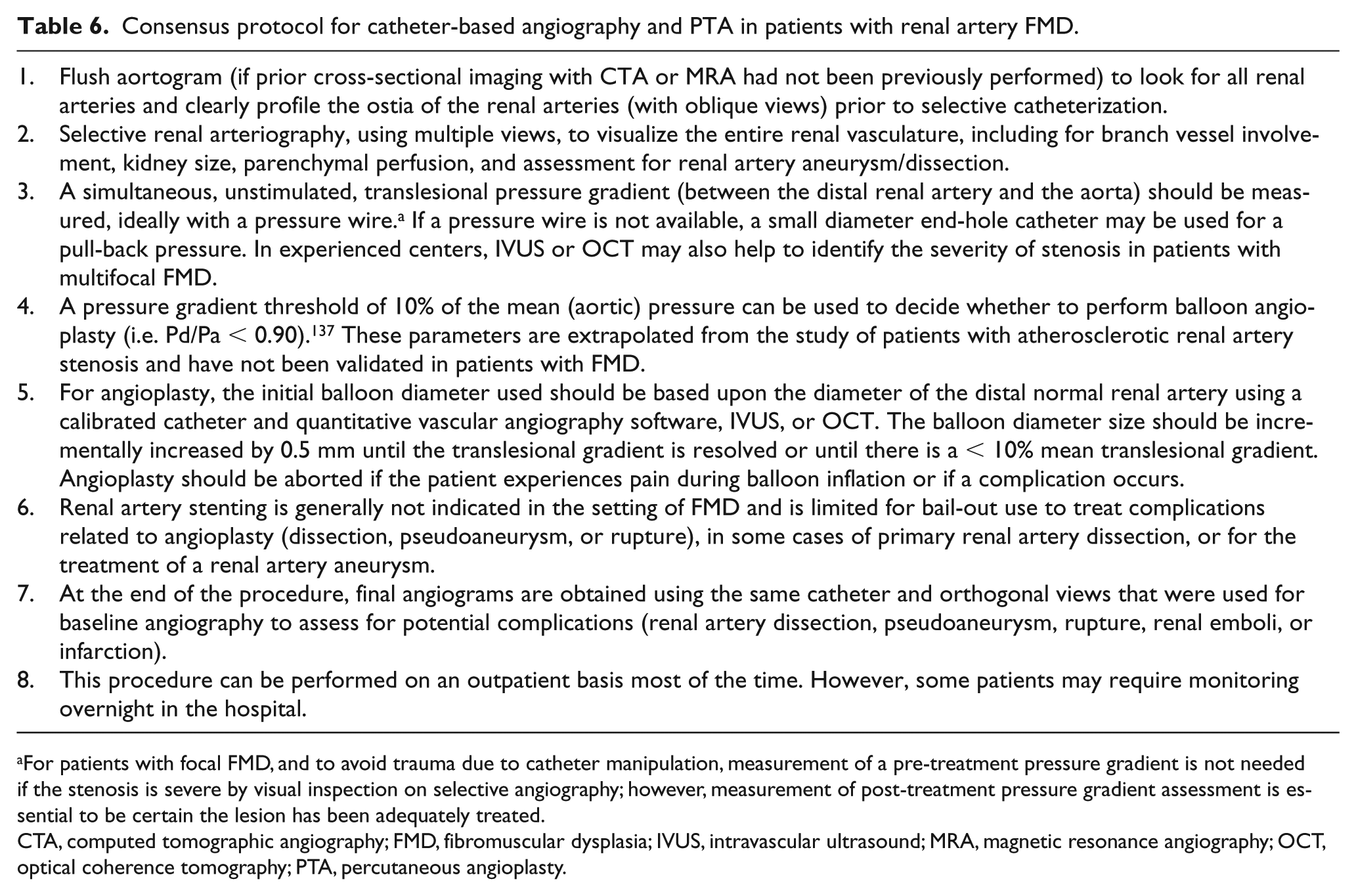
For patients with focal FMD, and to avoid trauma due to catheter manipulation, measurement of a pre-treatment pressure gradient is not needed if the stenosis is severe by visual inspection on selective angiography; however, measurement of post-treatment pressure gradient assessment is essential to be certain the lesion has been adequately treated.
CTA, computed tomographic angiography; FMD, fibromuscular dysplasia; IVUS, intravascular ultrasound; MRA, magnetic resonance angiography; OCT, optical coherence tomography; PTA, percutaneous angioplasty.
Cerebrovascular FMD
Historic estimates of cerebrovascular FMD report a lower frequency of involvement as compared to renal artery FMD; however, contemporary reports that include systematic imaging of arterial beds beyond the initial site of diagnosis have revealed similar rates of cervical artery and renal artery disease.2,4,69,70 In cases of CeAD (carotid or vertebral) related to FMD, focal neurologic findings with or without associated neck, face, or head pain may occur.1,71 Prior publications report that the prevalence of FMD in individuals with CeAD may be as high as 15–20%, although vascular beds beyond the cerebrovascular circulation were not evaluated for FMD in the majority of these cases.71–73 In the US Registry for FMD, 26% of subjects experienced an arterial dissection, most often in the carotid or vertebral arteries. 1 In the French ARCADIA Registry, CeAD was observed in 20/165 (12%) patients who presented with symptomatic cerebrovascular FMD. 2 Most often, symptoms related to cerebrovascular FMD are non-specific and may include headaches in ~50% of patients (especially confirmed and self-reported migraine type), pulsatile tinnitus (a ‘whooshing noise’ in the ears timed to the heart beat), and dizziness or light-headedness.2,4 Notably, 5.6% of patients in the US Registry presented with no symptoms and FMD was identified incidentally on imaging. 4
The lack of specific symptoms in FMD presents a challenge, as up to 25% of women in the general population may experience migraine headaches in their lifetime and only a subset will have FMD identified on a cerebrovascular imaging exam. The American Academy of Neurology guidelines advocate for neuroimaging for patients with migraine who have neurologic findings on physical examination or a change in the quality or severity of headache, but this approach would potentially miss a sizeable portion of patients with FMD because this neuroimaging does not necessarily include the cervical arteries. 74 The diagnosis of FMD should be considered and imaging pursued in patients with a cardinal symptom or sign of cervical artery FMD (Table 2).5,6
Diagnostic approach to cerebrovascular FMD
There are inadequate data to recommend one imaging modality over another for the diagnosis of cerebrovascular FMD. Catheter-based angiography remains the diagnostic gold standard; however, in most centers, this modality has been replaced by CTA or contrast-enhanced MRA as the initial imaging modality. Catheter-based angiography is typically reserved for complicated cases that may require intervention, such as the repair of an aneurysm or pseudoaneurysm related to dissection, or in rare cases of hemispheric neurological symptoms despite medical therapy associated with severe stenotic lesions. In high-volume centers with experience in vascular duplex ultrasonography for the evaluation of carotid FMD, it is reasonable to start with a carotid duplex exam, although this modality is inadequate to assess the vertebral and intracranial arteries for FMD. To date, there are no validated criteria for the diagnosis of carotid FMD by duplex ultrasound. However, characteristic findings may be identified that support the diagnosis, including turbulence, elevated velocities, and tortuosity in the mid-distal portion of the ICA, an area which is typically unaffected by atherosclerosis.5,6,12 This is in contrast to atherosclerosis, which typically affects the origin/proximal vessel (see Table 3). Carotid duplex may also be useful for interval follow-up and surveillance of patients with carotid artery FMD.5,6 Although catheter-based angiography remains the diagnostic gold standard, in most cases this modality has been replaced by non-invasive CTA or MRA.
Unruptured aneurysm is the primary manifestation of intracranial FMD. For patients with confirmed FMD in any location, brain imaging with CTA or MRA should be performed to evaluate for intracranial aneurysm, as the prevalence of intracranial aneurysms is significantly increased compared to the general population.1,5,6 In the US Registry, 12.9% of women had an intracranial aneurysm on imaging and a higher percentage of these were in a high-risk location (posterior circulation) and of larger size than comparable studies that screened the general population. 11 More than one-half of patients with intracranial aneurysm had multiple aneurysms. 11
Carotid bulb diaphragm
An entity named ‘carotid web’ or ‘carotid bulb diaphragm’ has been classified as atypical FMD of the carotid bulb by some authors and has been described predominantly in black/Afro-Caribbean patients.75–77 Although diaphragms were mainly reported in the carotid bulb, they have also been described in the ostium and V3 segment of the vertebral artery.78,79 These diaphragms are endoluminal webs or spurs that can be visualized as linear defects on CTA or MRA. This entity seems to be associated with a high risk of ischemic stroke, likely via an embolic mechanism, which may justify carotid stenting or endarterectomy in the setting of recurrent ischemic events despite medical management.76,77,80 Few cases in published series had pathologic specimens available for histologic review. Those that did describe ‘a loose matrix of edematous tissue and sparse spindle cells, especially in the outgrowth, resulting in intimal hyperplasia’, which is consistent with historic reports of this finding.81–83 However, it is not clear that this entity is consistent with classic intimal FMD, and there are no reported analogous findings in any other arterial bed to support a diagnosis of FMD. 84 Additionally, histologic evaluation of some of these lesions represents atheroma. 85 Thus, interpretation of these lesions with imaging alone should be approached with caution and it seems that this entity is likely distinct from the clinical syndrome of FMD discussed in this document.
FMD in other locations – visceral, iliac, brachial artery FMD
Beyond the renal and cervical arteries, FMD can be present in any arterial bed, with more common additional locations being the visceral, lower, and upper extremity arteries (Figure 3). 4 Involvement of these other arterial beds generally occurs among patients with multivessel FMD.
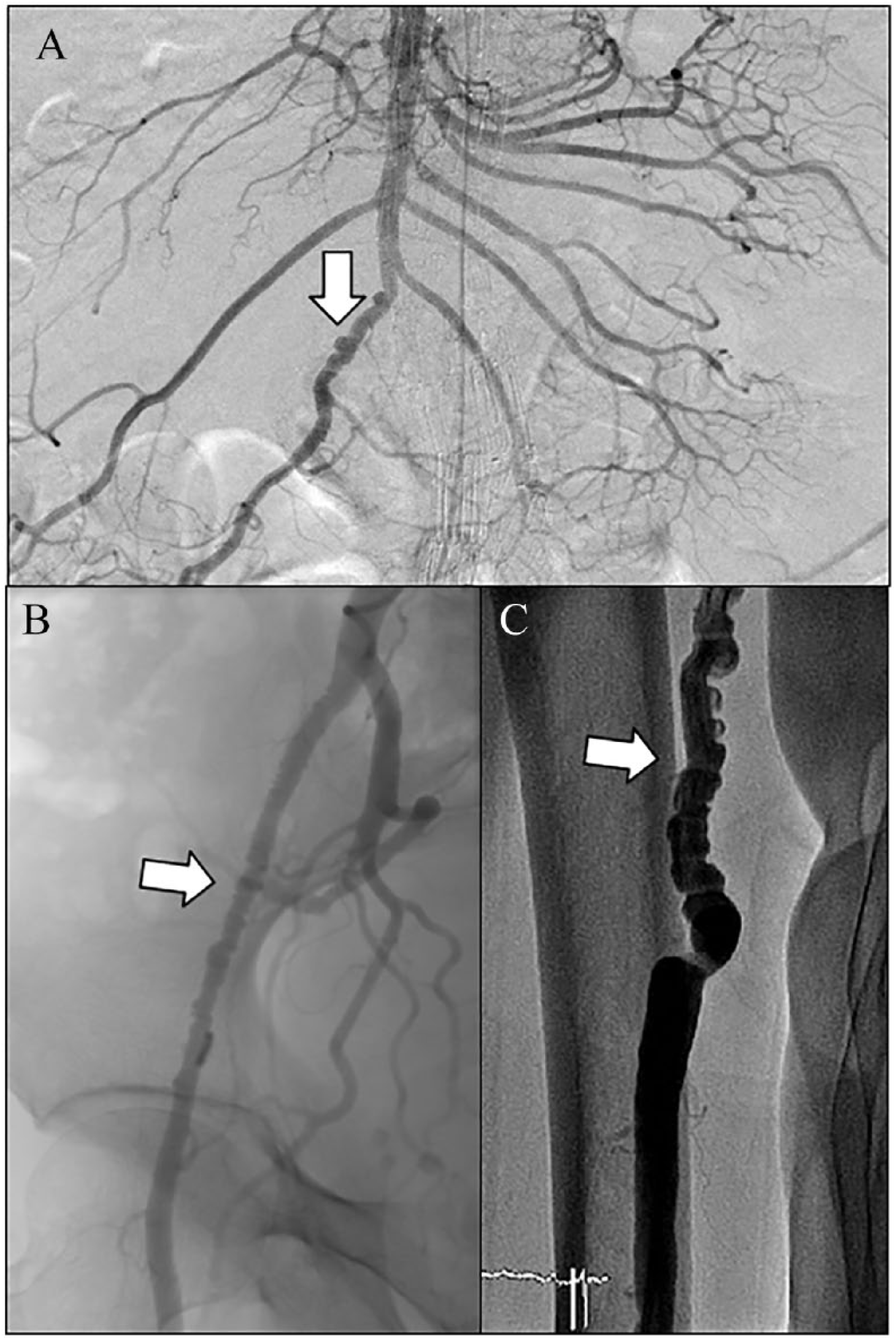
Angiographic images of multifocal FMD (arrows) from the superior mesenteric (A), external iliac (B), and brachial arteries (C).
Visceral artery FMD
Visceral artery FMD includes the celiac axis and hepatic and splenic arteries, and the superior and inferior mesenteric arteries. The US Registry and the French ARCADIA Registry reported visceral artery involvement in 19.3% (95/493) and 17.5% (82/469) of patients who underwent imaging studies.2,86 The Polish ARCADIA-POL Registry reported mesenteric involvement in 13.2% (19/144) and splenic artery involvement in 10.4% (15/144) of patients. 64 Patients with visceral FMD are more likely to have aneurysms or dissections compared to those without visceral FMD (41.2% and 35.6% vs 19.7% and 20.6%, respectively). 86 In the US Registry, visceral locations accounted for 13.0% and 5.9% of all aneurysms and dissections, respectively. 1 In the Polish ARCADIA-POL Registry, aneurysms in the splenic arteries were found in 7.8% of patients. 64 Visceral artery FMD can present as postprandial flank or abdominal pain, mesenteric ischemia, aneurysms, dissections, or with an abdominal bruit. 4 Visceral artery FMD may also be an incidental finding on an imaging study obtained for other purposes. Cases of FMD involving the hepatic artery and associated with spontaneous dissection presenting with acute abdominal pain and shock have been reported.87,88
Iliac and lower extremity FMD
Lower extremity FMD is most commonly multifocal and bilateral, and typically involves the external iliac arteries; however, it has also been reported in common iliac, internal iliac, common femoral, deep femoral, superficial femoral, and popliteal arteries.2,64,89,90 In the French ARCADIA and Polish ARCADIA-POL registries, FMD involving the iliac arteries was present in 14.7% (69/469) and 7.6% (11/144) of patients, respectively.2,64 In a study from the Cleveland Clinic where 100 of 449 FMD patients had lower extremity imaging, generally for symptoms or signs (femoral bruit) of involvement, 62% had FMD in the lower extremity arteries. 89 Potential symptoms include claudication, foot or toe ischemia, and atypical leg symptoms; dissections and aneurysms may occur. The majority of patients with lower extremity involvement are asymptomatic and may be diagnosed by femoral bruit noted on physical examination or incidentally on imaging studies. Standing waves on catheter-based angiography can be misdiagnosed as lower extremity FMD and are an important differential diagnosis (Table 3). Standing waves are a benign phenomenon that may appear with regularly shaped ‘string of beads’, but do not have the same clinical implications as FMD. 57
Upper extremity FMD
Upper extremity FMD has been reported in 15.9% (10/63) of patients who underwent upper extremity imaging in the US Registry. 4 It typically involves the brachial artery, although it has been reported in the subclavian, axillary, radial, and ulnar arteries.4,91 It is most commonly of the multifocal type with the majority of patients having both asymptomatic and bilateral involvement. 91 Symptoms of upper extremity FMD may include finger or hand ischemia (rest pain, discoloration, ulceration or gangrene) from thromboembolism or dissection and hand or arm claudication.91–94 Other manifestations include Raynaud’s phenomenon, paresthesia, and rarely aneurysms.91–94 Brachial bruit and discrepant arm blood pressures are frequently identified on physical exam when brachial FMD is present. 91
Diagnostic approach and imaging for FMD at other locations
To date, no studies have compared the accuracy of diagnostic imaging modalities for visceral, lower, or upper extremity FMD. In experienced centers, duplex ultrasound can be used to identify FMD by demonstrating stenosis, marked turbulence in both color Doppler and spectral Doppler waveforms, and potential for delayed up-stroke (parvus-et-tardus waveform) in arterial segments distal to areas of stenosis. 4 Findings must be differentiated from atherosclerotic disease based on location of the lesion and absence of plaque. In some cases, color power angio and grayscale imaging may show a beaded arterial appearance and intraluminal webs. Duplex ultrasound is likely to have the greatest diagnostic value in assessing the readily accessible brachial arteries as it may inadequately visualize the external iliac and visceral arteries.4,6 Although duplex can be a good initial diagnostic tool in experienced centers, it is operator dependent and less sensitive than CTA, MRA, or catheter-based angiography for the diagnosis of FMD at other locations. Hence, if there is strong clinical suspicion of FMD, then further testing with other forms of imaging is recommended even if duplex evaluation is unremarkable or non-diagnostic. Though seldom required for diagnostic purposes alone, catheter-based angiography remains the gold standard for diagnosis of FMD, including for involvement of the visceral and extremity arteries.
Systemic nature of FMD
In the ARCADIA Registry, systematic imaging of 469 patients presenting either as renal or cerebrovascular FMD led to the identification of focal or multifocal FMD lesions in at least one other vascular bed in 48% of patients, and of other vascular lesions such as aneurysms or dissections in another 18%, leading to an overall prevalence of 66.3% of multivessel FMD as defined in the current consensus. 2 These findings are consistent with those of the US Registry, in which more than 50% of patients now have multivessel involvement, though in the latter systematic imaging was not undertaken in all patients (Table 5). Along the same lines, in a single-center retrospective series of 113 consecutive patients with FMD who underwent a dedicated chest to pelvis CTA protocol, new findings were identified in a significant percentage of patients: 55 (48.7%) new FMD lesions, 21 (18.6%) new aneurysms, and three (2.7%) new arterial dissections. 69
Although in the ARCADIA study, the probability of having cerebrovascular FMD was higher in patients with bilateral rather than unilateral renal FMD (OR, 1.88; 95% CI, 0.99–3.57) and, not unexpectedly, the probability of having renal FMD was higher in patients with cerebrovascular FMD with hypertension (OR, 3.4; 95% CI, 1.99–6.15), these correlations are not strong enough to restrict comprehensive vascular imaging to specific subgroups of patients with FMD. 2 Therefore, and also in view of the availability of new CTA protocols allowing for high-quality image acquisition with decreased irradiation and contrast exposure, the sequential imaging approach recommended in previous consensus documents can be abandoned in favor of brain to pelvis cross-sectional imaging by CTA or contrast-enhanced MRA in all patients with FMD.4,6,61,69,95 At present, coronary artery imaging for potential manifestations of FMD is not recommended in the absence of symptoms (see SCAD and coronary FMD below).
Management of FMD
Medical therapy
Antiplatelet therapy
There are no trials assessing the utility of medical therapy in FMD or prospectively comparing medical therapy to intervention in this population. As patients with FMD may present with thrombotic and thromboembolic events, even in the absence of dissection or aneurysm, antiplatelet agents are reasonable for both symptomatic and asymptomatic FMD.4,59,91 This practice is also supported by FMD pathophysiology, especially that of multifocal FMD, as intra-arterial webs and areas of dilatation may serve as a nidus for platelet aggregation. 1 Nevertheless, one should keep in mind that there are no placebo-controlled studies of antiplatelet therapy for FMD and there are no data to support one agent over the other. Accordingly, the potential benefits versus risks of antiplatelet therapy should be weighed on an individual basis, including factors such as prior thromboembolic events, arterial dissection, or revascularization procedures (each of which would support antiplatelet use), as well as risk factors for bleeding (e.g. prior history of subarachnoid hemorrhage or other bleeding events, large intracranial aneurysm). In the US Registry, 72.9% of patients were prescribed antiplatelet therapy, with aspirin being the most commonly prescribed agent. 59 Older age, concomitant coronary artery disease, prior vascular intervention, and isolated cerebrovascular FMD were factors associated with higher rates of antiplatelet use. 59
Treatment of hypertension
Because the ideal blood pressure target in patients with FMD is unknown, it is reasonable to follow general recommendations, such as those of the 2017 American College of Cardiology/American Heart Association multisocietal Guideline for the Prevention, Detection, Evaluation, and Management of High Blood Pressure in Adults and the recently published guidelines of the European Society of Cardiology and European Society of Hypertension.96,97 The majority of patients with FMD receive antihypertensive medications. 59 There are several potential justifications for this practice. First, hypertension is common among patients with FMD, either due to essential or renovascular hypertension associated with renal artery involvement. 4 Although all antihypertensive medication can be prescribed in renovascular hypertension, angiotensin-converting enzyme (ACE)-inhibitors or angiotensin receptor blockers (ARB) have been recommended in this setting.97,98 Following SCAD, beta-blockers may have a protective effect. 99 Control of hypertension is particularly important for patients with FMD who have intracranial aneurysms, as well as aneurysms at other locations. Certain antihypertensive medications (i.e. beta-blockers, calcium channel blockers, ARBs) may also be effective as preventive therapies for migraine.
Management of headache and pulsatile tinnitus
Medical therapy for the care of the patient with FMD should also address common symptoms of headache and pulsatile tinnitus that may have an impact on quality of life. 4 In the US Registry, significant headache was reported in 67.5% of patients, with more than one-half of patients reporting headaches at least weekly. 100 Although migraines are the most common headache type among patients with FMD (38% of patients in the US Registry; 28% in ARCADIA), headache may also be related to uncontrolled hypertension or CeAD.2,4,101 Migraines may occur in patients with FMD even in the absence of cerebrovascular involvement. As for all patients with migraine, the approach to migraine in patients with FMD may include lifestyle modification to avoid triggering factors, preventive therapies, and medications to abort migraines. Although there are no specific studies of migraine therapies for patients with FMD, particular caution is advised in prescribing tryptans, ergots, and other vasoconstrictive agents. This is especially important among those patients with a prior history of CeAD or SCAD, in whom these agents may be contraindicated. 101
As discussed above, pulsatile tinnitus has recently been recognized as a common manifestation of cerebrovascular FMD, reported as a presenting symptom in 32% of all patients in the US Registry. 102 Patients may respond to reassurance and education, but other approaches including sound or cognitive behavioral therapy may be helpful for some patients with more severe symptoms, though experience is limited for management of pulsatile (compared to non-pulsatile) tinnitus.103–105 Consultation with audiology and otolaryngology may be helpful to evaluate hearing and to assess for other causes of pulsatile tinnitus beyond FMD.
Additional considerations
Statins, which are routinely prescribed for atherosclerotic cardiovascular disease, are not recommended routinely for patients with FMD in the absence of another indication, such as hyperlipidemia or concomitant atherosclerosis.106–108
Smoking cessation has been shown to have many health-related benefits in the general population. 109 Patients with FMD who smoke have been shown to have a higher prevalence of aneurysms and more adverse events, including the need for vascular procedures.40,41 Smoking cessation should be strongly encouraged for all patients with FMD who continue to smoke.
FMD is predominantly a disease of women, and concern has been raised for exogenous hormone therapies in these patients (e.g. oral contraceptive pills or hormone replacement therapy). To date, however, these concerns remain theoretical, as no data exist to support the safety or harm associated with exogenous female hormones in FMD.
Finally, patients with FMD often require guidance regarding physical limitations, especially if a prior arterial dissection has occurred. There are no data to inform on such guidance, however, and the risk of adverse arterial events differs for each patient. Some activities are known to be associated with CeAD in the general population, including chiropractic neck manipulation and roller coaster rides.110,111 These are best avoided. Other activities that include prolonged neck extension or severe neck traction, weight training or heavy lifting, and physical blunt-force contact (e.g. martial arts) should be addressed on a case by case basis.
Management of arterial dissection and aneurysm in patients with FMD
Cervical artery dissection and intracranial aneurysm
Cervical artery dissection (CeAD)
In the absence of data from randomized trials specific to patients with FMD, management of CeAD (i.e. carotid or vertebral) among patients with FMD is similar to that of patients without FMD.112,113 In acute stroke due to CeAD, both intravenous thrombolysis and mechanical thrombectomy can be used in eligible patients, although there is no specific data regarding the benefit of these therapies in this situation.114,115 In case of carotid artery occlusion or severe carotid stenting due to CeAD, acute carotid artery stenting is sometimes required before mechanical thrombectomy can be performed. As the vast majority of patients with CeAD will not require thrombolysis, antithrombotic treatment is used in order to prevent recurrent ischemic events. The American Heart Association/American Stroke Association guidelines recommend treatment with either an anticoagulant or an antiplatelet agent for at least 3–6 months in patients with CeAD associated with ischemic stroke or TIA, and this position has been supported by the results of the CADISS trial.113,116 The consensus of the writing committee is that this recommendation also applies to patients with CeAD in the setting of underlying FMD. There are very limited data on the use of direct oral anticoagulants in the management of CeAD. 117 Beyond the initial 3–6 months, antiplatelet therapy is generally continued long term. Endovascular therapy (e.g. carotid artery stenting) is typically restricted to cases with persistent cerebrovascular ischemia despite optimal medical therapy.118,119 Additionally, pseudoaneurysms resulting from a dissection are at low risk for ischemic events or rupture and rarely require endovascular treatment.120,121 If endovascular intervention is indicated, careful attention should be made to avoid iatrogenic vascular injury during groin access or guide catheter placement. However, it is unknown whether the existence of FMD increases the risk of iatrogenic dissection or post-stenting pseudoaneurysm development.
Intracranial aneurysm
As discussed above, the writing committee recommends screening patients with FMD for unruptured intracranial aneurysm given the significant prevalence in this population, although the management of this entity remains controversial. The mean annual risk of rupture of unruptured intracranial aneurysm is < 1% in the general population, but it is unknown whether FMD is associated with an increased risk of rupture. 122 Management choice is influenced by the life expectancy of the patient, the estimated risk of rupture, the risk of complications of preventive treatment, and the level of anxiety caused by the awareness of having an aneurysm. 122 The risk of rupture depends on many factors, including aneurysm-related factors (number, size, shape, and location of aneurysms), and patient characteristics (geographical region, hypertension, smoking history, alcohol use, prior history of rupture). 122 In the US Registry, among patients with intracranial aneurysm, 43% were ⩾ 5 mm and 19% were located in the posterior circulation, a high-risk feature. 11 There are two modalities available for preventive aneurysm exclusion: surgical clipping and endovascular coiling with or without additional devices, such as regular stents or flow-diverting stents. The surgical and endovascular management of intracranial aneurysm in patients with FMD does not differ from that of patients without FMD.123,124 Most intracranial aneurysms are amenable to coil embolization, especially with newer devices that are available to assist in the treatment of wide-necked aneurysms. 125 Surgical clipping is also feasible in many cases, and the choice of the best treatment modality depends on anatomical factors and the assessment of the neurointerventionalist as well as patient preference. 126 In the absence of intervention, patients with unruptured intracranial aneurysm are often advised to undergo follow-up imaging to monitor for aneurysm growth. However, the optimal frequency of follow-up is unknown. 122
Renal and visceral artery aneurysms and dissection
The prevalence of visceral artery aneurysm and dissection among all comers with FMD is unknown as population-based studies are lacking. Furthermore, defining aneurysm in an artery affected by FMD is not straightforward given the tortuous and beaded appearance of arteries affected by multifocal FMD and challenges distinguishing a prominent beaded segment from a small aneurysm. Thus, although published rates of aneurysms in FMD exist, a consensus (size) definition for aneurysms in multifocal FMD does not.1,2 Notwithstanding, within the US Registry, aneurysm, dissection or both were present in 41.7% of patients; in the ARCADIA Registry, aneurysms were present in 26% whereas dissections were present in 15.1% of patients.1,2 Aneurysms may be asymptomatic or present with distal embolization of thrombotic content or rupture.
Renal and visceral artery dissection
Renal or visceral artery dissection may be asymptomatic or present with distal thromboembolic events (e.g. renal or splenic infarct). Renal infarction, often related to underlying dissection, may be an initial manifestation of renal FMD.127,128 In the US Registry, renal artery dissection was the presenting sign of FMD in 3.1% of patients. 4 In a French single-center series including 186 patients with renal infarction, dissection was observed in 76 patients (40.8%) and occlusion in 75 (40.3%). 127 Predominant renal artery lesions (n = 151; 81.2%) were atherosclerotic disease (n = 52; 34.4%) followed by dissecting hematoma (n = 35; 23.2%) and FMD (n = 29; 19.2%). Renal artery dissection and infarction may be a more common presentation of FMD in men than women. 3 In a series of 42 patients with visceral artery dissection, aneurysm was rare and only two patients had evidence of underlying FMD. 129 Notably, not all patients were screened for FMD.
As discussed above, patients with FMD generally should receive an antiplatelet agent. If a renal or visceral artery dissection is detected, short-term (e.g. 3–6 months) anticoagulation may be prescribed empirically, particularly in the setting of distal thromboembolic lesions, followed by long-term antiplatelet therapy. Others prefer antiplatelet therapy (i.e. aspirin alone or in combination with clopidogrel) for initial treatment of renal or visceral artery dissection.130,131 Future studies are needed given data comparing anticoagulation and antiplatelet agents after CeAD; but at this time, there are inadequate data to make a consensus point for renal and visceral artery dissection. 113 As is the case for patients without FMD, the majority of renal and visceral artery dissections in patients with FMD are managed with medical therapy and surveillance imaging. Interventional procedures for renal or visceral dissection are warranted if there is progressive end-organ malperfusion, progressive dissection over time, or secondary aneurysm. Potential procedures include covered stent, coil embolization, or surgical repair. However, it should be noted that renal artery dissections often occur in distal branches, which would preclude the use of stents. Recanalization of a dissected artery that supplies a portion of the kidney that is infarcted is unlikely to be beneficial.
Renal and visceral artery aneurysm
Patients with FMD who are found to have small renal or visceral artery aneurysms will require periodic clinical follow-up and surveillance imaging studies, though there are inadequate data to inform the optimal frequency of follow-up for a given aneurysm size. Maintaining adequate control of hypertension and complete smoking cessation is particularly important among patients with aneurysmal disease.
Among patients who do not have FMD, intervention for renal and visceral artery aneurysms is generally offered if the size exceeds 2 cm. This practice is based on limited data, including several small case series of patients with splenic and renal artery aneurysms, but no data exist specifically in FMD.132,133 Also, it is important to note heightened concern for the risk of aneurysm rupture during pregnancy, and the size threshold for when to consider intervention for a renal, hepatic, or splenic aneurysm in a woman with FMD of childbearing age who is contemplating future pregnancy.134–136 Although not based on good clinical studies, many experts in treating patients with FMD consider intervention on such aneurysms at a diameter threshold of less than 2 cm in women of childbearing age. Potential procedures to treat aneurysms include coiling, covered stents, or surgery (i.e. resection and/or bypass). Procedures should be avoided if an occluded aneurysm is detected, or if treatment may sacrifice vital organ parenchyma.
Renal angiography and revascularization
As discussed above, catheter-based angiography remains the gold standard for assessment of renal FMD. Measurement of a pressure gradient, usually with a flow wire, is necessary to avoid angioplasty of lesions, especially of the multifocal type, that are not hemodynamically significant (Figure 2). A pressure gradient of 10% of mean (aortic) pressure (i.e. Pd/Pa < 0.90) is proposed as a threshold for hemodynamically significant renal FMD for angioplasty, though it is acknowledged that this value is based upon the study of atherosclerotic renal artery stenosis and needs to be validated in the setting of FMD. 137 Further, measurement of a pressure gradient can be used to be sure the gradient is obliterated after angioplasty for both multifocal and focal FMD. Stent kinking and fracture have been reported in the setting of renal FMD.138,139 Accordingly, in the absence of the demonstrated added value of stenting, angioplasty alone is the revascularization approach of choice for renal artery FMD, and stenting is reserved for the treatment of procedural complications, such as a flow-limiting dissection or arterial rupture. A proposed consensus-based protocol for catheter-based angiography and angioplasty for renal FMD is shown in Table 6. This protocol is based upon the clinical experience of experts at high-volume clinical centers and it is intended that this protocol will allow for standardization of diagnostic angiograms for renal FMD and for angioplasty procedures, and that prospective data will be collected to validate its use to potentially improve outcomes in these patients.
Surgery remains the primary approach in rare patients with complex FMD lesions of the arterial bifurcation or branches, stenoses associated with complex aneurysms, or following failure of angioplasty. Repeat angioplasty may be attempted following primary failure of angioplasty or recurrent stenosis; however, repeated procedures should be undertaken with caution to prevent jeopardizing future surgical options.6,140
Reported outcomes following revascularization for renal FMD have been variable. In a meta-analysis by Trinquart and colleagues, the rate of cure of hypertension (defined as blood pressure < 140/90 mmHg without medication) was only 36% after angioplasty across 11 clinical studies (range 14–85%), with the probability of being cured associated with younger patient age at the time of treatment and shorter duration of hypertension. 141 Savard and colleagues demonstrated that focal FMD was associated with a higher hypertension cure rate after angioplasty than multifocal FMD. 10 Finally, in the meta-analysis, 18% of patients underwent a repeat procedure. 141 Although it is reasonable to assume that improved case selection of patients with hemodynamically significant renal FMD for angioplasty and confirmation of obliteration of the trans-renal pressure gradient after angioplasty may improve interventional outcomes, this requires further study, and this has been identified as a priority for future FMD research initiatives (Table 7).
FMD research priorities.
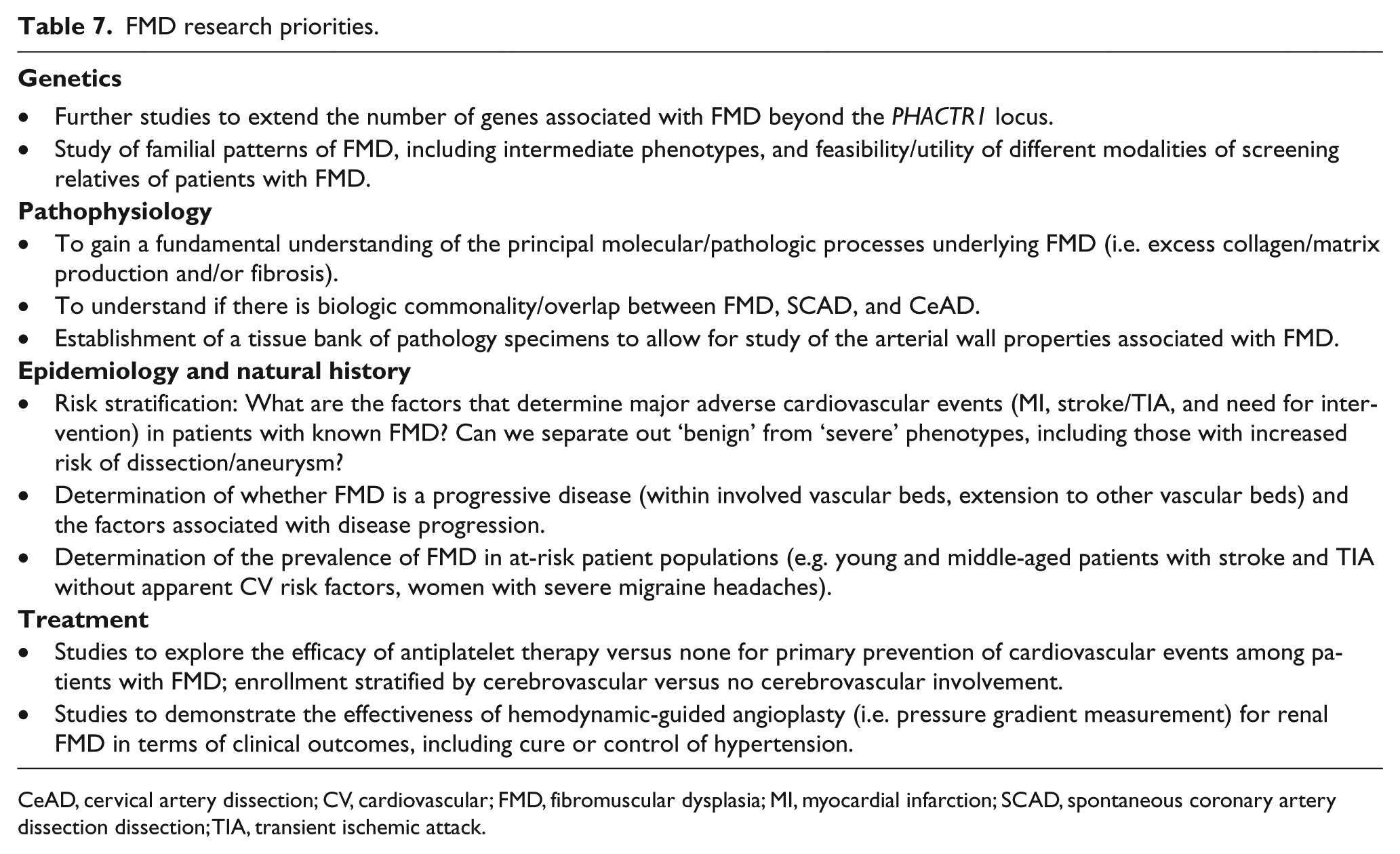
CeAD, cervical artery dissection; CV, cardiovascular; FMD, fibromuscular dysplasia; MI, myocardial infarction; SCAD, spontaneous coronary artery dissection dissection; TIA, transient ischemic attack.
Care following renal angioplasty
Following renal angioplasty, aspirin 75–100 mg daily is prescribed indefinitely, though some operators empirically prescribe a short course of dual antiplatelet therapy (e.g. 4–6 weeks). Antihypertensive medications given prior to angioplasty can be usually stopped at discharge after successful angioplasty, and the need for medication is reassessed frequently at follow-up visits during the first post-procedure year. Surveillance with renal artery duplex ultrasound may include a study on the first office visit post-angioplasty (usually within 1 month) and every 6 months for 24 months, then yearly, to detect findings suggestive of restenosis. Imaging may be obtained more frequently in the setting of an unexplained increase in blood pressure and/or decline in renal function.
Spontaneous coronary artery dissection and coronary FMD
Spontaneous coronary artery dissection (SCAD)
SCAD is an uncommon cause of acute myocardial infarction (AMI).142–144 It has a strong female predilection (> 90% female), with a minority of cases (~10%) occurring during or after pregnancy.145–160 SCAD accounts for 10–25% of AMIs in women under the age of 50 years and 50% of AMIs occurring in the post-partum period.150,155,156,158,161 It is a rare but recognized cause of sudden cardiac death. 162 Unlike in atherosclerotic AMI where the primary pathophysiologic event is the generation of luminal thrombus at sites of plaque rupture or erosion, coronary insufficiency in SCAD arises from external compression of the true lumen by the development of a false lumen within the outer third of the tunica media of the coronary vessel wall. The cause of SCAD is unknown. Familial cases have been described and rare cases are reported in association with hereditary connective tissue disorders, but most cases of SCAD are sporadic. 163 In the coronary circulation, SCAD has been shown to be associated with increased arterial tortuosity. 16
SCAD can usually be diagnosed angiographically, although intracoronary imaging (e.g. with optical coherence tomography) can be helpful in equivocal cases (Figure 4).164–166 Outcomes after percutaneous coronary intervention (PCI) are significantly worse than for atherosclerotic disease, primarily because of the risk of extension of the dissection and thus the false lumen.145–147,149,150 In addition, after coronary artery bypass grafting (CABG), long-term subclinical graft failure rates appear high, probably due to competitive flow following healing of the native coronary following SCAD. 145 For these reasons, there is a growing consensus in favor of conservative (medical) management when possible (e.g. TIMI 3 flow in the affected vessel and no ongoing documented ischemia). Although most dissections appear to heal completely within 3–6 months, outcomes following AMI due to SCAD are impacted by a high reported incidence of recurrent SCAD, with 10.4% reported from 327 patients in one prospective series followed for a median 3.1 years.99,143,145–147,149,150,167 Data on optimal medical therapy after SCAD remain limited, with initial evidence suggesting a potential role for beta-blockade and control of hypertension in reducing the recurrence risk. 99 The optimal regimen and duration of antiplatelet therapies in conservatively managed SCAD remains unclear. More details on SCAD pathophysiology, diagnosis, and management can be found in recently published scientific statements.168,169
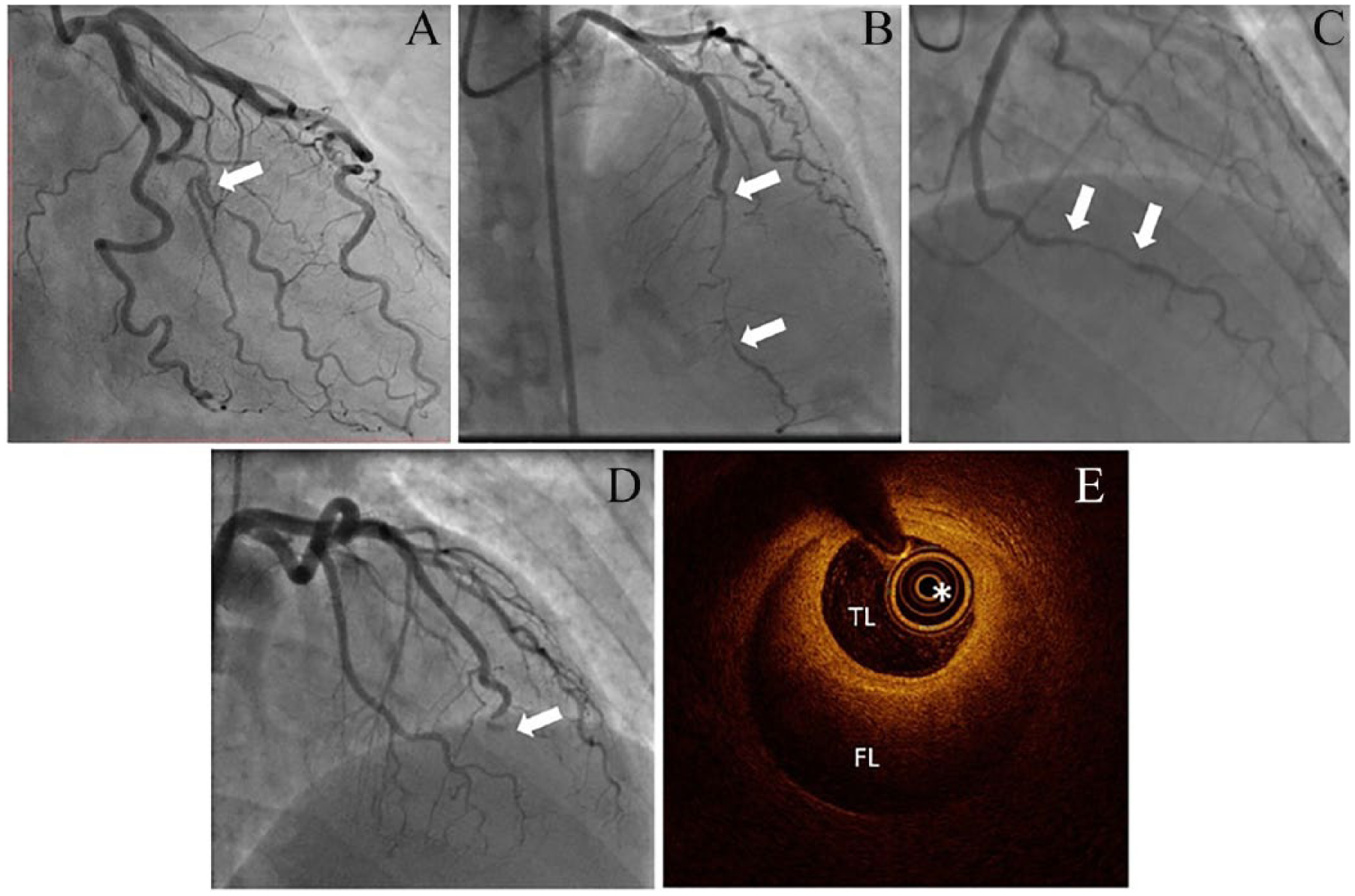
Angiographic classification of SCAD (arrows), proposed by Saw and colleagues. 165 Type 1 SCAD – with a dual lumen and flap in the mid-LAD coronary artery (A), type 2 SCAD with a long segment of narrowing in the mid-distal LAD with recrudescence of the vessel distally (B), and type 3 SCAD resembling an atherosclerotic lesion with diagnosis requiring intracoronary imaging (C). A fourth angiographic appearance of SCAD leading to coronary artery occlusion has been proposed. 169 In this case (D), there was a total occlusion of the LAD, with SCAD only confirmed after restoration of distal flow. (E) A typical optical coherence tomography image of SCAD, showing the imaging catheter (*) within the TL surrounded by the compressing crescentic FL.
Relationship between SCAD and FMD
Pate and colleagues published the first case series describing findings of renal FMD in young patients presenting with acute coronary syndromes and unusual coronary lesions. 170 These unusual coronary lesions were subsequently identified as SCAD in a publication using OCT 171 . Since then there have been numerous single-institution studies that have reported the findings of multifocal FMD in the extracoronary beds of patients with SCAD.
The estimated prevalence of FMD among patients with SCAD varies according to the modality of screening for FMD. In a small study of 12 patients with SCAD who underwent whole-body MRA combined with duplex ultrasound of the renal and carotid arteries, the prevalence of FMD was ~16%. 172 In contrast, when using a combination of renal or iliac artery injection during coronary angiography or CTA/MRA, the prevalence of FMD findings among patients with SCAD ranges from 45% to 62.7%.171,173 FMD of extracoronary vascular beds may be more frequent among those SCAD patients with a higher coronary tortuosity score. 16 In current series, the most predominantly affected vascular beds are the renal, carotid/vertebral, and iliac arteries.95,146,173–175 In three studies in which the information was available, 29–70% of SCAD patients with FMD extracoronary lesions had involvement of two or more vascular beds.95,171,173 Extracoronary FMD associated with SCAD appears to be mostly, if not only, of the multifocal type. 173 Finally, besides typical FMD multifocal lesions, other extracoronary vascular abnormalities, such as aneurysms, dissections, irregularities, undulations and/or tortuosity, have been reported in a substantial proportion of SCAD survivors.95,173 Accordingly, it appears appropriate to recommend imaging of all vessels, from brain to pelvis, at least once in all patients who have had SCAD, usually with CTA or MRA, in order to assess for FMD and other non-coronary arterial abnormalities.
Whereas FMD is highly prevalent among patients with SCAD, coronary dissection is an uncommon occurrence among patients with FMD. According to the US Registry, 10.5% (25/237 dissections) of patients with arterial dissection experienced coronary dissection; however, among all patients in the Registry, coronary dissection was only reported in 2.7%. 1 Thus, it is clear that SCAD, although occurring among patients with FMD more frequently than in the general population, is still an uncommon event in large FMD patient registries. Although it is possible that coronary tortuosity is more frequent in patients with classical extracoronary FMD, the performance of non-invasive imaging modalities, such as coronary CTA, for detection of such abnormalities has not been studied and, anyhow, identification of such lesions will not influence patient management.16,176 Therefore, at this time, screening for coronary FMD in patients without angina is not recommended.
Is there coronary FMD beyond SCAD?
Though a link between FMD and SCAD has been established, more controversial is, firstly, whether SCAD is a distinct entity or simply a clinical complication of FMD, and, secondly, whether there are definite coronary manifestations of FMD other than coronary artery dissection.
A key aspect of the first controversy, whether SCAD effectively equals FMD, is the difference between the histopathological descriptions that form the historical basis of both of these conditions and the clinical and angiographic syndromes, which currently define these diagnoses. Two sites of coronary FMD that are well described histologically are aorto-ostial coronary left mainstem FMD and small vessel FMD affecting arterial branches supplying the conduction system (e.g. atrioventricular and sinoatrial nodal arteries).177–187 Both have been associated with sudden cardiac death in rare post mortem reports in adults and children. However, although histopathologically consistent with FMD, these patterns of disease appear distinct from the clinical phenotype of both ‘typical’ SCAD and ‘classical’ renal and/or cerebrovascular multifocal FMD. Thus, these histopathological entities probably represent distinct clinical entities.
Among patients with SCAD who are found to have FMD, it is unclear if SCAD occurs at sites of pre-existent subclinical coronary FMD or, more generally, if coronary manifestations can be definitively attributed to FMD per se. A number of case reports describe coronary histology consistent with FMD in post mortem cases of SCAD, but others do not.162,188–192 Angiographic and intracoronary imaging abnormalities have been described from patients with SCAD and FMD, but such findings do not appear universal among patients with SCAD and have not been correlated with histologic findings.193–195 Furthermore, series reporting follow-up imaging after conservatively managed SCAD usually describe complete restoration of angiographic coronary architecture with healing of the false lumen, although this could miss histological abnormalities which do not affect luminal geometry.145,146,149,150,153 Therefore, pending detailed post mortem SCAD series, coupled with a systematic study of the coronary vascular bed in patients with FMD without SCAD, coronary FMD remains an elusive entity.
Follow-up and longitudinal care
FMD is a chronic vascular disease that requires longitudinal care focused on medical therapy as well as periodic imaging of affected vascular beds. It is the consensus of the writing committee that after initial comprehensive evaluation, patients with FMD be seen in follow-up at least annually by a health care provider who has experience in management of this disease. Patients with more severe symptoms or disease may require more frequent follow-up. Clinical evaluation during follow-up should include: history of interval vascular events, evaluation of symptoms that may be associated with FMD (e.g. migraine headaches, neck pain, pulsatile tinnitus, claudication, mesenteric angina), and assessment of blood pressure control. Evaluation should also include measurement of blood pressure and vascular physical examination (for pulse deficits and bruits). Adherence to medical therapy, particularly to an antiplatelet agent and medications for treatment of hypertension, should be assessed, along with potential adverse reactions to these medications. For patients with renal artery involvement, blood chemistries for renal function and serum electrolytes should be monitored at least annually, along with periodic urinalysis to screen for albuminuria in patients with other concomitant risk factors. Education should include the review of potential warning signs and symptoms of TIA, stroke, and arterial dissection (CeAD or SCAD), and the need to seek immediate medical care should any develop.
At this time, data are insufficient to recommend a specific algorithm for follow-up imaging studies for patients with FMD. Imaging surveillance, including choice of imaging modality and frequency of imaging, must be customized to each patient based upon the nature and severity of symptoms, distribution of vascular bed involvement, extent and severity of arterial lesions, and the presence or absence of arterial dissections or aneurysms (and aneurysm size), as well as local imaging resources and experience. Patients who have undergone revascularization procedures, such as renal angioplasty, may require more frequent imaging surveillance, particularly within the 2 years following the procedure (see above).
Follow-up during pregnancy
Pre-conceptive counseling with a health care provider with experience in the management of FMD as well as a high-risk obstetrician or maternal fetal medicine specialist may be helpful for patients with FMD who are contemplating pregnancy, particularly patients with high-risk features such as prior history of CeAD or SCAD or those with poorly controlled hypertension. Patients with FMD who decide to become pregnant require more intensive follow-up throughout pregnancy with a customized care plan and close monitoring by a team of health care providers that generally includes a high-risk obstetrician or maternal fetal medicine specialist and a provider with expertise in FMD. A plan for delivery, including planned caesarian section or facilitated second phase of labor for vaginal delivery, should be customized to the specifics of each patient’s case, including prior history of dissection or presence of an aneurysm. Though there are limited data available, literature suggests a significantly increased risk of pre-eclampsia among women with renal FMD.196,197 Monitoring for the development of hypertension throughout pregnancy and management of pregnancy-related hypertension requires frequent clinical follow-up throughout each trimester of pregnancy and in the immediate post-partum period.
Impact of FMD on quality of life and the role of patient associations
See the online supplement for discussion of quality of life considerations and international FMD patient associations.
Emerging biomarkers and future directions
See the online supplement for discussion of ultrasound echo tracking and the ‘triple signal’, fibroblast-based investigation, and ultra-high resolution ultrasound of the artery wall.
Current research priorities
Survey of the writing committee initially identified 28 research topics for further investigation ranging from studies related to the pathogenesis (genetic and environmental) of FMD, its epidemiology and natural history, diagnosis and clinical management, and strategies to optimize patient and health care provider awareness. These topics were reviewed and ranked by the full writing committee to identify its top 10 research priorities for FMD (Table 7). It is intended that this list serves to motivate basic, clinical, and translational investigators to pursue the study of FMD, and that scientific organizations may consider these topics for future strategic research and funding initiatives.
Supplemental Material
Supplemental_Emerging_biomarkers_and_future_directions_final – Supplemental material for First International Consensus on the diagnosis and management of fibromuscular dysplasia
Supplemental material, Supplemental_Emerging_biomarkers_and_future_directions_final for First International Consensus on the diagnosis and management of fibromuscular dysplasia by Heather L Gornik (Co-Chair), Alexandre Persu (Co-Chair), David Adlam, Lucas S Aparicio, Michel Azizi, Marion Boulanger, Rosa Maria Bruno, Peter de Leeuw, Natalia Fendrikova-Mahlay, James Froehlich, Santhi K Ganesh, Bruce H Gray, Cathlin Jamison, Andrzej Januszewicz, Xavier Jeunemaitre, Daniella Kadian-Dodov, Esther SH Kim, Jason C Kovacic, Pamela Mace, Alberto Morganti, Aditya Sharma, Andrew M Southerland, Emmanuel Touzé, Patricia van der Niepen, Jiguang Wang, Ido Weinberg, Scott Wilson, Jeffrey W Olin and Pierre-Francois Plouin in Vascular Medicine
Supplemental Material
Supplemental_Impact_of_FMD_on_QoL_and_role_of_patient_assoc_final – Supplemental material for First International Consensus on the diagnosis and management of fibromuscular dysplasia
Supplemental material, Supplemental_Impact_of_FMD_on_QoL_and_role_of_patient_assoc_final for First International Consensus on the diagnosis and management of fibromuscular dysplasia by Heather L Gornik (Co-Chair), Alexandre Persu (Co-Chair), David Adlam, Lucas S Aparicio, Michel Azizi, Marion Boulanger, Rosa Maria Bruno, Peter de Leeuw, Natalia Fendrikova-Mahlay, James Froehlich, Santhi K Ganesh, Bruce H Gray, Cathlin Jamison, Andrzej Januszewicz, Xavier Jeunemaitre, Daniella Kadian-Dodov, Esther SH Kim, Jason C Kovacic, Pamela Mace, Alberto Morganti, Aditya Sharma, Andrew M Southerland, Emmanuel Touzé, Patricia van der Niepen, Jiguang Wang, Ido Weinberg, Scott Wilson, Jeffrey W Olin and Pierre-Francois Plouin in Vascular Medicine
Supplemental Material
Supplemental_Table_1_-_rev – Supplemental material for First International Consensus on the diagnosis and management of fibromuscular dysplasia
Supplemental material, Supplemental_Table_1_-_rev for First International Consensus on the diagnosis and management of fibromuscular dysplasia by Heather L Gornik (Co-Chair), Alexandre Persu (Co-Chair), David Adlam, Lucas S Aparicio, Michel Azizi, Marion Boulanger, Rosa Maria Bruno, Peter de Leeuw, Natalia Fendrikova-Mahlay, James Froehlich, Santhi K Ganesh, Bruce H Gray, Cathlin Jamison, Andrzej Januszewicz, Xavier Jeunemaitre, Daniella Kadian-Dodov, Esther SH Kim, Jason C Kovacic, Pamela Mace, Alberto Morganti, Aditya Sharma, Andrew M Southerland, Emmanuel Touzé, Patricia van der Niepen, Jiguang Wang, Ido Weinberg, Scott Wilson, Jeffrey W Olin and Pierre-Francois Plouin in Vascular Medicine
Footnotes
Acknowledgements
The authors acknowledge Dr Christopher Bajzer (Cleveland Clinic), Dr Robert Lookstein (Mount Sinai Medical Center), Dr Alan Matsumoto (University of Virginia), and Dr Sanjay Misra (Mayo Clinic) for their insights on renal FMD and prior participation in working groups of the International FMD Research Network focused on renal angiography and angioplasty, which formed a foundation for Table 6. The authors thank Ms Marianne Khoury (Cleveland Clinic) for her assistance in coordinating and formatting the manuscript; Dr Laurent Toubiana (INSERM UMRS 1142 LIMICS/IRSAN, Paris, France) and Dr Silvia Di Monaco (Cliniques Universitaires Saint-Luc, Brussels, Belgium/AOU Città della Salute e della Scienza, Turin, Italy) for data extraction and analysis of the European FMD Registry (Tables 4 and 5); and Dr Xiaokui Gu (University of Michigan) for data extraction and analysis of the US Registry for FMD (Tables 4 and 5). They also wish to acknowledge Dr Pasquale Scoppettuolo (Hôpital Erasme, Brussels, Belgium) for providing panel C of Figure 1, Dr Robert Lookstein for providing panels A–C of Figure 2, Professor Patrick Chenu and Professor Frank Hammer (Cliniques Universitaires Saint-Luc, Brussels, Belgium) for panels A and C of ![]() , respectively, and Dr Lucas Aparicio (Hospital Italiano, Buenos Aires, Argentina) for panel B of the same figure. Dr David Adlam wishes to acknowledge the ESC-ACCA SCAD study group and the BeatSCAD organization. Finally, Mrs Cathlin Jamison wishes to acknowledge Dr Véronique Godin (FMD-Be) for fruitful discussion and contribution to the section on the role of patient associations. The authors thank all of the patients who have participated in international registries and research studies of FMD, CeAD, and SCAD, as these studies have greatly helped to advance our understanding of these diseases.
, respectively, and Dr Lucas Aparicio (Hospital Italiano, Buenos Aires, Argentina) for panel B of the same figure. Dr David Adlam wishes to acknowledge the ESC-ACCA SCAD study group and the BeatSCAD organization. Finally, Mrs Cathlin Jamison wishes to acknowledge Dr Véronique Godin (FMD-Be) for fruitful discussion and contribution to the section on the role of patient associations. The authors thank all of the patients who have participated in international registries and research studies of FMD, CeAD, and SCAD, as these studies have greatly helped to advance our understanding of these diseases.
This contribution is being co-published in the following journals: Journal of Hypertension and Vascular Medicine. There will be minor differences in the version published in Vascular Medicine due to copy-editing differences.
Declaration of conflicting interests
The authors declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: Drs Gornik and Olin are non-compensated members of the Medical Advisory Board of the FMD Society of America (FMDSA), a non-profit organization. Ms Pamela Mace is an employee of the FMDSA. The other authors declared no conflict of interest.
Funding
The authors have disclosed the following sources of funding for the research, authorship, and/or publication of this article. Dr. Froehlich has received funding to the Michigan Clinical Outcomes Research and Reporting Program (MCORRP) from the FMDSA to support the US Registry for FMD. Dr. Ganesh has received support from HL139672 and the Doris Duke Charitable Foundation. The other authors have no financial disclosures related to this article.
Supplemental material
The supplementary material is available online with the article.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.