
Abstract
Arterial stiffness is a precursor for the development of hypertension and premature cardiovascular disease (CVD). Physical activity has been associated with lower arterial stiffness among largely White populations, but the types of activity required and whether these findings apply to Black adults remain unknown. We examined whether physical activity levels were associated with arterial stiffness among Black adults in two independent cohorts. In the Morehouse-Emory Cardiovascular (MECA) Center for Health Equity, 378 Black adults (age 52.8 ± 10.3, 39.7% male) without known CVD living in Atlanta, GA were recruited. Arterial stiffness was measured as pulse wave velocity (PWV). Total and domain-specific physical activity were assessed by self-report. Multiple linear regression models were used to investigate differences across physical activity levels after adjusting for age, sex, CVD risk factors, and socioeconomic status. Findings were validated in an independent cohort of Black adults (n = 55, age 50.4 ± 9.2, 23.6% male). After adjustment for covariates, lower arterial stiffness was associated with higher self-reported levels of sport/exercise (6.92 ± 1.13 vs 7.75 ± 1.14, p < 0.001, highest vs lowest quartile) and home/life activities (7.34 ± 1.24 vs 7.73 ± 1.07, p = 0.04, highest vs lowest quartile), but not work, active living, or the overall physical activity scores. These findings were replicated in the independent cohort where higher levels of sport/exercise remained associated with lower arterial stiffness (6.66 ± 0.57 vs 8.21 ± 0.66, p < 0.001, highest vs lowest quartile). Higher levels of sport/exercise and home/life-related physical activities (in comparison to occupational physical activity) are associated with lower arterial stiffness in Black adults.
Introduction
Black Americans have the highest prevalence of hypertension (40.8% for men and 41.5% for women) across any racial/ethnic group in the United States, which translates into disproportionate numbers of deaths from myocardial infarction, stroke, and end-stage renal disease within this vulnerable group.1–3 The biological mechanism behind these disparities has yet to be fully elucidated. Arterial stiffness, a direct manifestation of early vascular aging, often is a precursor to clinical hypertension and is associated with future adverse cardiovascular disease (CVD) outcomes.4–7 Given that Black Americans have higher arterial stiffness compared to White Americans, independent of blood pressure and other risk factors, it has been proposed that the increased prevalence of hypertension in Black individuals is mediated by abnormal arterial stiffness.8,9
Physical activity has been shown to be protective of the development of arterial stiffness in multiple populations including young adults, 10 men, 11 and women. 12 Prior studies have demonstrated that among Black Americans, physical activity, in particular sport/exercise-related activity, is associated with lower incident hypertension. 13 However, whether physical activity is associated with lower arterial stiffness among Black adults has yet to be explored, despite the higher prevalence of both arterial stiffness and incident hypertension in these individuals. Herein, our objective was to examine the association between domain-specific physical activity (active living, work, home/life, and sport/exercise) and arterial stiffness among Black adults in two independent cohorts recruited from a southern metropolitan city. We hypothesized that those reporting increased physical activity, particularly sport/exercise-related activities, would exhibit lower arterial stiffness.
Methods
Study participants
The Morehouse-Emory Cardiovascular (MECA) Center for Health Equity study included 502 individuals self-identifying as Black or African American, between the ages of 30 and 70, recruited from the community between 2016 and 2019 using convenience sampling. Further details on this study, including study design, recruitment, and data collection, have been published elsewhere. 14 Briefly, patients with known history of CVD, such as coronary artery disease, myocardial infarction, congestive heart failure, atrial fibrillation, cerebrovascular accidents, peripheral arterial disease, and cardiomyopathies were excluded. Other exclusion criteria included pregnant or lactating women, those with mobility issues or chronic diseases (human immunodeficiency virus infection, cancer, or systemic lupus erythematosus), substance abuse (alcohol or illicit drugs), and severe psychiatric illness. Participants were asked to complete study visits either at Morehouse School of Medicine or Emory University School of Medicine to complete a physical examination, questionnaires, and blood draws, conducted by trained personnel. Of the 502 participants recruited, 124 were excluded due to missing physical activity, arterial stiffness, or high-sensitivity C-reactive protein (hs-CRP) data. The study was approved by the Institutional Review Boards of both Emory University and Morehouse School of Medicine. All participants provided informed consent for study participation.
Measurement of physical activity
Physical activity was evaluated using the Jackson Heart Study (JHS) Physical Activity Questionnaire, which is composed of 30 items validated for use in Black adults and was derived from the Baecke Questionnaire of Habitual Physical Activity.13,15 The questionnaire assesses physical activity in four domains, with the goal to obtain information about participants’ physical activity in several settings: (A) active living; (B) occupational activities; (C) home, family, yard, and garden; and (D) sports and exercise. For the sport/exercise section, participants were asked to report the frequency and duration of these activities. Scores ranged from 0 to 4 for each domain, for a total physical activity score from 0 to 16, with higher scores representing higher physical activity. Participants were then stratified by quartiles of their physical activity score, with higher quartiles representing increasing amounts of physical activity. The questionnaire is presented in online Supplemental Table 1.
Replication cohort
The Morehouse and Emory Team up to Eliminate Health Disparities (META-Health) is an independent cohort of Black participants recruited between 2005 and 2010 from the Atlanta, GA metropolitan area where participants with known CVD, pregnant or lactating females, and those with known chronic illnesses (e.g., HIV, autoimmune disorders, and cancer) were excluded. Leisure-time and sports-related physical activity assessed using the Baecke Questionnaire of Habitual Physical Activity 16 and carotid-femoral pulse wave velocity (PWV) measurements were available for 55 participants. Informed consent was obtained from all study participants and the study was approved by both the Emory University and Morehouse School of Medicine Institutional Review Boards.
Measurement of arterial stiffness
We recorded PWV as a measure of arterial stiffness noninvasively using the SphygmoCor Pulse Wave Velocity system (AtCor Medical, Australia) as previously described. 17 In brief, carotid-femoral artery PWV was determined using transcutaneous Doppler flow velocity recordings simultaneously over the common carotid artery and the femoral artery. Velocity (distance/time in m/s) was calculated by measuring the time interval between electrocardiogram R-wave and the recorded waveforms at each site. The distance between sites was measured manually by the operator. Distance was measured as the number of meters between the area of femoral pulse to the area of the carotid pulse by subtracting the distance from the carotid location to the sternal notch from the distance between the sternal notch and the femoral site of measurement. At the time of study, quality control indexes were evaluated, and nonacceptable readings were discarded. Reproducibility studies in our laboratory on consecutive days on nine subjects demonstrated a coefficient of variation of 3.8% for PWV.
Measurement of hs-CRP
Hs-CRP, which represents an inflammatory biomarker, was measured by Abbott Laboratories (Abbott Park, IL, USA).
Statistical analysis
Demographic, socioeconomic, and clinical characteristics were presented by quartiles of total physical activity score. Continuous variables were reported as mean (± SD) and compared using analysis of variance tests across the quartiles. Categorical variables were reported as frequencies and proportions (%) and compared using chi-squared tests. Kruskal–Wallis nonparametric tests were performed on non-normally distributed variables.
In the MECA sample, multivariable linear regression was used to assess the relationship between quartiles of total physical activity and its domains (reference quartile 1, the lowest amount of physical activity) and measures of arterial stiffness (PWV treated as continuous variable). Covariates were added in a stepwise manner to assess the effect of additional covariate adjustment: Model 1: unadjusted; Model 2: adjusted for age, sex, systolic blood pressure (continuous), current smoker (yes vs no), diabetes (yes vs no), and hyperlipidemia (yes vs no); Model 3: Model 2 + socioeconomic status defined by income (< $25,000, $25,000 – $50,000, > $50,000), and education (high school or less, some college/tech school, college or higher); Model 4: Model 3 + hs-CRP (continuous, to account for chronic inflammation). To confirm that findings would be independent of medication use, we additionally adjusted for hypertension, lipid, and diabetes treatment.
Similarly, in the META-Health sample, multivariable linear regression was used to assess the relationship between quartiles of leisure-time and sports-related physical activity (reference quartile 1) and measures of arterial stiffness (PWV treated as continuous variable) after adjusting for age, sex, CVD risk factors as above, and socioeconomic status defined by income and education. All statistical analyses were performed using R 4.0 (R Foundation for Statistical Computing, Vienna, Austria) and p < 0.05 was considered statistically significant.
Results
The mean age was 52.8 ± 10.3 and 39.7% were male in the MECA cohort of 378 participants. Those who reported higher levels of overall physical activity were younger, more likely to be male, employed either part-time/full-time, and had lower body mass index, hs-CRP, and rates of smoking and diabetes (Table 1). Univariate predictors of PWV were age, sex, presence of hypertension, hyperlipidemia, diabetes, and the home and sport/exercise indices of the JHS Physical Activity Questionnaire (Table 2).
Demographic, socioeconomic, and clinical characteristics of the cohort stratified by quartiles (quartile 1 = lowest, quartile 4 = highest amount of physical activity) of the Total Physical Activity index.
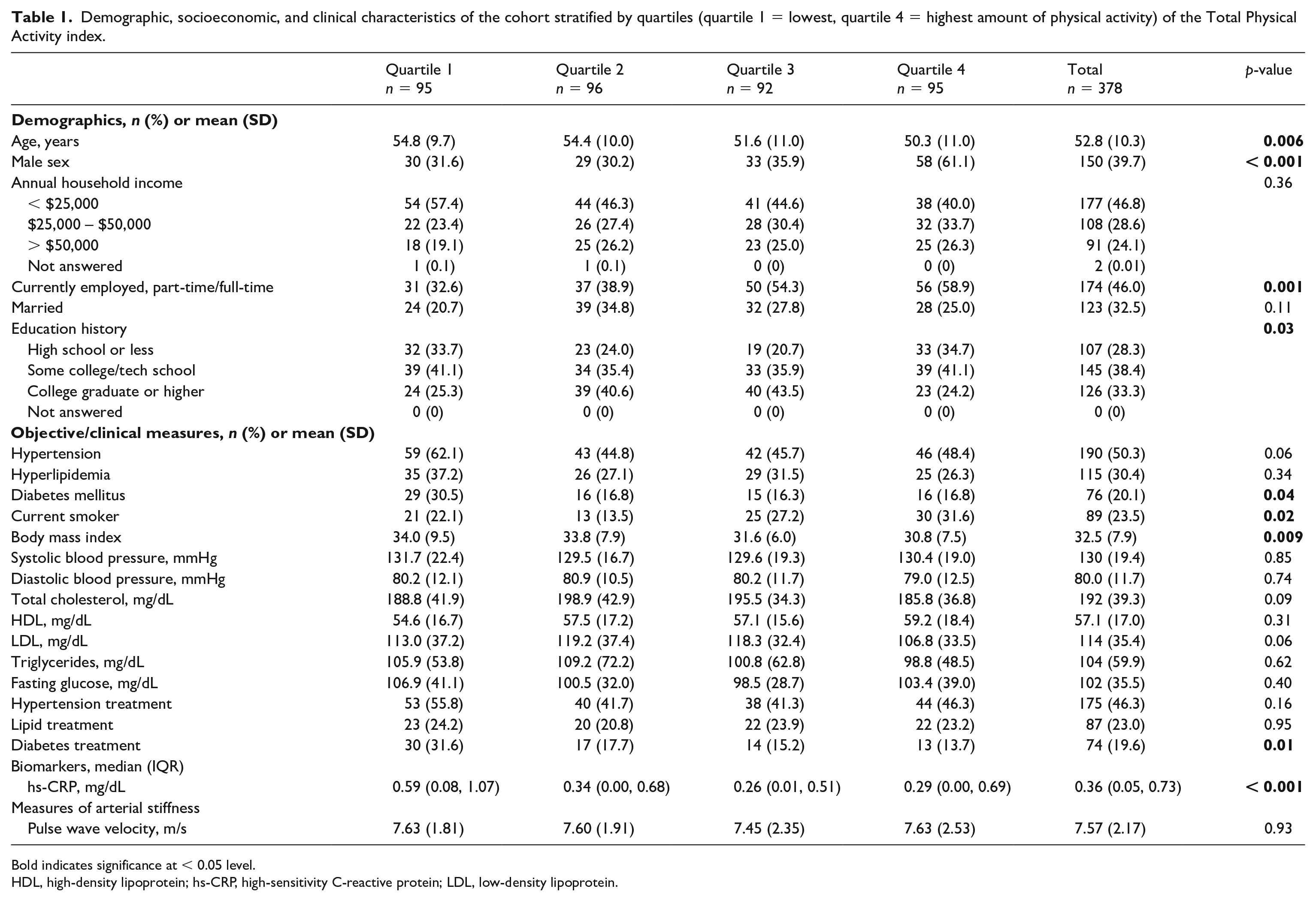
Bold indicates significance at < 0.05 level.
HDL, high-density lipoprotein; hs-CRP, high-sensitivity C-reactive protein; LDL, low-density lipoprotein.
Univariate predictors of arterial stiffness in the MECA cohort.
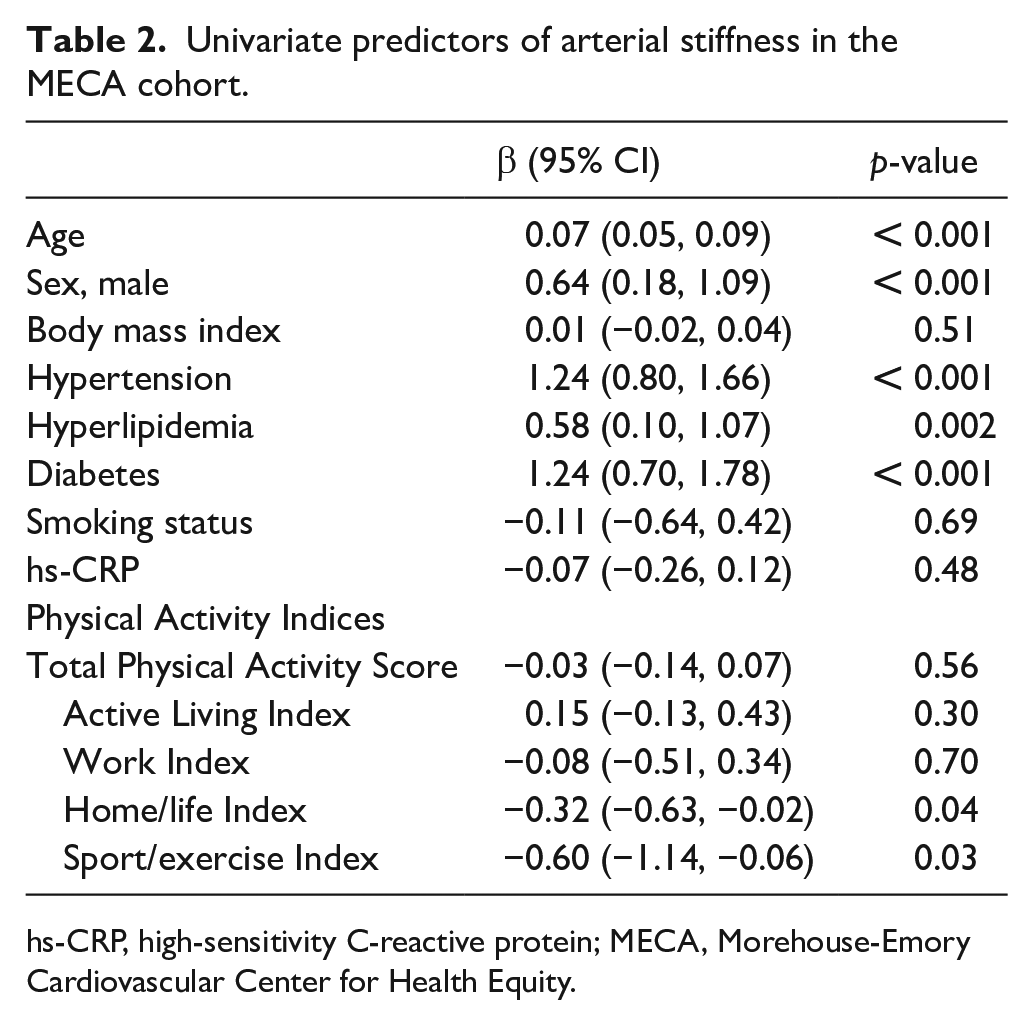
hs-CRP, high-sensitivity C-reactive protein; MECA, Morehouse-Emory Cardiovascular Center for Health Equity.
In multivariable linear regression, being in quartile 4 (highest) versus quartile 1 (lowest) of the home/life index was associated with lower arterial stiffness after adjusting for age, sex, CVD risk factors, and socioeconomic factors (Table 3). Thus, those in the highest compared to lowest quartile of home-related physical activity had a lower adjusted PWV (7.34 ± 1.24 vs 7.73 ± 1.07, p = 0.04) (Figure 1). These associations remained after additionally adjusting for hs-CRP (Table 3). Similarly, the associations remained after additionally adjusting for hypertension, lipid, and diabetes medication use.
Multivariable analysis examining the association between the Total Physical Activity index and its subcomponents by quartiles of physical activity and arterial stiffness measured as average pulse wave velocity in the MECA cohort.
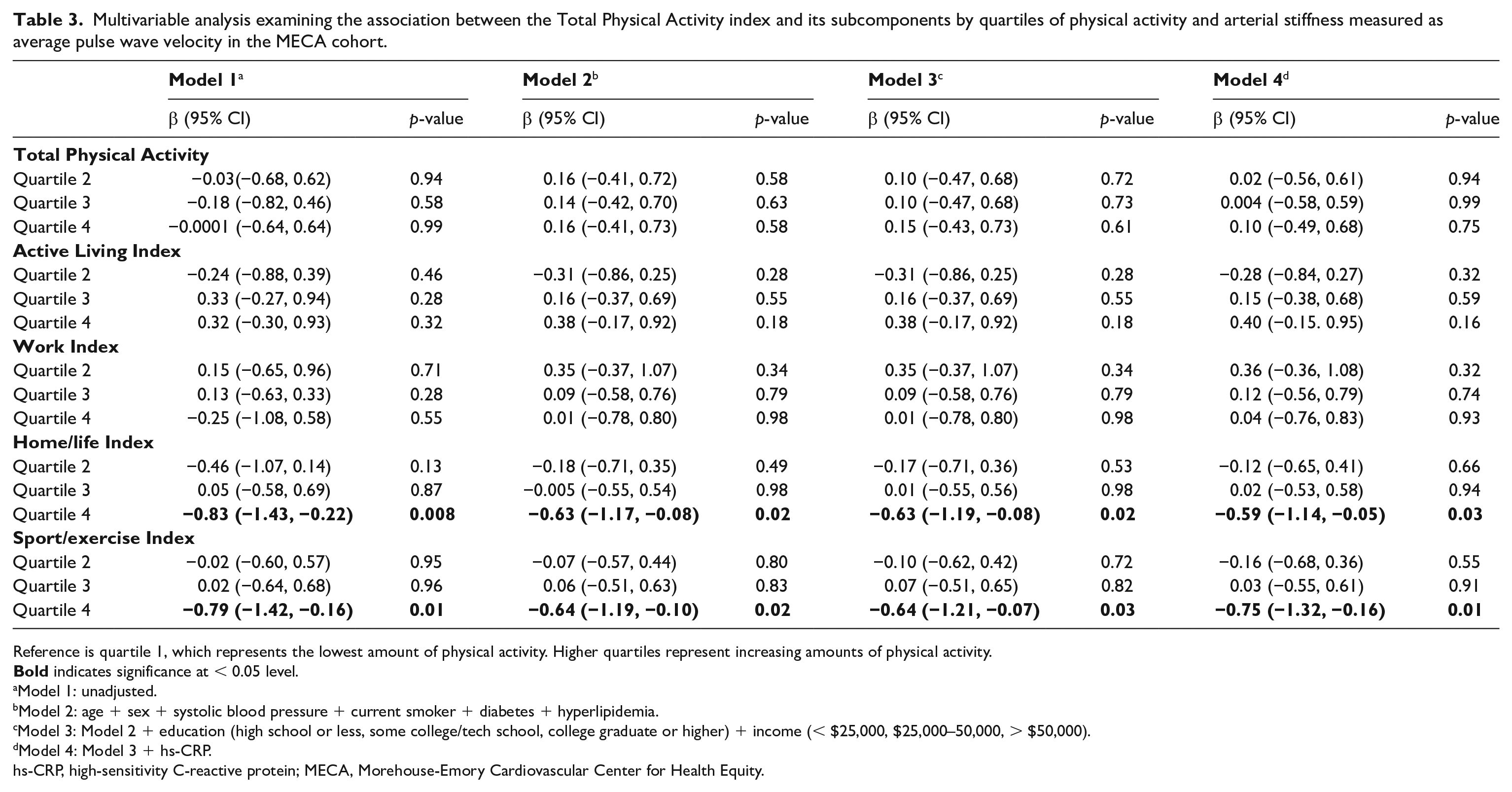
Reference is quartile 1, which represents the lowest amount of physical activity. Higher quartiles represent increasing amounts of physical activity.
Model 1: unadjusted.
Model 2: age + sex + systolic blood pressure + current smoker + diabetes + hyperlipidemia.
Model 3: Model 2 + education (high school or less, some college/tech school, college graduate or higher) + income (< $25,000, $25,000–50,000, > $50,000).
Model 4: Model 3 + hs-CRP.
hs-CRP, high-sensitivity C-reactive protein; MECA, Morehouse-Emory Cardiovascular Center for Health Equity.
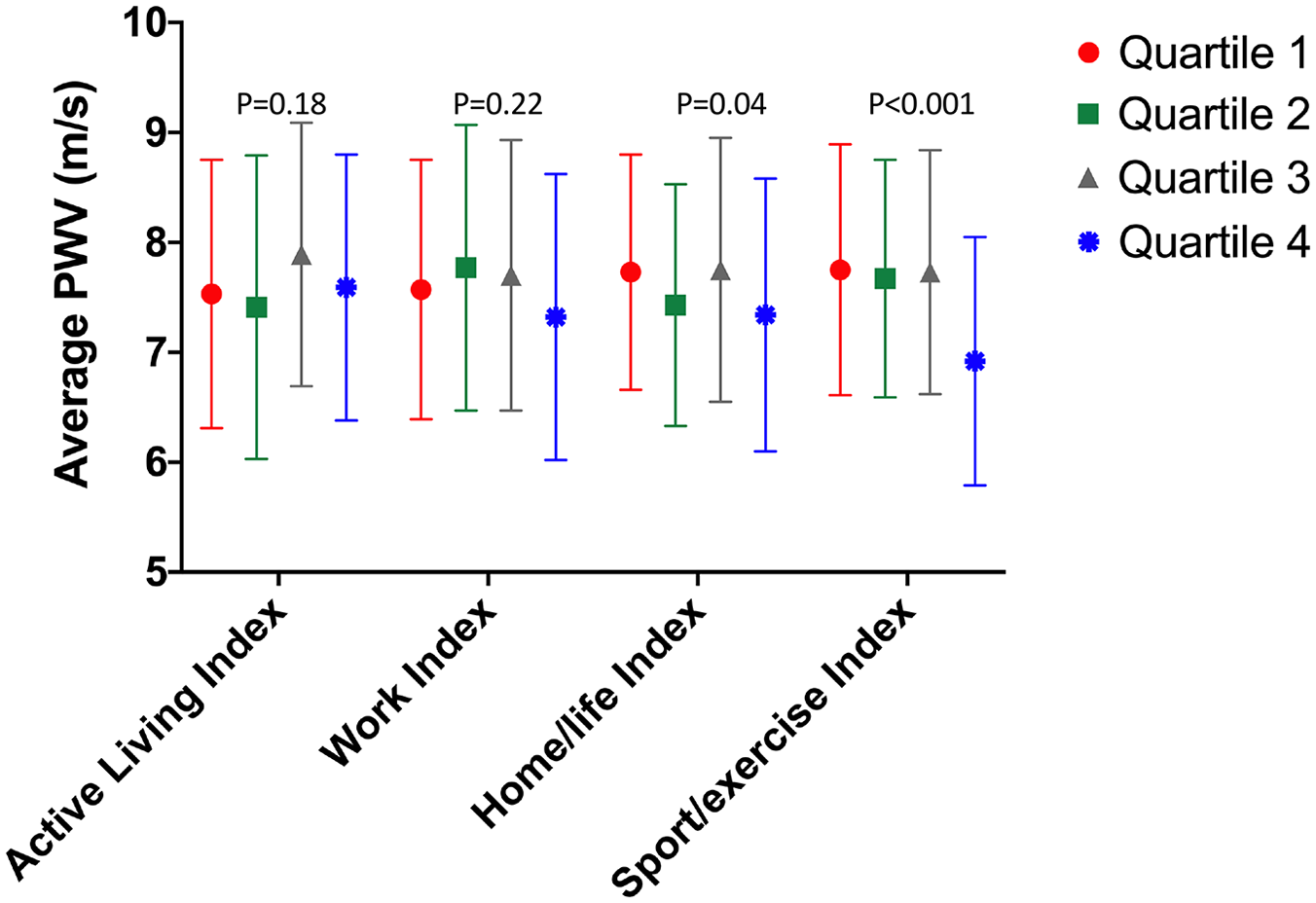
Average pulse wave velocitya stratified by quartiles of the domains of physical activity.
Reporting the highest (vs lowest) level of sport and exercise physical activity was also associated with lower arterial stiffness after stepwise adjustment for age, sex, CVD risk factors, and socioeconomic status (Table 3). Thus, those in the highest compared to lowest quartile of sport/exercise-related physical activity had lower adjusted PWV (6.92 ± 1.13 vs 7.75 ± 1.14, p < 0.001). No associations were noted for total physical activity, active living, and work indices. These associations remained after additionally adjusting for hs-CRP (Table 3). Similarly, the associations remained after additionally adjusting for hypertension, lipid, and diabetes medication use (online Supplemental Table 2).
In the META-Health replication cohort (n = 55), the mean age was 50.4 ± 9.2 and 23.6% were male (online Supplemental Table 3). Hypertension was prevalent in 41.8% of the population, and 60% had an annual household income of > $50,000. Similar to the MECA cohort, in multivariable linear regression, being in the highest versus lowest quartile of sport/exercise activity was associated with lower arterial stiffness after adjusting for the CVD risk factors (β = −1.66 [−3.14, −0.17], p = 0.03). The association remained significant after additionally adjusting for education and income (β = −1.71 [−3.28, −0.15], p = 0.04). Thus, those in the highest compared to the lowest quartile had lower adjusted PWV (6.66 ± 0.57 vs 8.21 ± 0.66, p < 0.001). No associations were noted for leisure-time activity and arterial stiffness.
Discussion
In this cross-sectional analysis of Black Americans from two separate cohorts from a major Southern metropolitan US city, we demonstrated that increased participation in sport/exercise-related activities was associated with lower arterial stiffness independent of age, sex, socioeconomic status, and traditional CVD risk factors including hypertension, hyperlipidemia, and diabetes. In addition, in the larger cohort, we also found that increased participation in home/life-related activities was independently associated with lower arterial stiffness.
Although the association between physical activity and lower arterial stiffness has been demonstrated in other populations,10–12 to our knowledge, we are the first to demonstrate it among Black Americans, where there are large CVD risk factor and outcome disparities. 18 Increased participation in sport/exercise-related activities was associated with lower risk of incident hypertension among Black participants in the JHS. 13 Similarly, increased physical activity has been associated with lower prevalence of CVD risk factors such as diabetes in Black adults. 19 In our study, we noted that the associations with arterial stiffness are independent of traditional CVD risk factors including hypertension, which suggests that the beneficial effects of higher levels of sport/exercise and home/life activities impacts vascular health upstream of the development of clinical hypertension.
Arterial stiffness, which is normally associated with age and hypertension, is a direct manifestation of early vascular aging. 5 Even in healthy cohorts without known CVD or CVD risk factors, elevated arterial stiffness is an independent predictor of future CVD events and all-cause mortality.20–23 Arterial stiffness remains an important marker when assessing vascular health because even in cohorts with a high prevalence of risk factors, its predictive value goes beyond measuring traditional risk factors, including 24-hour blood pressure.20,24 This is especially important for Black individuals, as prior studies have demonstrated that populations of black African descent have increased central arterial stiffness all throughout the life course as well as a higher increase in arterial stiffness at younger ages.8,9,25,26 Multiple racial differences in arterial physiology likely underlie such differences – for example, Black individuals have (a) impaired endothelium-dependent and -independent vasodilation compared to White individuals,27,28 (b) enhanced endothelin-1 dependent vasoconstrictor tone, 29 and (c) generate more oxidant stress leading to enhanced nitric oxide (NO) inactivation30,32 – but few studies have examined modifiable protective factors such as physical activity for arterial health in Black individuals.
Physical activity positively affects arterial stiffness and central aortic distensibility through influencing structural elements (interstitial collagen of the arterial wall), functional elements (vasoconstrictor tone, endothelial function), and reducing chronic inflammation, which in turn improves endothelial function.11,32–34 Our findings were independent of the hs-CRP level, suggesting that physical activity, in particular sport/exercise and home/life activities, lead to improved arterial stiffness through mechanisms beyond inflammation in Black adults. As described above, Black individuals have impaired endothelial function compared to White individuals27–29 and, therefore, our findings have important public health ramifications as one means of improving cardiovascular health in Black adults maybe through targeting physical activity. Further research assessing the optimal amount of physical activity that is required to improve vascular health among Black adults is warranted.
Whereas select subdomains of the physical activity demonstrated associations with arterial stiffness, total physical activity did not, which highlights the importance of assessing domain-specific activity types among Black Americans. Prior literature has demonstrated the importance of distinguishing between leisure and nonleisure physical activity as Black Americans engage in high amounts of occupational activity but lower leisure-time activity.35,36 We add to the literature by demonstrating that leisure-time versus occupational activities are associated with lower arterial stiffness and, thus, better cardiovascular health. Although our findings are consistent with the JHS where sport/exercise activities were associated lower incident hypertension, we further add to the literature by demonstrating that Black individuals who are active around the home and garden also have better vascular health. Thus, encouraging leisure-time activities including sport/exercise and home/life activities is important in improving cardiovascular health among Black adults.
Study strengths and limitations
Limitations firstly include the fact that the physical activity data are self-reported and not confirmed with wearables. Secondly, although the Black population in the Atlanta metropolitan area is large (> 1.6 million) 37 and diverse socioeconomically, our study may not represent all Black communities in the US. However, our findings are consistent with prior studies conducted among Black adults in different geographic locales that investigated hypertension. 13 Thirdly, our data are cross-sectional and longitudinal studies are required to further determine causality and decipher mechanisms. One of the major strengths of our study is that we validated our findings in an independent cohort. In addition, our data provide a mechanistic pathway through which physical activity improves vascular health and thus impedes development of hypertension in a group with very high prevalence.
Conclusion
In summary, we demonstrated that higher levels of sport/exercise and home/life activities are independently associated with lower arterial stiffness, a marker of early vascular aging that predisposes individuals to greater CVD risk. Future studies are needed to determine whether interventions designed to improve home/life/sport activities in Black Americans will improve cardiovascular health in this population.
Supplemental Material
sj-pdf-1-vmj-10.1177_1358863X211032725 – Supplemental material for Association of physical activity with arterial stiffness among Black adults
Supplemental material, sj-pdf-1-vmj-10.1177_1358863X211032725 for Association of physical activity with arterial stiffness among Black adults by Shabatun J Islam, Nour Beydoun, Anurag Mehta, Jeong Hwan Kim, Yi-An Ko, Qingchun Jin, Peter Baltrus, Matthew L Topel, Chang Liu, Mahasin S Mujahid, Viola Vaccarino, Mario Sims, Kiran Ejaz, Charles Searles, Sandra B Dunbar, Tené T Lewis, Herman A Taylor, Priscilla Pemu and Arshed A Quyyumi in Vascular Medicine
Footnotes
Acknowledgements
We would like to thank the participants of MECA and META-Health, as well as the research coordinators, without whom the studies would not have been possible.
Data Availability
Data are available from the corresponding author on reasonable request.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The American Heart Association 0000031288, Abraham J & Phyllis Katz Foundation, Byron Williams Jr, MD Fellowship Fund, and the National Institutes of Health T32 HL130025 & T32 HL007745-26A1.
Supplementary material
The supplementary material is available online with the article.