
Abstract
Cardiovascular disease (CVD) has emerged as a leading cause of non-HIV-related mortality among people living with HIV (PLWH). Despite the growing CVD burden in PLWH, there is concern that general population risk score models may underestimate CVD risk in these patients. Imaging modalities have received mounting attention lately to better understand the pathophysiology of subclinical CVD and provide improved risk assessment in this population. To date, traditional and well-established techniques such as echocardiography, pulse wave velocity, and carotid intima thickness continue to be the basis for the diagnosis and subsequent monitoring of vascular atherosclerosis and heart failure. Furthermore, novel imaging tools such as cardiac computed tomography (CT) and cardiac CT angiography (CCTA), positron emission tomography/CT (PET/CT), and cardiac magnetic resonance (CMR) have provided new insights into accelerated cardiovascular abnormalities in PLWH and are currently evaluated with regards to their potential to improve risk stratification.
Keywords
Introduction
Human immunodeficiency virus (HIV) infection continues to be a major global public health issue with the number of people living with HIV (PLWH) increasing steadily. In 2018, the total number of infected people was 37.9 million, with nearly 70% of them residing in sub-Saharan Africa. 1 The early diagnosis and widespread uptake of antiretroviral treatment (ART) has shifted HIV infection from a progressively fatal condition to a chronic disease. 2 Although most PLWH are based in low- and middle-income countries, treatment access has increased impressively in recent years, resulting in more than 62% of PLWH using ART and 53% of them being virally suppressed. 3
While globally 10% of PLWH are aged ⩾ 50 years, in the United States this percentage has reached 50% and is expected to increase to 70% in 2030. 4 With the ageing of PLWH, causes of death have shifted towards non-communicable diseases, which now account for nearly 70% of deaths. 5 Cardiovascular disease (CVD) has emerged as a leading cause of non-HIV-related mortality and even PLWH with undetectable viral load are twice as likely to develop accelerated coronary artery atherosclerosis compared with similar, age-matched general population individuals. 6 However, studies assessing the association between immune markers and CV outcomes have provided mixed results (Figure 1). 7 Accelerated atherosclerosis in this population seems to be related with non-calcified atherosclerotic plaques, platelet reactivity, pro-coagulant state, inflammation, specific ART exposure and an excess of traditional cardiovascular factors.8,9 Recently, the predominant phenotype of HIV-associated cardiomyopathy has significantly shifted from heart failure with reduced (HFrEF) to heart failure with preserved ejection fraction (HFpEF) and subclinical systolic dysfunction. 10 The pathogenesis of cardiomyopathy is likely multifactorial and may be a result of inflammation due to opportunistic infections, as well as immune dysregulation and micronutrient deficiency, especially in patients with high viral loads and a low number of CD4 cells. 11
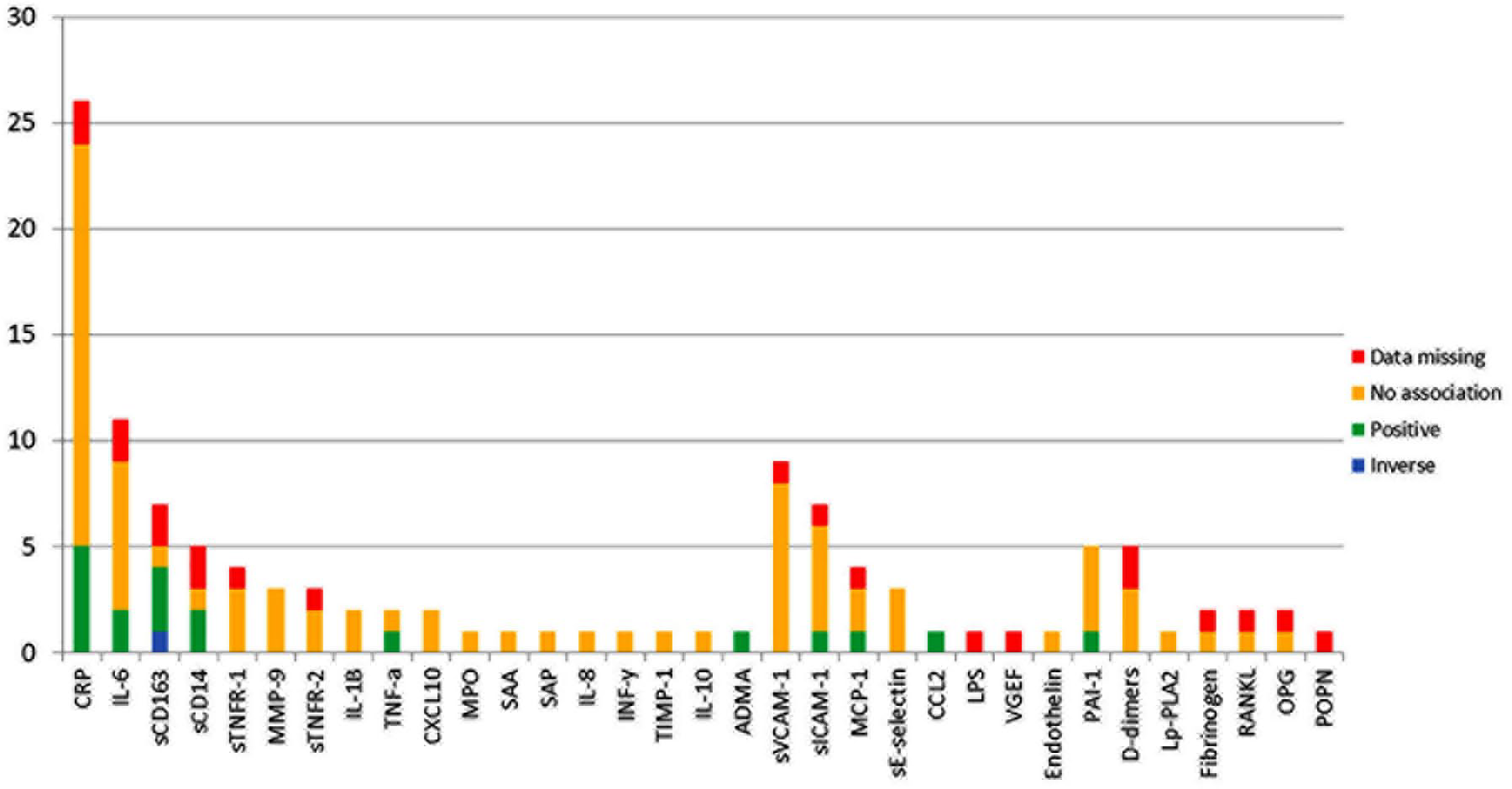
Association of immune markers with surrogate CVD outcomes.
Proposed risk score models developed for general population may underestimate CVD risk in PLWH, as they do not include HIV-specific parameters. 12 Imaging modalities have received mounting attention lately in order to better understand the pathophysiology of subclinical CVD and provide improved risk assessment in this population. 13 Well-established techniques such as conventional echocardiography, pulse wave velocity (PWV), and carotid intima–media thickness (cIMT) continue to be the basis for the diagnosis and subsequent monitoring in this population. However, novel imaging tools such as cardiac computed tomography (CT) and cardiac CT angiography (CCTA), positron emission tomography/computed tomography (PET/CT), and cardiac magnetic resonance (CMR) have provided new insights into accelerated cardiovascular abnormalities in PLWH (Figure 2).
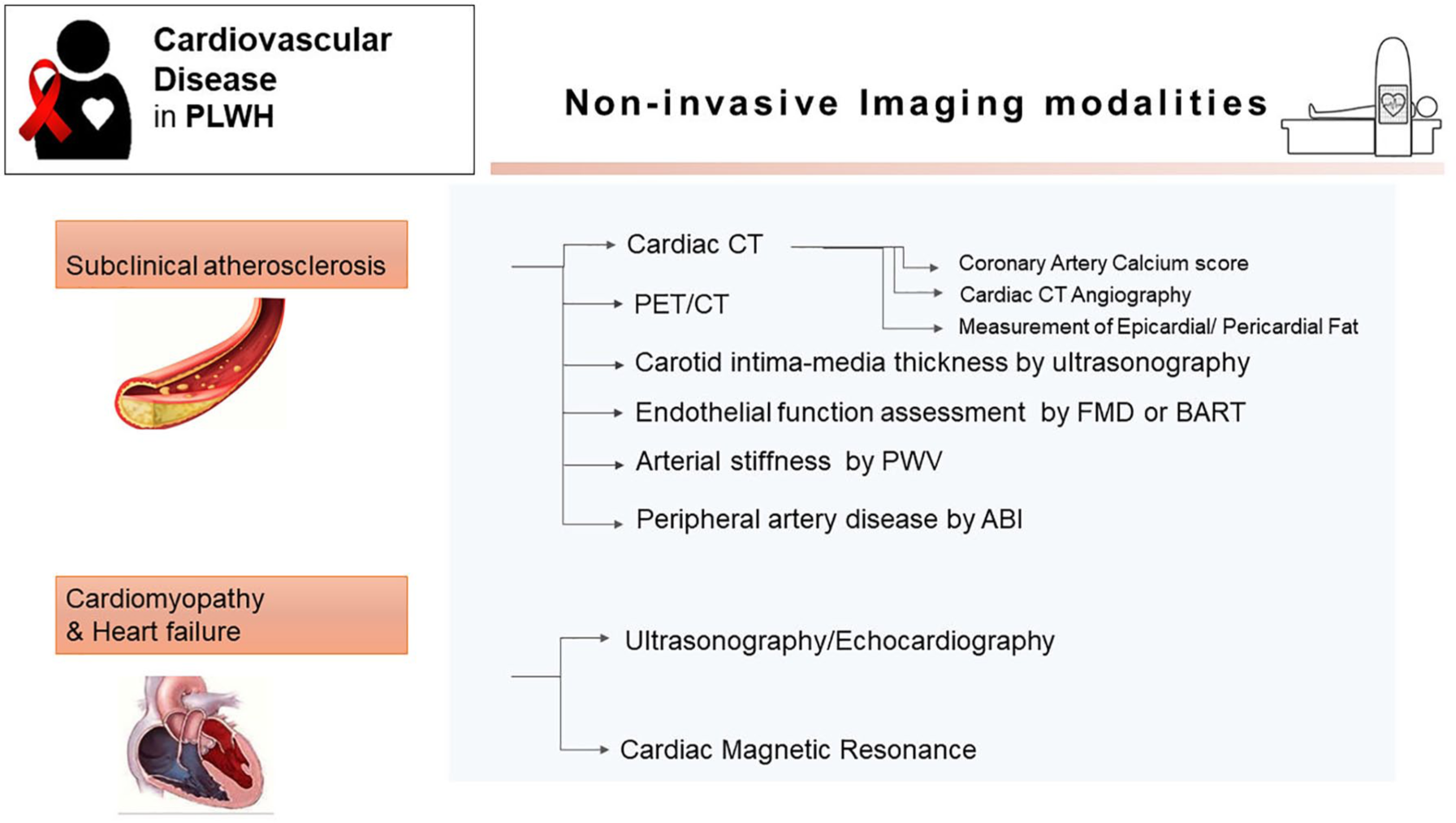
Non-invasive cardiovascular imaging modalities in patients with HIV.
The aim of this review is to provide an overview of the possible additive utility of imaging modalities in screening subclinical CVD and predicting future CVD risk in PLWH, along with discussion of underlying disease mechanisms.
Subclinical cardiovascular atherosclerosis imaging
Given the significant association of subclinical atherosclerosis with incident CVD, several imaging modalities have been established for primary and secondary prevention in the general population. Although the incidence of clinical CVD is low in PLWH, it is two times higher than that observed in individuals without HIV. 1 Cardiac CT and ultrasonography have been used for the diagnosis of subclinical atherosclerosis among PLWH in numerous of studies.
Cardiac CT
Cardiac CT can identify subclinical coronary artery disease (sCAD) by (i) calculating the amount of coronary artery calcium (CAC), (ii) detecting the composition of the atherosclerotic plaque when using intravenous contrast material, (iii) assessing the epicardial/pericardial fat volume and density, and (iv) evaluating arterial inflammation using PET/CT.
Coronary artery calcium (CAC) score
The usefulness of the CACs, using non-contrast CT, to identify sCAD and stratify patients at risk for future CVD events has been documented in the general population.14,15
CAC has been shown to progress more rapidly in PLWH, although this progress may be related mostly to overrepresentation of traditional risk factors. 16 Moreover, a lower prevalence of CAC in a sub-Saharan African cohort of PLWH compared with US subjects was reported, while HIV infection was not associated with a CACs > 0. 17 Importantly, Raggi et al. found that a CACs > 100 was associated with a threefold increased risk for adverse events in PLWH. 18 However, given that CACs does not reliably detect non-calcified plaques, CACs may underestimate the risk of future CVD events among PLWH, who present increased rates of non-calcified atherosclerotic plaques.19,20 Nevertheless, this is still a contentious issue, since more recent studies did not find any significant association between HIV infection and high-risk plaque features.16,17
Cardiac CT angiography (CCTA)
In the general population, sCAD is associated with cardiovascular events. 21 The type of plaques that are considered ‘vulnerable’ are non-calcified, low attenuation plaques with a necrotic, lipid-rich core, napkin-ring sign, spotty calcification, and positive remodeling (Figure 3). Although earlier studies demonstrated a link between HIV infection and sCAD, this association remains controversial, with recent large-scale studies not supporting these findings. These inconsistencies may be attributed to differences in race, age, duration of infection and ART therapy, HIV serostatus, and cardiovascular risk profile between studies.
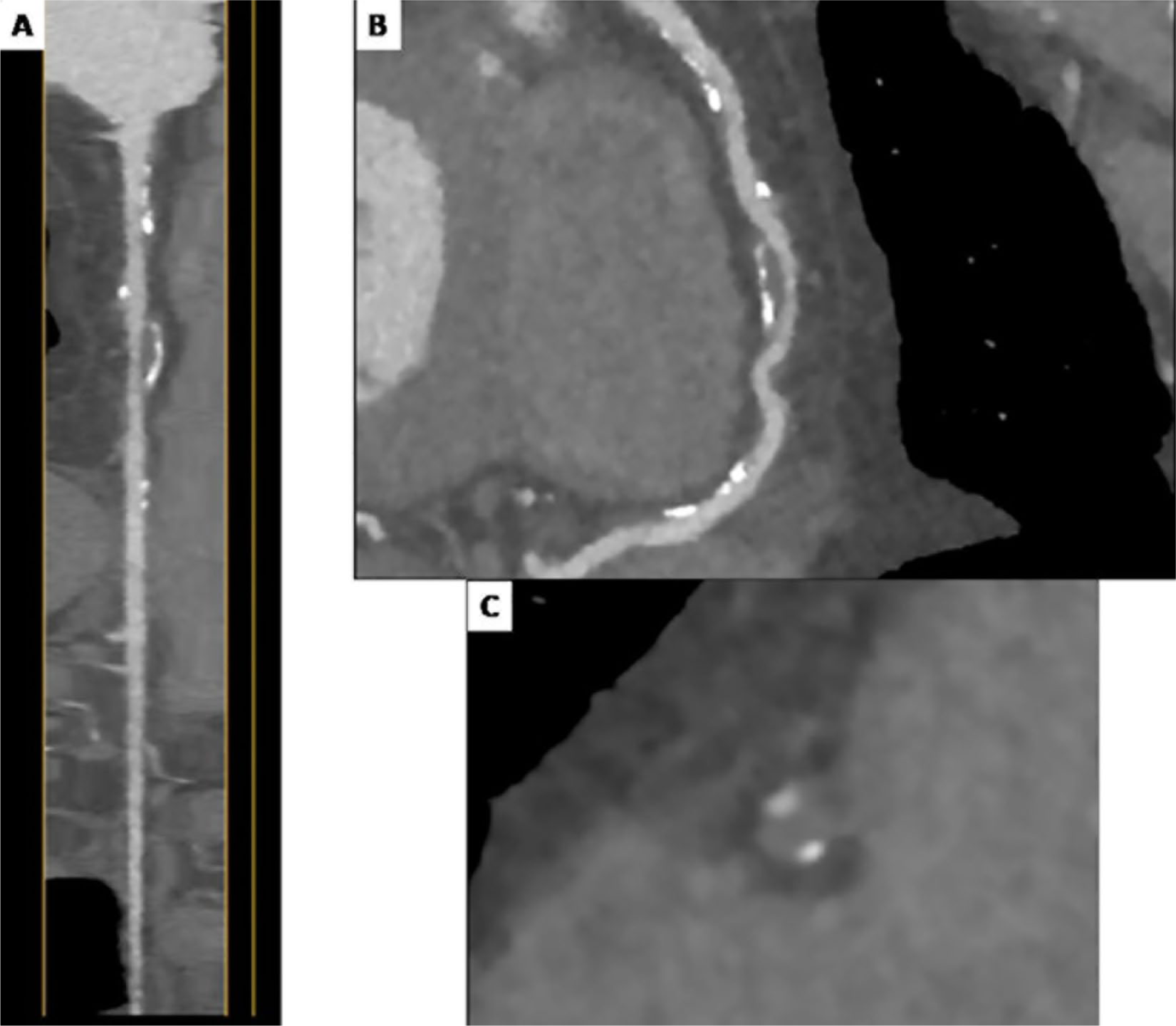
CCTA performed in an asymptomatic 43-year-old man with HIV. (A) Straightened multiplanar reconstruction; (B) multiplanar curved reconstruction; and (C) axial image of an atherosclerotic plaque demonstrating multiple vulnerable characteristics: positive remodeling, low attenuation, and spotty calcification.
In previous reports, prevalent sCAD, assessed by CCTA, was positively associated with elevated levels of monocyte activation biomarkers in treated HIV-infected men, supporting that systemic inflammatory dysregulation contributes to atherogenesis. 22 Asymptomatic HIV-positive men had a higher prevalence and degree of sCAD compared to controls. 23 Moreover, increased levels of soluble CD163, a marker of macrophage activation, was strongly related to the presence of non-calcified coronary plaques among asymptomatic PLWH with undetectable HIV viral load, suggesting that there is a unique inflammatory-related predilection of non-calcified plaques in PLWH. 24 A significant relationship between vulnerable plaque presence and higher degrees of inflammation was also supported by a subsequent meta-analysis of nine studies. 9
Accordingly, a larger prospective observational study, the Multicenter AIDS Cohort Study (MACS), confirmed the positive association of high-risk atherosclerotic plaques with HIV-positive serostatus. 20 The authors also revealed an independent association between degree of sCAD and longer ART duration, which was attributed to the potential adverse metabolic effects of older ART regimens. Accordingly, HIV-positive women also had significantly higher prevalence of non-calcified coronary plaques compared with unaffected female controls, while the HIV-infected women with non-calcified plaques had the highest levels of systemic immune activation. 25
However, these CCTA findings were not confirmed in more recent studies. Thus, in an observational study of 1429 African Americans, there was no significant association between HIV infection and sCAD. 26 Similar findings were published in a large-scale, European CCTA study conducted in Switzerland. 16 After adjustment for Framingham risk scores, 428 infected participants had a similar degree of non-calcified/mixed plaques and high-risk plaques and lower overall coronary atherosclerosis on CCTA than 276 HIV-negative controls. Furthermore, the authors did not identify any association of ART duration with plaque presence. These contradictory data may arise from the well-controlled HIV infection in the era of modern ART regimens and decreasing smoking rates in the latter study. The same group demonstrated an increased risk of non-calcified/mixed plaque presence on CCTA in subjects exposed to abacavir, but not to tenofovir or efavirenz. 27
Further investigation is warranted to determine the association between non-calcified plaque burden and long-term outcomes in PLWH and identify patients at high risk for an acute event, for whom early CCTA screening is required.
Epicardial/pericardial fat
Non-contrast CT has been also used to measure epicardial or pericardial adipose tissue, an imaging marker that has been associated with progression of CAC, traditional CVD factors, and sCAD in the general population. 28 HIV-related subcutaneous fat dysfunction and changes in fat distribution caused by ART, commonly referred to as lipodystrophy, are often seen among PLWH and have been linked to overall mortality. 29 Furthermore, visceral adipose tissue was independently associated with the presence of non-calcified coronary plaque on CCTA among 597 HIV-infected men. 30
Limited data exist regarding the evaluation of epicardial/pericardial fat in PLWH, which, however, suggest their potential contribution to the subclinical atherosclerotic process (Figure 4). 31 A close correlation of epicardial fat with visceral adipose tissue accumulation and CACs was recently reported. 32 Moreover, independent associations of pericardial fat volume/density with markers of inflammation and abnormal diastolic function in PLWH were also reported. 33 Additionally, PLWH seem to have increased epicardial fat compared to controls, which is associated with the presence of coronary plaques and ART duration.34,35 Importantly, Scherzer et al. reported that epicardial fat could predict myocardial infarction and death in PLWH. 36 Nevertheless, further research is required to investigate whether epicardial/pericardial fat is metabolically active, thus promoting an inflammatory milieu that contributes to progression of coronary atherosclerosis.
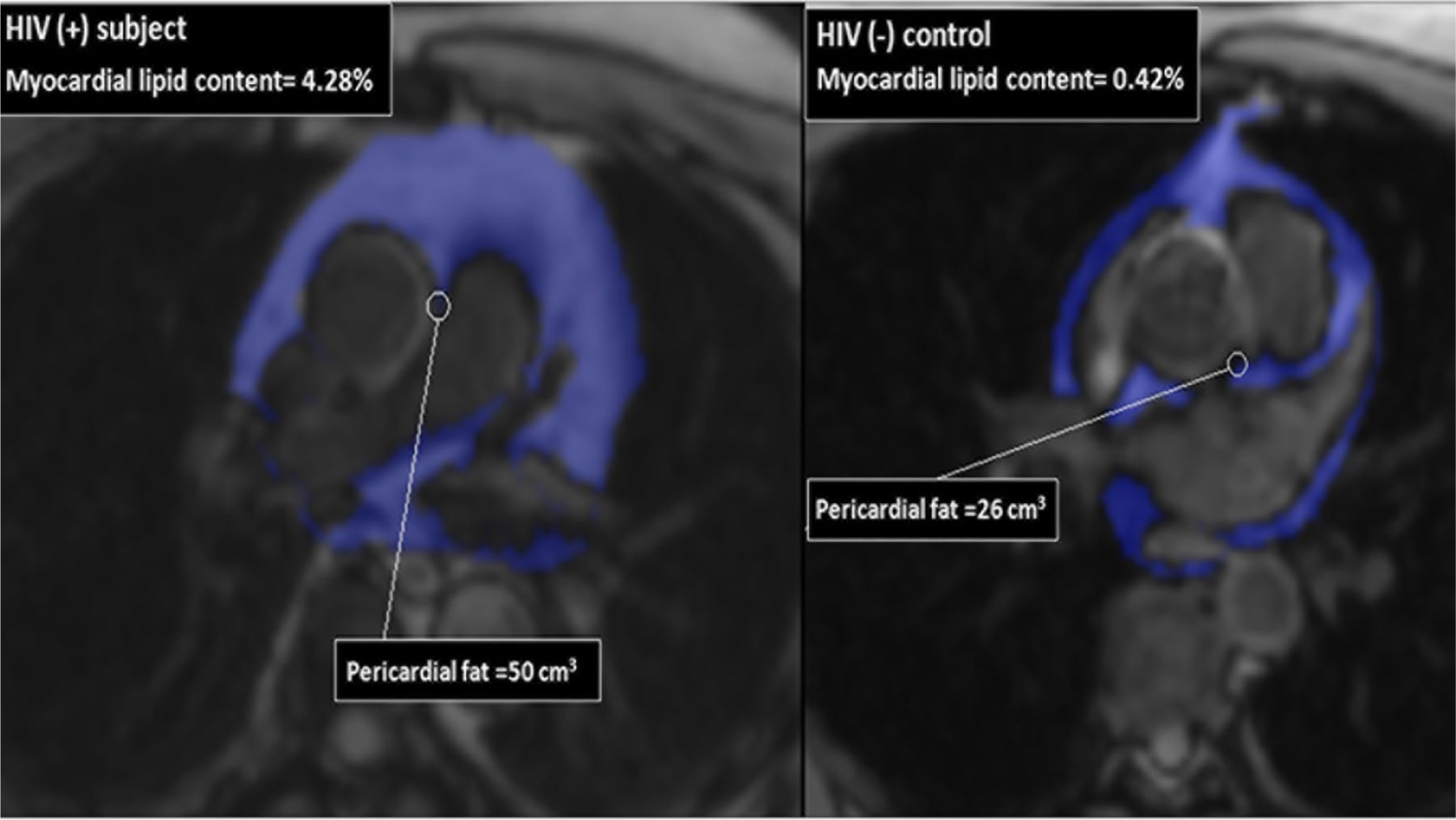
Pericardial fat volume quantification on CMR at the level of the left main origin. Right: the high pericardial fat volume of a 49-year-old patient with HIV, with a BMI of 24 kg/m2 and 27 years on ART. Left: the low pericardial fat volume of a 49-year-old volunteer without HIV, with a BMI of 29.5 kg/m2. ART, antiretroviral treatment; BMI, body mass index; CMR, cardiac magnetic resonance.
PET/CT
Being a hybrid imaging technique, PET/CT provides information about disease process, combining the functional data of PET with the anatomical information of CT imaging, thus offering essential information on the diagnoses, treatment, and long-term monitoring of infectious, inflammatory, and malignant diseases. 37 PET/CT associated with 18F-fluorodeoxyglucose (18F-FDG) uptake provides a measurement of glucose metabolism as a surrogate for inflammation. The increased cellular glucose utilization by inflammatory cells and macrophages results in increased 18F-FDG uptake, an analog of glucose, quantifiable by 18F-FDG PET. Increased arterial 18F-FDG PET/CT uptake is associated with progression of atherosclerotic plaques and identifies the patients at risk for adverse cardiovascular outcomes. 37
Several studies using 18F-FDG PET/CT have been conducted to (i) provide evidence of arterial inflammation in PLWH, (ii) investigate the effects of HIV on CVD, and (iii) assess treatment effect in PLWH.38,39 PLWH with undetectable viral load have significantly higher arterial inflammation in the aorta compared to non-infected controls, and similar aortic inflammation compared to atherosclerotic controls. 39 These findings supported an emerging role of macrophage arterial infiltration in subclinical atherosclerotic process among PLWH. Furthermore, arterial inflammation has been linked to sCAD in HIV. Tawakol et al. published that there was a link between increased arterial inflammation on PET/CT and high-risk coronary plaque morphology on CCTA among PLWH on ART, underlining that inflammation can potentially play a role in the formation of vulnerable atherosclerotic plaques. 40 Recently, a prospective vascular PET/CT study confirmed that HIV was associated with increased aortic 18F-FDG uptake. 41 Contrary, others failed to find a significant difference in carotid and aortic FDG uptake between infected and healthy controls (Figure 5), 42 while a recent study showed that marginally higher aortic inflammation existed in 121 PLWH compared with controls. 43 More recently, there has been increased interest in the use of other than 18F-FDG tracers in PET/CT for the investigation of subclinical atherosclerosis in PLWH. Hence, 18F-sodium fluoride uptake (NaF), a marker of calcification of atherosclerotic plaques, was found to have higher sensitivity to detect sCAD compared with 18F-FDG PET/CT in 93 PLWH on ART. 44 This finding indicates that a PET/CT scan can detect different pathways within the atherosclerotic process, as NaF uptake has been associated with calcification, whereas FDG has been utilized to image arterial inflammation. Future studies are needed to clarify the clinical implications of this observation.
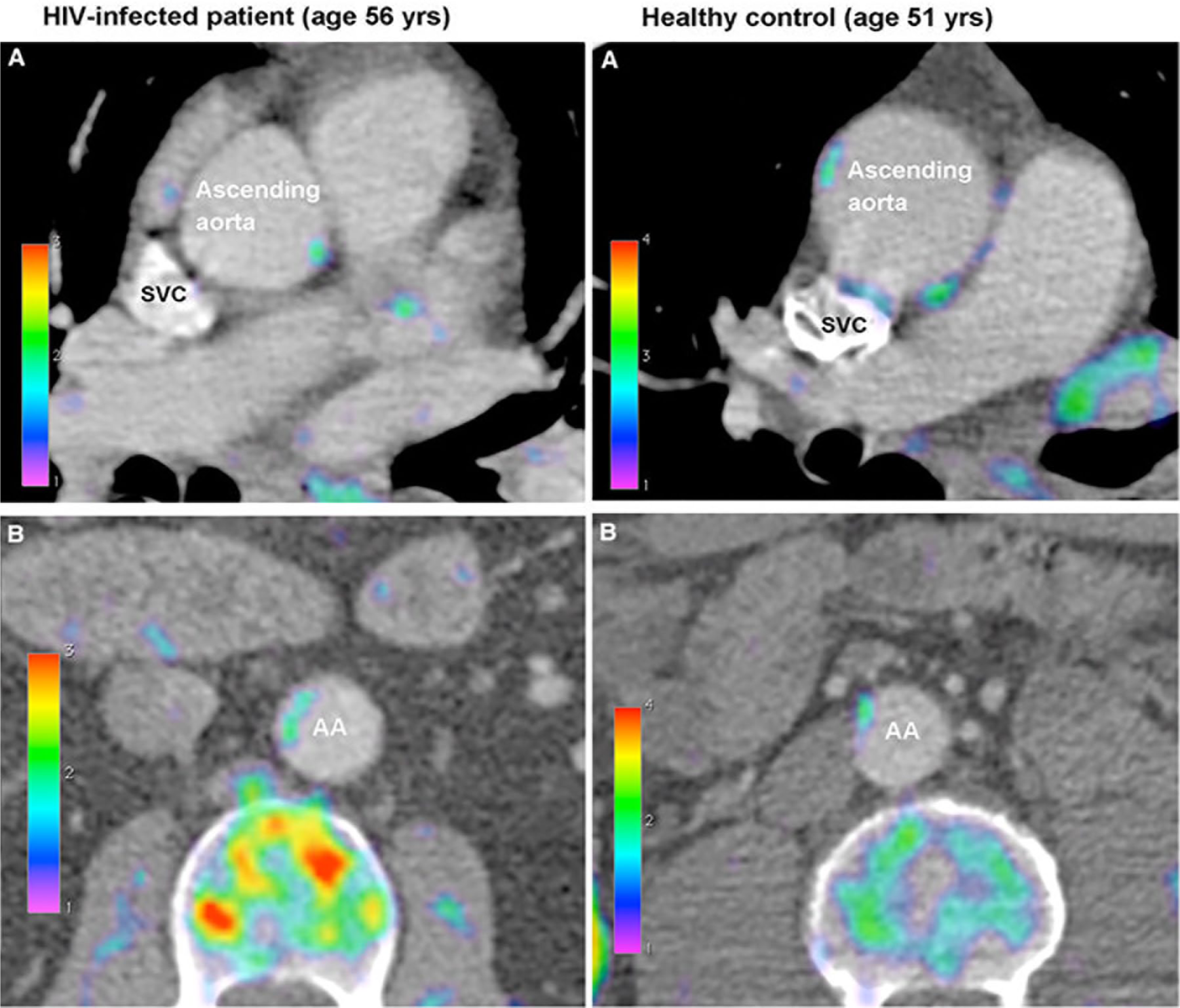
Fusion PET/CT axial images from the ascending (panel A) and abdominal (panel B) aorta of an HIV-infected patient and a healthy control showing modest FDG uptake in the arterial wall.
PET/CT scanning has also been used to evaluate therapy response in HIV infection. Zanni et al. found in a small study of 12 ART naïve individuals that arterial inflammation did not decrease 6 months after ART initiation. 45 Despite the insufficient power of the study, this observation is in keeping with a subsequent trial, in which arterial inflammation appeared to be independent of HIV disease activity. 46 Given that these findings may have important therapeutic implications, further longitudinal studies are required to explore whether the control of viremia alone is insufficient to reduce arterial inflammation and subsequent progression of subclinical atherosclerosis.
Statins have an anti-inflammatory effect on vascular inflammation and a beneficial effect on cardiovascular events in the general population, with increased inflammation and low levels of low-density lipoprotein cholesterol (LDL-C). A significant reduction of non-calcified coronary plaque volume was demonstrated in a randomized, double-blind trial in a group of 40 virally suppressed PLWH with low LDL-C levels after 1 year of treatment with atorvastatin compared to placebo. 47 Unlike the earlier study of Tawakol et al., where early reduction of aortic and carotid inflammation on PET/CT after atorvastatin therapy had been demonstrated in individuals without HIV, 48 Lo et al. did not find any significant between-group differences after longer follow-up among PLWH. 47 Statin therapy for the primary prevention of CAD in PLWH is being addressed by the ongoing REPRIEVE study, a large, multicenter trial assessing the efficacy of pitavastatin to prevent major adverse cardiovascular events. 49
There is evidence that inflammation and chronic immune and platelet activation lead to or amplify peripheral endothelial dysfunction in PLWH. Coronary endothelial dysfunction, a highly predictive marker of future cardiovascular events, has been evaluated using PET/CT in PLWH on ART by a Danish group. 50 They published that myocardial flow reserve was similar in PLWH and controls, in contrast to their earlier longitudinal study where a significant decrease in maximal myocardial perfusion and myocardial perfusion reserve, assessed by PET/CT, and in flow-mediated dilation, were detected after ART initiation.50,51 Nonetheless, its small population and short follow-up, possibly detecting transient alterations, limit this study. Subsequently, the same group demonstrated that HIV-positive women had significantly lower myocardial flow reserve and hence increased cardiovascular risk compared with HIV-positive men, a finding which cannot be readily explained. 52 Further investigation is warranted to determine the pathophysiological link between coronary endothelial function and HIV disease and to assess the utility of PET/CT for early identification of patients at risk of adverse CVD outcomes.
Carotid artery intima-media thickness (cIMT)
cIMT, as measured non-invasively by ultrasonography, has been increasingly used as a surrogate marker of the presence and extent of sCAD, predicting future cardiovascular events in the general population. 53 However, current guidelines do not recommend the routine use of cIMT for primary prevention. 53 cIMT studies in PLWH have yielded conflicting results, with the majority demonstrating significantly higher cIMT, particularly in the bifurcation region, for infected rather than uninfected individuals. 54 The observed divergence among the results can be explained by different approaches in assessing cIMT, the operator-dependency of the technique, inclusion of rather small sample sizes, length of follow-up, and different sociodemographic characteristics. On one hand, large studies did not find differences in cIMT progression in PLWH compared with uninfected controls.55,56 Notably, in the FRAM study, the HIV association was stronger with internal than with common cIMT and it was more prevalent in women than in men, explaining in part why studies measuring cIMT only in the common carotid may have found little association of HIV infection with cIMT. 56
On the other hand, others observed that elevated high-sensitivity C-reactive protein levels were a significant predictor of carotid atherosclerosis progression in the bifurcation compared to the common carotid region among PLWH. 57 The same group in a subsequent longitudinal study found that cIMT and plaque at baseline were independent predictors of death among PLWH, 58 whereas cIMT progression was more rapid in the bifurcation and internal carotid artery regions when compared with common carotid arteries. 59
The role of ART is even less clear than the role of HIV. Accordingly, Vos et al. demonstrated that ART was related to thicker cIMT among rural people living in South Africa, signifying the metabolic and atherogenic effect of ART. 60 These results were consistent with studies carried out in the USA,56,57 but in contrast with other studies conducted in sub-Saharan Africa. 61 Two studies, one using ultrasound and the other magnetic resonance imaging, demonstrated that cIMT progression was likely attributable to an increased prevalence of traditional risk factors in PLWH.62,63
Further data are required to clarify the relation of cIMT with the inflammatory process, as well as its utility for HIV disease risk stratification, and as a surrogate marker for therapeutic interventions using either statins or therapies targeting specific inflammatory pathways.
Endothelial function assessment
Endothelial dysfunction is an important precursor of atherogenesis. 64 Brachial artery ultrasound is a widespread technique for non-invasive assessment of endothelial function, by measuring flow-mediated dilation (FMD). Although endothelial dysfunction in PLWH has been demonstrated in numerous studies, the mechanisms by which this occurs remain incompletely understood. Increased reactive oxygen species production and oxidative stress, as a result of the direct effects of HIV proteins and treatment with ART, have been proposed as the common underlying pathway in the pathogenesis of endothelial dysfunction in PLWH. 65
Brachial arterial reactivity testing (BART) has been used to measure endothelial dysfunction and to assess the impact of ART on vascular pathology in PLWH, with inconsistent findings. A link between HIV infection and endothelial dysfunction, in PLWH not on ART and with detectable HIV RNA levels, has been reported in previous studies, with worse endothelial dysfunction being connected with higher viral loads. 66
The influence of ART on endothelial dysfunction has gained increasing interest in the literature, with studies having yielded divergent results. More recent studies have demonstrated a positive effect of ART initiation on endothelial function, although the degree of improvement likely does not reach levels seen in people without HIV and varies by ART class. A prospective randomized study demonstrated a rapid improvement in FMD in 82 ART-naïve individuals within 4 weeks of ART initiation, highlighting the importance of combined ART to reduce cardiovascular risk in PLWH. 67 Subsequently, Ho et al., extending these findings to a cohort of 74 effectively ART-treated adults, found that worse endothelial function was associated with a low nadir CD4 count, underlying that the degree of immunological compromise prior to initiation of ART was associated with endothelial dysfunction. 68 A meta-analysis indicated that PLWH receiving ART demonstrated no reduction in FMD when compared with those naïve to ART, especially under treatment with protease inhibitor drugs, probably due to altered lipid metabolism. 69
Novel interventions, targeting inflammation and immune activation, are currently being investigated in order to reduce the risk of CVD in PLWH. In a randomized study, pitavastatin improved endothelial function as assessed by BART in infected persons. 70 In another prospective, randomized trial, the use of aspirin did not show any effect on either the markers of immune activation and inflammation or endothelial function measured by FMD in PLWH. 71 Recently, Hsue et al. published that a low dose of methotrexate was safe and associated with a significant decrease in CD8 cells, but did not have significant effects on inflammatory biomarkers and endothelial function in a randomized, multicenter trial comprising 176 treated PLWH. 72 Finally, Macatangay et al. administered dipyridamole in 17 infected individuals on ART for 12 weeks and compared them with 18 infected individuals who received placebo. 73 Although there was no significant difference in FMD between the two groups, dipyridamole significantly decreased activated CD4 cells, underlining that alterations in adenosine metabolism may contribute to T-cell activation in PLWH. Further studies are needed to clarify the mechanisms of endothelial dysfunction in HIV infection and to define intervention targets with beneficial impact in PLWH.
Arterial stiffness
PWV is widely used as a measure of arterial stiffness, a validated surrogate marker of atherosclerosis, which predicts future cardiovascular risk and improves risk classification. 74 Although there is growing evidence that structural and functional changes occur in the large arteries of PLWH, whether aortic stiffness and vascular ageing are influenced by HIV infection ‘per se’ or related to medical/behavioral factors, remains a topic of debate. In a meta-analysis, a link between immunodepression and arterial stiffness was found. 75 By contrast, a subsequent meta-analysis demonstrated conflicting conclusions regarding the impact of HIV infection on vascular health, mainly because of the use of variable techniques to measure PWV and the presence of confounding factors in the studies. 76
PWV studies in PLWH have also yielded conflicting results regarding the impact of ART on arterial stiffness. No differences in PWV and arterial elasticity were seen between infected, treated and untreated participants in the PURE study, 77 while other reports have shown that ART may accelerate the atherosclerotic process, demonstrating a significant increase of PWV in treated PLWH compared with ART-naïve controls, especially under treatment with protease inhibitor-containing drugs.66,78
Moreover, in addition to traditional risk factors, immune markers, such as a low CD4:CD8 ratio and current CD4 < 200/mm3, have been associated with vascular ageing, supporting the deleterious effect of HIV infection on vascular health.66,79 In a recent study conducted in South Africa, Kelly et al. demonstrated that CD4 and CD8 T-cell exhaustion were associated with arterial stiffness, which remained elevated during the first 3 months of ART. 80
Additional longitudinal studies are needed to establish a causal relationship between both immunodeficiency/immune activation and its related drug treatment with vascular ageing in the population of PLWH.
Asymptomatic PAD
Symptomatic or asymptomatic PAD, defined non-invasively as an ankle–brachial index (ABI) ⩽ 0.90, is the third leading cause of CVD morbidity and mortality globally, after CAD and stroke. 81 There are conflicting reports in the literature about whether the prevalence of PAD in PLWH, ranging from 2% to 27%, is higher or lower than in the general population. 82 The observed wide range may be due to small sample sizes, lack of a control group in most studies, different definitions of PAD employed, and the presence of confounding factors. Recent studies found that HIV infection was associated with a higher risk of PAD.83,84 On the contrary, others have shown low prevalence of PAD in PLWH that is similar to the prevalence in the general population. 85 Recently, a large cross-sectional study did not report an association of HIV infection with PAD beyond that of traditional vascular risk factors. 86
Conflicting results have also been reported regarding the role of ART on PAD. Agu et al. published that an ABI < 0.9 had a positive link with ART and CD4 count < 200 cells/mL, as well as an inverse relationship with treatment duration, in a Nigerian HIV group. 87 In contrast, Kwiatkowska et al. did not find any relation between ABI alterations and either the status or the course of HIV infection or duration of ART treatment in 111 Polish PLWH compared with 40 uninfected controls. 85
Taken together, inconsistent data probably indicate the underdiagnosis and undertreatment of PAD among PLWH. Further longitudinal studies are needed to understand the role that HIV treatment plays in PAD prognosis.
Risk of heart failure
Echocardiography
PLWH have increased risk of HF. 88 Although in the pre-ART era the predominant HIV-related echocardiography findings were decreased left ventricular systolic function, in the ART era the prevailing HF phenotypes appear to be diastolic or/and subclinical systolic dysfunction. 89 Tissue Doppler imaging and speckle tracking (Figure 6) are more sensitive techniques to detect early changes in myocardial function compared with conventional echocardiography. 90
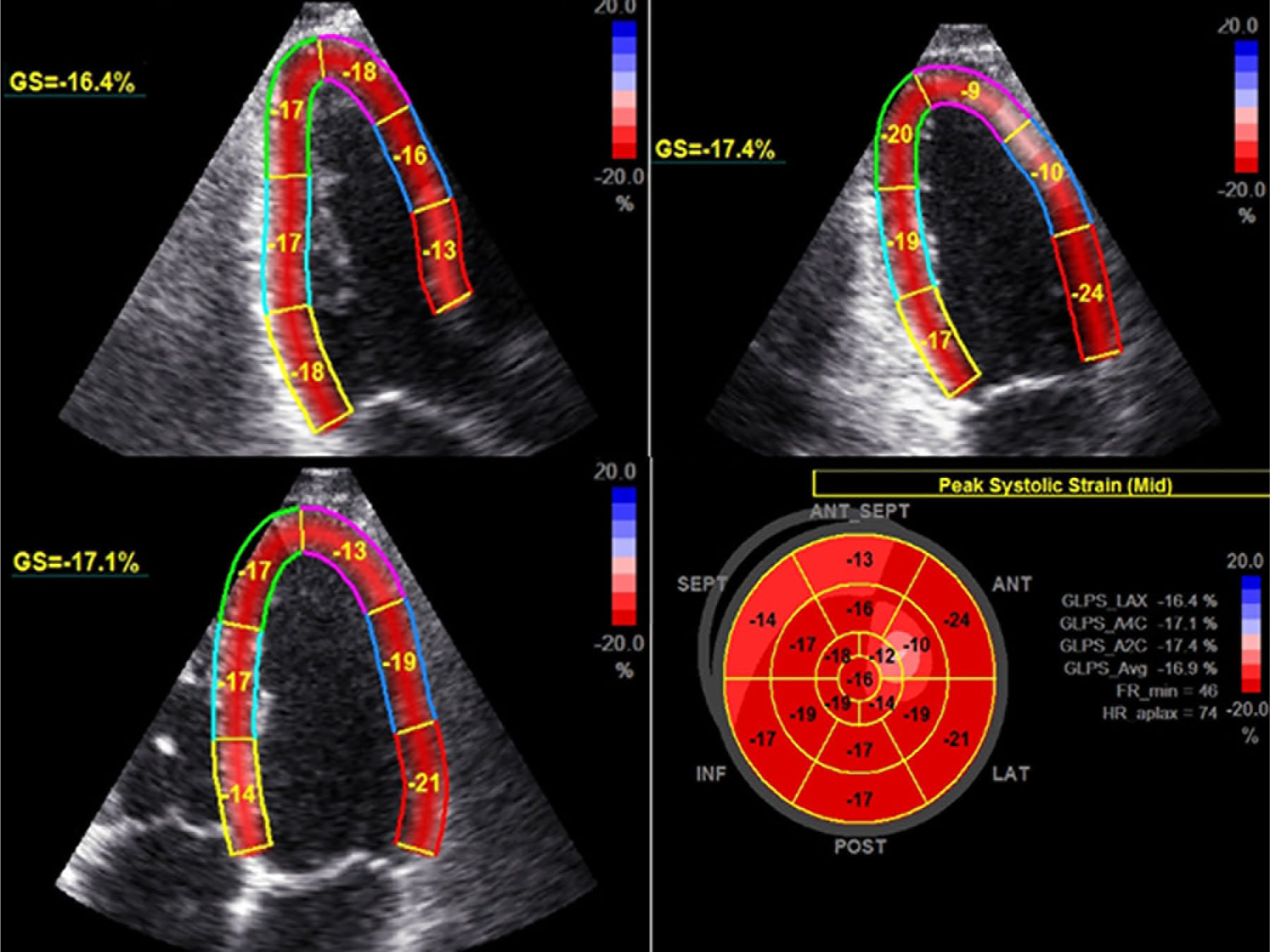
Left ventricular global and segmental strain analysis from standard views and bull’s eye diagram, performed in a 34-year-old asymptomatic HIV-positive man. (A) Apical three-chamber view; (B) apical two-chamber view; (C) apical four-chamber view; and (D) bull’s eye map. Despite two-dimensional echocardiography demonstrating a normal left ventricle ejection fraction of 65%, speckle tracking echocardiography revealed GLS of –16.9%, indicating subclinical cardiomyopathy.
In a recent meta-analysis that included 125,382 PLWH, HF prevalence was 6.5% higher than that reported by studies in the general population, despite the lower average age of PLWH. 89 Furthermore, there was a suggestion of decline in HFrEF and rise in HFpEF over a 30-year period. Consistent with these findings, an increased incidence of HF among PLWH and a shift towards HFpEF were also confirmed by others. 91 On the contrary, in South Africa, where ART uptake is lower, a high prevalence of systolic dysfunction (28%) was found among PLWH, without any case of HFpEF being reported. 92
Although HIV is associated with a higher risk of developing diastolic dysfunction, the pathophysiological mechanism is still unclear. 93 In the contemporary CHART study, diastolic dysfunction was associated with alterations in cardiac structure and function, as assessed by speckle tracking echocardiography, findings which were not evident on routine imaging. 94 In keeping with this, Buggey et al. also found that Ugandan HIV participants had an increased left ventricular mass index, decreased left ventricular global longitudinal strain, and higher odds of diastolic dysfunction compared with matched individuals without HIV. 35
Further research is needed to clarify the prognosis of these cardiac abnormalities and to inform about prevention and treatment strategies.
Cardiac magnetic resonance (CMR)
CMR and magnetic resonance spectroscopy techniques allow an extensive assessment of cardiac structure, function, and fat metabolism in asymptomatic PLWH. HIV-related myocardial fibrosis and steatosis, diastolic dysfunction, and subclinical systolic dysfunction have been demonstrated in CMR studies. 95 Cardiac steatosis was related with deranged plasma lipids, while the presence of fibrosis was likely attributed to subclinical myocarditis. Subclinical myocardial inflammation derived from CMR indices was also reported by Luetkens et al. 96 In keeping with these studies, Ntusi et al. demonstrated alterations in systolic and diastolic function and a high prevalence of chronic subclinical myocardial edema and fibrosis in PLWH on ART in sub-Saharan Africa. 97 Similarly, Thiara et al. found reduced systolic function, evident by strain parameters, despite normal ejection fraction in 95 PLWH, 93% of whom were on ART. 98 Subclinical myocardial dysfunction was associated with increased levels of systemic immune biomarkers, myocardial steatosis, and diffuse myocardial fibrosis.
We need further longitudinal and randomized control trials to better evaluate the prevalence, the mechanism, and the prognostic significance of cardiac steatosis, as well as potential therapeutic interventions which may improve cardiac abnormalities in PLWH.
Future perspectives
With CVD burden having tripled among PLWH over the last two decades, early and effective detection of high-risk patients has become increasingly important. Given that HIV-associated CVD is responsible for 2.6 million disability-adjusted life years per annum with the majority in sub-Saharan Africa, there is an imperative need for more research from this area of the world. 1 Ιmaging modalities have provided new insights into the pathophysiological process of subclinical CVD in PLWH, and could be potentially useful for screening, risk prediction, and re-stratification, especially in those who are considered to be at intermediate risk. However, at present, given the insufficient data for the additive value of imaging on commonly used risk algorithms, the routine use of different screening modalities in this special population is not recommended. However, when abnormal values of such markers are identified, reclassification of the individual into a higher CVD risk category should be considered and thus aggressive management and diligent monitoring is advised. Additional large-scale, prospective studies should be undertaken to assess the ability of subclinical imaging markers to improve risk stratification and meaningfully alter outcomes in PLWH. Furthermore, novel imaging techniques, such as carotid temperature assessment by microwave radiometry, which have produced promising results in other patient cohorts, should also be tested in PLWH. 99
Footnotes
Acknowledgements
We would like to thank Georgios Benetos (National and Kapodistrian University of Athens, School of Medicine, Hippokration Hospital, Athens, Greece) for kindly providing Figure 3.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.