
Abstract
The purpose of the current study was to investigate the association between bone mineral density (BMD) scores and the prevalence of peripheral artery disease (PAD) in a large cohort of subjects who underwent arterial Doppler assessments and calcaneal bone densitometry. The study was performed using data obtained from Life Line Screening Inc. Subjects were self-selected and paid for screening tests. The prevalence of PAD was significantly higher in men with osteopenia (4.5%) and osteoporosis (10.9%) compared to men with normal BMD (3.0%) (p<0.001). Osteopenia (odds ratio (OR) 1.3) and osteoporosis (OR 2.3) were found to be independent risk factors for the presence of PAD in men. The prevalence of PAD was significantly higher in women with osteopenia (4.8%) and osteoporosis (11.8%) compared to women with normal BMD (3.3%) (p<0.001). Osteopenia (OR 1.15) and osteoporosis (OR 1.8) were found to be independent risk factors for the presence of PAD in women. The current study reports a strong association of abnormal BMD analysis with the prevalence of PAD, which persists even when controlling for age and associated atherosclerotic risk factors. Although the mechanism by which these two disease processes is related is not completely elucidated, the presence of osteoporosis should make clinicians aware of the possibility of occult PAD or associated atherosclerotic disease in appropriate patients.
Introduction
Atherosclerosis and osteoporosis are prevalent disease processes that lead to significant morbidity and mortality worldwide. Peripheral artery disease (PAD) affects 3–10% of the population, which is escalated to 15–20% in persons older than 70 years. 1 Low bone mass affects 54 million Americans and results in over two million fractures annually.2,3 Complications of atherosclerosis include myocardial infarction, stroke, death, and limb loss. Osteoporosis-related fractures are associated with a high mortality rate and significant economic burden.2,4 While osteoporosis is known to be more common in women, men are at a higher risk for fracture-related death. Although men have a higher incidence of PAD, women are more likely to die from complications of atherosclerosis. 5 Both diseases have similar risk factors, including advanced age, diabetes, hypertension, dyslipidemia, sedentary lifestyle, and genetic predisposition.6,7
Vascular calcification and bone mineral loss were previously attributed to age-related changes, although recent studies suggest an association beyond the aging process itself.5,8–11 Recent studies have also shown that these disease processes may share a similar etiology at the molecular level.7,12,13 For example, both atherosclerosis and osteoporosis have been linked to estrogen deficiency, vitamin D receptor polymorphisms, vitamin K deficiency, lipid oxidation, inflammation, and hyperhomocysteinemia.6,7 Furthermore, specific cells, proteins, and cytokines that are involved in osteogenesis have also been found in calcified arterial plaques, further implicating similar pathophysiology in the development of these two disease states. 14
Studies have previously shown that a greater magnitude of bone loss is associated with a greater amount of vascular calcification. 10 A correlation, in certain populations, has been found between osteoporosis and carotid artery disease, large artery calcification, PAD, stroke, and all-cause mortality. 10 In addition, low bone mineral density (BMD) has been identified as an independent predictor of cardiovascular mortality, and osteoporosis and related fractures are more common in patients with cardiovascular disease. 15 Although PAD is a known predictor of coronary artery disease (CAD), the association between PAD and osteoporosis has been studied much less frequently and has been exhibited mostly in women in small, specific study populations. The aim of this study was to investigate whether a decreased BMD is predictive of the prevalence of PAD, and whether this association is independent of age and common risk factors.
Methods
Study population
The study was performed using data obtained from the Life Line Screening Inc. Database (LLS, Independence, OH, USA), a provider of community based preventative health screenings. Data and informed consent for research were collected in a standardized method by this organization. The Life Line Screening Inc. provided the data to the Society for Vascular Surgery (SVS) for research purposes, allowing this study to be performed without requiring Institutional Review Board approval. The data were provided without any financial consideration or editorial control over analysis or publication. The cohort consisted of self-referred subjects who voluntarily paid for vascular screening between 2003 and 2008 at over 20,000 sites. Individuals completed a questionnaire reporting on clinical characteristics and demographics, including cardiovascular risk factors, family history and other comorbidities. All demographic information was self-reported and not verified by a physician. A history of hypertension, diabetes, or hyperlipidemia was determined by a prior physician diagnosis or medication use. A smoking history was considered significant if subjects reported smoking 100 cigarettes or more. Subjects of all ages were included in the study. 16
Ascertainment of BMD and PAD
Ankle–brachial indices (ABI) were measured to evaluate for PAD and bone densitometry was performed to evaluate for evidence of bone mineral loss. To determine ABI, systolic blood pressure measurements were taken from bilateral brachial and posterior tibial (PT) arteries. The dorsalis pedis (DP) artery pressure was used if a PT signal was not audible. The ankle systolic pressure was divided by the higher of the two brachial artery systolic pressures to obtain an ABI. PAD was diagnosed when one or both legs had an ABI of ⩽0.9. 17 T-scores were calculated using ultrasound bone densitometry. A portable ultrasound densitometer was used to evaluate BMD of the calcaneus. A normal T-score was defined as −1.0 or higher, osteopenia was defined by a T-score between −1.0 and −2.5, and osteoporosis was indicated by a T-score of −2.5 or lower. Carotid artery stenosis (CAS) (⩾50%) was determined by duplex ultrasound (peak systolic velocity (PSV) ⩾125 cm/s). Abdominal aortic aneurysm (AAA) was determined by the greater of the anteroposterior or transverse measurements of the infra-renal abdominal aorta on ultrasound. AAA was defined as having an infra-renal abdominal aortic diameter ⩾3 cm.
Statistical analysis
The prevalence of subject demographics and comorbidities, including smoking, hypertension, hyperlipidemia, prior myocardial infarct, AAA, CAS, diabetes and PAD, were reported in percentages. Comparisons of these factors in patients with normal BMD, osteopenia, and osteoporosis were examined by performing a χ2 test.
Logistic regression was performed to determine the association between PAD and BMD. Odds ratio (OR) and the 95% confidence interval (CI) were calculated to determine the risk of PAD in the group of subjects with normal BMD, osteopenia, and osteoporosis. Furthermore, multiple logistic regression analysis was performed controlling for age, smoking, diabetes mellitus, hypertension, and hypercholesterolemia. Subjects older than 50 years were compared to a control group of patients aged 40–50 years to determine the OR for having PAD in each subsequent age decile (see Table 3). All subjects were included in this analysis. The OR of PAD in subjects with normal BMD, osteopenia, and osteoporosis was determined for each age decile: 40–50, 51–60, 61–70, 71–80, 81–90 (Figures 1 and 2). Subjects older than 90 years of age were excluded in this analysis.
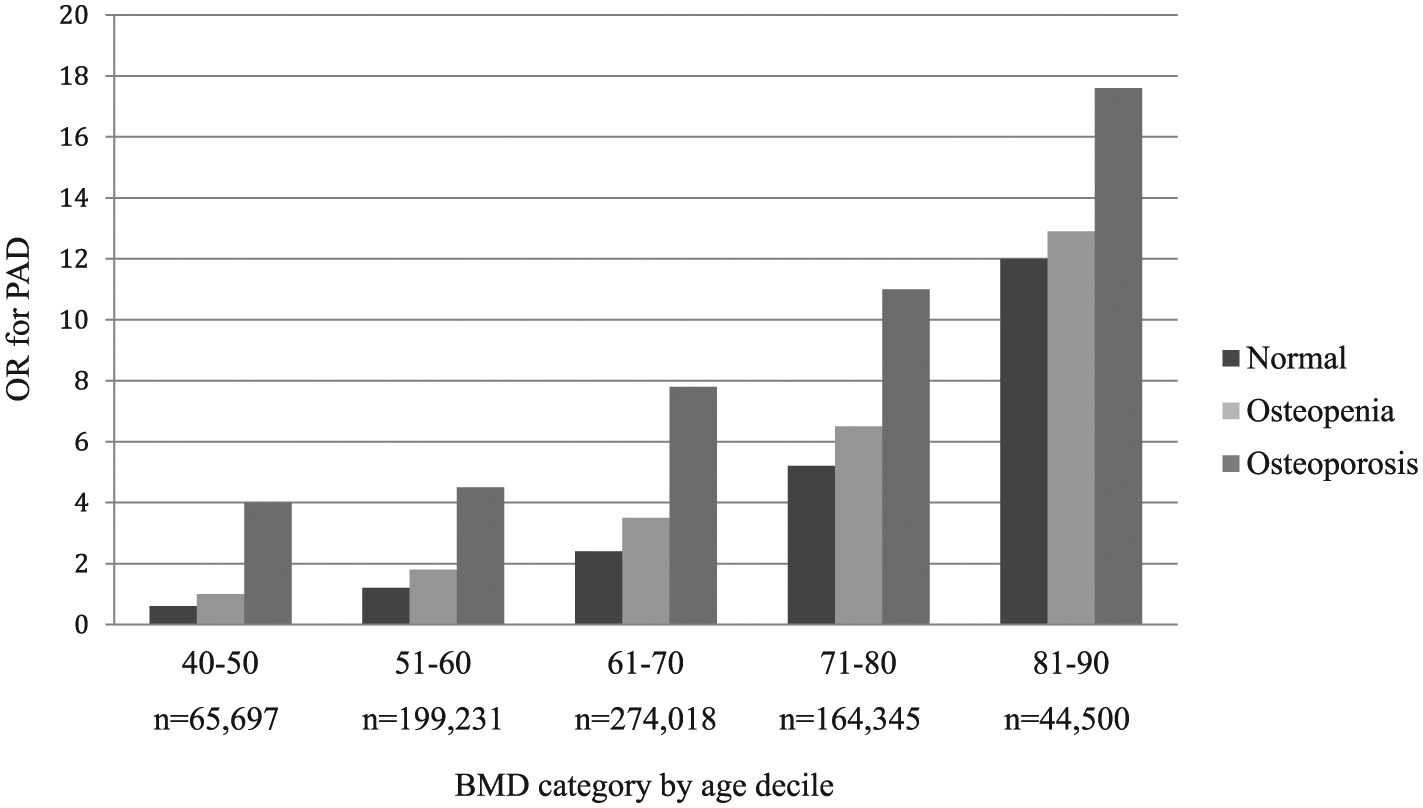
The odds ratio (OR) for peripheral artery disease (PAD) in men with osteopenia and osteoporosis compared to men with a normal bone mineral density (BMD) within the same age decile. In predicting the OR for PAD in men, the standard error (SE) = 0.014 for subjects with osteopenia and the SE = 0.038 for subjects with osteoporosis.
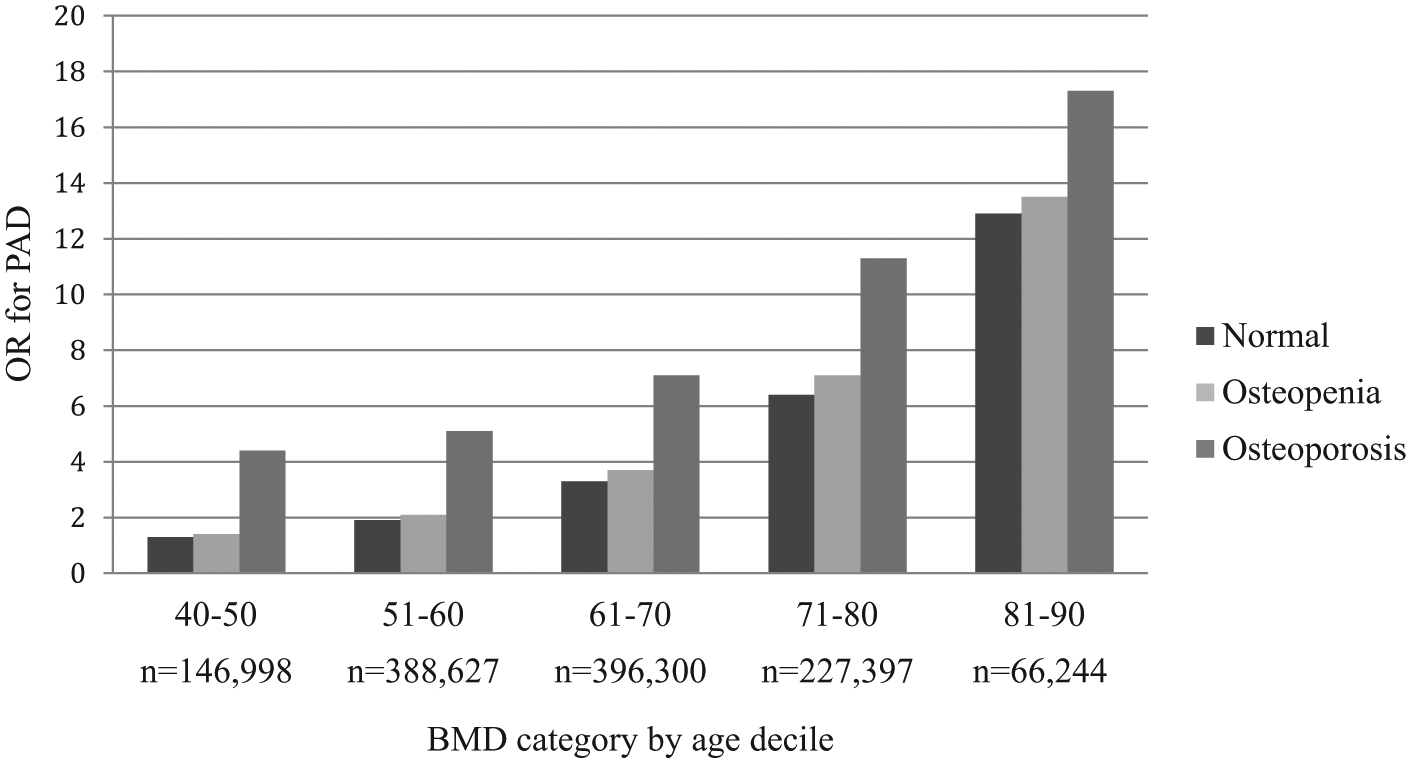
The odds ratio (OR) for peripheral artery disease (PAD) in women with osteopenia and osteoporosis compared to women with a normal bone mineral density (BMD) within the same age decile. In predicting the OR for PAD in women, the standard error (SE) = 0.01 for subjects with osteopenia and the SE = 0.02 for subjects with osteoporosis.
Results
Population characteristics
A total of 2,023,081 subjects, including 766,172 (38%) men and 1,256,909 (62%) women, were included in the study. Subject demographics are outlined in Table 1 and Table 2. Subjects of all ages were included in the study. Only subjects aged 40–99 years were included in the logistic regression analysis. When separated by age groups 40–50, 51–60, 61–70, 71–80, 81–90, and 91–100, there were 65,697, 199,231, 274,018, 164,345, 44,500, and 2241 men (n = 750,032) and 146,998, 388,627, 396,300, 227,397, 66,244, and 3593 women (n = 1,229,159), respectively.
Demographics and clinical characteristics of men by bone mineral density (BMD) category.
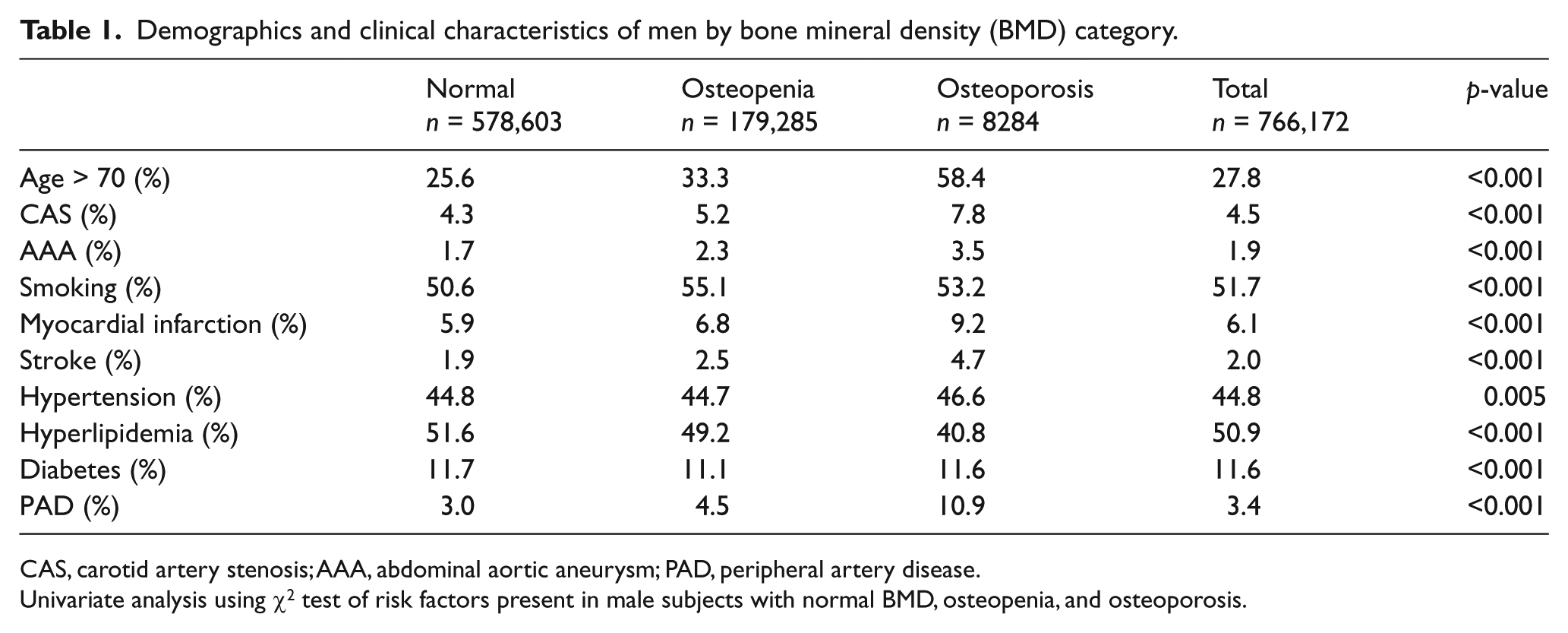
CAS, carotid artery stenosis; AAA, abdominal aortic aneurysm; PAD, peripheral artery disease.
Univariate analysis using χ2 test of risk factors present in male subjects with normal BMD, osteopenia, and osteoporosis.
Demographics and clinical characteristics of women by bone mineral density (BMD) category.
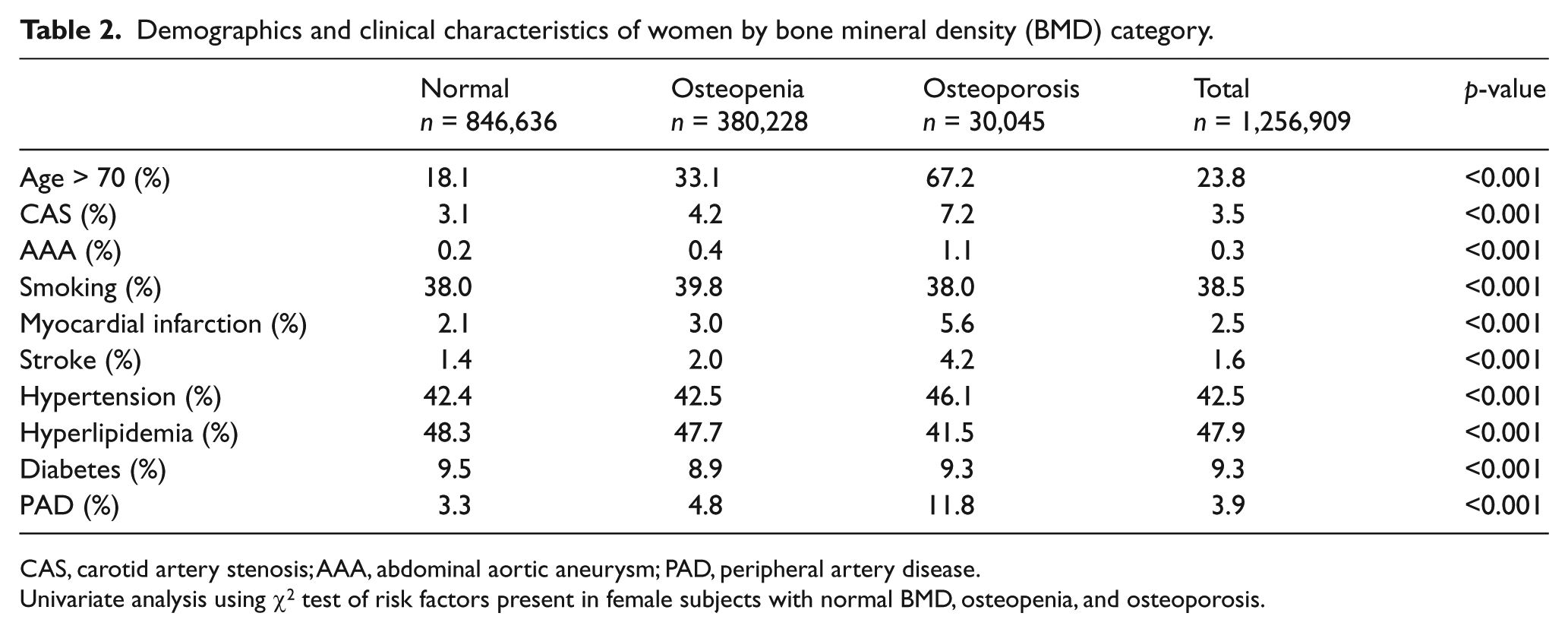
CAS, carotid artery stenosis; AAA, abdominal aortic aneurysm; PAD, peripheral artery disease.
Univariate analysis using χ2 test of risk factors present in female subjects with normal BMD, osteopenia, and osteoporosis.
Male subject characteristics
Peripheral artery disease was reported in 3.4% (26,039) of all male subjects. Osteopenia was reported in 23.4% (179,285) and osteoporosis was reported in 1.1% (8284) of 766,172 total male subjects. The largest group of men with normal BMD (36.4%) and osteopenia (35.4%) were in the age group 61–70 years. The largest group of men with osteoporosis (33.6%) was in the 71–80 age group. Moderate to severe CAS was seen in 4.3% of men with normal BMD, 5.2% of those with osteopenia, and 7.8% of those with osteoporosis (p<0.001). A history of AAA was found in 1.7% of men with normal BMD, 2.3% with osteopenia, and 3.5% with osteoporosis (p<0.001). A smoking history was reported in 50.6% of men with normal BMD, 55.1% with osteopenia, and 53.2% with osteoporosis (p<0.001). A prior heart attack was reported in 5.9% of men with normal BMD, 6.8% with osteopenia, and 9.2% with osteoporosis (p<0.001). Prior stroke was reported in 1.9% of men with normal BMD, 2.5% with osteopenia, and 4.7% with osteoporosis (p<0.001). Hypertension was noted in 44.8% of men with normal BMD, 44.7% with osteopenia, and 46.6% with osteoporosis (p=0.005). High cholesterol was seen in 51.6% of men with normal BMD, 49.2% with osteopenia, and 40.8% with osteoporosis (p<0.001). Diabetes was reported in 11.7%, 11.1%, and 11.6% of men with normal BMD, osteopenia, and osteoporosis, respectively (p<0.001).
Female subject characteristics
Peripheral artery disease was reported in 3.9% (49,624) of all female subjects. Osteopenia was reported in 30.3% (380,228) and osteoporosis was reported in 2.4% (30,045) of 1,256,909 female subjects. The largest age group of women with normal BMD (34.1%) was 51–60 years, the largest group with osteopenia (32.8%) was 61–70 years, and the largest group with osteoporosis (36.7%) was 71–80 years. Carotid artery stenosis was reported in 3.1% of women with normal BMD, 4.2% of women with osteopenia, and 7.2% of women with osteoporosis (p<0.001). AAA was found in 0.2% of women with normal BMD, 0.4% with osteopenia, and 1.1% with osteoporosis (p<0.001). A smoking history was reported in 38% of women with normal BMD, 39.8% with osteopenia, and 38% with osteoporosis (p<0.001). A prior heart attack was reported in 2.1% of women with normal BMD, 3.0% with osteopenia, and 5.6% with osteoporosis (p<0.001). Prior stroke was reported in 1.4% of women with normal BMD, 2.0% with osteopenia, and 4.2% with osteoporosis (p<0.001). Hypertension was noted in 42.4% of women with normal BMD, 42.5% with osteopenia, and 46.1% with osteoporosis (p<0.001). High cholesterol was seen in 48.3% of women with normal BMD, 47.7% with osteopenia, and 41.5% with osteoporosis (p<0.001). Diabetes was reported in 9.5%, 8.9%, and 9.3% of women with normal BMD, osteopenia, and osteoporosis, respectively (p<0.001).
Results in male subjects
Based upon BMD scores, osteopenia was diagnosed in 23.4% of men and osteoporosis was diagnosed in 1.1% of men. Men with abnormal T-scores did not have a markedly different risk factor profile than men with normal T-scores, but those with abnormal T-scores were older and had a higher rate of CAS, AAA, and prior stroke and myocardial infarction (Table 1). The prevalence of PAD was significantly higher in men with osteopenia (4.5%) and osteoporosis (10.9%) than in men with normal BMD (3.0%) (p<0.001).
Results in female subjects
Based upon BMD scores, osteopenia was diagnosed in 30.3% of women and osteoporosis was diagnosed in 2.4% of women. Women with abnormal T-scores did not have markedly different risk factor profiles from women with normal T-scores, although women with abnormal T-scores were older and had a higher prevalence of CAS, AAA, and prior stroke and myocardial infarction (Table 2). The prevalence of PAD was significantly higher in women with osteopenia (4.8%) and osteoporosis (11.8%) compared to women with normal T-scores (3.3%) (p<0.001).
Multivariate results in male subjects
Logistic regression analysis was performed for men aged 40–99 years, which included 750,032 men. Logistic regression controlling for age and risk factors revealed both osteopenia (OR 1.3, 95% CI 1.27–1.35, p<0.001) and osteoporosis (OR 2.3, 95% CI 2.14–2.49, p<0.001) to be independently associated with the presence of PAD in men (Table 3). When patients were stratified by age, it was noted that men older than 50 years with osteoporosis had a significantly increased prevalence of PAD compared to the 40–50 years subject group, and there was a positive linear correlation between the prevalence of osteoporosis and PAD with increasing age (Figure 1). Male subjects with osteoporosis had an increased prevalence of PAD compared to male subjects with osteopenia.
Logistic regression analysis for the prevalence of peripheral artery disease (PAD) in men and women.
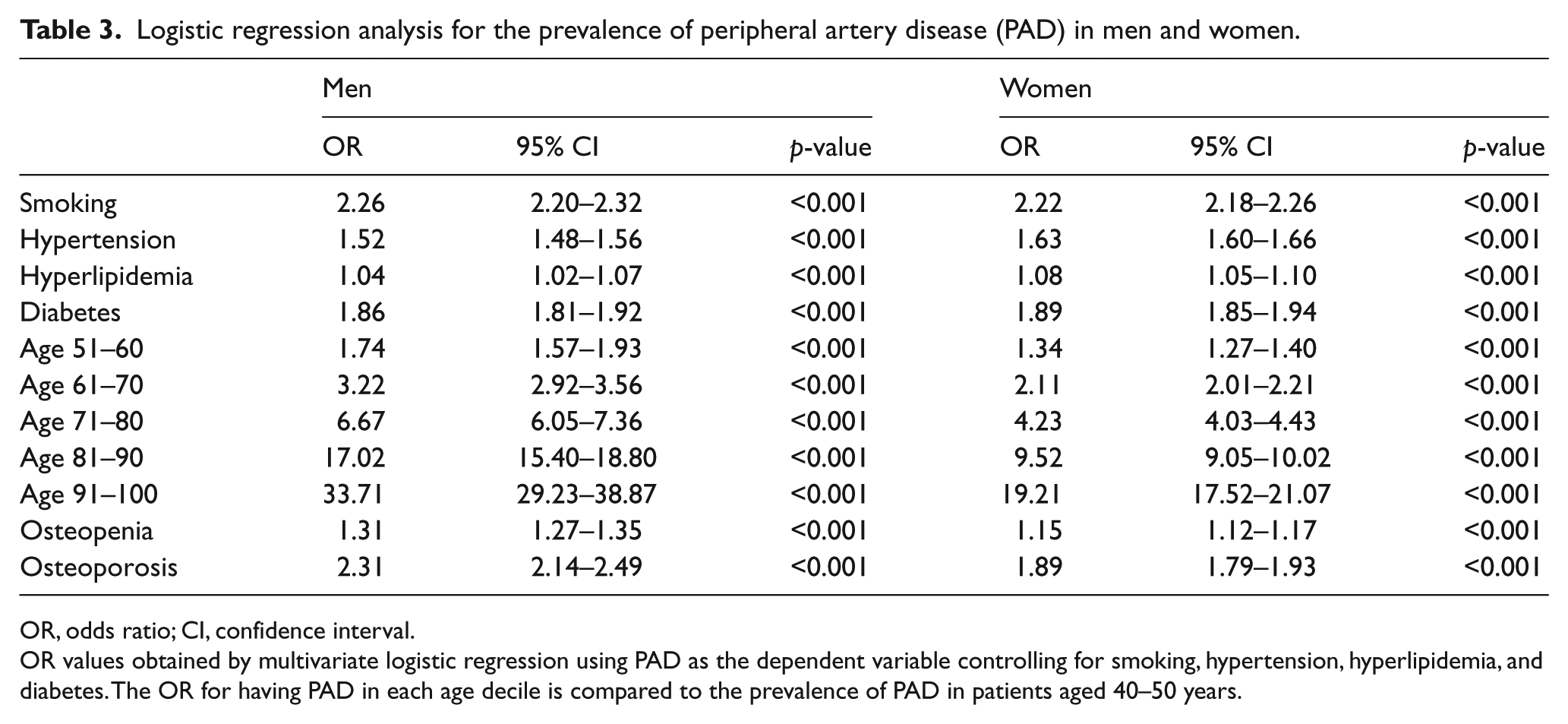
OR, odds ratio; CI, confidence interval.
OR values obtained by multivariate logistic regression using PAD as the dependent variable controlling for smoking, hypertension, hyperlipidemia, and diabetes. The OR for having PAD in each age decile is compared to the prevalence of PAD in patients aged 40–50 years.
Multivariate results in female subjects
Logistic regression analysis was performed for women aged 40–99 years, which included 1,229,159 women. Logistic regression revealed both osteopenia (OR 1.15, 95% CI 1.12–1.17, p<0.001) and osteoporosis (OR 1.89, 95% CI 1.79–1.93, p<0.001) to be independently associated with the presence of PAD in women (Table 3). When patients were stratified by age, it was noted that women older than 50 years with osteoporosis had a significantly increased prevalence of PAD compared to the 40–50 years subject group, and there was a positive linear correlation between the prevalence of osteoporosis and PAD with increasing age (Figure 2). Female subjects with osteoporosis had an increased prevalence of PAD compared to female subjects with osteopenia.
Discussion
In this study, we investigated the relationship between osteoporosis and PAD in a large cohort who underwent screening for PAD and bone densitometry. To our knowledge this is the largest study investigating the association between PAD and osteoporosis performed to date. The major findings of this study are: (1) subjects with osteoporosis had an almost twofold increased risk of concomitant PAD compared to patients with normal BMD; (2) this relationship persisted after controlling for known risk factors; (3) there was a graded response for the prevalence of PAD with decreased BMD; and (4) when subjects were stratified by age, the association between PAD and osteoporosis was evident in each age group. These findings suggest that an association exists between atherosclerosis and osteoporosis independent of shared risk factors and independent of the aging process.
Previous studies have suggested a relationship between PAD and osteoporosis, although the exact nature of this association is difficult to interpret given the variability in methods used to assess for osteoporosis and PAD. In a study by Mangiafico et al., the prevalence of PAD, defined as an ABI ⩽0.9, was 18.2% in 345 women with osteoporosis at the femoral neck and 3.8% in 360 women with normal BMD. 18 Wang et al. studied 2487 healthy men and women in a Chinese population and found a low BMD was associated with increased brachial–ankle pulse wave velocity. This association was stronger in postmenopausal women, although no significant association was seen when using ABI. 19 The Rancho Bernardo study, a prospective study established in 1972, found that women with PAD determined by ABI were more likely to have osteoporosis, measured by dual-energy X-ray absorptiometry (DXA) at the hip and lumbar spine, compared to women without PAD; however, this was not independent of age, and these findings were not seen in men. 15 In another study by Vogt et al., ABI was positively correlated with BMD at the hip (correlation coefficient 0.074), calcaneus (0.064), and proximal (0.060) and distal radius (0.070) in 1292 women when adjusting for age. Importantly, the correlation was positive regardless of the location at which BMD was measured. 20 While BMD in our study was measured with calcaneal ultrasound densitometry, it is not the current standard for ascertaining BMD. Studies show that BMD measured at the calcaneus may correlate with central BMD measurements, but may be more sensitive with an adjusted T-score cut-off. 21 Most of the studies looking at PAD and BMD were performed in relatively small and single ethnicity populations, included predominantly female subjects, and did not consistently control for confounding variables. Hyder et al., in 2009, studied a large multiethnic population and found an association between lower volumetric trabecular BMD of the lumbar spine and increased coronary and abdominal aortic calcium by quantitative computed tomography. 22
While there is a paucity of data evaluating the relationship between PAD and osteoporosis, studies have demonstrated an association between the development of CAD and osteoporosis, particularly in postmenopausal women.23–26 A recent study by Seo et al. showed that postmenopausal women with decreased BMD at the lumbar spine or femoral neck had a 2.86- and 3.35-fold risk, respectively, of having CAD after controlling for risk factors, including age. 27 The Rotterdam study, a prospective cohort study initiated in 1990, found that BMD loss at the femoral neck was associated with increased coronary artery calcification in women with lower estradiol levels. 11 Additionally, Marcovitz et al. demonstrated an OR of 5.6 for predicting CAD by coronary angiography in men with osteoporosis, illustrating an association between CAD and osteoporosis in both sexes.24,28 This further supports an association between osteoporosis and atherosclerotic disease in variable vascular beds.
The association between atherosclerosis and osteoporosis at the population level suggests a similar etiology at the molecular level. It has been hypothesized that low BMD is a form of vascular disease of the bones, and studies have shown that diminished bone perfusion on magnetic resonance imaging (MRI) is related to higher carotid atherosclerosis, lower BMD, and high bone matrix fat. 29 The processes of bone mineralization and atherosclerotic plaque formation both involve hydroxyapatite crystallization. 30 In addition, similar signaling molecules, such as gamma-carboxyglutamate, osteopontin, and BMP-2, have been observed in calcified arterial walls and bone matrix. 31 Furthermore, osteopontin, a glycoprotein in bone matrix, is present in higher levels in the serum and plaques of patients with CAD, and osteoprotegerin, a marker of bone remodeling, is present in smooth muscle cells of arteries.6,32 This hypothesis is demonstrated in the Tromsø study by Jorgensen et al., where a significant inverse correlation between BMD and carotid artery plaque echogenicity was seen, indicating that low bone mass is associated with an increased risk of echogenic-calcified atherosclerotic plaques. 33
Both osteoporosis and atherosclerosis have been linked to an overall inflammatory state, leading to hardening of soft tissues, including arteries, and softening of hard tissues, such as bone. 34 Markers of inflammation, such as C-reactive protein (CRP), tumor necrosis factor alpha (TNF-α), and interleukin-6 (IL-6), have been found to be more prevalent in the circulation of subjects with atherosclerosis and osteoporosis, and these markers have been associated with increased cardiovascular mortality and bone resorption. 35
Atherosclerosis and osteoporosis have both been shown to be inducible in atherosclerosis-prone mice subject to a high-fat diet. In addition, low density lipoprotein (LDL) has been shown to inhibit osteoblast differentiation and increase calcification of smooth muscle cells. 36
It has been well-demonstrated that women have a higher risk of both osteoporosis and cardiovascular disease after menopause. 37 This risk is linked to a decrease in endogenous estrogen, leading to increased parathyroid hormone (PTH) levels, which stimulate bone loss and subsequent soft tissue, including arterial calcification.38,39 Both estrogen and vitamin D receptors are found in vascular endothelial and smooth muscle cells.40,41 Additionally, studies have determined that a specific BSmI polymorphism of the vitamin D receptor gene is associated with low BMD, and may be more frequent in patients with CAD.6,42
The effects of statins in osteoporosis and bisphosphonates in atherosclerosis have been studied to determine if the benefits of these drugs cross over to both disease processes. 14 Statins, which inhibit the HMG-CoA reductase activity, are anti-inflammatory, decrease LDL in the circulation, and improve endothelial function in arteries. This class of drugs has also been shown to increase BMP-2 and osteoblast activity leading to increased bone formation. It has not been confirmed that statins prevent osteoporosis, although statins at conventional doses may not reach the bones at therapeutic doses after hepatic breakdown. 32 Bisphosphonates, known to inhibit osteoclast function, are taken up by macrophages when delivered in liposomes, and have been shown to decrease circulating macrophage activity and neo-intimal hyperplasia in stents in rabbits. 32
While further research is necessary to ascertain a relationship between atherosclerosis and osteoporosis, the strong association between PAD and decreased BMD shown in this study has important implications for disease prevention. Currently, there are no guidelines recommending generalized screening for PAD. However, the United States Preventative Task Force (USPTF) recommends screening for osteoporosis in women aged 65 years and older. 43 Based on our findings, obtaining ABIs may be an appropriate next step in patients diagnosed with osteopenia or osteoporosis. The ABI is a quick, non-invasive, and inexpensive method to assess for atherosclerosis without exposing the patient to ionizing radiation. While it is known that elderly patients are at higher risk for both osteoporosis and atherosclerosis, we found that these processes may occur concomitantly in younger men and women as well. Subjects aged 40–60 years with osteoporosis also had an increased prevalence of PAD compared to subjects with normal BMD (Figure 1 and Figure 2). Based on these results, men and women diagnosed with osteoporosis at an earlier age may have a higher risk for developing atherosclerotic disease. Younger patients could benefit from preventative medical therapy to delay atherosclerotic disease progression and prevent future disease-related morbidity.
While the current study identified a higher prevalence of PAD in subjects with lower BMD in both sexes, there are important differences between the findings in men and women. A larger percentage of men studied were >70 years of age, and men overall had a higher baseline rate of CAS, AAA, hypertension, hyperlipidemia, diabetes, prior myocardial infarction, and smoking history. Interestingly, the prevalence of PAD in women (3.9%) was higher than the prevalence of PAD in men (3.4%). The prevalence of PAD in women with osteoporosis (11.8%) was also higher than the prevalence of PAD in men with osteoporosis (10.9%). Both men and women with lower BMD had a higher prevalence of PAD despite age, although the OR for having PAD in subjects with osteoporosis was higher for men than women (OR 2.3 and 1.89, respectively).
Strengths and limitations
Study limitations include that subjects were self-referred and paid for screening tests, which raises concern for selection bias. The large size of the cohort may be representative of the general population, although it is possible that wealthier or more highly educated patients self-reported for screening. While it cannot be proven that this screening population is representative of the general Unites States population, the prevalence of risk factors measured in the current study are similar to those in other published studies, such as the National Health and Nutrition Examination Survey – a survey of the civilian, non-institutionalized population of the United States.16,44 In addition, subjects reported their own demographics and medical history, which raises concern for reporting bias as the data are neither physician generated or validated. Certain risk factors such as a history of chronic kidney disease (CKD), BMI, family history, race, ethnicity, and socioeconomic status were also not accounted for in this study.
Another limitation to this study is that BMD was measured at a peripheral site, while the World Health Organization recommends BMD to be measured at a central site, such as the lumbar spine or femoral neck. For this reason, fewer studies have evaluated BMD at the calcaneus. While ultrasound rather than DXA was used to determine BMD in this study, ultrasound may be a more cost-effective and easily accessible method to screen for osteoporosis. Studies have shown that although the quantitative ultrasound (QUS) T-score threshold for diagnosing osteoporosis may need to be adjusted, there is a moderate sensitivity for QUS when compared to DXA at the calcaneus using a cut-off score of −2.5.2,21
Although an ABI >1.4 may be consistent with non-compressible calcified arteries in certain patient populations, these patients were not included in the PAD cohort as further imaging would be necessary to ascertain a diagnosis of PAD.
The current study has several strengths, including the large cohort of men and women, which allowed for significant power and strong external validity. The study also reported on many risk factors, which allowed for adjustment of multiple covariates. In addition, all patients underwent non-invasive vascular and BMD screening tests that have high sensitivities and specificities for the diagnoses of PAD and osteoporosis.
Conclusion
Atherosclerosis and osteoporosis have previously been shown to share similar risk factors and cellular components, suggesting a relationship beginning at the molecular level. While this relationship has not been established at this time, a correlation between the prevalence of PAD and osteoporosis has been demonstrated in clinical studies, mostly in postmenopausal women. This study appears to confirm a significant association between PAD and osteoporosis in men and women of all ages, which may have important implications for future disease prevention. Further studies are necessary to elucidate a potential relationship between these disease processes at the molecular level.
Footnotes
Acknowledgements
This study was presented at the 2015 Eastern Vascular Society 29th Annual Meeting, Baltimore, MD, 25 September.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.