
Abstract

Keywords
Critical limb ischemia (CLI) is a severe clinical condition of ischemic pain at rest or tissue loss related to peripheral artery disease (PAD).1,2 Endovascular arterial revascularization plays a vital role in patients with CLI. The initial recanalization strategy is the antegrade approach, which is not feasible in approximately 20% of the patients. 3 In this study, we aimed to describe our outcomes of the subintimal arterial flossing with the antegrade–retrograde intervention (SAFARI) in patients with lower extremity tissue loss due to CLI.
We retrospectively reviewed patients who underwent lower extremity arterial intervention between 2012 and 2015. The patients who underwent femoropopliteal/infrapopliteal recanalization using the SAFARI, for Rutherford category (RC) 5 and 6 diseases, following an unsuccessful antegrade recanalization attempt, were identified. The patients’ demographics, comorbidities, amputations, primary patency rates, limb salvage rates, and major amputation-free survival rates (AFS) are reported. Institutional review board approval was obtained for this study (no. 19082502IRB01), and informed consent was obtained from all patients before the procedure.
The procedure is illustrated in Figure 1. After an unsuccessful antegrade recanalization attempt, patients were evaluated for an appropriate retrograde access site in the same session or a different session according to the proceduralist’s preference. After administering local anesthesia with lidocaine 1%, under ultrasonographic or fluoroscopic guidance, retrograde access was gained using a 21-gauge micro-puncture access needle (Cook, Inc., Bloomington, IN, USA). Then, a 0.018-inch micro-puncture kit guidewire was inserted into the micro-puncture needle, and the needle was exchanged for a 3-F micro-puncture access sheath. Through this access, a 0.018-inch hydrophilic tip wire was introduced, followed by a 0.018-inch CXI support catheter (Cook, Inc.) or Quick-Cross (Spectranetics, Colorado Springs, CO, USA). If the wire crossed the occlusions and met with the 4-mm snare (Merit Medical, South Jordan, UT, USA) in the lumen of the subintimal plane introduced from the antegrade approach by the rendezvous technique, the wire was captured by the snare and through-and-through access was achieved by pulling the wire out from the femoral access sheath. Once the flossing access was obtained, arteries were treated with varying combinations of percutaneous transluminal angioplasty, atherectomy, and stent placement via the antegrade approach.
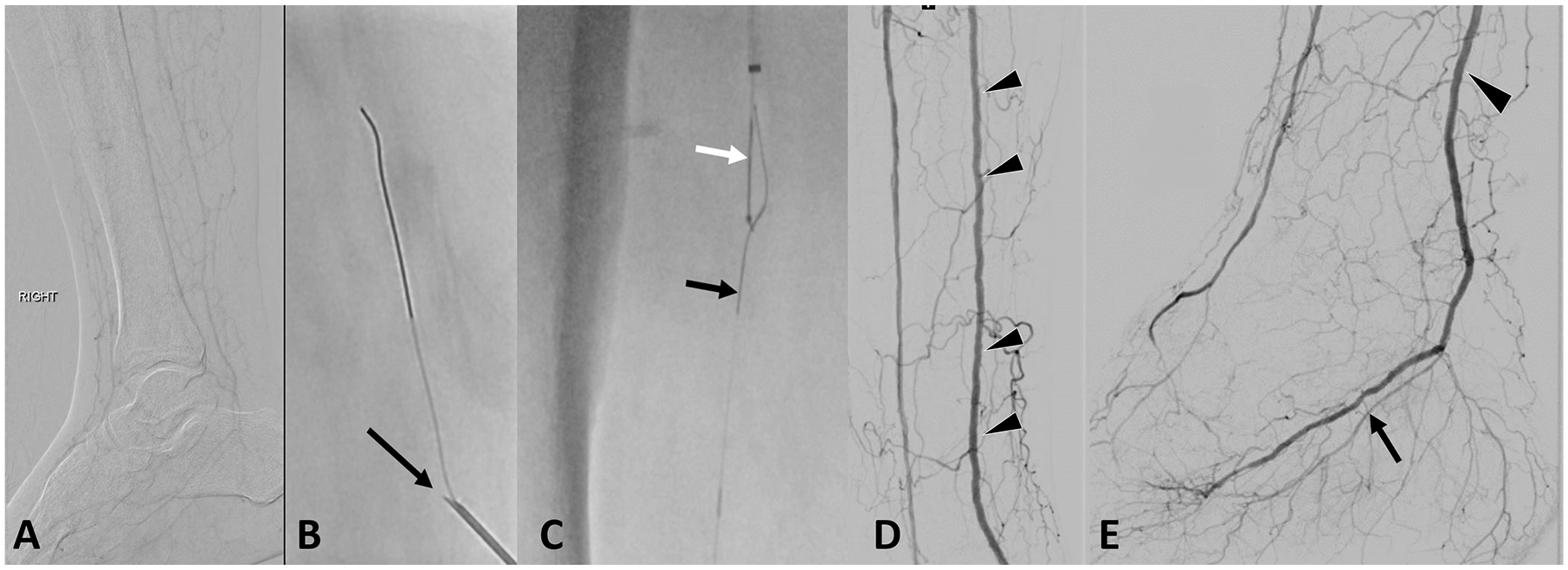
(A) Right lower extremity DSA demonstrates occlusion of the posterior tibial and plantar arteries. (B) Puncture of the posterior tibial artery with a micro-puncture needle (black arrow) and the introduction of a guidewire wire via retrograde access. (C) A through-and-through flossing access was gained: the retrograde guidewire (black arrow) was captured with the antegrade snare (white arrow) and pulled out from the antegrade access sheath. (D, E) Postangioplasty DSA demonstrates the patency of the posterior tibial (arrow) and plantar arteries (arrowheads).
The primary patency, AFS, and limb salvage rates were calculated using the Kaplan–Meier Product Limit method and 95% CI, and are shown in the online Supplemental Figure. Statistical analysis was performed utilizing SAS 9.4 software (SAS Institute, Inc., Cary, NC, USA).
A total of 286 patients underwent lower extremity arterial intervention between 2012 and 2015. Among these, 62 limbs in 56 patients were identified (31 men, 25 women; mean age 71.7 [range 38–98] years). Significant past medical history included: hypertension 89% (n = 50), diabetes 76% (n = 43), hyperlipidemia 64% (n = 36), history of smoking 51% (n = 29), coronary artery disease 23% (n = 13), and prior failed bypass surgery 21% (n = 12). Thirteen (21%) limbs had RC-5 disease and 49 (79%) limbs had RC-6 disease (online Supplemental Table). The retrograde access site was the anterior tibial artery or dorsalis pedis artery in 60% (n = 37) of the limbs, posterior tibial artery in 27% (n = 17), and the peroneal artery in 13% (n = 8). Angioplasty was performed in all patients: at the femoropopliteal level in 7% (n = 4), at the infrapopliteal level in 20% (n = 12), and both levels in 73% (n = 46) of the limbs. Atherectomy was used in 30% (n = 19) and an Outback re-entry device (Cordis, Bridgewater, NJ, USA) was used in 20 limbs (32%). The technical success rate was 98%. A minor complication occurred in one of 62 (2%) procedures. Among the 55 successfully treated patients, the median follow-up time was 14 months, ranging from 1 to 53 months. One patient was lost to follow-up at 1 month, three at 1–6 months, three at 6–12 months, one at 12–24 months, and seven patients beyond 24 months. Among the patients who were followed up, 20% (n = 11) died due to cardiac and infectious reasons. AFS rates were 91% (95% CI: 79–96%), 85% (95% CI: 71–93%), and 85% (95% CI: 71–93%) at 6, 12, and 24 months, respectively. The primary patency rates at 6, 12, and 24 months were 81% (95% CI: 68–90%), 74% (95% CI: 59–84%), and 66% (95% CI: 44–81%), respectively (online Supplemental Figure). The limb salvage rates at 6, 12, and 24 months were 91% (95% CI: 81–96%), 87% (95% CI: 74–93%), and 87% (95% CI: 74–93%), respectively. There was no significant statistical difference in the primary patency (p = 0.105), AFS (p = 0.550), and limb salvage rates (p = 0.497) between the RC-5 and RC-6 diseases. There were two patients (3%) with above-the-knee amputations and six patients (10%) with below-the-knee amputations at the 24-month follow-up. Before the intervention, ankle–brachial index (ABI) data were available in 48 limbs (78%); of these, five limbs had non-compressible arteries. In the 43 limbs (70%), the mean ABI was 0.66. At 30 days after the SAFARI, ABI data were available in 24 limbs (39%); of these, four limbs had non-compressible arteries. In the 20 (32%) limbs, the mean ABI was 0.79.
Patients with RC-5 and RC-6 diseases have an increased risk of morbidity, independent of all other comorbidities. Therefore, these patients tend to have more amputations and higher mortality rates than those with lesser RCs, independent of all other comorbidities.4,5 Therefore advanced recanalization techniques play a crucial role to decrease the mortality and mortality rates.
Our study highlights that the SAFARI technique is feasible and safe, with a technical success rate of 98%. The technical success rates of combined antegrade and retrograde recanalization vary in the literature between 85% and 100%.3–8 Even though there is variability among the success rates, overall the success rates remain high. We believe that this wide range in the rates is a result of differences in experience and used devices.
Limitations of this study are its retrospective and single center nature, non-standardized patient follow-up, and lack of uniformity among the patients and used devices.
SAFARI is an advanced revascularization technique, which can be utilized when the antegrade approach is unsuccessful. This safe technique can improve the limb salvage and amputation-free survival rate. Multicentric studies with a large number of patients are needed to confirm the long-term efficacy of this technique.
Supplemental Material
FIGURE2 – Supplemental material for Outcomes of subintimal arterial flossing with antegrade–retrograde intervention on patients with critical limb ischemia and tissue loss
Supplemental material, FIGURE2 for Outcomes of subintimal arterial flossing with antegrade–retrograde intervention on patients with critical limb ischemia and tissue loss by Merve Ozen, Fang Zhu, Chen Ma, Shelly Bhanot, Bulent Arslan and Ulku Cenk Turba in Vascular Medicine
Supplemental Material
Table_VM – Supplemental material for Outcomes of subintimal arterial flossing with antegrade–retrograde intervention on patients with critical limb ischemia and tissue loss
Supplemental material, Table_VM for Outcomes of subintimal arterial flossing with antegrade–retrograde intervention on patients with critical limb ischemia and tissue loss by Merve Ozen, Fang Zhu, Chen Ma, Shelly Bhanot, Bulent Arslan and Ulku Cenk Turba in Vascular Medicine
Footnotes
Acknowledgements
We would like to thank Dr. Volkan Beylergil for his contribution.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Supplementary material
The supplementary material is available online with the article.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.