
Abstract

Fibromuscular dysplasia (FMD) is a noninflammatory, nonatherosclerotic arterial disease that can affect any artery but most commonly affects the renal, carotid, and vertebral arteries, predisposing to stenosis, aneurysm, dissection, and/or tortuosity.1–3 While headache is a common symptom reported by patients with FMD, little is known about this relationship.4,5 The etiology of FMD is not known, nor is it understood why such a high percentage of patients with FMD experience headaches. 6 In addition to FMD, patients with associated vascular abnormalities, such as intracranial aneurysm and cervical carotid and vertebral artery dissection, also commonly experience headache.5,7,8
The aim of this study was to report the frequency and characteristics of headache in a cohort of patients enrolled in the United States Registry for FMD and to identify clinical factors associated with the presence of this symptom. From 2009 through 2016, 1433 adult patients 18 years of age and older were enrolled in the Registry. Eligibility for enrollment was determined by site investigators based on identifying the characteristic appearance of multifocal or focal FMD from vascular imaging in at least one vascular bed.2,5 Eligible subjects provided written informed consent.
Demographic and clinical data, family history, headache-related variables, presenting signs and symptoms at the time of FMD diagnosis, and medications taken at the time of enrollment were recorded. An assessment of headache at initial Registry enrollment included query for presence of headache, type of headache (migraine or other), frequency of headache, whether headache was associated with menses, and whether headache(s) required suppressive medication. The Institutional Review Board (IRB) at the University of Michigan, the Data Coordinating Center for the US Registry of FMD, approved this study (HUM00022250). In addition, all participating sites in the Registry obtained individual institutional IRB approval.
Patients were categorized into two groups: those with and those without reported headaches at the time of Registry enrollment. Univariate analysis was conducted by comparing demographics, past medical history, symptoms and signs at time of FMD diagnosis, arterial bed involvement, and family history between the two groups using Student’s t-tests, Wilcoxon rank-sum tests, chi-squared tests and Fisher’s exact tests. Variables with p < 0.1 and those deemed clinically important were further tested for independent significance in multivariable logistic regression analysis. A Mantel–Haenszel chi-squared test was used to examine whether patients who had a history of depression experience more frequent headaches than patients without a history of depression. A two-sided p-value was considered statistically significant as p < 0.05. All analyses were performed with statistical software SAS 9.4 (SAS Institute Inc., Cary, NC, USA).
Complete headache information was available in 1251 (87%) patients, which comprise the population included in this report. The mean age of the study population was 56.0 ± 12.4 years. The majority were women (n = 1177, 94.1%) and less than 5% reported a family history of FMD. A total of 844 (67.5%) patients reported a history of headache, while 407 (32.5%) did not report headache. Univariate analysis showed that patients with headache were more likely to have extracranial carotid or vertebral artery FMD, be diagnosed at a younger age, have a history of aneurysm or dissection in the extracranial carotid, intracranial or vertebral arteries, have pulsatile tinnitus or stroke at the time of FMD diagnosis, and have a history of depression, anxiety, and dizziness. Patients with headache were less likely to have hypertension at the time of FMD diagnosis (59.5% vs 65.3%, p = 0.042). Patients with depression reported daily (37.8% vs 24.0%) or weekly (31.1% vs 26.0%) headaches more frequently as compared to patients without depression (p = 0.003).
Subsequent multivariable analysis confirmed patients with headache were more likely to have a history of extracranial carotid/intracranial/vertebral dissection (odds ratio (OR) 2.44, p < 0.001), extracranial carotid/intracranial/vertebral aneurysm (OR 2.10, p = 0.007), reported symptom of dizziness (OR 2.57, p < 0.001) and/or pulsatile tinnitus (OR 2.30, p < 0.001), and be diagnosed at a younger age (50.6 ± 13.8 years vs 58.0 ± 13.8 years, OR 1.48 for each 10-year decrease in age, p < 0.001) than those without headache (Figure 1).
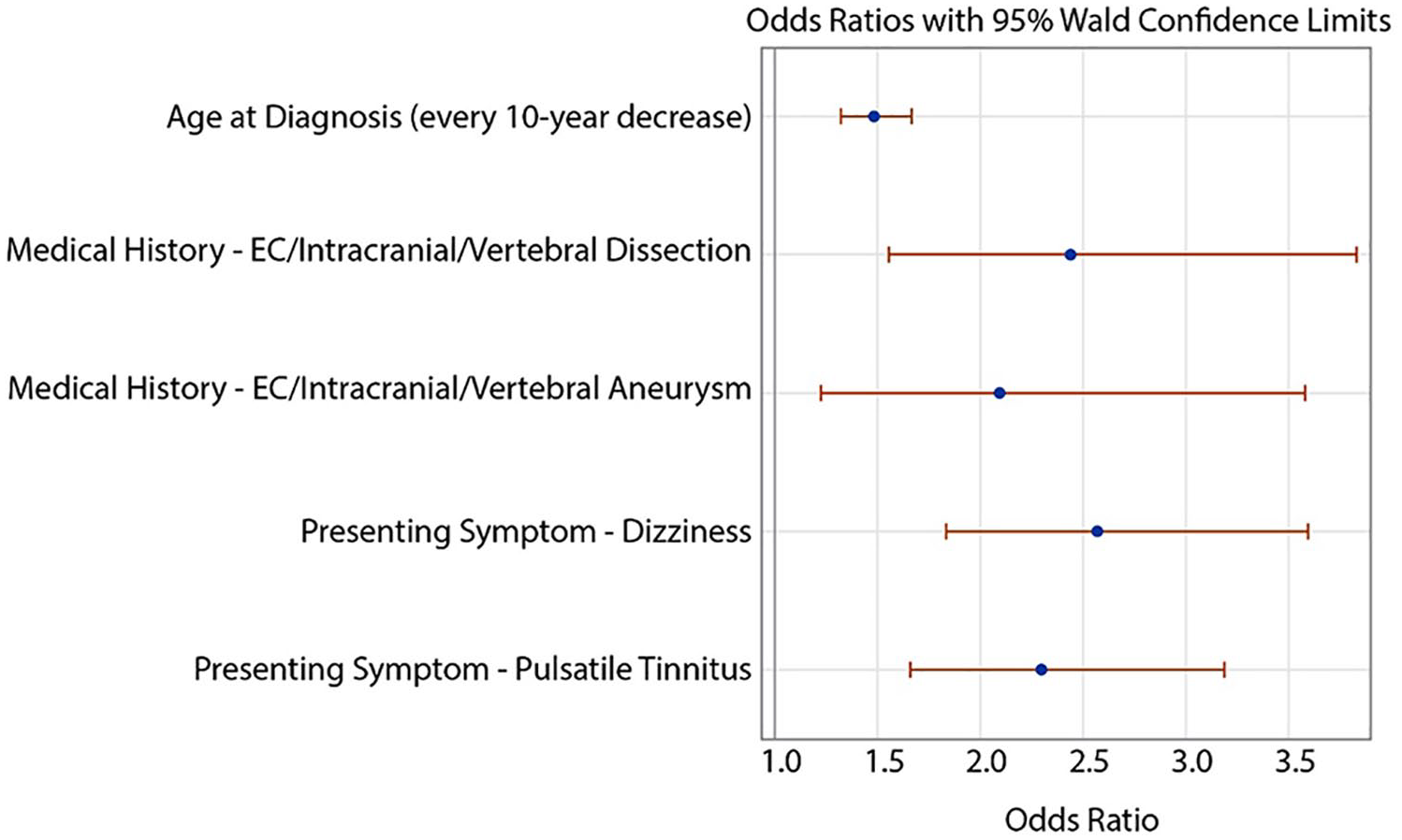
Clinical characteristics associated with headache among patients with FMD in the United States Registry.
Among 369 patients with headache who reported frequency of symptoms, 101 (27.4%) reported daily headaches and 99 (26.8%) reported weekly headaches, while 169 (45.8%) reported infrequent headaches. Headache type was reported in 763/844 (90.4%) patients. Of those, 398/763 (52.2%) described migraine type, 78/763 (10.2%) reported tension type, 76/725 (10.5%) reported an association of headache with menstruation (i.e. around the time of the menstrual period), and 113/763 (14.8%) patients reported taking suppressive medication.
In a large registry-based cohort of patients with FMD, approximately two-thirds of patients experience headaches (67.5%). Among those, more than half experienced migraine-type headaches with episodes occurring frequently (daily or weekly). Headache among patients with FMD was associated with younger age at the time of FMD diagnosis, symptoms of dizziness and pulsatile tinnitus, and a history of extracranial carotid, intracranial, or vertebral dissection or aneurysm. Patients with a history of depression were more likely to have frequent headaches.
As is the case with all Registry data, this study is observational and descriptive. The lack of a non-FMD control group is another limitation of this study. However, in comparison with our findings, it has been previously reported that approximately 20.7% of adult women in the general population experience migraines or severe headaches, 9 of which 15.7% report vertigo or dizziness. 10 Given the variability in practice patterns among the various Registry centers, as well as the limitations of available data collected in the Registry, the optimal treatment of patients with headache related to FMD cannot be determined from this report. Given the prevalence of headache as a potentially morbid clinical manifestation among patients with FMD, additional study should focus on understanding mechanisms of headache, opportunities for prevention and treatment of vascular complications associated with headache (i.e. cerebrovascular aneurysms and dissections), and optimal treatments for preventive and abortive therapies in this unique patient population.
Footnotes
Acknowledgements
We thank Rachel Krallman and Eva Kline-Rogers of Michigan Clinical Outcomes Research and Reporting Program (MCORRP) for their work coordinating the US Registry for FMD. We thank Pamela Mace, Executive Director of the Fibromuscular Dysplasia Society of America for her support of the Registry and its investigators. We thank all patients enrolled in the US Registry for FMD for their participation and support.
Dr Naomi Hamburg served as Guest Editor for this manuscript.
Declaration of conflicting interests
The authors declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: Jeffrey W Olin and Heather L Gornik are volunteer members of the Medical Advisory Board for the Fibromuscular Dysplasia Society of America; Heather L. Gornik has equity with FlexLife Health; Bruce Gray is a nonfinancial consultant for Gore; Esther Kim participated on an advisory board for Acer Therapeutics; Andrew Southerland has research support from Diffusion Pharmaceuticals, Inc. and is a legal expert reviewer for Stroke and Vascular Neurology; James Froehlich is a consultant for Merck, Janssen, Novartis, Pfizer, and Boehringer-Ingelheim, and receives grant funding from Blue Cross Blue Shield of Michigan and the Fibromuscular Dysplasia Society of America; the remainder of the authors have no conflicts of interest to disclose.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The United States Registry for Fibromuscular Dysplasia is funded by the Fibromuscular Dysplasia Society of America, a nonprofit organization.