
Abstract
Sedentary behavior is associated with cardiovascular disease (CVD) and mortality, independent of physical activity. The biological mechanisms underlying these associations are largely unknown. We hypothesized that obese subjects with sedentary desk jobs, when assigned a sit–stand desk, will reduce daily sedentary time, and show improvement in arterial flow-mediated dilation (FMD), an early indicator of CVD. Overweight and obese subjects without known CVD were recruited at our institution and given an adjustable sit–stand desk at work. Activities were quantified with an accelerometer for 7 days at baseline and during the intervention. FMD of the brachial and superficial femoral arteries, fasting lipids, insulin and glucose labs, and anthropometrics were measured at baseline, and 12 and 24 weeks. Repeated one-way ANOVA tests were used to compare measurements over time. Fifteen participants were enrolled (93% female, mean age 40 ± 5 years, mean body mass index [BMI] 33 ± 5). Mean daily sedentary time at work decreased by 90 minutes from baseline (385 ± 49 minutes) to 12 weeks (297 ± 80 minutes, p = 0.002) and 24 weeks (295 ± 127 minutes, p = 0.015). Femoral FMD increased from baseline (4.9 ± 1.7%) to 12 weeks (6.4 ± 2.3%, p = 0.043) and further to 24 weeks (8.1 ± 3.2%, p = 0.009). Significant improvement in fasting triglycerides and insulin resistance occurred. There was no change in brachial FMD, exercise activity, step counts, weight, or BMI. A significant reduction in sedentary time during working hours was identified with utilization of a sit–stand desk and sustained over 24 weeks. Improvements in FMD, triglycerides, and insulin resistance provide insight into mechanisms of adverse health risks associated with sedentary behavior.
Introduction
Epidemiologic evidence suggests that long-term health consequences related to a lack of exercise activity are distinct from and additive to those of habitual sedentary behavior. Sedentary behavior is defined as behaviors that involve low levels of energy expenditure (1.0–1.5 METS) and include sitting, watching TV, reading, and driving.1,2 Over the past 50 years, sedentary jobs have increased 83% and currently account for 80% of all US jobs. 3 Sedentary behavior is now recognized as an independent risk factor for total all-cause mortality, cardiovascular disease and mortality, cancer-related mortality, metabolic syndrome, and type 2 diabetes (TDM).4–7 Owing to the high burden of sedentary behaviors in modern-day societies, workplace intervention and strategies to combat sedentary behaviors may be beneficial to employee health. According to the Centers for Disease Control and Prevention (CDC), lack of time or having a busy schedule is the most common reason that adults do not engage in physical activity. A standing desk requires no additional time commitment from employees, making it an attractive and relatively effortless behavioral intervention.
Vascular endothelial function, assessed by brachial artery flow-mediated dilation (BA-FMD), is a valuable indicator of vascular health and predictor of future cardiovascular events.8,9 BA-FMD also correlates with coronary endothelial function and is a useful tool in translational science.10,11 Improvements in BA-FMD are associated with reduced risk of cardiovascular events. Meta-analyses indicate a significant 8–13% lower risk of cardiovascular events per percent point increase in BA-FMD.12–15 While there are no studies correlating changes in superficial femoral artery FMD (SFA-FMD) to cardiovascular events, SFA-FMD is nitric oxide mediated like BA-FMD. Furthermore, focal training of the leg can improve local SFA-FMD while having less impact on BA-FMD. 16 A recent study showed that 3 hours of uninterrupted sitting reduced SFA-FMD, though brachial FMD was preserved. 17 However, it has not been determined whether a longer, sustained intervention to reduce daily sedentary behavior impacts cardiovascular health, including brachial and/or femoral FMD. Standing desks have gained popularity, but whether replacing sitting with standing is sufficient to effect meaningful and measurable health benefits remains unknown.
We hypothesized that overweight and obese subjects with sedentary jobs, when assigned use of a sit–stand desk, will reduce their daily sedentary time and demonstrate improvement in physiologic parameters and disease markers from baseline through the end of the 24-week intervention. The primary aim of our study was to assess the feasibility of workplace interventions to reduce daily sedentary time in obese, sedentary, office-based employees. Our secondary aim was to assess the impact of reducing sedentary time on FMD and other markers of cardiometabolic health with measurements at baseline and during the intervention.
Materials and methods
Subject recruitment and study design
Overweight and obese office workers at the Medical College of Wisconsin were recruited via flyers posted on institutional bulletins, in newsletters, and on the intranet. Institutional Review Board (IRB) approval was obtained (Medical College of Wisconsin). A brief overview of the study was provided over the phone, and initial eligibility was determined in the form of a short questionnaire, which contained inclusion and exclusion criteria. Sedentary office employees ages 18–50 years with a body mass index (BMI) of ⩾ 26 kg/m2 were included. ‘Sedentary’ was defined as spending greater than 75% of their (8 hours or longer) workday sitting at a desk. This included at least one period of 2 hours or longer of uninterrupted sitting time per workday and was assessed by self-report. Subjects were required to work standard office hours (08:00 to 17:00 ± 1 hour for start/end times) and asked to maintain current levels of exercise activity. Permission from the subjects’ supervisor was needed to participate in the intervention. Exclusion criteria included: known history of atherosclerotic cardiovascular disease (myocardial infarction, stroke, coronary stent, coronary artery bypass grafting, angina, and peripheral vascular disease), diabetes treated with insulin or other diabetes medications (pre-diabetes was acceptable, defined as a glycosylated hemoglobin (HbA1c) of 5.7–6.4% or fasting glucose of 100–125 mg/dL), hypertension (screening systolic blood pressure (SBP) ⩾ 150 mmHg or diastolic blood pressure ⩾ 90 mmHg or on treatment for hypertension), use of cholesterol-lowering medications or low density lipoprotein (LDL) cholesterol ⩾ 190 mg/dL, pregnancy, lactating or planning to get pregnant within the next 6 months, current tobacco use within the previous 12 months, current excessive alcohol use (more than 14 drinks/week for females, more than 28 drinks/week for males), current illicit drug use, known thyroid disease, current use of diet pills or supplements other than a multi-vitamin or supplements contained in a multi-vitamin, plans to diet in the next 6 months, musculoskeletal issues that would interfere with prolonged periods of standing, history of migraines, history of phosphodiesterase-5 inhibitor use within the last 5 days of the screening visit and inability to refrain from use of this medication for 5 days prior to each FMD study. If the subject satisfied the above-mentioned criteria, a screening visit was scheduled, during which written informed consent, baseline vital signs, height, weight, medical history and medication use, and screening (fasting) laboratory assessments were obtained. Additional study visits were scheduled for baseline, 12- and 24-week visits. These study visits included vascular function testing, accelerometer application (activPAL™; PAL Technologies, Glasgow, Scotland), laboratory testing, vital signs, height, weight, and waist and hip circumference. Medical history and medication and supplement use were updated at each study visit.
Standing desk intervention
This was an unblinded, nonrandomized study design where each subject served as his or her own control over a 6-month period. We used low-cost, non-electric, height-adjustable sit–stand desks that are delivered fully assembled (VariDesk®; Dallas, TX, USA). The desks fit dual monitors and little effort is required to move the desk up and down. A study team member installed the sit–stand workstation for enrolled subjects and provided instructions and demonstration on use. The workstation has a two-tier design with an upper deck area large enough to accommodate a dual-monitor setup and a lower deck for full-sized keyboard and mouse, adjustable to 11 height settings. Subjects were encouraged to keep the workstation in the standing position for most of the workday with the understanding that transitions to the sitting position, such as for lunch, fatigue, or joint aches, were acceptable. An anti-fatigue mat was provided to minimize back and leg discomfort. Enrolled participants did not receive any prompts or reminders to reduce sedentary behavior after the initial desk installation and training.
Physical activity monitoring
Accelerometry measurements were obtained for 7 consecutive days at baseline prior to introduction of the sit–stand desk, and again at 12 and 24 weeks, using a compact (35 mm × 53 mm × 7 mm, 15 g) and re-usable physical activity monitor that adheres to the subject’s anterior thigh with a nitrile sleeve and Tegaderm dressing and is easily concealable with any wardrobe. Subjects could shower with this dressing but were instructed to avoid baths or swimming (or remove the device for such activities). Standing and sitting times, sitting bouts (periods of at least 30 consecutive minutes of sitting), daily steps, cadence (walking speed), and exercise activity information were obtained from the monitor. Subjects were instructed to wear the accelerometer for a minimum of 14 hours per day and at least 6 out of 7 days. Subjects were asked to maintain their current levels of exercise activity and to refrain from dieting for the duration of the study. Accelerometer data were processed using (1) the accelerometer software application outputs and (2) a validated, custom R package (R Foundation for Statistical Computing, Vienna, Austria) that has been previously described. 18
Anthropometrics
BMI was calculated as weight in kilograms divided by height in meters squared. Waist circumference was measured 1 cm above the iliac crest, hip circumference at the widest circumference of the buttocks at the area of the greater trochanters, and waist-to-hip ratio (WHR) is the ratio of the two.
Bioimpedance measurements were obtained with the Omron HBF-514C Full Body Sensor Body Composition Monitor and Scale (Omron Healthcare, Lake Forest, IL, USA). These measurements included resting metabolism and percentages of body fat, visceral fat, and skeletal muscle.
Flow-mediated and nitroglycerin-mediated dilation
Vascular function assessments were performed at baseline, and 12- and 24-week visits. Premenopausal female subjects were instructed to schedule these visits during days 1–7 (menstruation) of their menstrual cycles to minimize the potential effects of sex-specific hormone fluctuations on vascular function. 19 The protocol has been previously described. 20 In brief, subjects were asked to fast for at least 12 hours prior to study visits. The brachial and superficial femoral arteries were imaged using a high-resolution 7.5–13 MHz probe at baseline and following a 5-minute occlusion of flow in the artery with a blood pressure cuff on the lower arm or lower leg inflated to supra-SBPs at least 50 mmHg above resting SBP or > 200 mmHg. On rapid deflation of the cuff, transient hyperemia stimulates nitric oxide production and release from the endothelium, resulting in dilation. To determine if there is endothelium-independent vasodilation, subjects were given 0.4 mg of sublingual nitroglycerin after a minimum of 10 minutes from the flow-mediated (endothelium-dependent) dilation assessment. Nitroglycerin-mediated vasodilation reflects vascular smooth muscle function and, when stable, serves to validate that any observed changes in BA-FMD truly reflect endothelial function. Subjects with a SBP less than 100 mmHg, history of migraine headaches or history of adverse reactions to nitroglycerin were not given nitroglycerin. Ultrasound images of the artery were obtained at baseline and for 10-second windows around the 1-, 2- and 3-minute marks following cuff deflation and again at 3 minutes after sublingual nitroglycerin administration. Images were digitized and stored. Blinded analysis was performed with commercially available software (Brachial Analyzer 6.10.2; Medical Imaging Applications, Coralville, IA, USA). A minimum of 20 minutes of rest was required between brachial and superficial femoral artery vascular function assessments. The percent increase in blood flow during hyperemia was expressed as the percent increase in flow from baseline.
Because there is a high degree of technical skill related to assessing FMD, we routinely assess the reproducibility of these measurements in our lab. The intraclass correlation coefficient (ICC) averaged for all four of our technicians is 0.97 with a 95% CI of 0.92–0.99 (p < 0.001), which compares the reproducibility of the four technicians for a given BA segment to be measured (n = 10 studies, each one blindly analyzed by four technicians). With regards to measuring the same study on 2 different days by the same technician, the ICC is 0.97 for a single measure; CI: 0.85–0.99, p < 0.001 (n = 8).
Biochemical analysis
Serum total cholesterol, high density lipoprotein (HDL) cholesterol, triglycerides, non-HDL cholesterol, glucose, insulin, HbA1c, and C-reactive protein (CRP) were measured by an automated analyzer in the Wisconsin Diagnostic Laboratory of the Medical College of Wisconsin. LDL cholesterol was calculated with the Friedewald formula. 21 Urine pregnancy testing was performed the morning of the baseline, 12-, and 24-week visits. The homeostatic model assessment of insulin resistance (HOMA-IR) was calculated as the product of insulin and glucose divided by 405. 22
Statistical analysis
Initial power analysis yielded 22 subjects to achieve 80% power (two-sided α = 0.05) with a reduction in sedentary time of 60 minutes/day (primary outcome) and SD of 100 minutes. However, enrollment ended prematurely secondary to lack of funding. Because we saw a larger effect size of 90 minutes/day (reduction in sedentary time), our statistician re-evaluated the power analysis to find that we remained 90% powered with 15 subjects and a two-sided α = 0.05 for significance.
All variables of interest were compared at baseline, 12, and 24 weeks for all subjects using repeated one-way analysis of variance (ANOVA). The exposure variable was derived from the sit–stand desk intervention (or control) and included objective measures of sedentary time, including mean daily sedentary time (Monday – Friday, 08:00 to 17:00), mean 24-hour sedentary time (Monday – Sunday – to account for behavioral changes outside of the workplace), and mean number of sedentary bouts > 30 minutes (Monday – Friday, 08:00 to 17:00). Standing time was assessed in a similar manner – and correlated (Spearman’s correlation) with changes in sitting time during work hours to ensure our intervention was utilized as expected. We also tested for differences in mean daily steps at work, mean daily steps over the entire week/weekend, and moderate-to-vigorous intensity physical activity (MVPA). We used Spearman’s correlation to analyze the relationship between sedentary time, sedentary bouts (defined as ⩾ 30 minutes of continuous sitting), and outcome variables. Acceptability of the sit–stand workstation intervention was assessed via questionnaire consisting of a 19-item five-point Likert scale (1: strongly disagree, 2: disagree, 3:neutral, 4: agree, 5: strongly agree) adapted from a previous trial. 5
Results
Subject characteristics are displayed in Table 1. Of 138 subjects screened, 18 subjects were consented. One subject was a screen failure (no history of hypertension but was hypertensive at the screening visit) and two subjects with baseline data were excluded from the final data analyses due to lack of follow-up visits (one subject changed employers and one subject had scheduling conflicts). Therefore, 15 subjects were analyzed with baseline and 12-week visits; 14 subjects had 24-week data (one subject became pregnant prior to the 24-week visit, which was a protocol violation). Subjects were predominantly female with mean age of 40 ± 5 years and mean BMI of 33 ± 5 kg/m2. Most subjects were employed as administrative assistants, research/project coordinators, or project managers at our institution. Twenty percent were African American with the remainder Caucasian. Prior to the intervention, the mean daily sedentary time (Monday – Friday from 08:00 to 17:00) at baseline was 385 ± 49 minutes.
Baseline characteristics.

Means ± SD for continuous variables.
BMI, body mass index.
Physical activity monitoring
Mean sedentary time, standing time, and stepping time at work Monday – Friday from 08:00 to 17:00 at baseline, 12, and 24 weeks are detailed in Table 2. Subjects demonstrated excellent compliance with accelerometer use (6 ± 1 days of use out of 7) across all three assessments. There was a sustained decrease in mean daily sedentary time at work of approximately 90 minutes at 12 weeks (297 ± 80 minutes, p = 0.002) and 24 weeks (295 ± 127 minutes, p = 0.015) compared to baseline (385 ± 49 minutes). There were no differences in sedentary time outside of work Monday – Friday (730 ± 116 vs 706 ± 99 vs 679 ± 129 minutes, p = 0.49) or on the weekend (730 ± 96 vs 718 ± 74 vs 701 ± 123 minutes, p = 0.73) from baseline to 12 and 24 weeks. The decrease in workday sedentary time was inversely related to an increase in standing time (r = −0.780, p = 0.008), Table 2. There was no change in MVPA step counts from baseline (3808 ± 1315) to 12 and 24 weeks (3859 ± 1075, p = 0.0857 and 4235 ± 1653, p = 0.246, respectively) or in mean daily MVPA minutes, Table 2. There was no change in mean daily steps over 24 weeks.
Accelerometer data.

Means ± SD for continuous variables.
p < 0.05 from baseline to 12 weeks.
p < 0.05 from baseline to 24 weeks.
MVPA, moderate-to-vigorous physical activity, defined as ⩾ 3 METS or ⩾ 100 steps/min.
The accelerometer categorizes number of daily sedentary bouts into three groups: < 30 minutes, 30–60 minutes, and > 60 minutes. There were trends towards a reduction in all categories of sedentary bouts with the only statistically significant change being the number of 30–60-minute bouts from baseline to 24 weeks (5.2 ± 1.8 to 3.7 ± 1.4, p = 0.029); Table 2. Similarly, there was a trend towards a reduction in the number of up and down transitions (Table 2).
Vascular outcomes
BA-FMD did not change from baseline to 24 weeks with the standing desk intervention (8.8 ± 3.4% to 8.9 ± 3.1%, p = 0.542). However, SFA-FMD increased from baseline (4.9 ± 1.7%) to 12 weeks (6.4 ± 2.3%, p = 0.043) and continued to increase by 24 weeks (8.1 ± 3.2%, p = 0.009 compared to baseline); Figure 1. There was no change in nitroglycerin-mediated (endothelium-independent) BA-FMD from baseline (28.0 ± 6.0%) to 12 weeks (28.6 ± 5.9%, p = 0.838) and 24 weeks (24.1 ± 2.9%, p = 0.155).
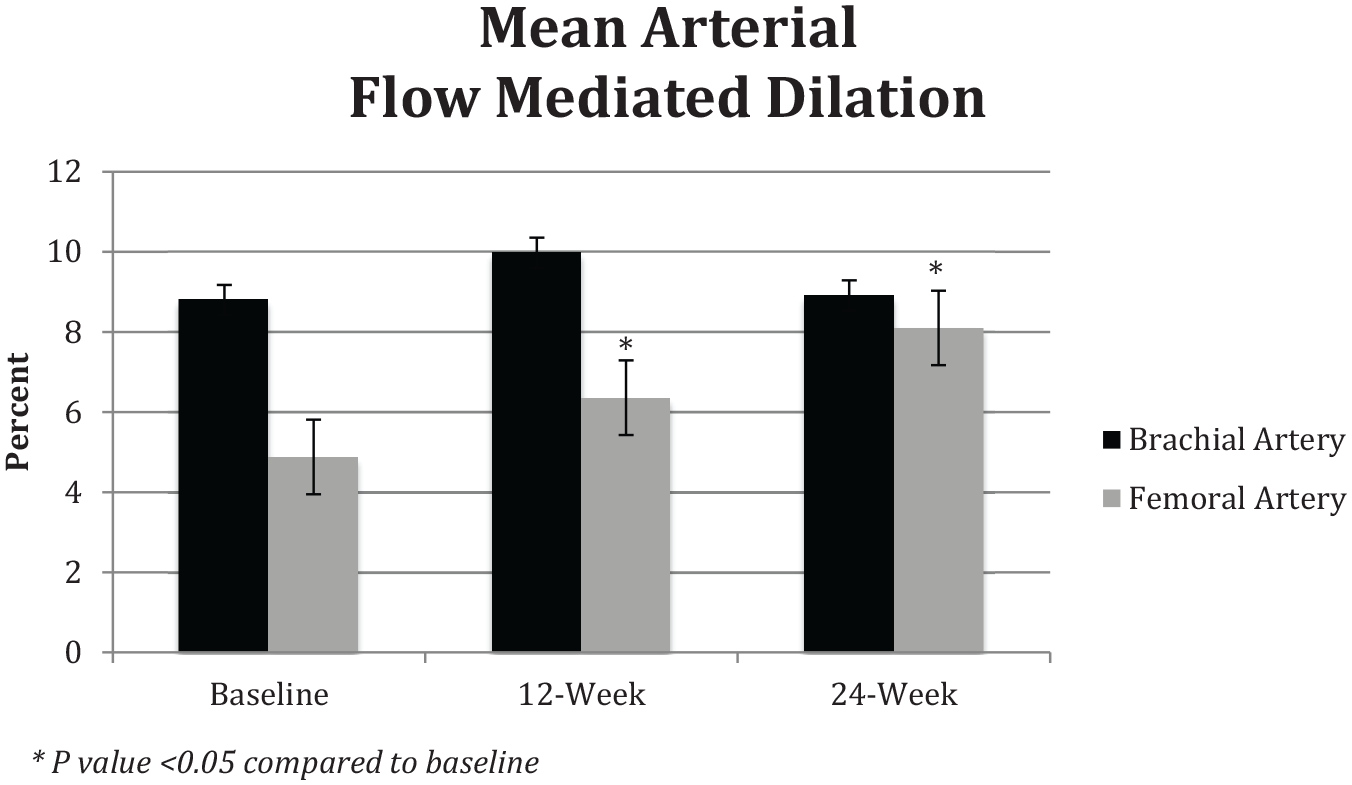
Changes in vascular flow-mediated dilation of the brachial and superficial femoral arteries over 24 weeks.
There was no change in pre-FMD femoral artery diameters across the three study visits (5.34 ± 0.52, 5.51 ± 0.57, 5.46 ± 0.58; p = 0.709). There was no change in pre-FMD brachial artery diameters across the three study visits (3.45 ± 0.46, 3.36 ± 0.35, 3.49 ± 0.27; p = 0.63).
Biochemical measures
A strong trend towards a reduction in total cholesterol was observed from baseline (191 ± 40 mg/dL) to 24 weeks (183 ± 36 mg/dL, p = 0.050). There was a significant 17% reduction in fasting triglycerides from baseline (124 ± 55 mg/dL) to 12 and 24 weeks (103 ± 39 mg/dL, p = 0.029 and 102 ± 49 mg/dL, p = 0.018, respectively). There was no change in LDL or HDL cholesterol levels. HOMA-IR improved from baseline (3.61 ± 1.88) to 24 weeks (2.77 ± 1.35, p = 0.022). Improvements in HOMA-IR were driven by a reduction in fasting insulin levels, which decreased from baseline 16.4 ± 7.1 µIU/mL to 12.4 ± 5.2 µIU/mL by 24 weeks (p = 0.004), while there was no change in fasting glucose levels or glycosylated hemoglobin over the course of the 24-week intervention (Table 3). There were significant correlations between a reduction in sedentary bouts (period of continuous sitting ⩾ 30 minutes) and improvement in glycosylated hemoglobin (ρ = 0.60, p = 0.02) and between a reduction in sedentary bouts and fasting triglycerides (ρ = 0.69, p = 0.006). There was no correlation between sedentary bouts and fasting insulin levels, HOMA-IR, and fasting glucose levels (data not shown). There were no changes in CRP over 24 weeks of intervention.
Laboratory data.

Means ± SD for continuous variables.
p < 0.05 from baseline to 12 weeks.
p < 0.05 from baseline to 24 weeks.
CRP, C-reactive protein; HbA1c, glycosylated hemoglobin; HDL, high density lipoprotein; HOMA-IR, homeostatic model assessment – insulin resistance; LDL, low density lipoprotein.
Other measures
There were no changes in resting heart rate, blood pressure (systolic or diastolic), weight, BMI, waist circumference, hip circumference, WHR, or bioimpedance measures of body composition. A likeability survey administered at completion of the 6-month study showed that subjects found the intervention was easy to operate, improved productivity, and improved muscle/joint and back pain (Figure 2).
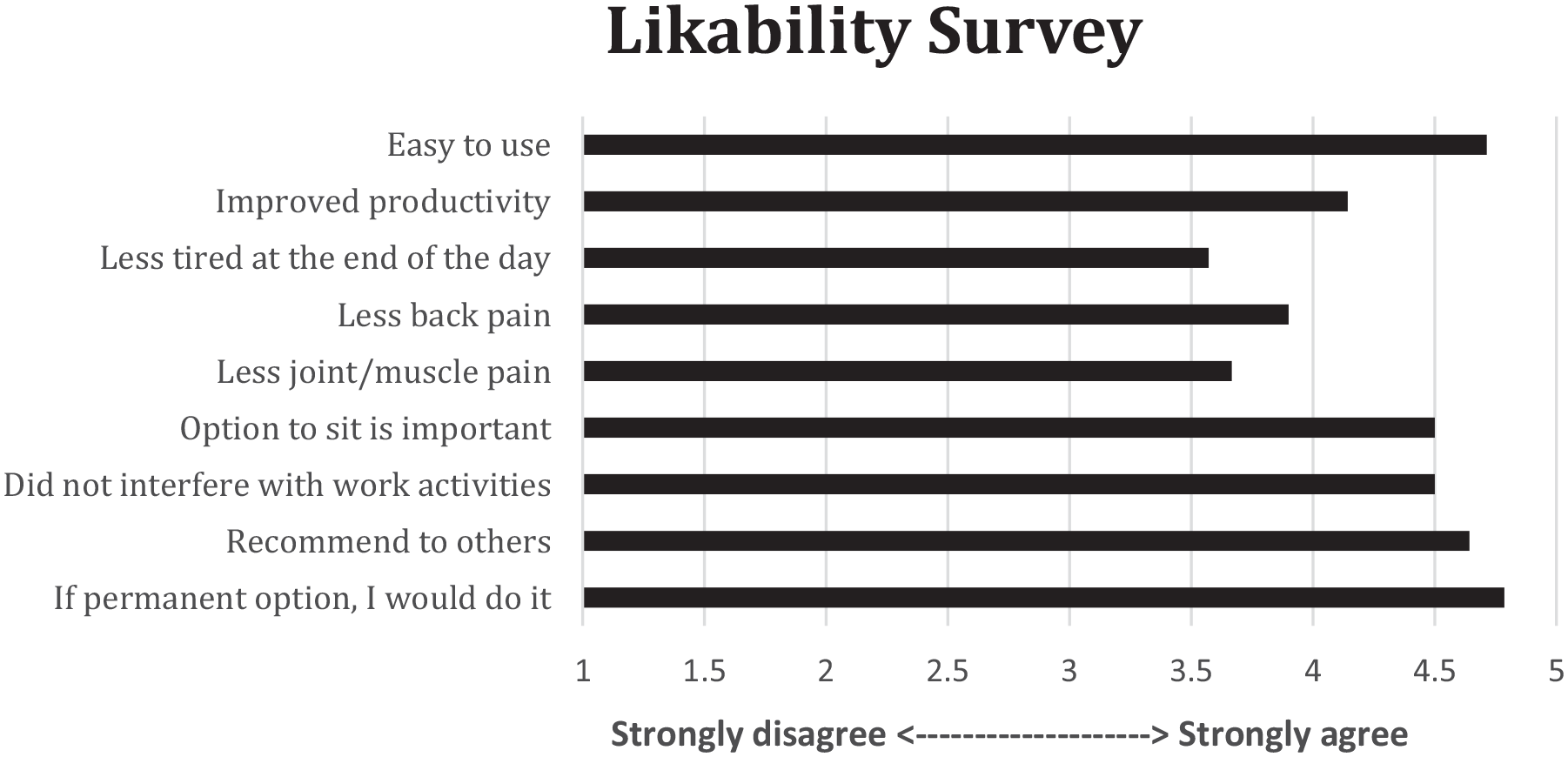
Acceptability of the sit–stand workstation intervention was assessed via questionnaire consisting of a 19-item five-point Likert scale adapted from a previous trial 5 under terms of Creative Commons Attribution 4.0 International License (http://creativecommons.org/licenses/by/4.0/).
Discussion
To our knowledge, this is the first sustained intervention to show improvement in lower extremity vascular function as assessed by SFA-FMD with a sit–stand desk intervention implemented in the workplace setting. Our results go beyond previous reports and demonstrate that a prolonged and easy-to-implement intervention to replace approximately 90 minutes of sitting with standing resulted in improvements in several important disease biomarkers, including vascular endothelial function, insulin resistance, and triglyceride levels, in healthy overweight and obese office-based employees. There were no changes in exercise activity, step counts, weight, or waist circumference.
Efforts to increase physical activity in the population have largely focused on increasing MVPA, with little attention given to reducing sedentary behaviors. The preventative role of MVPA in the development of chronic disease is irrefutable. 23 In the largest isotemporal (physical activity) study to date involving over 150,000 individuals and 20,000 deaths, Matthews and colleagues reported a mortality benefit for replacing sitting with 1 hour/day of light-intensity (or non-exercise) activity. 24 Another study showed a 5% reduction in all-cause mortality risk when replacing 1 hour of sitting with standing. 25 The major limitations of these studies and substitution methodologies are that most are cross-sectional and cannot estimate the actual impact of changing behavior on health. They do, however, provide useful insight into the potential benefits of reducing sedentary time. Furthermore, consistent use of the standing workstation was sustained through 6 months. Diet and exercise regimens are not this well-maintained. 26 Our pilot study now provides prospective, clinical trial evidence to support the notion that standing is indeed better than sitting and has the potential to translate into important population health benefits if implemented on a larger scale.
The results of the present study show that long-term reduction in sedentary time, by as little as 90 minutes/day, improves macrovascular endothelial dilator function in the lower extremities. Previous work has elucidated the importance of hemodynamic forces in structural and functional changes in vascular health.27,28 Restaino et al. found that 3–4 hours of sitting reduced blood flow and shear rate in lower limb conduit arteries correlating with a decline in lower limb artery endothelial function. 29 Although the underlying mechanisms are not fully understood, prior work suggests prolonged gravitational forces leading to increased hydrostatic pressure, increased muscle sympathetic nerve activity, and increased turbulent flow (due to changes in angles of major arteries while sitting) may be contributing to the connection between prolonged sedentary time and vascular disease.28–30 Our findings are important because interventions that improve endothelial function in the lower limbs would be expected to prevent or even improve peripheral vascular disease. There was no change in BA-FMD. It is possible that BA-FMD may not be a sensitive measure of endothelial function when primarily studying changes in sedentary behavior. Our findings are likely related to increased muscle fiber activation in the lower limbs with standing. In fact, Thijssen et al. demonstrated that BA-FMD responses differ by type and intensity of lower limb exercise. 31 Our results substantiate benefits to vascular health outside of moderate or vigorous-intensity exercise with important implications for future research in sedentary behavior.
In addition to the effects on vascular health, sedentary behavior has also been associated with increased risk of metabolic syndrome and TDM. 32 We saw a significant 23% improvement in insulin resistance at 6 months with the standing desk intervention, driven primarily by reductions in fasting insulin levels. A large meta-analysis of 18 studies totaling 794,577 subjects concluded that sedentary behavior mediates TDM, independent of exercise activity and BMI. 33 However, these prior data are limited by the cross-sectional design and high reliance on self-reported activity. Our findings show causality between a reduction in sedentary time and improved insulin resistance. Although we excluded individuals with diabetes in our study, most were found to have some insulin resistance related to elevated BMI, despite normal fasting glucose and glycosylated hemoglobin levels. Improvements in insulin resistance in our subjects were most substantial in those who decreased sitting by over 90 minutes/day, though we are underpowered to examine a dose–response relationship. Future randomized control trials will be important to corroborate these findings and determine if a dose–response relationship exists, as this would inform public health guidelines on limits for sedentary behaviors.
Even though we did not see a significant correlation between changes in daily sedentary time and fasting glucose or HbA1c, we did see a statistically significant and moderate-sized correlation between a reduction in sedentary bouts (at least 30 minutes of consecutive sitting) and lower HbA1c (ρ = 0.60, p = 0.023). This may be a chance finding though other cross-sectional studies have noted a positive relationship between breaks in sedentary behavior and cardiometabolic health.34–37 In a large, cross-sectional analysis from the Hispanic Community Health Study/Study of Latinos (HCHS/SOL), authors concluded that accruing sedentary time in prolonged, uninterrupted bouts may be deleteriously associated with biomarkers of glucose regulation. 37 An experimental study in obese children showed that interrupted sitting (3 minutes of moderate intensity walking every 30 minutes) compared to 3 hours of continuous sitting improved glucose metabolism. 38 Our study extends this concept of sedentary breaks, but simply by replacing sitting with standing. We saw a significant reduction in the number of 30–60-minute bouts from baseline to 24 weeks with trends towards reductions in sedentary bouts of all durations. Findings are similar to those of a randomized control trial of a standing desk intervention which successfully reduced total occupational sitting time without a significant change in bouts. 39 Perhaps breaking up the sedentary time is also needed to maximize cardiometabolic benefits, and this should be evaluated in future studies.
A sit–stand workstation was chosen for our intervention due to evidence from previous studies that demonstrated sit–stand desks to have high acceptability and usability in addition to success at reducing sedentary time at work. 40 A large systematic review of 33 studies totaling 25,446 subjects concluded that interventions focusing solely on reducing sedentary behavior appear to be more effective at reducing sedentary time than those that include strategies for both increasing physical activity and reducing sedentary behaviors. However, this finding was limited by the quality of the studies, classified as very low and moderate. 41 Project STAND was a randomized control trial to reduce sedentary time in young adults at risk for diabetes mellitus using a structured educational intervention program with a workshop, phone calls, and a self-monitoring tool. This intervention failed to show a significant reduction in sedentary behavior after 12 months, based on accelerometer-assessed sedentary time. 42 The investigators attribute the null findings to a lack of focus on modifying the environment. Leveraging the sedentary workplace environment, where we spend most of our waking hours, to reduce sedentary behaviors by implementing a sit–stand desk is feasible and requires no additional time commitment from the employees, making it an attractive and relatively effortless behavioral intervention. Furthermore, qualitative results from our likeability survey suggest sit–stand workstations are a feasible long-term intervention to reduce sedentary time, improve musculoskeletal discomfort, and increase productivity. These findings are consistent with other studies that sit–stand interventions have minimal to no deleterious effects on the musculoskeletal system.5,43,44
Strengths and limitations
Strengths of the present prospective study include long-term follow-up, use of a focused and easily accessible intervention, and objective quantitative activity data collection with the use of sophisticated accelerometers to distinguish sitting from standing behaviors. The intervention is really the ‘option to stand’ rather than sit during the workday. This is a strength because it heightens acceptability and even ‘the option of standing’ showed benefit. It is a limitation in that it does not allow for a dose–response analysis (even if more subjects enrolled) at higher levels of standing. There are additional limitations in this study that could be addressed in future research. First, the subjects were predominantly female, healthy obese, with minimal age variation. This likely reflects an inclusion bias and may limit generalizability of the findings to men and other age groups. Enrolled subjects likely had normal visceral fat (less than 10% with WHR < 1 and mean triglycerides around 124 mg/dL; Tables 1 and 3), so it would be important for future studies to include participants with more risk factors to determine if results are even more robust. This is pilot data, and the number of subjects was limited due to lack of funding. We did not assess dietary intake or habits of subjects, though we did request that they refrain from dieting during the trial period. However, the lack of significant changes in weight or BMI suggest individuals did not make large changes in diet that might have influenced the results. We were underpowered to examine dose–response relationships. Despite these limitations, this study contributes important findings to the evolving understanding of the impact of accelerometer-measured sedentary behavior on vascular health and clinical outcomes.45,46
Conclusions
Long-term use of a sit–stand workstation reduced daily sedentary time and led to improvements in lower extremity vascular function and markers of cardiometabolic health. The predominance of occupational sedentary activities affords high impact and clinically important targets for intervention strategies to change lifestyle behaviors. With more people working remotely from home during the COVID-19 pandemic, reducing sedentary behavior may be more important now than ever. 47 Our study underscores benefit to vascular health outside of exercise activities by simply replacing sitting with standing, and this will help to inform future prospective studies on a broader scale. Furthermore, the acceptability of sit–stand desks at home 48 and increased employee productivity, 49 combined with the potential health benefits, should more than offset the initial expense of purchasing the desk for employees, whether working from home or in the office.
Footnotes
Correction (December 2022):
Article updated to correct the x-axis title in Figure 2 to say “Strongly disagree” on the left and “Strongly agree” on the right
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
This study is funded in part by the Research and Education Program Fund, a component of the Advancing a Healthier Wisconsin endowment at the Medical College of Wisconsin. This award is supported by grant numbers UL1TR001436 and KL2TR001438 from the Clinical and Translational Science Award (CTSA) program of the National Center for Research Resources and the National Center for Advancing Translational Sciences. The content of this article is solely the responsibility of the authors and do not necessarily represent the official views of the NIH. Additional support provided by the Michael H Keelan Jr Research Foundation grant and the Sally Bentley Endowment.