
Abstract
While the presence of gender disparities in cardiovascular disease have been described, there is a paucity of data regarding the impact of sex in acute pulmonary embolism (PE). We identified all patients admitted to a tertiary care hospital with acute PE between August 1, 2012 through July 1, 2018. We stratified the presenting characteristics, management, and outcomes between women and men. Of the 2031 patients admitted with acute PE, 1081 (53.2%) were women. Women were more likely to present with dyspnea (59.8% vs 52.0%, p < 0.001) and less likely to present with hemoptysis (1.9% vs 4.0%, p = 0.01). Women were older (63.8 ± 17.4 years vs 62.3 ± 15.0 years, p = 0.04), but had lower rates of myocardial infarction, liver disease, smoking history, and prior DVT. PE severity was similar between women and men (massive: 4.9% vs 3.6%; submassive: 43.9% vs 41.8%; p = 0.19), yet women were more likely to present with normal right ventricular size on a surface echocardiogram (63.2% vs 54.8%, p = 0.01). In unadjusted analyses, women were less likely to survive to discharge (92.4% vs 94.7%, p = 0.04), but after adjustment, there was no sex-based survival difference. There were no sex differences in the PE-related diagnostic studies performed, use of advanced therapies, or short-term outcomes, before and after adjustment (p > 0.05 for all). In this large PE cohort from a tertiary care institution, women had different comorbidity profiles and PE presentations compared with men. Despite these differences, there were no sex disparities in PE management or outcomes.
Introduction
Pulmonary embolism (PE) is the third most common cause of cardiovascular death worldwide, with similar prevalence in men and women.1–3 Much of the sentinel research of cardiovascular disease was performed in male-dominated cohorts, 4 resulting in a persistent deficit of knowledge regarding ways in which sex may impact disease course and outcomes. While sex-mediated differences in coronary artery disease have been the subject of significant attention, less is known about how sex factors into the disease course of PE. 1
It is well-established that women and men can have different presentations and outcomes for the same cardiovascular illness. For example, women more often present with ‘atypical’ symptoms of acute coronary syndrome (ACS), such as nausea or epigastric pain, whereas men tend to present with chest pain. Although women are less likely to undergo a revascularization procedure, the 30-day mortality rate following ACS is lower in women. 5 Prior research has explored similar disparities between men and women with acute PE, but with conflicting findings. For instance, it has been shown previously that women with acute PE more often present with dyspnea and less often present with hemoptysis or chest pain when compared with men. 6 However, another study found a higher rate of syncope among women, but similar rates of dyspnea and chest pain between men and women with acute PE. 7 Sex differences have been explored in the management and outcomes of patients with acute PE, but these studies have been small.8,9 Women with PE may have greater mortality and complications, such as major bleeding when receiving anticoagulation,7,10 although not all studies have shown a significant difference. 11 Multivariable analysis has suggested that sex does not independently predict fatal PE, but rather that patient factors predisposing to worse outcomes (such as advanced age and immobility) are more common in women with PE. 10
Few studies on sex differences in PE assess patient demographics and PE characteristics with the level of granularity needed to adequately adjust for patient factors that could confound evaluation of use of advanced therapies and outcomes. Furthermore, there are no data to our knowledge that evaluate the potential impact of pulmonary embolism response teams (PERTs) on sex-specific outcomes. Given the current limited and conflicting data regarding sex differences with acute PE, we used a PE database from a large, single, tertiary care center to explore contemporary sex differences in demographics, risk factors, clinical presentation, inpatient management, and outcomes among patients admitted with acute PE.
Methods
Study population
We included all patients with acute PE who were admitted to Beth Israel Deaconess Medical Center (BIDMC) between August 2012 and July 2018. Patients with acute PE were identified using an internal billing claims database (International Classification of Diseases (ICD), 9th edition: 415.13, 415.19; ICD, 10th edition: I26.02, I26.09, I26.92, I26.99), and by using a prospective registry of patients who received a PERT consult after the introduction of this team in August 2015. This dataset has been previously described in greater detail. 12 The BIDMC Institutional Review Board approved this study with a waiver of patient informed consent (approval number 2017P000047).
Clinical characteristics and outcomes
Retrospective chart review was performed to confirm diagnosis of acute PE and to evaluate patient demographics, comorbidities, clinical presentation, PE risk factors, PE severity, diagnostic studies, treatment modalities, and outcomes for each patient presenting with acute PE. PE severity was stratified into high risk/massive (associated with hypotension, vasopressor or inotrope requirement, cardiac arrest, or lactate elevated above 5 mmol/L), intermediate risk/submassive (associated with either right ventricular (RV) strain or elevated biomarkers), or low risk (none of above). The primary outcomes evaluated were clinical presentation, acuity of care (including intensive care unit (ICU) admission and requirement for intubation or vasopressors), treatments received (including anticoagulation, inferior vena cava (IVC) filter placement, intravenous (IV) fibrinolysis, catheter-based therapies, surgical embolectomy, and extracorporeal membrane oxygenation (ECMO)), and clinical outcomes (major bleeding, in-hospital survival, 90-day readmission, and 90-day VTE recurrence). Major bleeding was defined as fatal bleed, intracranial hemorrhage, bleed requiring transfusion of two or more units of blood, or bleed requiring intervention.
Statistical analysis
Metric and normally distributed variables are reported as mean ± SD. Non-normally distributed variables are presented as median (IQR). Categorical variables are presented as frequency and percentage. Patients were stratified according to sex and analyzed for differences in baseline characteristics, diagnostics, initial management, and outcomes using Fisher’s exact or χ2 tests, and for continuous variables were compared using Student’s t or Wilcoxon rank sum tests. To account for differences in characteristics, we used inverse probability of treatment weighting (IPTW) to evaluate the adjusted risk of the following outcomes between men and women: major bleeding, survival to discharge, readmission at 90 days, and recurrent VTE at 90 days. Only patients with complete data were included in the IPTW analysis. Covariates incorporated in the model included age, comorbidities (using the list of chronic comorbid health conditions included in the Charlson Comorbidity Index (CCI) 13 ), PE risk factors, markers of illness severity, and year of presentation (to account for the influence of the development and implementation of a PERT program at our institution in August 2015), as listed in online Supplemental Table 2. STATA v16.1 (StataCorp LLC, College Station, TX, USA) was used to perform all analyses. A p-value of less than 0.05 was considered significant.
Results
Patient demographics and clinical characteristics
Of 2031 patients included in the study, 1081 (53.2%) were women and 950 (46.8%) were men. Baseline demographics and clinical characteristics are presented in Table 1. Women had a higher mean age than men (63.8 ± 17.4 years vs 62.3 ± 15.0 years, p = 0.04), and were less likely to have a history of tobacco use (43.1% of women vs 53.3% of men, p < 0.001), prior VTE (19.3% of women vs 24.2% of men, p < 0.01), myocardial infarction (6.6% of women vs 9.7% of men, p = 0.01), and advanced liver disease (1.4% of women vs 3.5% of men, p < 0.01). Conversely, women more often had rheumatologic disorders (6.1% of women vs 3.3% of men, p < 0.01) and dementia (4.0% of women vs 1.7% of men, p < 0.01). Men with acute PE were more likely to be taking an antiplatelet medication at presentation (27.8% of women vs 33.0% of men, p = 0.01), while women were more likely to be on oral contraceptive pills or receiving hormone replacement therapy (8.2% of women vs 0.4% of men, p < 0.01).
Patient demographics and baseline characteristics.
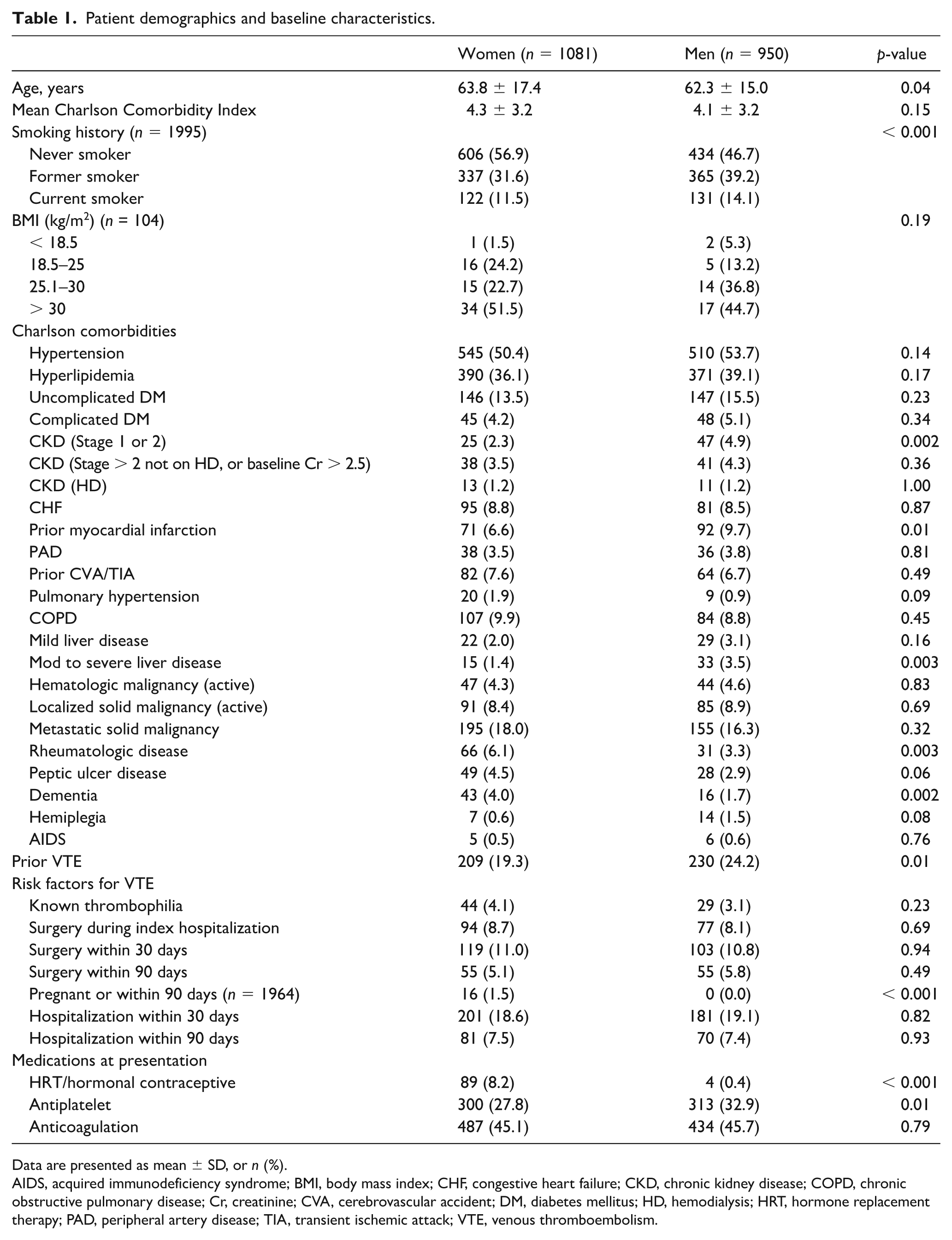
Data are presented as mean ± SD, or n (%).
AIDS, acquired immunodeficiency syndrome; BMI, body mass index; CHF, congestive heart failure; CKD, chronic kidney disease; COPD, chronic obstructive pulmonary disease; Cr, creatinine; CVA, cerebrovascular accident; DM, diabetes mellitus; HD, hemodialysis; HRT, hormone replacement therapy; PAD, peripheral artery disease; TIA, transient ischemic attack; VTE, venous thromboembolism.
Dyspnea was a more common clinical presentation for women with acute PE (59.8% of women vs 52% of men, p < 0.01), whereas hemoptysis was less frequent (1.9% of women vs 4.0% of men, p < 0.01) (Figure 1). Men and women with acute PE did not significantly differ in frequency of asymptomatic presentation or presentation with other symptoms, including chest pain, syncope, and cardiac arrest.
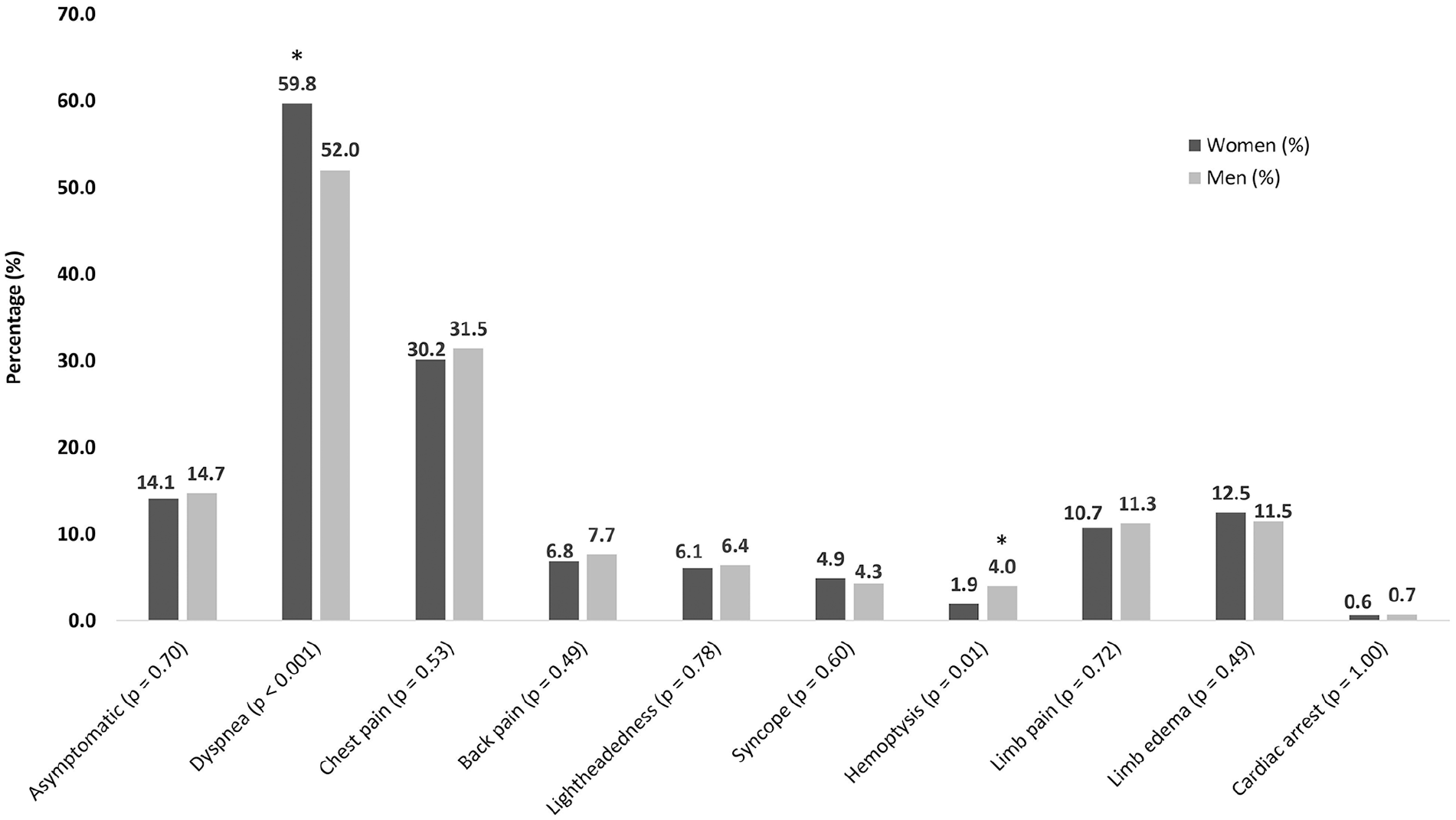
Clinical presentation of female and male patients with acute PE. Women with acute PE were more likely to present with dyspnea, while men with acute PE were more likely to present with hemoptysis.
Diagnostics
PE severity (massive, submassive, or low risk) was similar between women and men, as shown in Table 2. However, women with acute PE were more likely to have normal RV size on a surface echocardiogram (63.2% of women vs 54.8% of men), while men were more likely to have moderate or severe RV enlargement (9.5% of women vs 15.6% of men, p < 0.01). Women with acute PE had a higher median N-terminal pro-brain natriuretic peptide (NT-proBNP) (605 pg/mL [IQR 143–2582] vs 319 pg/mL [IQR 82–1576], p < 0.001). The proportion of patients with concomitant DVT was similar between women and men (43.2% of women vs 45.4% of men, p = 0.40), but among these, women were more likely to have a distal DVT (8.1% of women vs 5.1% of men, p < 0.01). There were no sex-based differences in PE location, computed tomography (CT) evidence of right heart strain, RV function on surface echocardiogram, or troponin elevation (Table 2).
Diagnostic characteristics of acute PE.
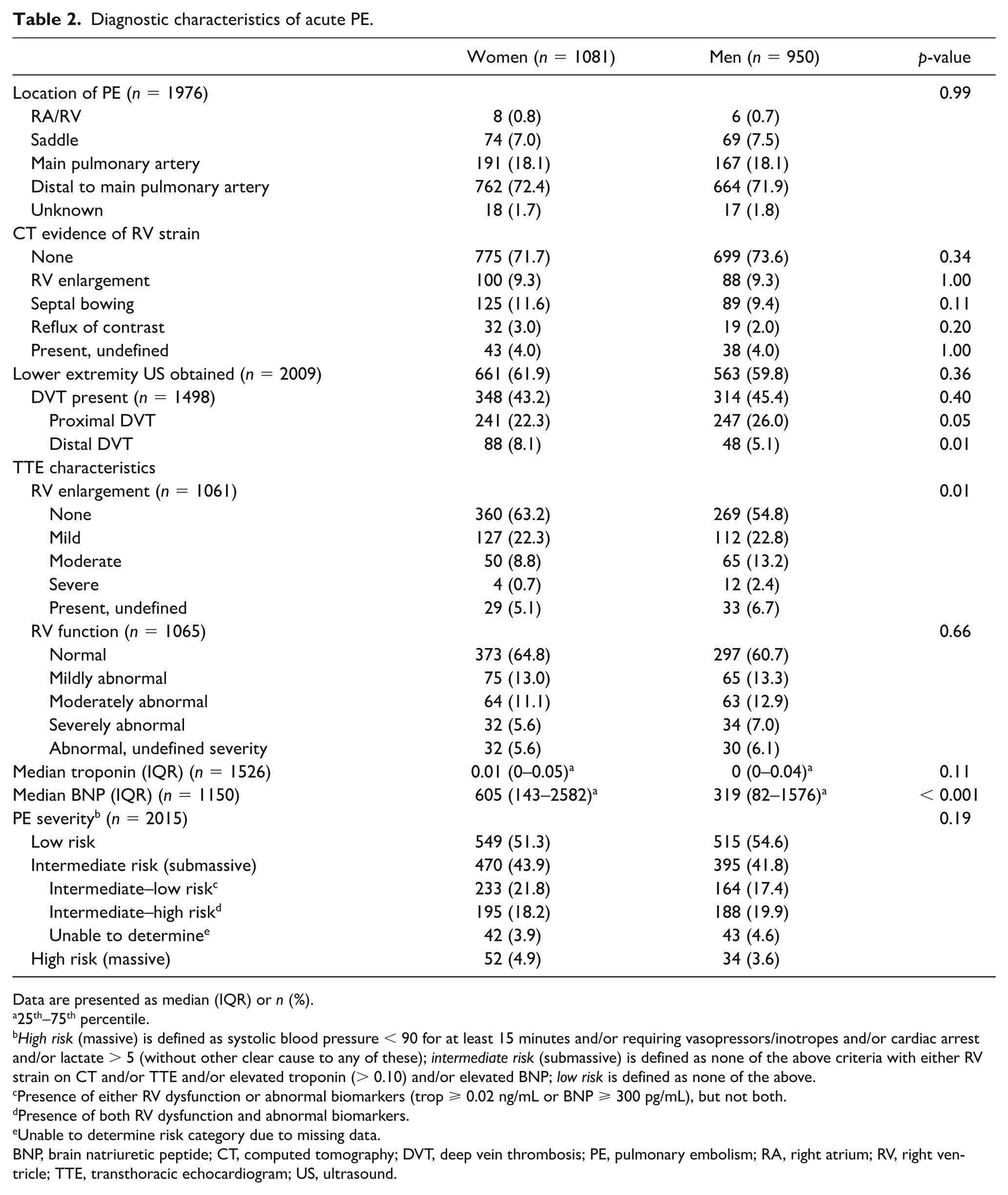
Data are presented as median (IQR) or n (%).
25th–75th percentile.
High risk (massive) is defined as systolic blood pressure < 90 for at least 15 minutes and/or requiring vasopressors/inotropes and/or cardiac arrest and/or lactate > 5 (without other clear cause to any of these); intermediate risk (submassive) is defined as none of the above criteria with either RV strain on CT and/or TTE and/or elevated troponin (> 0.10) and/or elevated BNP; low risk is defined as none of the above.
Presence of either RV dysfunction or abnormal biomarkers (trop ⩾ 0.02 ng/mL or BNP ⩾ 300 pg/mL), but not both.
Presence of both RV dysfunction and abnormal biomarkers.
Unable to determine risk category due to missing data.
BNP, brain natriuretic peptide; CT, computed tomography; DVT, deep vein thrombosis; PE, pulmonary embolism; RA, right atrium; RV, right ventricle; TTE, transthoracic echocardiogram; US, ultrasound.
Management and outcomes
There were no significant sex-based differences in any of the inpatient management endpoints evaluated for patients with acute PE, including diagnostic studies performed, need for intubation, vasopressor use, anticoagulant use, IVC filter placement, and use of advanced therapies (including systemic thrombolysis, ultrasound and non-ultrasound catheter thrombolysis, non-lytic catheter therapy, surgical embolectomy, and ECMO) (Table 3). In addition, discharge anticoagulant regimens were similar between sexes.
Management of acute PE.
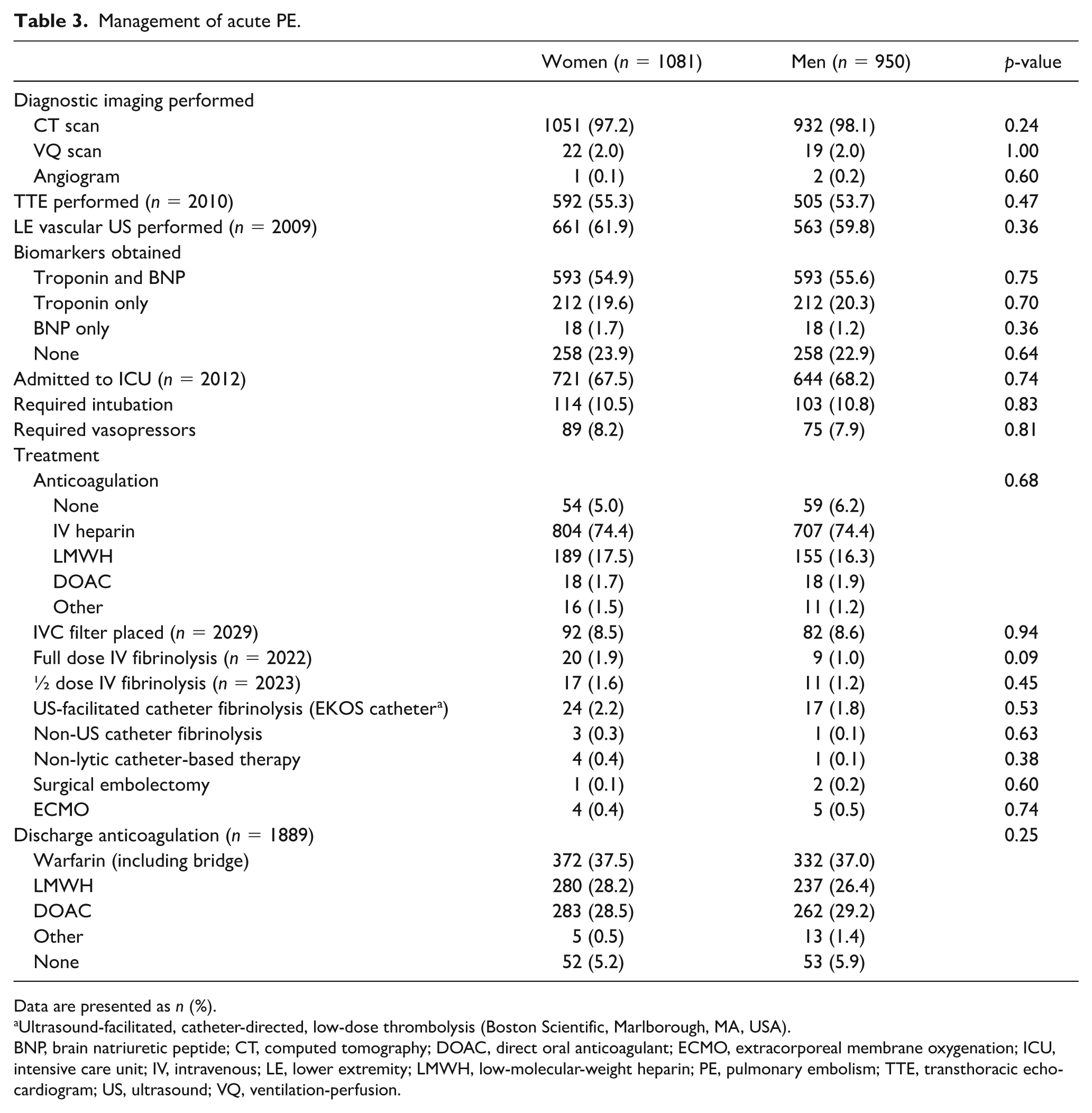
Data are presented as n (%).
Ultrasound-facilitated, catheter-directed, low-dose thrombolysis (Boston Scientific, Marlborough, MA, USA).
BNP, brain natriuretic peptide; CT, computed tomography; DOAC, direct oral anticoagulant; ECMO, extracorporeal membrane oxygenation; ICU, intensive care unit; IV, intravenous; LE, lower extremity; LMWH, low-molecular-weight heparin; PE, pulmonary embolism; TTE, transthoracic echocardiogram; US, ultrasound; VQ, ventilation-perfusion.
In unadjusted analyses, women were less likely to survive to discharge compared with men (92.4% of women vs 94.7% of men, p = 0.04), although the proportion of deaths attributable to PE did not differ (online Supplemental Table 1). There were no sex-based differences in the rate of major bleeding, readmission at 30 or 90 days, or recurrent DVT or PE within 90 days (Figure 2). After adjustment, there was no longer a difference in risk of in-hospital survival between men and women. In addition, adjusted rates of outcomes remained similar between sexes (online Supplemental Table 2).
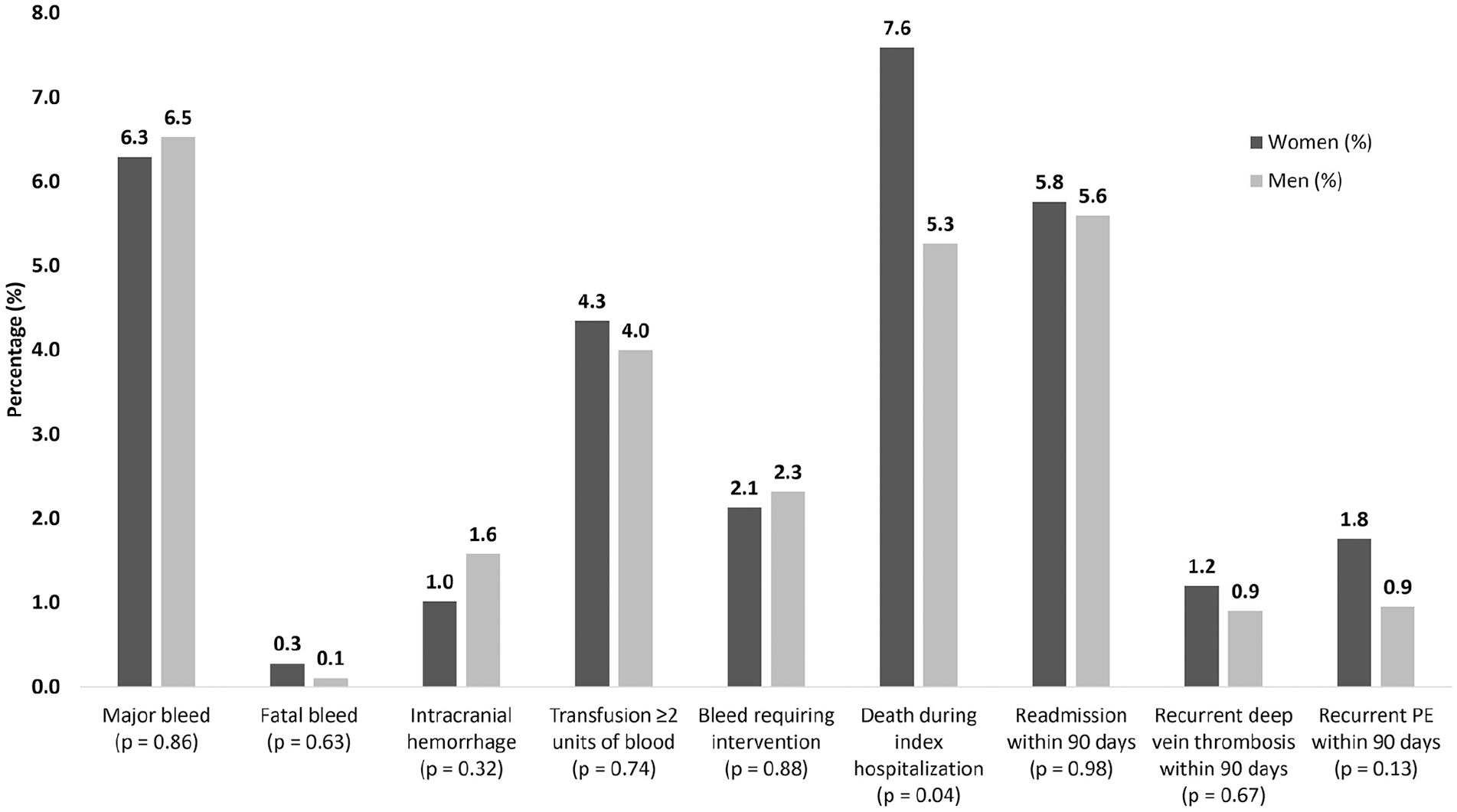
Outcomes of female and male patients with acute PE. Crude rates of in-hospital death were greater among women than men. Following adjustment, there were no significant sex differences in any PE outcomes evaluated.
When survival to discharge was stratified by pre-PERT era (August 2012 to July 2015) and post-PERT era (August 2015 – July 2018), a lower survival to discharge rate for women was noted in the pre-PERT era (91.5% of women vs 95.0% of men, p = 0.045), while in the post-PERT era there was no sex-based survival difference (93.1% of women vs 94.5% of men, p = 0.33). In the pre-PERT era, women also had a significantly higher rate of recurrent PE at 90 days (1.7% of women vs 0.2% of men, p = 0.04). When stratified by pre-PERT era and post-PERT era, no management endpoints or other outcomes were found to have sex-based differences (online Supplemental Tables 3–6). To account for the potential impact of the PERT program, we adjusted for the year of presentation in our primary analysis, and found no sex-based differences in our endpoints (online Supplemental Table 2).
Discussion
In this study, we demonstrated that there are sex-related differences in multiple aspects of acute PE. In particular, despite being of similar age, men had a greater burden of cardiovascular risk factors (i.e. prior myocardial infarction and tobacco use) whereas women had more traditional VTE risk factors (i.e. rheumatologic disorders, pregnancy and hormonal replacement therapy). Women also presented more often with dyspnea and normal RV function. Despite these differences, we found no relationship between sex and the management of acute PE or related outcomes.
It is notable that the prevalence of certain comorbid conditions differed by sex in our study. While men and women with acute PE had an overall similar burden of chronic illness, men had more traditional risk factors for atherosclerotic disease. Prior research suggests overlap between VTE and atherosclerosis risk factors, 14 and this association may play a greater role in the presentation of men with VTE given the higher prevalence of such diseases. Furthermore, commonly acknowledged PE risk factors may not be equally predictive for women and men. 15 For instance, women were less likely to be active smokers than men or to have prior VTE. The lack of characteristics commonly associated with PE may have clinical implications, and could lead to delay in diagnosis. 16 This highlights the value of a comprehensive evaluation of patient comorbidities, which is absent from prior studies on this topic.7,8
We also noted a difference in presenting symptoms between men and women. Women were more likely to present with dyspnea, whereas men were more likely to present with hemoptysis. These findings align with a previous study by McHugh et al. of 2454 patients, which found that women with acute PE were more likely than men to present with dyspnea, less likely to present with hemoptysis, and equally likely to present with syncope or cough. 6 However, our findings on the prevalence of chest pain as a presenting symptom differ from this previous study, as we found no sex-based variation in the rate of chest pain, while McHugh et al. reported a higher prevalence of chest pain as a presenting symptom of acute PE in men. As dyspnea is a common presentation of many cardiovascular disorders, it may be particularly prudent to consider underlying PE as a diagnosis among women if no alternative condition is immediately present. The similar PE severity between women and men in our study differs from prior literature 9 and allowed us to evaluate patient presenting symptoms without confounding from PE severity.
Echocardiographic RV enlargement and elevated NT-proBNP are conventionally thought to be associated with poor outcomes in patients with acute PE. 17 Despite the fact that PE severity and outcomes did not differ between men and women in this study, women with acute PE were more likely to have normal RV size on a transthroracic echocardiogram (TTE). This may suggest that RV size is not as strong a prognostic indicator in female patients, or that a different size cut-off to define RV enlargement in women is warranted. Although no difference in RV strain was detected between sexes on CT, a TTE may provide a more comprehensive assessment of RV function and risk stratification post-PE. 18 It has also been previously shown that women have higher proBNP than men of similar age, 19 which we also found in our analysis. This aligns with sex-based BNP differences following myocardial infarction. 20 However, the opposite trend has been shown previously in heart failure, where studies have shown that male patients have higher average BNP levels than females.21,22 This illustrates that while the presence of abnormal BNP levels has a role in risk stratifying patients with acute PE, other clinical data, such as sex, should also be taken into account.
We found that at our tertiary care center, contemporary PE management and outcomes did not appear to have sex-based differences. While it has been reported that men with PE are more likely to undergo thrombectomy, 11 this was not observed in our analysis. We did find that prior to adjustment, women with acute PE were less likely to survive to discharge during our study period. However, after adjustment, this risk was no longer apparent. As such, comorbid factors, such as advanced age and dementia, likely mediated this relationship. Furthermore, our results may differ from prior reports as we were able to adjust for PE severity, which is closely related to treatment strategy selection. 10 Our findings agree with previous research showing that sex does not independently predict fatal PE, but that patient factors that lead to worse outcomes may be more common in women with PE. When these demographic factors are accounted for, there are no sex-mediated factors that determine PE-related mortality. 10
To our knowledge, there are no prior data evaluating the potential impact of a PERT on sex-specific outcomes. Interestingly, when we stratified outcomes by pre-PERT and post-PERT eras, women during the pre-PERT era had a lower rate of survival to discharge and a higher rate of PE recurrence at 90 days, which was no longer observed in the post-PERT era. However, in adjusted analyses that took into account year of presentation, we found no sex differences in any outcome. Despite this, we do feel that there is likely a positive influence of PERT programs in reducing disparities in how patients of different backgrounds are managed, as PERT provides a more standardized and algorithmic approach to PE treatment. This is an important area for future investigation.
Limitations
This study was performed at a single tertiary care center site, and our results may differ from other patient populations and healthcare systems. Nonetheless, by leveraging our medical center’s electronic medical record, we were able to provide detailed data on all PE patients, including reporting key patient characteristics, such as smoking history and Charlson Comorbidity Index, which were missing from prior comparative analyses.7,8 Data on race or ethnicity were not uniformly collected in this study, which could affect the applicability of our findings to other patient populations. It is possible that patients who present atypically with PE may go undiagnosed, and this study was not designed to capture the prevalence of this. Owing to inconsistencies in data collection, we were not able to differentiate between contraceptive use and hormone replacement therapy. Our study does not account for transgender patients; other research suggests that transgender women have a higher VTE risk than cisgender men and women. 23 Whether there is disparity in acute PE outcomes for transgender patients is an area for future investigation.
Conclusions
In this large, contemporary analysis of patients hospitalized with acute PE, we found differences in predisposing risk factors for the development of PE in women compared with men, as well as variations in presenting symptoms. Despite these findings, there were no sex-based differences in PE severity or need for advanced therapies. Importantly, we did not observe a difference in in-hospital or post-discharge outcomes between women and men with acute PE.
Supplemental Material
3._Supplemental_Table_1 – Supplemental material for Sex differences in presentation, management, and outcomes among patients hospitalized with acute pulmonary embolism
Supplemental material, 3._Supplemental_Table_1 for Sex differences in presentation, management, and outcomes among patients hospitalized with acute pulmonary embolism by Abby M Pribish, Sebastian E Beyer, Anna K Krawisz, Ido Weinberg, Brett J Carroll and Eric A Secemsky in Vascular Medicine
Supplemental Material
Supplemental_Table_2 – Supplemental material for Sex differences in presentation, management, and outcomes among patients hospitalized with acute pulmonary embolism
Supplemental material, Supplemental_Table_2 for Sex differences in presentation, management, and outcomes among patients hospitalized with acute pulmonary embolism by Abby M Pribish, Sebastian E Beyer, Anna K Krawisz, Ido Weinberg, Brett J Carroll and Eric A Secemsky in Vascular Medicine
Supplemental Material
Supplemental_Table_3 – Supplemental material for Sex differences in presentation, management, and outcomes among patients hospitalized with acute pulmonary embolism
Supplemental material, Supplemental_Table_3 for Sex differences in presentation, management, and outcomes among patients hospitalized with acute pulmonary embolism by Abby M Pribish, Sebastian E Beyer, Anna K Krawisz, Ido Weinberg, Brett J Carroll and Eric A Secemsky in Vascular Medicine
Supplemental Material
Supplemental_Table_4 – Supplemental material for Sex differences in presentation, management, and outcomes among patients hospitalized with acute pulmonary embolism
Supplemental material, Supplemental_Table_4 for Sex differences in presentation, management, and outcomes among patients hospitalized with acute pulmonary embolism by Abby M Pribish, Sebastian E Beyer, Anna K Krawisz, Ido Weinberg, Brett J Carroll and Eric A Secemsky in Vascular Medicine
Supplemental Material
Supplemental_Table_5 – Supplemental material for Sex differences in presentation, management, and outcomes among patients hospitalized with acute pulmonary embolism
Supplemental material, Supplemental_Table_5 for Sex differences in presentation, management, and outcomes among patients hospitalized with acute pulmonary embolism by Abby M Pribish, Sebastian E Beyer, Anna K Krawisz, Ido Weinberg, Brett J Carroll and Eric A Secemsky in Vascular Medicine
Supplemental Material
Supplemental_Table_6 – Supplemental material for Sex differences in presentation, management, and outcomes among patients hospitalized with acute pulmonary embolism
Supplemental material, Supplemental_Table_6 for Sex differences in presentation, management, and outcomes among patients hospitalized with acute pulmonary embolism by Abby M Pribish, Sebastian E Beyer, Anna K Krawisz, Ido Weinberg, Brett J Carroll and Eric A Secemsky in Vascular Medicine
Footnotes
Dr Geoff Barnes served as Guest Editor for this manuscript.
Declaration of conflicting interests
The authors declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: Eric A Secemsky: research grants to BIDMC: AstraZeneca, BD, Boston Scientific, Cook, CSI, Medtronic, Philips, and UCSF; consulting/speaking: Abbott, Bayer, BD, Cook, CSI, Janssen, Medtronic, and Philips. The authors declare that there are no other conflicts of interest.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Eric Secemsky is funded in part by a NIH/NHLBI K23HL150290.
Supplementary material
The supplementary material is available online with the article
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.