
Abstract
Introduction:
Poor quality neighborhood environments are independent risk factors for cardiovascular disease (CVD) but are understudied in Black adults, who face large CVD health disparities. Arterial stiffness, a marker of early vascular aging, precedes development of hypertension and adverse CVD events but the effect of neighborhood on arterial stiffness among Black adults remains unknown.
Objective:
We compared the association between neighborhood environment and arterial stiffness among Black adults in Jackson, MS and Atlanta, GA.
Methods:
We studied 1582 Black adults (mean age 53 ± 10, 35% male) living in Jackson, MS from the Jackson Heart Study (JHS) and 451 Black adults (mean age 53 ± 10, 39% male) living in Atlanta, GA from the Morehouse-Emory Cardiovascular Center for Health Equity (MECA) study, without known CVD. Neighborhood problems (includes measures of aesthetic quality, walking environment, food access), social cohesion (includes activity with neighbors), and violence/safety were assessed using validated questionnaires. Arterial stiffness was measured as pulse wave velocity (PWV) using magnetic resonance imaging in JHS and as PWV and augmentation index (AIx) using applanation tonometry (SphygmoCor, Inc.) in MECA. Multivariable linear regression models were used to examine the association between neighborhood characteristics and arterial stiffness, adjusting for potential confounders.
Results:
Improved social characteristics, measured as social cohesion in JHS (β = −0.32 [−0.63, −0.02], p = 0.04) and activity with neighbors (β = −0.23 [−0.40, −0.05], p = 0.01) in MECA, were associated with lower PWV in both cohorts and lower AIx (β = −1.74 [−2.92, − 0.56], p = 0.004) in MECA, after adjustment for CVD risk factors and income. Additionally, in MECA, better food access (β = −1.18 [−2.35, − 0.01], p = 0.05) was associated with lower AIx and, in JHS, lower neighborhood problems (β = −0.33 [−0.64, − 0.02], p = 0.04) and lower violence (β = −0.30 [−0.61, 0.002], p = 0.05) were associated with lower PWV.
Conclusion:
Neighborhood social characteristics show an independent association with the vascular health of Black adults, findings that were reproducible in two distinct American cities.
Introduction
Neighborhood of residence is an independent risk factor for poor cardiovascular health. 1 Those living in socioeconomically disadvantaged neighborhoods not only have a higher burden of cardiovascular disease (CVD) risk factors, but also have higher CVD incidence and mortality.2–6 The impact of neighborhood characteristics on cardiovascular health (CVH) is of critical importance for Black adults, a community that has been traditionally understudied and continues to suffer from disparate levels of CVD when compared to White individuals. 7 In addition, Black adults have also been disproportionately affected by the rapidly changing dynamics (i.e. gentrification) of many neighborhoods in the US, 8 manifesting as poor health outcomes.9,10 Recently, our group demonstrated that poor neighborhood social characteristics (e.g. low social cohesion) are associated with a higher burden of CVD risk factors such as poor diet and exercise habits, and prevalent obesity in Black adults in Atlanta, GA. 11 However, whether these differences in CVH due to neighborhood environments are being manifested biologically as subclinical CVD have not been elucidated.
Higher arterial stiffness, a direct manifestation of early vascular aging, is a marker of subclinical CVD and a precursor to clinical hypertension, which is then associated with future adverse CVD outcomes.12–15 Since Black adults have both the highest prevalence of hypertension across any racial ethnic group in the US and higher arterial stiffness compared to White individuals, it has been proposed that the increased prevalence of hypertension in this group could be mediated in part through early vascular aging.16–20 Thus, it becomes important to understand protective factors, including neighborhood characteristics, that will slow the development of arterial stiffness and improve CV outcomes in this group. Therefore, we examined specific features of neighborhood physical (i.e. violence, aesthetic quality, food access, etc.) and social (i.e. cohesion) environments in relation to arterial stiffness, a marker of subclinical CVD, among Black adults from two distinct Southern US cities: Jackson, MS and Atlanta, GA. We hypothesized that favorable neighborhood physical and social characteristics would be associated with lower arterial stiffness among Black adults in both of these cities, and that this association would be independent of cardiovascular disease risk factors and individual income level.
Methods
Study population
Jackson Heart Study (JHS)
We used data from the JHS, a single-site, community-based cohort study of Black adults (n = 5306) from the tri-county (Hinds, Madison, and Rankin) area of the Jackson, Mississippi metropolitan area. The JHS is a longitudinal study of genetic and environmental risk factors for CVD among Black adults; details about recruitment, data collection, and study variables are described elsewhere.21,22 We excluded participants with known CVD (n = 1393) at baseline. Perceptions of neighborhood characteristics, household income, education, and census tract information were drawn from JHS Exam 1, which was conducted between 2000 and 2004. Magnetic resonance imaging (MRI)-derived arterial stiffness measures were available in 1662 individuals, together with clinical characteristics (blood pressure, body mass index [BMI], diabetes status, etc.) from JHS Exam 2 (2005–2008, n = 241) or JHS Exam 3 (2009–2013, n = 1421). An additional 80 individuals were excluded from the analysis due to missing data on the neighborhood measures yielding a final analytic sample of 1582. The study was approved by the institutional review boards of the University of Mississippi Medical Center, Jackson State University, and Tougaloo College and all participants provided written informed consent.
Morehouse-Emory Cardiovascular (MECA) Center for Health Equity
In the MECA study, 502 individuals between the ages of 30 and 70 self-identifying as Black or African American were recruited from 229 census tracts in the Atlanta, GA metropolitan area using convenience sampling between 2016 and 2019. Further details have been published elsewhere. 23 Those with known history of CVD (e.g. myocardial infarction, congestive heart failure, cerebrovascular accidents, coronary artery disease, peripheral arterial disease, atrial fibrillation, and cardiomyopathies) and select chronic diseases (cancer, human immunodeficiency virus infection, or lupus) were excluded. Other exclusion criteria included substance abuse (alcohol or illicit drugs), psychiatric illnesses, pregnancy, and current breastfeeding. In addition, those reporting mobility issues and thus not able to increase their exercise levels, were excluded. Participants completed a physical exam, blood draws, pulse wave velocity (PWV) and radial pulse wave analyses (measures of arterial stiffness), and questionnaires at either Morehouse School of Medicine or Emory University School of Medicine during the study visit. The institutional review boards of both institutions approved the study protocol, and all participants provided written informed consent. Of the 502 recruited for the study, 51 were excluded due to missing data on neighborhood quality measures or poor-quality data on the arterial stiffness measures, resulting in a final sample of 451 for analysis.
Self-reported neighborhood characteristics
Jackson Heart Study (JHS)
Perceptions of neighborhood characteristics were measured using the Neighborhood Health Questionnaire, a reliable and valid questionnaire previously used in studies of CVD, 24 and presented as Table S1 in the online supplementary material together with further details. Neighborhood characteristics were classified into three categories: social cohesion, problems, and violence (Table S2).25,26 Neighborhood problems included six questions that encompassed topics such as aesthetic quality, walking environment, and food access. The social cohesion scale was composed of five items, which included topics such as trust in neighbors and willingness to help neighbors. The violence scale encompassed five items, which inquired about violent neighborhood activities and safety. For analysis and interpretation purposes, measures were coded, whereby higher scores represented improved or favorable characteristics.
Morehouse-Emory Cardiovascular (MECA) Center for Health Equity
We assessed perceptions of neighborhood characteristics using the Neighborhood Health Questionnaire, a reliable and valid questionnaire previously used in studies of cardiovascular health, including the JHS, as above. 24 The questionnaire and further details are presented in the supplementary material (Table S1, available online). In brief, participants answered a series of questions pertaining to seven domains of neighborhood physical and social characteristics: aesthetic quality, walking environment, availability of healthy foods, safety, violence, social cohesion, and activities with neighbors.
Measurements of arterial stiffness
Jackson Heart Study (JHS)
Participants underwent MRI scanning on a 1.5-T whole-body MRI scanner (Siemens Espree; Siemens, Erlangen, Germany; 70 cm bore, advanced cardiac package, TIM Matrix surface coil). 27 The JHS MRI protocol was designed for consistency with the Multi-Ethnic Study of Atherosclerosis (MESA). 28 Aortic PWV was calculated from phase-contrast images acquired in the ascending and descending thoracic aorta, as previously described. 29 The intraclass correlation coefficient for PWV analyses in repeated, blinded analyses of 96 scans was 0.82.27,29
Morehouse-Emory Cardiovascular (MECA) Center for Health Equity
We recorded PWV and radial pulse wave noninvasively using the SphygmoCor PWV system (Sydney, Australia) as measures of arterial stiffness and pulse wave reflection, respectively, as previously described. 30 In brief, peripheral pressure waveforms were recorded from the radial artery at the wrist using applanation tonometry with a high-fidelity micromanometer. After 20 sequential waveforms were acquired, a validated generalized transfer function was used to estimate the corresponding central aortic pressure waveform. Augmentation index (AIx) was derived and normalized to a heart rate of 75 beats/min due to sensitivity of the measurement to heart rate.
Carotid-femoral artery PWV was determined using transcutaneous Doppler flow velocity recordings simultaneously over the common carotid artery and the femoral artery. Velocity (distance/time in m/s) was calculated by measuring the time interval between electrocardiogram R-wave and the recorded waveforms at each site. The distance between sites was measured manually by the operator. Distance was measured as the number of meters between the area of femoral pulse to the area of the carotid pulse by subtracting the distance from the carotid location to the sternal notch from the distance between the sternal notch and the femoral site of measurement. At the time of study, quality control indexes were evaluated and nonacceptable readings were discarded. Reproducibility studies in our laboratory on consecutive days on nine subjects demonstrated a coefficient of variation of 20.3% and 3.8% for AIx and PWV, respectively.
Study covariates
The following information was gathered via self-report on questionnaires using similar collection protocols across both studies: age, sex, annual household income (< $25,000, $25,000 to $50,000, > $50,000), education (less than high school, high school graduate or some college/technical school or greater), and smoking status. During the physical exam, vital signs (e.g. blood pressure) and anthropometric measurements were collected. Blood was drawn after > 6 hours of fasting to measure plasma levels of cholesterol and glucose. Further details are presented in the supplementary material (Table S2, available online).
Statistical analysis
Demographic, socioeconomic, and clinical characteristics are presented for the JHS and MECA samples, where continuous variables were reported as means (± SD) and categorical variables were reported as frequencies and proportions (%). The outcome variable was arterial stiffness measured as PWV using MRI in JHS, and as PWV and AIx using applanation tonometry (SphygmoCor, Inc.) in MECA, as described in detail above. The predictor variables were neighborhood characteristics. In order to ease comparison across the two study samples, neighborhood measures were conceptually grouped as following. Neighborhood social cohesion also includes activity with neighbors, which was separately analyzed in MECA. Neighborhood problems include measures of aesthetic quality, walking environment, and food access, which were also separately analyzed in MECA. Similarly, neighborhood violence and safety were conceptually grouped.
Generalized linear mixed regression models were constructed (with census tract-specific random intercepts to account for correlations among people living within the same neighborhood) to examine the relationship between each of the domains of neighborhood characteristics (measured as a continuous variable) and measures of arterial stiffness (PWV and AIx, measured as a continuous variable). Covariates were added in a stepwise manner to assess the effect of additional covariate adjustment: Model 1: unadjusted + height in inches (only for AIx as this measurement is dependent of height of subject); Model 2: adjusted for age + sex (male vs female) + systolic blood pressure + BMI + diabetes + smoking + height in inches (only for AIx); Model 3: Model 2 variables + socioeconomic status defined by annual household income. A final model was created substituting mean arterial pressure (MAP) for systolic blood pressure and additionally adjusting for heart rate (only for PWV as the AIx variable was already normalized to a heart rate of 75 beats per minute) and hypertension treatment. All statistical analyses were performed using R 4.0 (R Foundation for Statistical Computing, Vienna, Austria); p < 0.05 was considered statistically significant.
Results
The mean age was 53.2 ± 10.2 and 35.3% were male in the JHS sample, and in the MECA sample the mean age was 53.1 ± 10.2 and 38.9% were male (Table 1). More participants in JHS had higher annual household income (39.3% vs 20.5% had income > $50,000) and were more educated (75.1% vs 69.6% had at least some college education) in comparison to MECA. In terms of clinical variables, the prevalence of hypertension (63.2% vs 53.9%) was higher, and diabetes (8.0% vs 24.7%) and smoking (10.3% vs 23.3%) were lower in JHS, though BMI was approximately the same across both samples. In JHS, the mean PWV was 7.93 ± 6.36 m/s, whereas in MECA it was 7.61± 2.09 m/s. The mean AIx in MECA was 20.4 ± 12.8.
Demographic, socioeconomic, and clinical characteristics of the Jackson Heart Study (Jackson, MS) and the Morehouse-Emory Cardiovascular Center for Health Equity (Atlanta, GA) cohorts.
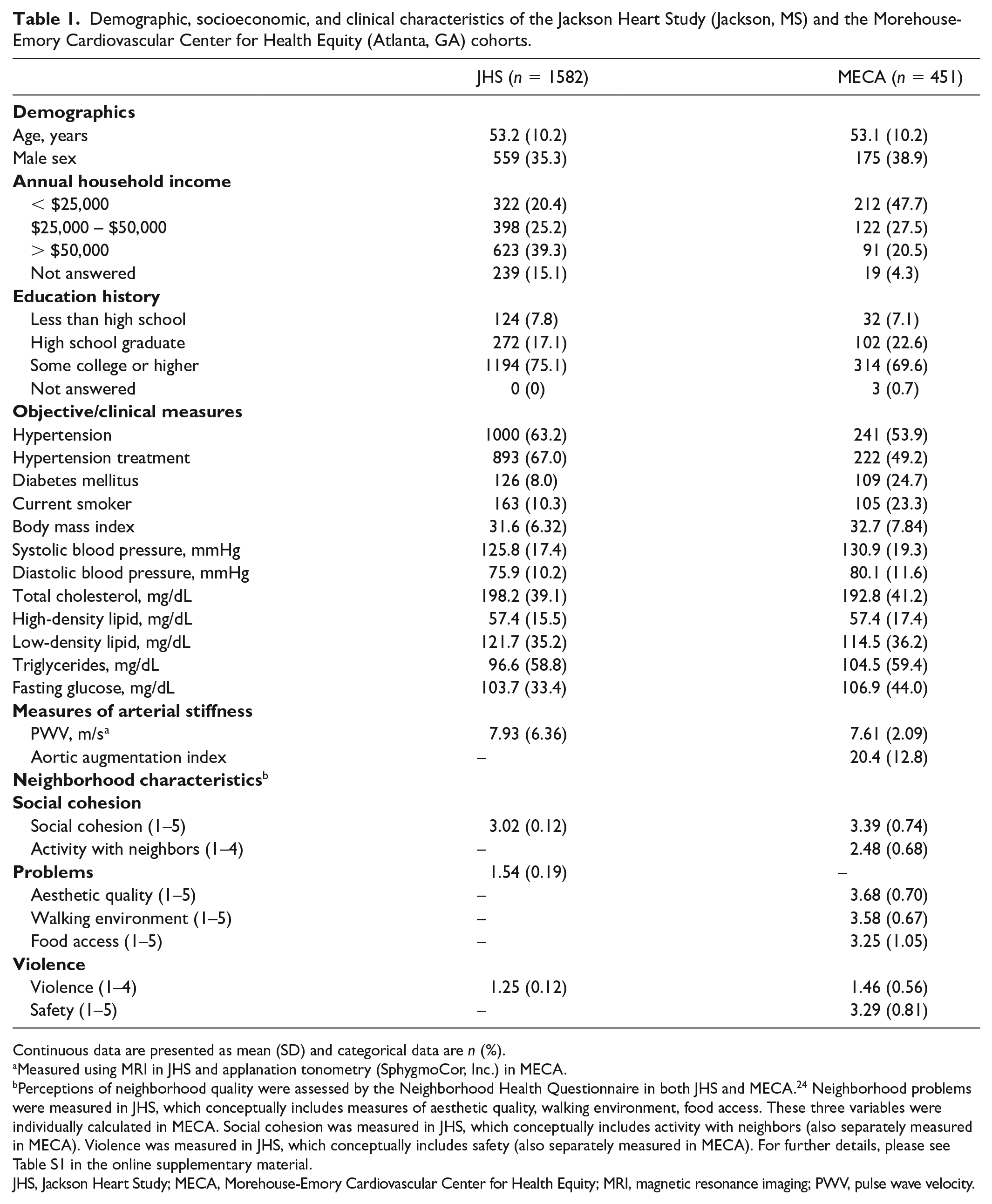
Continuous data are presented as mean (SD) and categorical data are n (%).
Measured using MRI in JHS and applanation tonometry (SphygmoCor, Inc.) in MECA.
Perceptions of neighborhood quality were assessed by the Neighborhood Health Questionnaire in both JHS and MECA. 24 Neighborhood problems were measured in JHS, which conceptually includes measures of aesthetic quality, walking environment, food access. These three variables were individually calculated in MECA. Social cohesion was measured in JHS, which conceptually includes activity with neighbors (also separately measured in MECA). Violence was measured in JHS, which conceptually includes safety (also separately measured in MECA). For further details, please see Table S1 in the online supplementary material.
JHS, Jackson Heart Study; MECA, Morehouse-Emory Cardiovascular Center for Health Equity; MRI, magnetic resonance imaging; PWV, pulse wave velocity.
In the JHS, those who reported living in neighborhoods with favorable characteristics (⩾ median) in terms of neighborhood problems (PWV = 7.46 ± 5.68 vs 8.55 ±7.11, p = 0.001) and violence (7.29 ± 5.54 vs 8.68 ±7.13, p < 0.001) had lower arterial stiffness (Table S3). Univariate predictors of arterial stiffness included age, hypertension, smoking, and neighborhood problems and violence (Table S4). In MECA, those who reported favorable activity with neighbors (AIx = 19.0 ± 13.4 vs 21.9 ± 11.9, p = 0.02) and walking environment (19.1 ± 11.8 vs 21.8 ± 13.5, p = 0.03) had lower augmentation index (Table S3, available online). In MECA, univariate predictors of arterial stiffness (as measured by AIx) included age, hypertension, and activity with neighbors (Table S4, available online).
In multivariable linear regression, favorable social characteristics, measured as social cohesion in JHS (β = −0.32 [−0.63, −0.02], p = 0.04) and activity with neighbors (β = −0.23 [−0.40, −0.05], p = 0.01) in MECA, were associated with lower PWV in both cohorts and social cohesion was associated with lower AIx (β = −1.74 [−2.92, −0.56], p = 0.004) in MECA, after adjustment for CVD risk factors and income (Tables 2 and 3, Figure 1). Additionally, in MECA, better food access (β = −1.18 [−2.35, −0.01], p = 0.05) was associated with lower AIx, and in JHS, lower neighborhood problems (β = −0.33 [−0.64, −0.02], p = 0.04) and lower violence (β = −0.30 [−0.61, 0.002], p = 0.05) were associated with lower PWV after adjustment for CVD risk factors and income. Results were similar when models were adjusted for heart rate, MAP, and hypertension treatment (Table S5, available online).
Multivariable analysis of neighborhood characteristics* and arterial stiffness measured as pulse wave velocity in the Jackson Heart Study cohort (Jackson, MS).
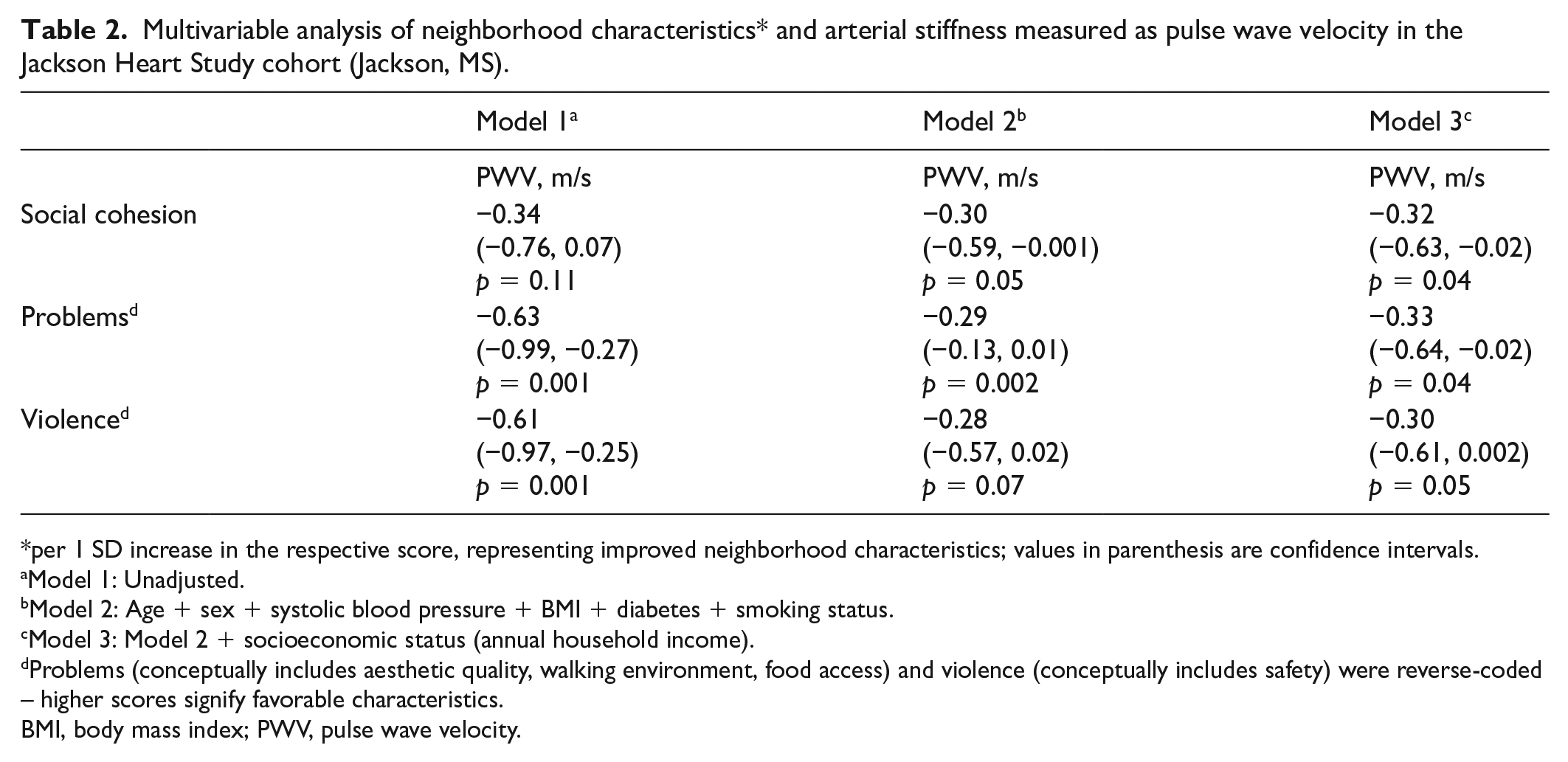
per 1 SD increase in the respective score, representing improved neighborhood characteristics; values in parenthesis are confidence intervals.
Model 1: Unadjusted.
Model 2: Age + sex + systolic blood pressure + BMI + diabetes + smoking status.
Model 3: Model 2 + socioeconomic status (annual household income).
Problems (conceptually includes aesthetic quality, walking environment, food access) and violence (conceptually includes safety) were reverse-coded – higher scores signify favorable characteristics.
BMI, body mass index; PWV, pulse wave velocity.
Multivariable analysis of neighborhood characteristics* and arterial stiffness measured as average pulse wave velocity and aortic augmentation index in the MECA cohort (Atlanta, GA).
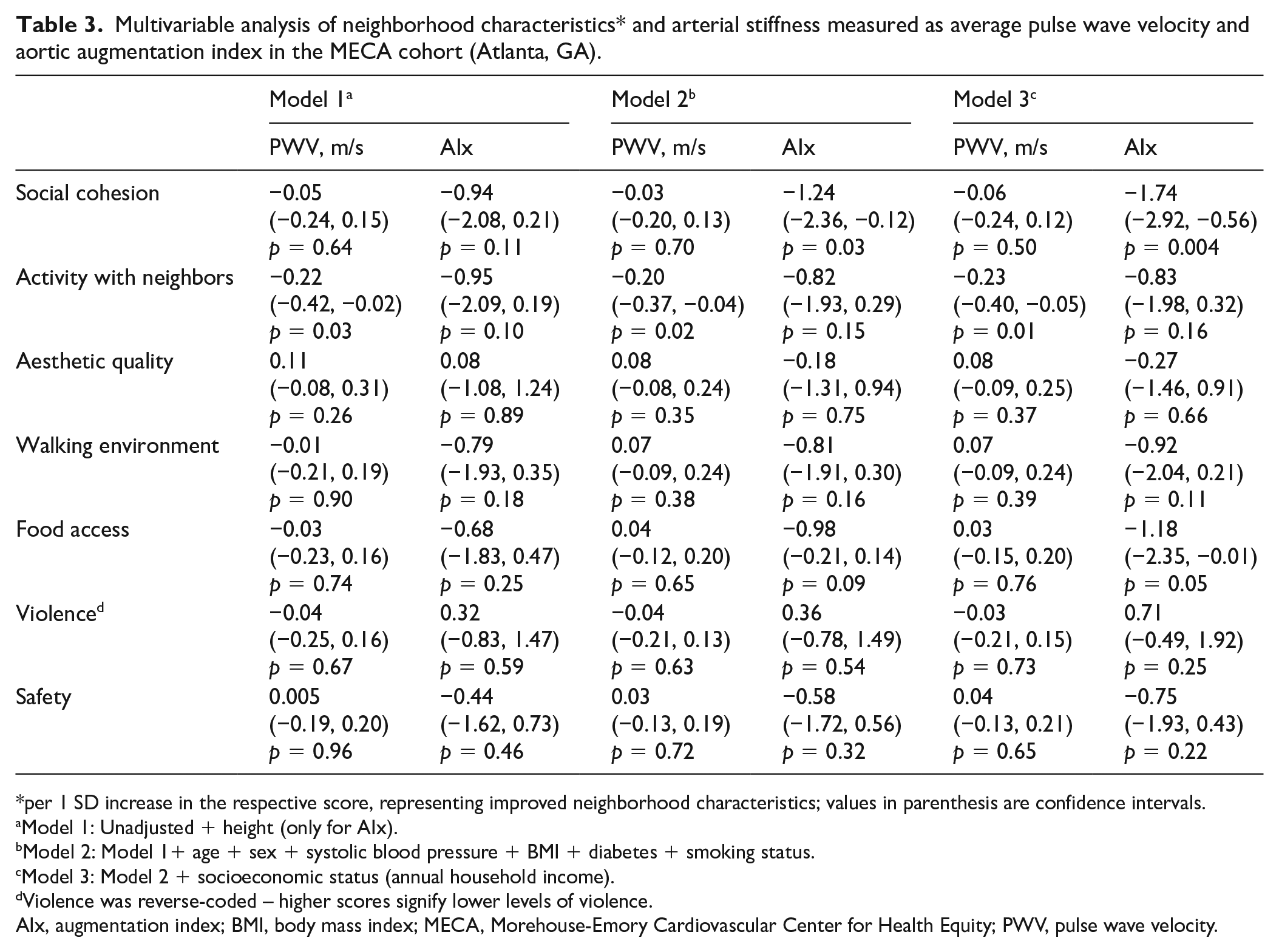
per 1 SD increase in the respective score, representing improved neighborhood characteristics; values in parenthesis are confidence intervals.
Model 1: Unadjusted + height (only for AIx).
Model 2: Model 1+ age + sex + systolic blood pressure + BMI + diabetes + smoking status.
Model 3: Model 2 + socioeconomic status (annual household income).
Violence was reverse-coded – higher scores signify lower levels of violence.
AIx, augmentation index; BMI, body mass index; MECA, Morehouse-Emory Cardiovascular Center for Health Equity; PWV, pulse wave velocity.
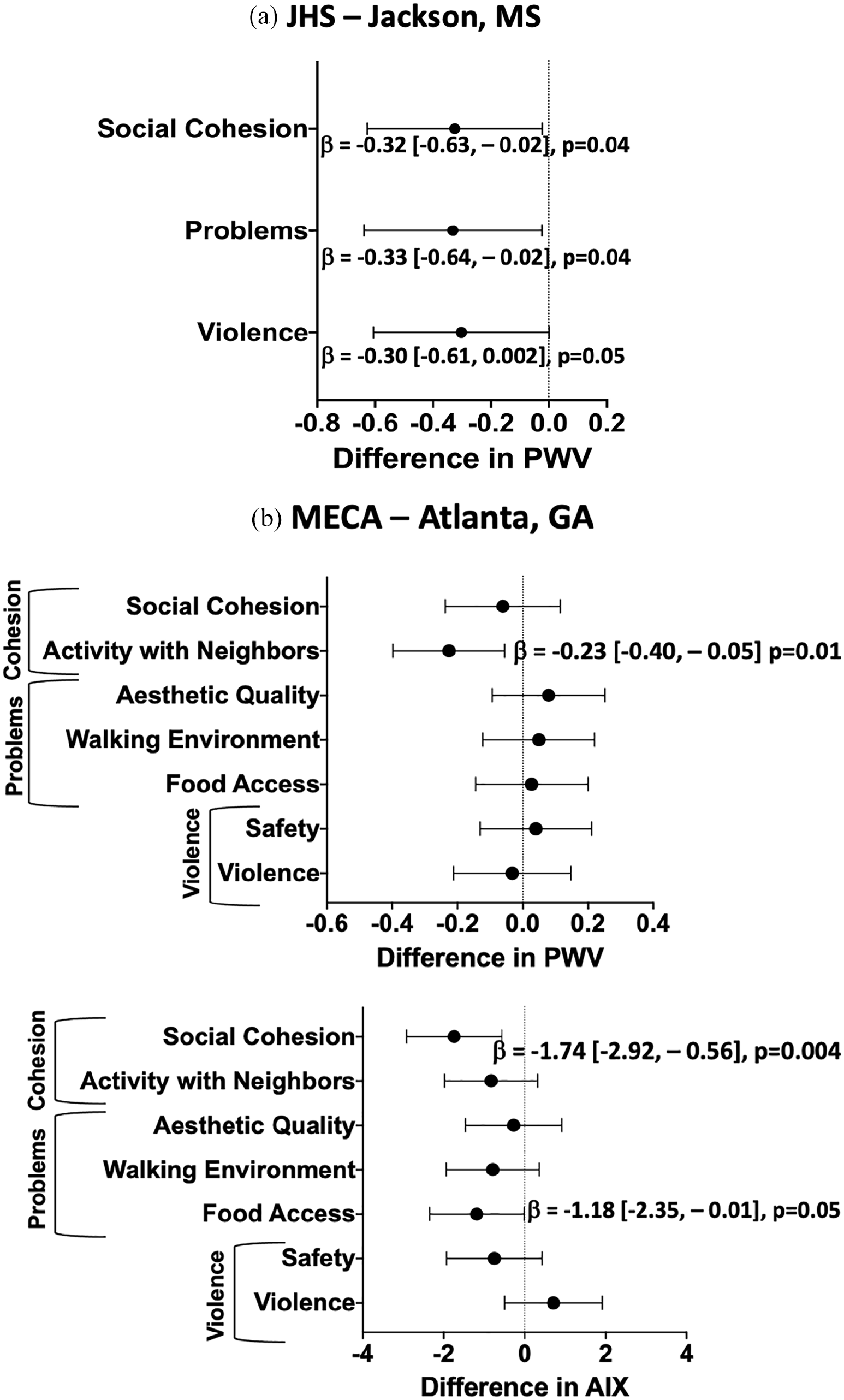
Association between components of neighborhood characteristics* and arterial stiffness. (
Discussion
We have demonstrated that desirable neighborhood social characteristics including social cohesion and activity with neighbors were associated with lower arterial stiffness among Black adults living in two distinct Southern US cities. We noted that these associations were independent of age, sex, blood pressure, BMI, diabetes, and individual-level socioeconomic status. Additionally, we demonstrated that lower neighborhood problems and violence were associated with lower arterial stiffness in JHS and improved food access was associated with lower arterial stiffness in MECA.
To our knowledge, this is the first study to find an association between neighborhood social characteristics and arterial stiffness, a biological marker of subclinical CVD that is associated with future CVD events.9,12 Arterial stiffness, though normally associated with age and hypertension, can be a direct manifestation of early vascular aging and is actually higher among Black adults where hypertension and CVD is especially prevalent and, thus, represents an important early biological marker to study in order to reduce CVD disparities.13,16–18,20 Even in healthy cohorts without known CVD or risk factors, elevated arterial stiffness is associated with future CVD events.31,32 Since our findings are independent of age and hypertension, we are demonstrating that healthy Black Americans living in neighborhoods with poor social characteristics have evidence of early vascular aging, which may be a precursor to the higher prevalence of hypertension and higher risk of future CVD events in Black individuals. We have previously shown in the MECA population that poor neighborhood social characteristics are associated with a greater burden of CVD risk factors among Black adults, 11 and now demonstrate that poor neighborhood characteristics are associated with worse vascular function, even after accounting for these risk factors. The factors mediating these associations require further investigation, and may include psychosocial factors such as stress or discrimination. Nonetheless, our findings have important ramifications as improving neighborhood social characteristics could represent a tangible entry point for public health officials to improve CVH and reduce health disparities among Black adults.
One of the novelties of our study is the reproducibility of our findings regarding the impact of neighborhood social cohesion among Black adults in two Southern US cities. Although prior studies have demonstrated the association between improved neighborhood social characteristics and cardiovascular risk factors in multiethnic populations,33–35 few studies have examined these associations in Black adults, and when examined have been single site with mixed findings.36–38 In a study of older adults aged 65 or greater in Chicago, IL, associations between social cohesion (conceptualized as social interactions with neighbors) and stroke mortality were found in White but not Black adults. 39 Prior findings from the JHS have demonstrated that higher social cohesion was associated with lower incidence of Type 2 diabetes among men and women 38 and, in a separate analysis, low social cohesion was associated with increased cumulative biological risk which encompasses multiple physiological (including the cardiovascular) systems among men only. 37 Although low social cohesion was shown to be not associated with incident CVD in the JHS during an approximately 10-year follow-up time period, 5 we demonstrate here that subclinical vascular disease, measured as arterial stiffness, was independently influenced by low social cohesion in this cohort. Similarly, Black individuals who live in neighborhoods with low social cohesion in Atlanta, GA also have evidence of early vascular aging. Replicating these findings in two distinct cities highlights the importance of neighborhood social cohesion in regard to CVH in Black adults.
Findings for other neighborhood characteristics have been mixed, however, across the two geographic locales. In the JHS, both lower neighborhood violence and problems (encompassing aesthetic quality, walking environment, and food access) were associated with lower arterial stiffness. In MECA, neighborhood violence was not associated with arterial stiffness, which highlights the fact that the neighborhood impacts on CV disease risk factors and disease may vary by geographic locales within the US since they arguably represent very different contexts for Black Americans in terms of segregation, historical policies, and opportunity structures. Jackson, MS (514 per 100,000 residents) also has a lower rate of violent crime compared to Atlanta, GA (936 per 100,000 residents), which could also factor into our findings. 40 Better food access was associated with lower arterial stiffness in MECA, similar to findings in the Multi-Ethnic Study of Atherosclerosis (MESA) where better food access was associated with lower CVD risk factors. 41 Similarly, fewer neighborhood problems (which encompass food access) were associated with lower arterial stiffness in the JHS, but whether food access was driving this association remains undetermined. Of note, in Jackson, MS there is a larger percentage of the population with low access to food stores compared to Atlanta, GA (26.4% vs 23.5% 42 ) and, as such, future studies should examine these associations further.
Study limitations and strengths
There are several limitations that must be considered. Data on neighborhood characteristics are self-reported and to compare findings across JHS and MECA, we conceptually grouped domains of neighborhood characteristics. However, both studies used the same validated questionnaire, thus improving our ability to compare findings across both geographic locales. 24 Similarly, arterial stiffness, which is a marker of early vascular aging, was measured using different, albeit well-validated methods. Although the gold standard for measuring arterial stiffness is carotid-femoral PWV (that can be measured using MRI as in JHS, or applanation tonometry as in MECA), increases in aortic augmentation index (AIx, which was also measured in MECA) have been associated with an increased risk of future heart failure43,44 and all-cause 15-year mortality 45 and, as such, can be used as a surrogate. In the JHS, the variability of the MRI-based PWV measurement is high and therefore also represents a limitation. Finally, our study is cross-sectional, which limits our ability to draw causal inferences. However, our study is one of the largest conducted assessing the association of neighborhood characteristics and arterial stiffness among Black adults, with a combined sample size of greater than 2000 participants. We are also one of the first to uniquely assess these associations in two distinct Southern US cities, strengthening the implications of our findings that improving neighborhood social cohesion can potentially decrease CVD-related health disparities among Black adults.
Conclusion
Neighborhood social characteristics show an independent association with the vascular health of Black adults, findings that were reproducible in two distinct American cities. Future research is needed into neighborhood-level implementation strategies to improve the social environment and reduce health disparities among Black adults.
Supplemental Material
sj-docx-1-vmj-10.1177_1358863X221136163 – Supplemental material for Neighborhood characteristics and arterial stiffness among Black adults – Results from the Jackson Heart Study and Morehouse-Emory Cardiovascular Center for Health Equity
Supplemental material, sj-docx-1-vmj-10.1177_1358863X221136163 for Neighborhood characteristics and arterial stiffness among Black adults – Results from the Jackson Heart Study and Morehouse-Emory Cardiovascular Center for Health Equity by Shabatun J Islam, Jeong Hwan Kim, Xiaona Li, Yi-An Ko, Peter Baltrus, Gary F Mitchell, Ervin R Fox, Mahasin S Mujahid, Viola Vaccarino, Tené T Lewis, Herman A Taylor, Mario Sims and Arshed A Quyyumi in Vascular Medicine
Footnotes
Acknowledgements
The authors thank the staff and participants of the JHS and MECA study.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The American Heart Association 0000031288, Abraham J. & Phyllis Katz Foundation, Byron Williams Jr, MD Fellowship Fund, and the National Institutes of Health (T32 HL130025 and T32 HL007745-26A1). The JHS is supported and conducted in collaboration with Jackson State University (HHSN268201800013I), Tougaloo College (HHSN268201800014I), Mississippi State Department of Health (HHSN268201800015I), and University of Mississippi Medical Center (HHSN268201800010I, HHSN268201800011I, and HHSN268201800012I) under contracts from the National Heart, Lung, and Blood Institute (NHLBI) and National Institute on Minority Health and Health Disparities (NIMHD).
Disclaimer
The views expressed in this manuscript are those of the authors and do not necessarily represent the views of the National Heart, Lung, and Blood Institute; the National Institutes of Health; or the U.S. Department of Health and Human Services.
Supplementary material
The supplementary material is available online with the article.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.