
Abstract
The association between depression and peripheral artery disease (PAD) outcomes remains widely understudied. In patients with PAD undergoing a peripheral vascular intervention (PVI) who have a recent diagnosis of depression, it is unknown what their long-term outcomes are and what factors may mediate an adverse risk. We therefore studied 797 consecutive patients undergoing PVI across 33 Veterans Affairs (VA) centers. Depression and outcomes were documented from patients’ medical records. Outcomes included: (1) all-cause death; (2) non-fatal cardiovascular events (myocardial infarction, stroke); and (3) PAD-related events (including repeat PVI or amputation). Cox proportional hazards frailty models were constructed, adjusting for age. Additional covariates were selected if they resulted in at least 5% change in the age-adjusted hazard ratio (HR) for depression on outcomes. Overall, 265 (33%) patients had a diagnosis of depression. After a median follow-up of 955 days (range 1–6.25 years), 52 (6.5%) patients died, 30 (3.8%) experienced non-fatal cardiovascular events, and 176 (22.1%) had PAD-related events. Compared to patients without depression, depressed patients had higher rates of non-fatal cardiovascular events (6.4% vs 2.4%, p-value 0.0055). No differences for the other outcomes were noted. Higher risk for non-fatal cardiovascular events persisted after adjustment for age (HR 1.6, 95% CI 1.05–2.47). The only additional covariate that met our selection criteria was hypertension. After adjusting for hypertension, the association between depression and non-fatal cardiovascular outcomes attenuated (HR 1.53, 95% CI 0.99–2.35). In conclusion, a diagnosis of depression in veterans undergoing PVI was associated with increased risk of non-fatal cardiovascular events, mediated by age and hypertension.
Background
In peripheral artery disease (PAD), depression has been identified as an important and prevalent comorbidity that is associated with adverse outcomes including reduced physical functioning, health status, and potentially an adverse cardiovascular prognosis.1–5 About a third of patients with PAD have depressive symptoms.1–5 Having depressive symptoms may be a significant barrier for optimal adherence to the complex and stringent lifestyle regimens in PAD that are key to curbing patients’ cardiovascular risk, and thus contribute to worse health outcomes among this population.
Depression and its impact on overall and cardiac-specific outcomes among patients with PAD is relatively unknown. In addition, it is not entirely clear what the magnitude of risk is associated with an adverse cardiovascular prognosis, and what specific cardiovascular events may explain the association with adverse cardiovascular prognosis. To address these gaps, this study aimed to evaluate the prevalence of depression and its association with long-term cardiovascular prognosis – including death, the occurrence of myocardial infarction or stroke, and repeat peripheral vascular intervention (PVI) or amputation – in a sample of patients with PAD undergoing PVI within Veterans Affairs (VA) facilities. In addition, we aimed to identify potential mediators that explain the association between depression and an adverse long-term cardiovascular prognosis in PAD. Being able to further illuminate the problem of depression, its presentation and association with prognosis will allow us to further prioritize the care that is needed to help support patients with PAD that are dealing with comorbid depression.
Methods
Patients and study design
The study questions were addressed in a retrospective VA peripheral intervention database modeled after the VA CART (Veterans Affairs Clinical Assessment, Reporting, and Tracking) program. The CART program collects patient, medication, and procedural information from medical records related to catheterization procedures taking place within the VA using a standardized electronic data collection infrastructure. 6 Procedural information related to PVI procedures taking place at 33 VA sites from June 15, 2005 to August 20, 2010 were retrospectively abstracted from medical records and recorded. Outcomes data were manually abstracted and entered into purposely designed study case report forms. Outcomes data were ascertained based on the International Classification of Diseases, Ninth Revision (ICD-9) codes, and Current Procedural Terminology (CPT®) codes were used to derive procedural data. Other variables were derived from the VA Corporate Data Warehouse linked with the electronic medical record. Only patients with claudication or critical limb ischemia (rest pain or non-healing wounds) as indications were included.
Institutional review board approval for this study was obtained and a waiver for informed consent was provided since only anonymized data were used for the study.
Measures
Depression was defined as a diagnosis of depression in the 2 years preceding the PVI and was documented from ICD-9 codes recorded in the VA electronic medical records.
Outcomes included days from initial PVI to (1) all-cause death, (2) non-fatal cardiovascular events (myocardial infarction or stroke), and (3) PAD-related events (repeat PVI or amputation). If an event was not observed as of September 30, 2011, the patient was censored. The follow-up time was between 1 and 6.25 years.
Demographics included age, sex, and race; medical history and comorbidity information included tobacco use (ever), family history of coronary artery disease, diabetes, hypertension, hyperlipidemia, history of cardiovascular disease, congestive heart failure, chronic kidney disease, chronic obstructive pulmonary disease, obesity (body mass index (BMI): weight in kilograms divided by height in meters squared ≥ 30), post-traumatic stress disorder, sleep apnea, renal failure, being on dialysis, diastolic and systolic blood pressure, prior percutaneous coronary intervention, prior myocardial infarction, prior coronary artery bypass graft, and prior cardiac transplant.
The indication for the PVI procedure included the following categories: claudication, critical limb ischemia, or rest pain. Other procedural information that was recorded included the use of stents and the number of stents used.
Post-PVI care was captured through the discharge medications (angiotensin-converting enzyme (ACE) inhibitors, angiotensin receptor blockers (ARBs), beta-blockers, calcium channel blockers, nitrates, antiplatelets, statins prescribed within 3 months of PVI discharge), and the number of outpatient visits 1 year post-PVI. The variable for follow-up visits within a year was based on the number of outpatient cardiology visits in the year following the PVI. In cases where death was observed prior to a year, this variable represents less than a full year of observation time.
Depression care was captured through the use of antidepressants upon PVI discharge (serotonin–norepinephrine reuptake inhibitors (SNRIs), selective serotonin reuptake inhibitors (SSRIs)).
Statistical analyses
Patient characteristics were compared by depression history status (yes/no) using chi-squared tests for categorical variables and t-tests for continuous variables (except for follow-up visits at 1 year where a Kruskal–Wallis test was used and for the variable coated sirolimus-eluting stent where a Fisher’s exact test was used due to a small number of expected counts).
Kaplan–Meier plots were constructed to compare the survival curves for each endpoint by depression status. Specifically, comparisons were done for death, myocardial infarction/stroke, and PVI/amputation, and were tested for statistical significance using the log-rank test.
Cox proportional hazards frailty models 7 were constructed for each of the three outcomes to examine the risk associated with depression and subsequent PVI prognosis. Our base model generated an age-adjusted hazard ratio (HR) and 95% CI. The frailty model was used to account for correlation of outcomes within sites.
Given the low number of events in our study cohort, we were restricted in the number of covariates that we could include in the Cox models. Accordingly, we screened for variables in the sequential modeling that could have explanatory value for the association between depression and PVI prognosis. Variables in the Cox models were screened for proportional hazards violations using the cox.zph function in R. 8 In cases where a proportional hazards violation was observed, a time interaction with the variable being assessed was included in the model. Potential mediators were screened by adding them to a base model having age and depression as covariates to determine the percentage change in the HR for depression relative to the base model. A cut-off of 5% in the age-adjusted HR for depression status (i.e. if a covariate explained at least 5%, i.e. when an increase or decrease in the actual HR relative to the base model including only depression and age was observed of at least 5% after introducing the covariate) was used to define which variables were considered potential mediators. This method of selecting candidate explanatory variables is similar to prior work on depression and cardiovascular outcomes. 9
For a given outcome, all variables that exceeded the 5% threshold were included together in a final model. Variables were entered into a final model sequentially in blocks (defined below) to determine their successive impact on the HR for depression. Only variables that surpassed the 5% cut-off were included in a block when added to the final model. If no variables in a given block met the cut-off, then no variables from that block were entered (i.e. the block was skipped and the next block was considered).
The blocks and corresponding variables in the order of entry into the final models (if that block has at least one variable meeting the 5% cut-off) were the following: (1) demographics (age, sex, race); (2) cardiovascular history (prior percutaneous coronary intervention, prior myocardial intervention, prior coronary artery bypass graft, congestive heart failure, history of cardiovascular disease, history of cardiac transplant); (3) comorbid conditions (diabetes, chronic obstructive pulmonary lung disease, chronic kidney disease); (4) other risk factors (obesity, hypertension, hyperlipidemia, sleep apnea); (5) frequency of follow-up visits; (6) discharge medications (statins, antiplatelet medications); and (7) smoking status. For the Cox proportional hazards models, the number of follow-up visits was treated as a time varying covariate (i.e. the number of follow-up visits was changeable and was incremented at each unique visit date up to a year, unless an event happened prior to a year).
Statistical analyses were conducted with SAS 9.3 for Windows (SAS Institute, Cary, NC, USA). All tests were two-tailed and were considered statistically significant at the < 0.05 level.
Results
Our cohort consisted of 797 PVI patients: 786 (98.6%) were male, with a mean age of 65.1±8.9 years. A total of 265 (33.2%) patients had a history of depression prior to PVI. As compared with those who did not have a history of depression, patients known to have depression were more likely to be younger, be smoking, have higher rates of cardiovascular risk factors, including a more extensive cardiovascular history (such as a history of myocardial infarction and having undergone percutaneous coronary interventions or a coronary artery bypass graft), and they were more often taking antidepressants (Table 1). Patients with depression also more often had other comorbidities, including chronic obstructive pulmonary disease, being obese, a history of post-traumatic stress disorder, and sleep apnea. There were no differences in the indications for undergoing PVI or the cardiovascular medications received as a function of depression status. Depressed patients did, however, receive more care, as quantified by the number of cardiology outpatient follow-up visits after their PVI, compared with patients who did not have a history of depression.
Patient characteristics for the overall cohort and by depression status.
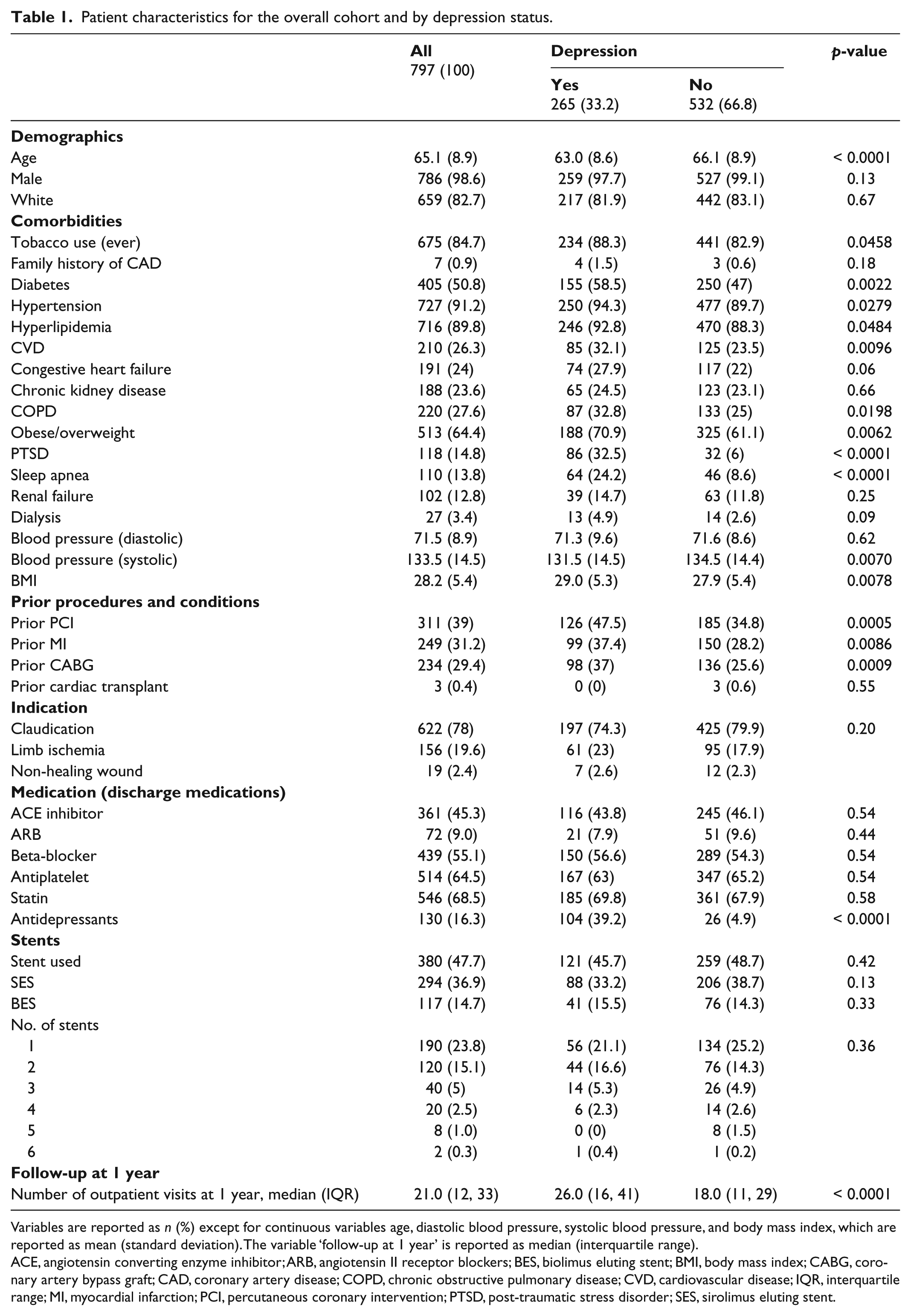
Variables are reported as n (%) except for continuous variables age, diastolic blood pressure, systolic blood pressure, and body mass index, which are reported as mean (standard deviation). The variable ‘follow-up at 1 year’ is reported as median (interquartile range).
ACE, angiotensin converting enzyme inhibitor; ARB, angiotensin II receptor blockers; BES, biolimus eluting stent; BMI, body mass index; CABG, coronary artery bypass graft; CAD, coronary artery disease; COPD, chronic obstructive pulmonary disease; CVD, cardiovascular disease; IQR, interquartile range; MI, myocardial infarction; PCI, percutaneous coronary intervention; PTSD, post-traumatic stress disorder; SES, sirolimus eluting stent.
The crude 1-year event rates for the overall population under study and by depression status is reported in Table 2. The follow-up time ranged from 1 to 6.25 years (median follow-up 955 days); an overall death rate of 6.5% (n=52) was noted and a rate of 3.8% (n=30) and 22.1% (n=176) was observed for the non-fatal cardiovascular and PAD-related event rates, respectively. Patients with known depression had a higher event rate for the endpoint myocardial infarction/stroke (6.4% vs 2.4%, p-value log-rank test=0.0055). There were no differences noted by depression status for the endpoints death and PAD-related events. The survival curves for the association between depression status and the three endpoints are depicted in Figures 1a–c. As only the univariable comparison between depression status and the endpoint myocardial infarction/stroke was statistically significant, we continued building our multivariable model only for that outcome in our main analyses.
Crude event rates at 1 year for the overall sample, and by depression status.
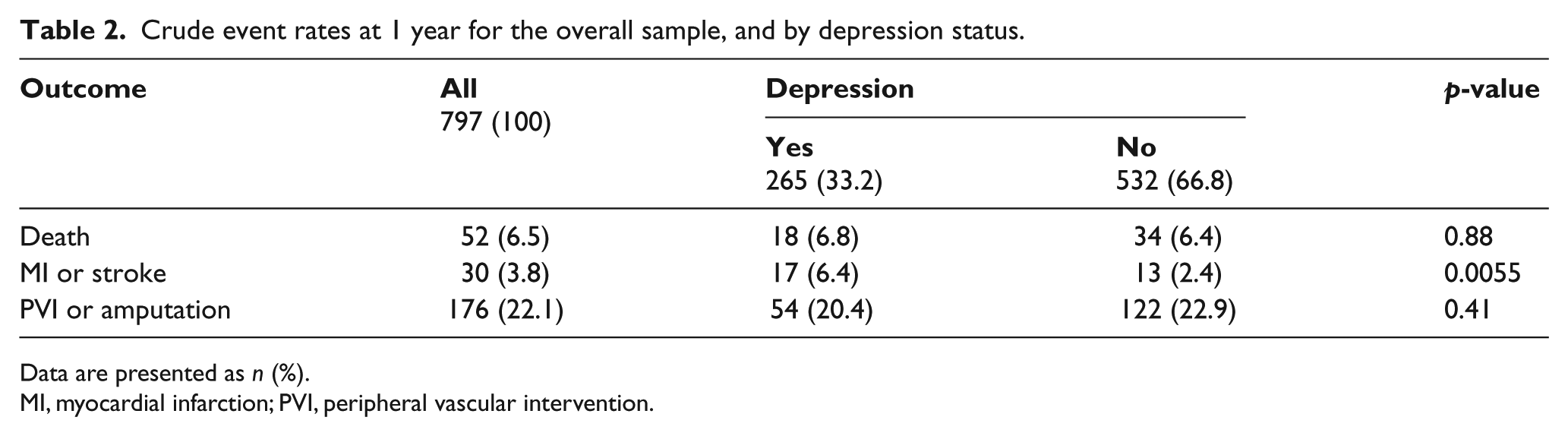
Data are presented as n (%).
MI, myocardial infarction; PVI, peripheral vascular intervention.
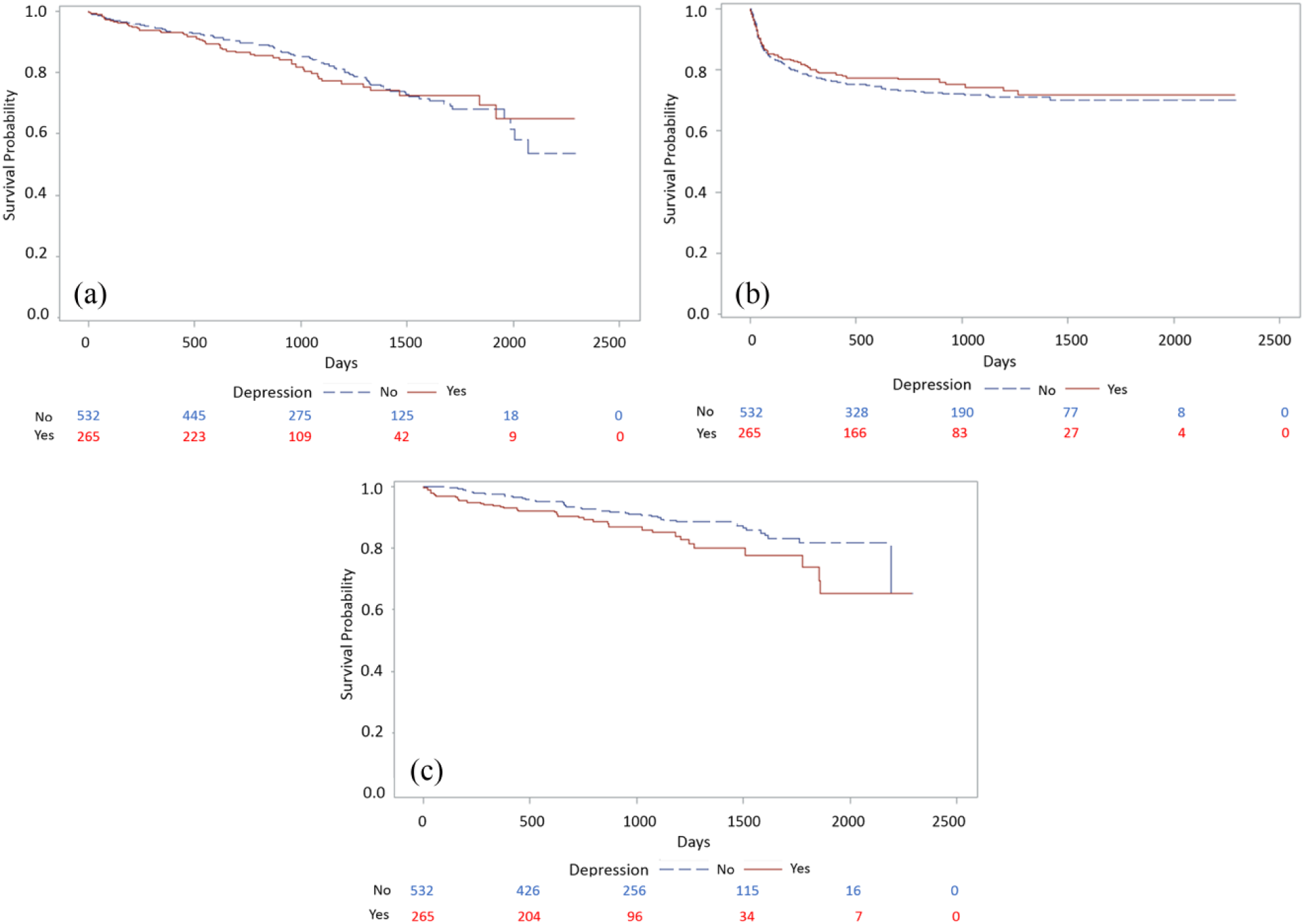
Kaplan–Meier survival plots for the outcomes (a) death; (b) repeat PVI/amputation; and (c) myocardial infarction/stroke. Two groups are compared: patients with known depression versus those without depression.
Only one variable (hypertension) had a change in HR from the base model that was greater than 5%. As a result, the final model consisted of age, depression status and hypertension. The HR associated with depression status in the base model was 1.61 (95% CI 1.05–2.47); following adjustment for the risk factor hypertension, the association between depression status and non-fatal cardiovascular events (HR=1.53, 95% CI 0.99–2.35) was no longer statistically significant. The complete overview of the percentage change in HR from the base model for each endpoint is provided in Supplemental Material Table 1. An overview of the final models with the potential mediators included for the outcome death and PAD-related events is also provided in the Supplemental Material (Table 2).
Discussion
In a US veterans sample, we found that approximately one-third of patients undergoing PVI had a recent diagnosis of depression, which was independently associated with a 60% increased risk of experiencing a myocardial infarction or stroke in the 5 years following their PVI. The association was no longer significant after adjusting for age and hypertension.
Patients with PAD have been previously found to be at risk of experiencing depressive symptoms,1–5,10–12 but rarely has there been such long-term follow-up available looking at specific outcomes and potential factors explaining their association. While we confirmed that about one-third of patients with PAD may be dealing with depression within the 2 years prior and at the time of their procedure, this study provides unique insight into the impact of depression on health outcomes in patients with PAD. Whereas the association between depression and cardiovascular outcomes has been extensively studied and established in patients with coronary disease, in PAD we are just beginning to understand what implications a diagnosis of depression has for the management of PAD, as well as for the outcomes of PAD. It is important to study these associations in various samples of patients with PAD, rather than to extend the findings from patients with coronary disease to patients with PAD.
It is therefore interesting that we only observed a clear relationship between depression and non-fatal cardiovascular events, including myocardial infarction or stroke. By also systematically evaluating potential mediators, we found that after introducing the risk factor hypertension in our analysis, the association between depression and non-fatal cardiovascular events attenuated. In coronary artery disease, most of the observed associations between depression and cardiovascular outcomes persisted following adjustment of clinical factors such as hypertension.9,13,14 This new information will need further confirmation in larger, more representative cohorts of PAD to see whether our findings can be replicated and further actionable implications may be derived for this vulnerable population.
Hypertension has been identified as one of the established risk factors in PAD 15 and has also been identified as a potential mechanism for the association between depression and cardiovascular disease, including the coronary arteries, but potentially also for the peripheral arteries. 16 Stress and depression may trigger a cascade of hemodynamic changes, including higher sympathetic tone, increasing levels of noradrenaline, and increased vasoconstriction, as well as elevation in systemic arterial pressure. 16 Although hypertension is a modifiable risk factor, the treatment of hypertension in PAD is not as prominently targeted as one of the metrics that define high-quality PAD management, although one can argue that hypertension as a diagnosis warrants treatment in itself to manage cardiovascular risk. 17
As with hypertension, depression is also a modifiable risk factor for which there have been no systematic recommendations or quality of care metrics defined 17 that would allow for a better identification and management of the condition in this population at risk. As a reference, the estimated history rates for a major depressive disorder are 11.7% in women and 5.6% in men of the general population. 18 The numbers that we have seen in this PVI cohort are many times higher than those observed in the general population and call for an increased awareness of this problem in patients with PAD. Detection of depressive symptoms through standardized instruments, such as those used in coronary populations (e.g. the Patient Health Questionnaire 19 ), and facilitating access to depression care would be two key components to improve the quality of care towards patients with PAD who are dealing with comorbid depression (e.g. through patients’ primary care network). Screening for depression in the general population and in patients with a chronic disease are now supported and recommended by the US Preventive Services Task Force. 20
Limitations
The current study should be interpreted against the following limitations. A retrospective design prevented us from doing a more precise case identification of depression and residual confounding; for example, the level of functional limitations overlapping with depressive symptoms should also be taken into account. Furthermore, we were not able to study a dose–response relationship between depressive symptoms and PAD outcomes, as we were not able to measure depressive symptoms through a standardized instrument. Our observations will need to be replicated in a larger prospective cohort to further address confounding and power issues (i.e. limited event rates) to which this study was subject to. Also, the causal pathways of the associations between depression, hypertension, and subsequent cardiovascular prognosis cannot be derived from our findings. Lastly, our cohort was predominantly male and recruited from a VA setting. Therefore, we did not have a chance to further investigate meaningful sex interactions 10 in the association between depression and PAD outcomes. A mostly male population and variability in the number of recruited patients across participating centers may pose limitations to the wider generalizability of our findings. Therefore, further replication is warranted in more representative PAD cohorts.
Conclusion
In conclusion, the history of depression burden for patients with PAD is large and associated with an increased risk of experiencing a stroke or myocardial infarction following PVI, potentially mediated by age and hypertension. Both depression and hypertension are modifiable factors, and represent important areas to further improve the quality of care and outcomes in patients with PAD.
Supplementary Material
Supplementary_material, VMJ770275_Supplementary_Material – Depression and long-term prognostic outcomes following peripheral endovascular interventions in the VA Healthcare System
Supplementary_material, VMJ770275_Supplementary_Material for Depression and long-term prognostic outcomes following peripheral endovascular interventions in the VA Healthcare System by Kim G Smolderen, Mary E Plomondon, Ehrin J Armstrong, Edward Hess, Stephen Waldo, Thomas T Tsai and Thomas M Maddox in Vascular Medicine
Footnotes
Acknowledgements
We would like to thank Philip Dattilo, MD (University of Colorado, Denver) for data collection support.
Dr. Bruce Gray served as guest editor for this manuscript.
Declaration of conflicting interests
The authors declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: Dr Smolderen receives research support from Boston Scientific, Abbott, and Merck Pharmaceuticals. Dr Waldo receives research support to the Denver Research Institute from Abiomed, Cardiovascular Systems Incorporated, and Merck Pharmaceuticals.
Funding
The authors disclosed no financial support for the research, authorship, and/or publication of this article.
Supplementary material
The supplementary material is available online with the article.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.