
Abstract
We retrospectively analyzed all endovascular procedures of infrapopliteal arterial lesions (n = 383) performed in 270 patients at our institution between December 2008 and January 2018. The overall technical success rate was 97% and yielded 98% for stenoses (n = 214) and 95% for occlusions (n = 169). Trans-Atlantic Inter-Society Consensus (TASC II) classification had no impact on success rates (TASC A + B vs C + D; 96.5% vs 96.9%, p = 0.837). Freedom from clinically driven target lesion revascularization (TLR) after 6 and 12 months was 88.3% and 77.2%. TLR was comparable for TASC A to C lesions and no difference was observed comparing groups of moderately complex TASC A/B lesions and more complex TASC C/D lesions (TASC A + B vs C + D; 78.5% vs 74.2%, p = 0.457). Freedom from TLR was significantly lower in very complex TASC D lesions (TASC A + B + C vs D; 79.7% vs 42.5%, p < 0.001). Multivariate analysis identified TASC D lesions (hazard ratio D/A: 1.5; overall p = 0.002), Fontaine class III and IV (hazard ratio III or IV/IIa or IIb: 2.4; p = 0.041), and occlusive lesions (hazard ratio occlusion/stenosis: 2.4; p = 0.026) as predictors for TLR. In conclusion, endovascular therapy for infrapopliteal artery disease was safe and accompanied with a promising long-term outcome.
Keywords
Introduction
Peripheral artery disease (PAD) is common, showing high prevalence rates of up to 15–20%, increasing with age.1–6 In these patients, arterial stenoses or occlusions may be present anywhere from the aortic bifurcation downstream to the pedal arteries of the lower limb. By far the most frequently underlying pathology observed is atherosclerosis, but in rare cases may also be linked to arteritis, radiation injury, trauma, or embolism. 7 Typical symptoms comprise intermittent claudication, rest pain or ulcer of the foot. However, with the infrapopliteal arteries being the vascular territory located at the very periphery of the vascular system, a variety of challenges regarding both diagnostics as well as therapy arise.
Recently, endovascular therapy has emerged as an established treatment option in PAD. In the light of an ongoing lack of randomized trials addressing treatment options for lower limb PAD, treatment strategies are based on expert recommendations such as the Inter-Society Consensus Documents for the Management of Peripheral Arterial Disease (Trans-Atlantic Inter-Society Consensus [TASC] I and II), the ESC (European Society of Cardiology) or AHA (American Heart Association) Guidelines.7–10 In general, a paradigm shift in treatment strategies for PAD could be observed over the years towards an endovascular-first approach for the majority of even anatomically complex lesions. This shift in clinical practice is due to the continued evolution and improvement of technology for endovascular treatment of PAD (i.e. particularly wires, balloons, and stents). At the same time, the influence of comorbidity, patient preference, and physician experience were highlighted. However, in 2015, for the first time, a dedicated subunit of the TASC document focused on infrapopliteal disease and its staged treatment. 11 The updated TASC II document classifies infrapopliteal lesions into categories TASC A – D. TASC A lesions representing the least and TASC D lesions the most complex form of lower limb atherosclerosis. So far there is only limited data from smaller studies, suffering from several methodical limitations, validating the TASC classification against outcomes.12,13
The aim of our study was to analyze all endovascular procedures of the infrapopliteal arterial vasculature performed over the last decade at our institution, considering the recently published updated TASC II classification, and to search for potential risk factors predicting the clinical outcome.
Methods
Patients
A total of 410 interventions in infrapopliteal lesions were performed between December 2008 and January 2018 at our institution. After excluding interventions in restenosis (n = 27), 383 lesions were included in the analysis. Standard institutional criteria for revascularization were hemodynamic significant stenosis ⩾ 50%, including total vessel occlusion in the presence of symptoms and/or trophic lesions. Symptoms were individually assessed for every patient based on the Fontaine classification. While improvement in quality of life was considered the primary purpose in patients with intermittent claudication (Fontaine stages IIa and IIb), limb salvage was the primary intention in patients with critical limb ischemia (CLI) (i.e. Fontaine stages III and IV). Other aspects taken into account in the decision-making process were concomitant diseases, life expectancy, and finally, patient wish. Standard diagnostic workup before and after the endovascular procedure consisted of ankle–brachial index (ABI) measurement and duplex ultrasound in all patients, and, optionally, magnetic resonance imaging or computed tomography if necessary. All participants provided written informed consent for the clinical procedure. In accordance with the local ethics committee, our retrospective analysis did not require additional informed consent. Whether plain angioplasty with or without a drug-eluting balloon (DEB) or a stent was utilized was left at the discretion of the interventionalist. All patients received a loading dose of clopidogrel followed by a dual antiplatelet therapy, including aspirin, for at least 4 weeks in total or longer depending on the usage of drug-eluting devices.
Angiography
Lower limb angiograms were digitally recorded. Qualitative morphological lesion characteristics, including degree of stenosis, lesion localization (peroneal artery, tibial-peroneal trunk, anterior or posterior tibial artery), and TASC classification, were evaluated by experienced interventionalists and defined visually.
TASC classification
TASC anatomic artery lesion classification is a characterization of the various patterns of atherosclerotic disease and provides guidance on treatment decisions. 11 Hereby, TASC A lesions representing the least complex (i.e. focal stenosis) and TASC D lesions the most complex (i.e. diffuse, occlusive) form of lower limb atherosclerosis. In TASC classification of infrapopliteal disease, TASC A lesions are defined as single focal stenosis, ⩽ 5 cm in length, in the target tibial artery, with occlusion or stenosis of similar or worse severity in the other tibial arteries. TASC B lesions consist of multiple stenoses, each ⩽ 5 cm in length, or a total length ⩽ 10 cm or a single occlusion ⩽ 3 cm in length, in the target tibial artery, with occlusion or stenosis of similar or worse severity in the other tibial arteries. TASC C lesions comprise multiple stenoses in the target tibial artery and/or single occlusion with a total lesion length > 10 cm, with occlusion or stenosis of similar or worse severity in the other tibial arteries. And finally, TASC D lesions are those with multiple occlusions involving the target tibial artery with a total lesion length > 10 cm or dense lesion calcification or nonvisualization of collaterals and the other tibial arteries occluded or with dense calcification. 11
Follow-up and main endpoint
Follow-up visits to the outpatient department of our clinic were routinely scheduled at 6 and 12 months after the index intervention, including interview and clinical examination. In the presence of clinical symptoms or a deteriorating wound situation, ABI measurement and duplex ultrasound examination were carried out. Restenosis was defined as a peak systolic velocity ratio > 2.4. Patients with both clinical symptoms and evidence of restenosis assessed by duplex ultrasound were scheduled for repeated angiography. Angiographic restenosis was defined as diameter reduction in the intervened vessel ⩾ 50% or occlusion.
Clinically driven target lesion revascularization (TLR) is the main endpoint of this trial. It is defined as revascularization of a previously intervened arterial segment performed on a patient who returns with clinical symptoms or a deteriorating wound situation and evidence of restenosis assessed by duplex ultrasound, following endovascular treatment of infrapopliteal PAD.
Statistical analysis
Characteristics of the patients, lesions, procedures, and follow-up outcomes are summarized using descriptive statistics: mean and SD for quantitative data and frequency (%) for qualitative data. Qualitative data were compared using the chi-squared test. The Kaplan–Meier method was applied to estimate freedom from clinically driven TLR. Kaplan–Meier curves and 95% confidence bands are given for the whole study cohort as well as subgroups of interest. Univariable and multivariable Cox regression models were fitted to investigate the influence of the potential predictor variables on the risk of restenosis/reocclusion. The estimated effect of each variable is presented as the hazard ratio (HR) together with 95% CIs. Data were analyzed using R 4.0.0 ×64 (R Foundation for Statistical Computing, Vienna, Austria), IBM SPSS Statistics, Version 26 (IBM Corp., Armonk, NY, USA), and SAS 9.4 (SAS Institute Inc., Cary, NC, USA).
Results
Patient characteristics
A total of 383 interventions were performed in 270 patients with de novo lesions of the infrapopliteal arteries. Patient characteristics of all patients evaluated are shown in Table 1. Average patient age was 73 ± 9.6 years and two-thirds of patients were male. The most common cardiovascular risk factors were hypertension and hypercholesterolemia, which were present in roughly 90% of patients. About half of all patients suffered from diabetes and had a history or present status of smoking. Cardiovascular comorbidities such as coronary artery disease (CAD) or carotid artery stenosis were found in the majority of patients. One-third of patients presented with CLI. Three-quarters of patients had a multilevel PAD involving at least one further region of the lower limb vasculature.
Patient characteristics.
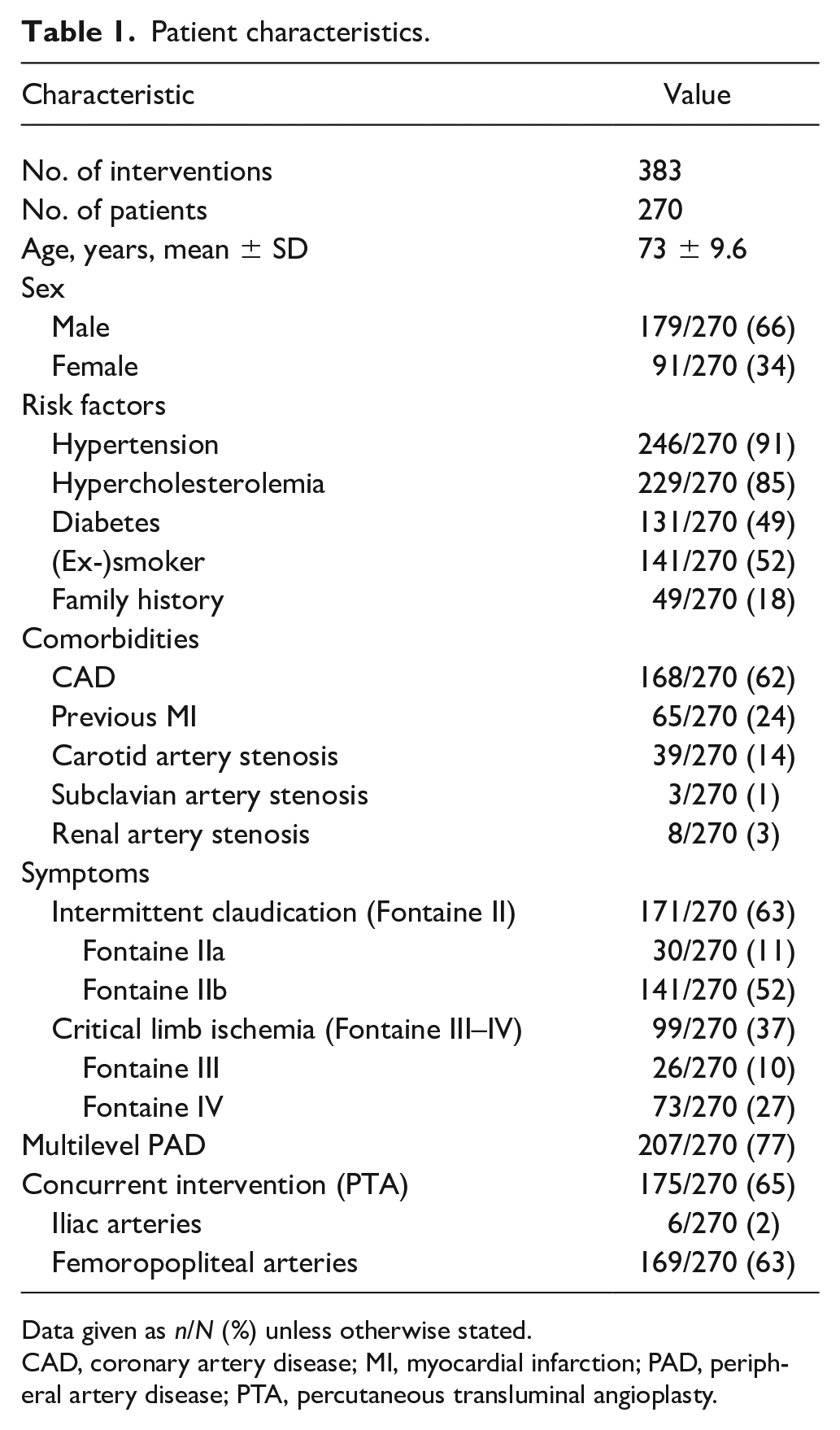
Data given as n/N (%) unless otherwise stated.
CAD, coronary artery disease; MI, myocardial infarction; PAD, peripheral artery disease; PTA, percutaneous transluminal angioplasty.
Lesion characteristics
All lesion characteristics are summarized in Table 2. Lesions of the tibial-peroneal trunk or the anterior tibial artery were predominant, accounting for two-thirds of all endovascular procedures. The residual third of interventions were performed in lesions of the posterior tibial artery or the peroneal artery. Distribution between stenotic and occlusive lesions was equal. The majority of lesions were categorized as TASC A and B, while about one-third accounted for complex TASC C and D lesions.
Lesion characteristics.
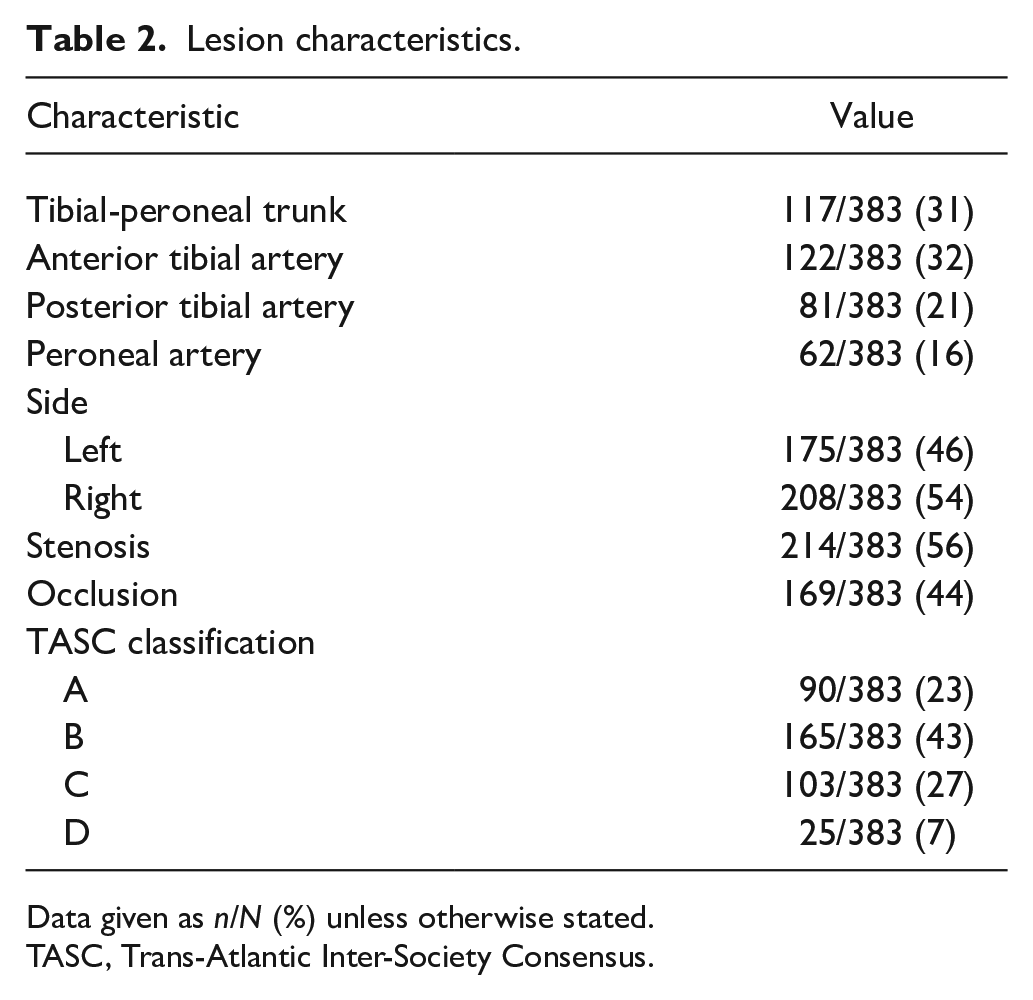
Data given as n/N (%) unless otherwise stated.
TASC, Trans-Atlantic Inter-Society Consensus.
Procedural characteristics
A total of 363 of 383 (95%) lesions were treated using an antegrade approach (i.e. ipsilateral cannulation of the common femoral artery). In 13 lesions (3%), a contralateral puncture was performed and the catheter advanced retrograde followed by a crossover maneuver in the aortic bifurcation. In the remaining seven lesions (2%), retrograde access from a pedal artery was chosen. As part of a procedure that included endovascular therapy of higher order arteries during the same interventional session, 245 (64%) of 383 lesions were treated. The overall technical success rate of the endovascular procedures was 96.7%. Successful treatment was achieved for 210 of 214 stenotic lesions (98.1%) and 160 of 169 total occlusions (94.7%). Lesion complexity defined by the TASC II classification had no impact on success rates when comparing moderately complex TASC A and B lesions to more complex TASC C and D lesions (TASC A + B vs C + D; 96.5% vs 96.9%, p = 0.837; Table 3). The majority of lesions were treated with plain balloon angioplasty. In one-quarter of lesions, the implantation of one or more stents was performed. Hereby, predominantly drug-eluting stents (DES) (89%) such as Xience (45%), Cypher (18%), Resolute (13%), Promus (6%), and Endeavor (6%) were used, while 11% were bare-metal stents (BMS) including Smart (6%) and Chromis (4%), and a single lesion was treated with an EverFlex stent. In 6% of lesions, a DEB was used.
Procedural characteristics.
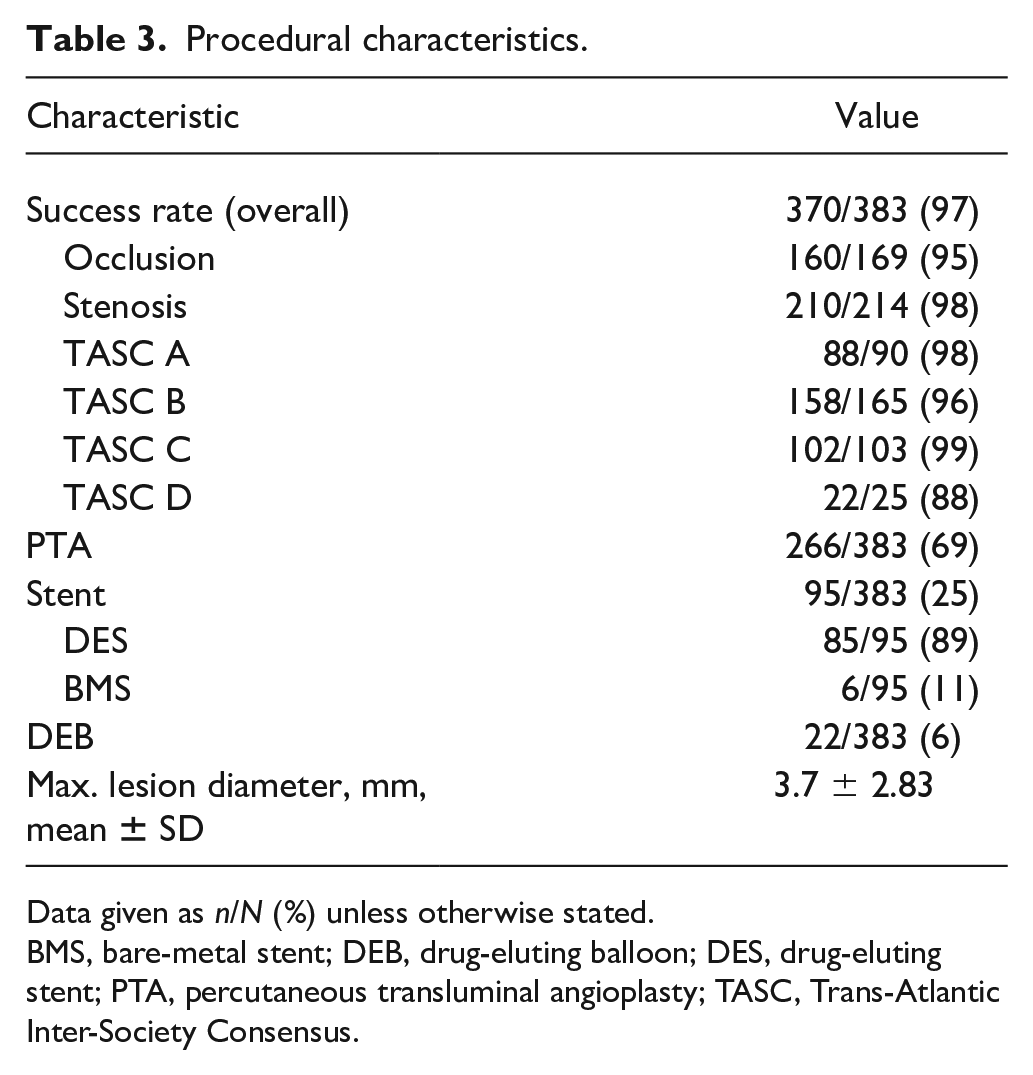
Data given as n/N (%) unless otherwise stated.
BMS, bare-metal stent; DEB, drug-eluting balloon; DES, drug-eluting stent; PTA, percutaneous transluminal angioplasty; TASC, Trans-Atlantic Inter-Society Consensus.
The overall periprocedural complication rate was low (7.7%) and consisted of access site complications (i.e. pseudoaneurysm (n = 9) and bleeding requiring blood transfusion (n = 17)). None of these patients needed surgical intervention.
Clinical follow-up
Clinical follow-up was available for 303 (79%) of the 383 lesions treated. The characteristics of patients lost to follow-up are summarized in online Supplemental Table 1. The median follow-up time was 6 months (range: 1–54 months). Two patients died in the follow-up period. The estimated probability of freedom from clinically driven TLR was 88.3% (95% CI: 84.2–92.4%) at 6 months and 77.2% (95% CI: 70.5–83.9%) at 12 months. In detail, 27 lesions (nine in claudicants and 18 in patients with CLI) received TLR after 6 months and 42 lesions (20 in claudicants and 22 in patients with CLI) after 12 months.
Predictors for clinically driven TLR identified by univariate analysis were the presence of CLI expressed by Fontaine class III and IV classification (p = 0.005), location of intervention within the anterior or posterior tibial arteries (i.e. distal lesions (p = 0.011)), and treatment of occlusive (p = 0.011) and very complex TASC D lesions (p < 0.001) (Figures 1–3; Table 4). No difference in clinically driven TLR was observed when comparing groups of moderate TASC A/B and more complex TASC C/D lesions (TASC A + B vs C + D; 78.5% vs 74.2%, p = 0.457). However, freedom from clinically driven TLR was significantly lower in very complex TASC D lesions (TASC A + B + C vs D; 79.7% vs 42.5%, p < 0.001) (Figure 3).
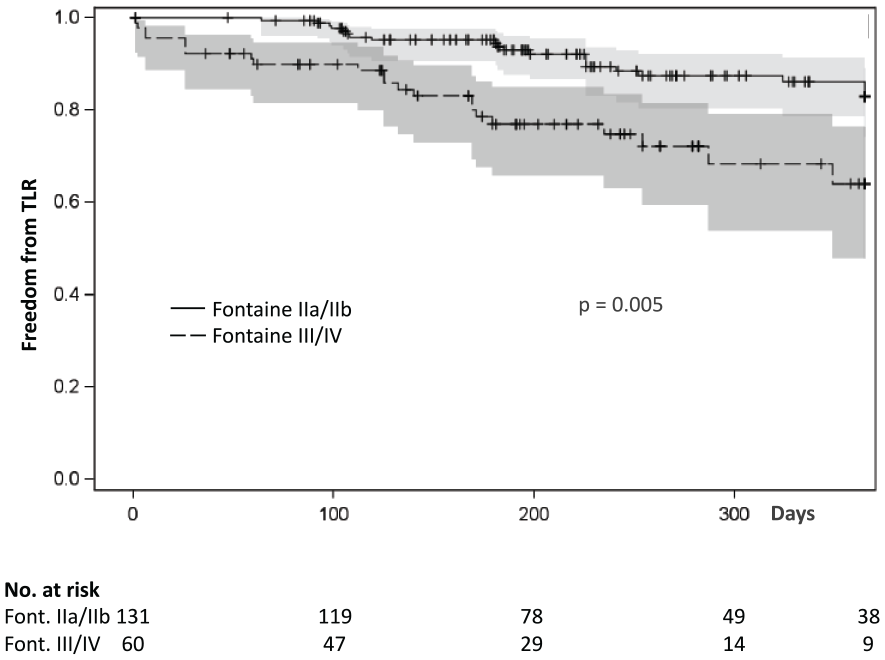
Kaplan–Meier freedom from TLR by Fontaine class.
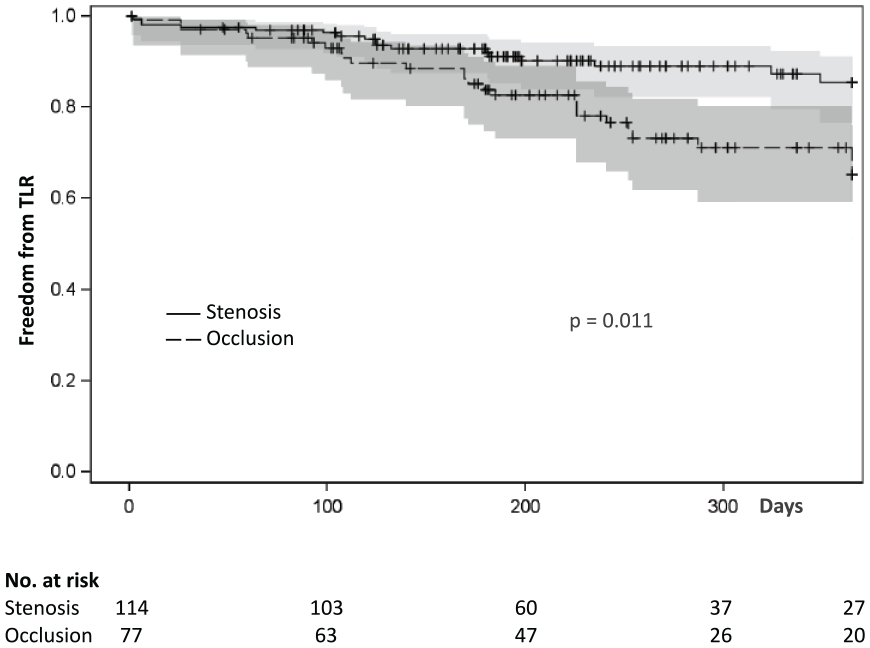
Kaplan–Meier freedom from TLR by lesion type.
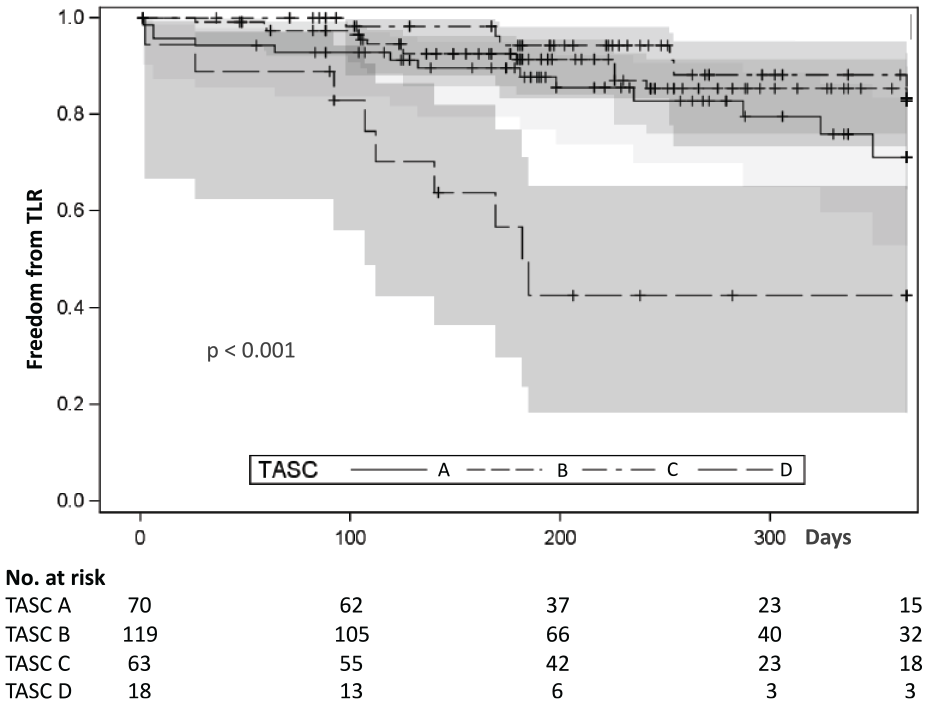
Kaplan–Meier freedom from TLR by TASC classification.
Univariable predictors of TLR.
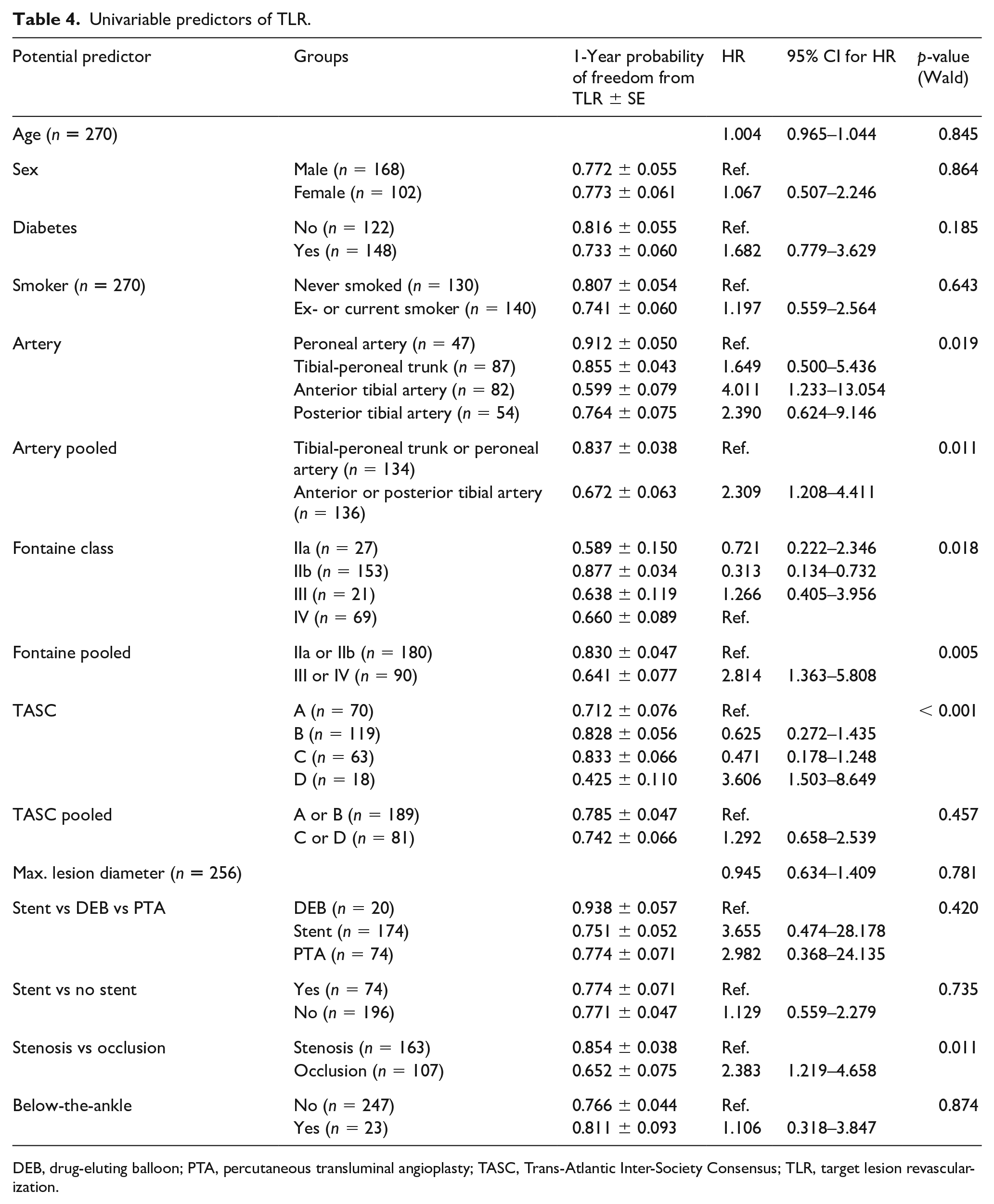
DEB, drug-eluting balloon; PTA, percutaneous transluminal angioplasty; TASC, Trans-Atlantic Inter-Society Consensus; TLR, target lesion revascularization.
In a multivariate analysis, the remaining significant predictors for TLR were CLI; that is, Fontaine class III and IV (p = 0.041), the presence of occlusive lesions (p = 0.026), and very complex TASC D lesions (p = 0.002) (Table 5). However, the type of intervention performed (i.e. stent, DEB or percutaneous transluminal angioplasty (PTA)) (p = 0.420), as well as the level of intervention above or below the ankle (p = 0.874), did not have a significant effect on the clinical outcome.
Multivariable predictors of TLR.
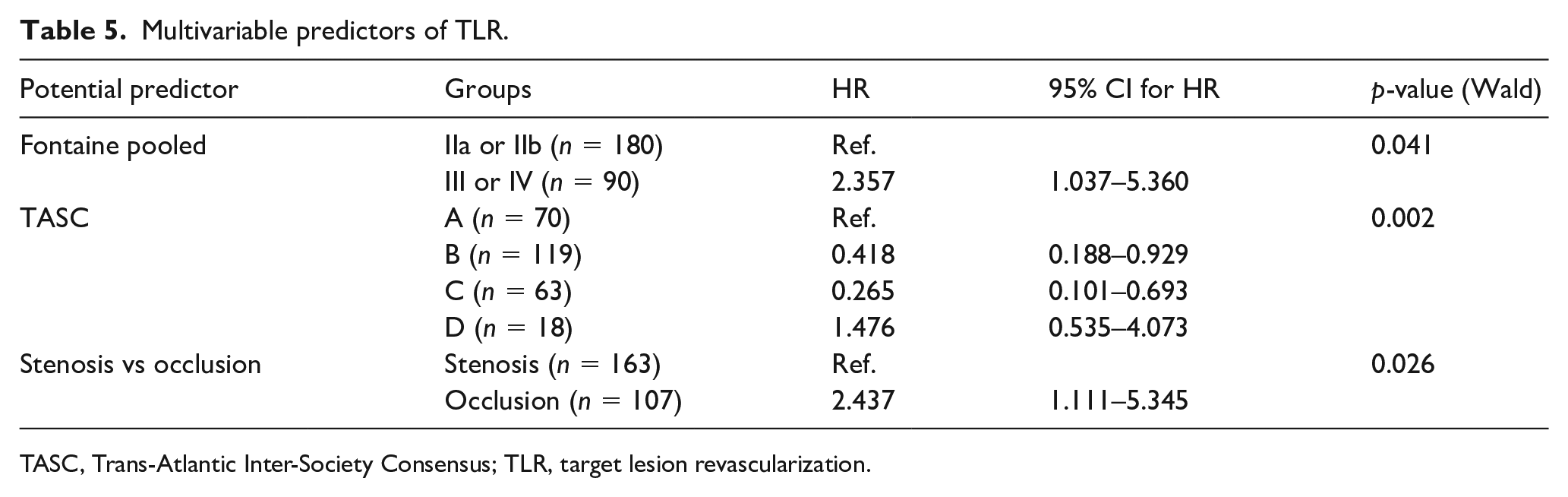
TASC, Trans-Atlantic Inter-Society Consensus; TLR, target lesion revascularization.
In an additional analysis limited to lesions in patients presenting with CLI, TASC D (i.e. very complex lesions) was a significant predictor of clinically driven TLR (p = 0.005) (online Supplemental Table 2).
Discussion
The major finding of this study is that endovascular therapy for infrapopliteal artery disease was safe and accompanied with promising long-term outcomes even in complex lesions as defined by the updated TASC II classification.
Recommendations for vascular care
As there is still a lack of randomized clinical trials comparing endovascular therapy and surgery for infrapopliteal disease, decision-making for revascularization in routine clinical practice is based on expert recommendations, such as the Inter-Society Consensus Documents for the Management of Peripheral Arterial Disease (TASC I and II), the ESC or AHA Guidelines.7–10 The original TASC document published in 2000 provided general recommendations for a primary endovascular or surgical approach based on the complexity of the underlying lesion. 8 These recommendations have been revised twice and for the first time in 2015 a dedicated subunit focused on the management of infrapopliteal disease. 11 However, to our knowledge, so far there have been only two smaller studies evaluating this recently published classification against outcomes.12,13 To date, AHA Guidelines support endovascular treatment solely for infrapopliteal PAD in patients with CLI and not for those with intermittent claudication. Given the promising results of this study, the concept of an endovascular-first approach including anatomically complex lesions is further supported and, moreover, endovascular therapy for below-the-knee lesions as an adjunct to femoropopliteal interventions may be considered a suitable strategy in patients with claudication in order to achieve sufficient arterial runoff.
Patient population
Whereas the majority of patients in our study were claudicants and approximately 40% suffered from CLI, in most previously published trials evaluating interventional therapy for infrapopliteal disease the populations mainly consisted of patients with CLI.12–19 This is an interesting aspect given the fact that therapeutic goals differ significantly between these two groups. While limb salvage is the chief objective in patients with CLI, symptom relief is the primary intention in patients with intermittent claudication. As mentioned above, the majority of patients underwent endovascular therapy for pelvic or femoropopliteal disease and infrapopliteal PAD during the same interventional session. This is driven by the fact that in many cases after treatment of a, for example, femoropopliteal lesion or even recanalization of a chronic obstruction, infrapopliteal arterial runoff is crucial regarding the short- and long-term outcome.20,21 Therefore, at our institution, we try to establish a one-, or better two-vessel arterial runoff in the lower limb following endovascular therapy for pelvic or femoropopliteal disease in order to guarantee a good long-term result. Nowadays, endovascular revascularization can be seen as a standard of care for patients with limb-threatening CLI. At the same time, the usefulness of endovascular procedures as a revascularization option for patients with claudication due to isolated infrapopliteal artery disease is unknown, which is reflected by the current ESC and AHA Guidelines.9,10 Our data show that revascularization of infrapopliteal PAD is a safe treatment option accompanied with a promising long-term outcome in both patients with CLI and those with intermittent claudication, femoropopliteal disease, and inadequate arterial runoff. Yet, further research on patients with claudication due to isolated infrapopliteal artery disease is needed to clarify and eventually broaden the indication for revascularization.
Endovascular procedure
The overall technical success rate in the present study was high, irrespective of the lesion morphology and yielded 98.1% for stenotic lesions and 94.7% for chronic total occlusions. Furthermore, the technical success rates were high for all types of TASC lesions. No significant difference regarding the technical success rates was found when comparing moderately complex TASC A and B lesions and more complex TASC C and D lesions (TASC A + B vs TASC C + D; 96.5% vs 96.9%, p = 0.837). This demonstrates the feasibility of the endovascular approach in the hand of experienced vascular specialists and is in line with or even surpasses recently published data.13–18,22 In addition, the overall periprocedural complication rate was low (7.7%) and consisted of minor complications such as vascular access site complications and bleeding requiring blood transfusion. Notably, no major complication (i.e. death or surgical revision) was observed. In other trials evaluating endovascular therapy for infrapopliteal disease, periprocedural complication rates ranged between 7.9% and 11.1%.13,17 In contrast, surgical revascularization using pedal bypass, however, comes along with significantly higher rates of perioperative complications, ranging from 12% to 42%, as shown in numerous previously published studies.23–26 These complications are mostly associated with the surgical procedure itself and general anesthesia (i.e. perioperative death), myocardial infarction, acute respiratory failure or graft/wound infection, and large hematomas needing further treatment.
Interventional strategy
Since the first reports of revascularization of infrapopliteal disease in the early 1990s, there has been a constant evolution of newer technologies and improvement of technology for endovascular treatment of PAD (i.e. wires, balloons, and stents). 27 In the early days, plain balloon angioplasty, with stenting reserved as a bailout technique for dissection, was considered to be the standard strategy. Following the publication of four randomized trials comparing DES to BMS and PTA only, there is now Level I evidence for the implantation for DES in infrapopliteal disease in anatomically suitable lesions (i.e. focal stenoses),14,16,22,28 while plain balloon angioplasty and DEB represent the preferred treatment option for long or distal lesions. At the same time, a randomized trial on DEB for below-the-knee interventions showed a nonsignificant trend toward higher amputation rates in the DEB compared to the PTA group, which led to a broad avoidance of DEB for the treatment of infrapopliteal lesions. 29 This debate was further fueled by a recently published meta-analysis from Katsanos et al. exhibiting a significant increase in mortality in patients treated with paclitaxel-coated balloons and stents, even though the study was limited to femoral and popliteal artery. 30 Taken together, the need for further data and experience is apparent. In our trial, one-quarter of patients were treated with a stent and, of these, 89% were DES. DEBs in our cohort were limited to a small proportion of interventions and even declined over the years as an effect of the crucial IN.PACT DEEP CLI trial mentioned above. 29 Yet, neither uni- nor multivariate analysis identified DES, BMS or DEB as potential predictors for an increase in TLR, possibly demonstrating that the choice of the interventional device is less important compared to the anatomical situation and the complexity of the lesion.
Long-term clinical outcome
For the entire population enrolled, freedom from clinically driven TLR was 88.3% (95% CI: 84.2%–92.4%) at 6 months and 77.2% (95% CI: 70.5–83.9%) at 12 months. These results are promising and compare well with or even excel previously published data showing rates of freedom from TLR ranging from 85% to 96% at 6 months and 66% to 93% at 12 months.14,16,19,22
Furthermore, there was no significant difference in clinically driven TLR between groups of moderate TASC A/B and more complex TASC C/D lesions (TASC A + B vs C + D; 78.5% vs 74.2%, p = 0.457). Still, we observed that freedom from clinically driven TLR was significantly lower in very complex TASC D lesions (TASC A + B + C vs D; 79.7% vs 42.5%, p < 0.001). Singh et al. 13 previously published a clinical trial focusing on comparing the updated TASC II classification against outcomes. In their retrospective analysis of 166 patients, TASC C/D lesions were associated with lower patency rates compared with TASC A/B lesions. In summary, these results show that the updated TASC II classification reflects not only anatomic complexity, but also influences clinical outcomes in patients with infrapopliteal PAD.
Another interesting finding in our analysis was that interventions in the anterior or posterior tibial arteries had a worse outcome compared to lesions of the tibial-peroneal trunk or peroneal artery (p = 0.011). This may suggest the fact that lesions in the tibial-peroneal trunk and peroneal artery are more focal stenoses or occlusions, generally located more proximally, whereas lesions of the tibial arteries are located more distally and therefore tend to come along with a variety of anatomic challenges (smaller vessel diameter, longer lesion length, more chronic occlusions), having a negative effect on the long-term clinical outcome.
Limitations
The current single-center retrospective study had all known limitations of such studies. Follow-up was completed by 79% of patients included in the analysis; consequently, for roughly one-fifth of the population, follow-up data are missing. The outcome in this proportion of patients remains unclear. The outcome in this subgroup may have been worse than in those patients available for follow-up. However, this is a limitation that occurs with the retrospective design of our study.
Conclusions
In this large, single-center, retrospective study, endovascular therapy for infrapopliteal artery disease was safe and accompanied by a promising long-term outcome for all types of lesions, as defined by the updated TASC II classification. These results are consistent with current guideline recommendations supporting the concept of an endovascular-first approach while including anatomically complex lesions. As there is still a lack of prospective randomized trials addressing this issue, observational data currently provide the highest level of evidence available.
Supplemental Material
sj-pdf-1-vmj-10.1177_1358863X20967091 – Supplemental material for Outcomes of endovascular treatment for infrapopliteal peripheral artery disease based on the updated TASC II classification
Supplemental material, sj-pdf-1-vmj-10.1177_1358863X20967091 for Outcomes of endovascular treatment for infrapopliteal peripheral artery disease based on the updated TASC II classification by Arne M Müller, Veronika Räpple, Christian Bradaric, Tobias Koppara, Victoria Kehl, Massimiliano Fusaro, Salvatore Cassese, Ilka Ott, Adnan Kastrati, Karl-Ludwig Laugwitz and Tareq Ibrahim in Vascular Medicine
Footnotes
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Supplementary material
The supplementary material is available online with the article.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.