
Abstract

Vascular calcification is a common complication of end-stage renal disease (ESRD), manifested as intimal and medial calcification of large arteries. 1 It is associated with reduced arterial elasticity, cardiovascular events, and all-cause mortality in patients who are on hemodialysis. Prior studies have identified several vascular calcification biomarkers, such as phosphate, osteoprotegerin (OPG), osteopontin (OPN), and fibroblast growth factor 23 (FGF23). 2 However, none of them has been demonstrated as a clinically useful predictor in ESRD. Galectin-3 is a 29–35 kDa protein expressed by activated macrophages, neutrophils, and many other types of cells. 3 It is associated with aortic valve calcification and arterial calcification in diabetes mellitus.4,5 Increased galectin-3 level was also observed in patients with peripheral artery disease. 6 Here, we explored the association between serum galectin-3 and abdominal aortic calcification (AAC) in patients on maintenance hemodialysis.
From June 2014 to January 2015, we enrolled 311 hemodialysis patients and performed a cross-sectional study to understand the associations between serum galectin-3 and various cardiovascular complications. This project was approved by the Ethics Committee of Renji Hospital, and written informed consent was obtained from all enrolled patients. Patients who underwent stable hemodialysis (three sessions a week for at least 3 months) were included for screening. Patients with any of the following conditions were excluded: heart failure (New York Heart Association Class III or IV or left ventricular ejection fraction < 40%), moderate or severe aortic valve stenosis, atrial fibrillation, second- or third-degree atrioventricular block, use of a pacemaker, recent myocardial infarction (MI) (⩽ 3 months), recent stroke (⩽ 3 months), recent transient ischemic attack (⩽ 3 months), pulseless extremity, malignancy, acute infectious diseases (⩽ 3 months), and those who refused to participate in this study. Blood samples were collected before the midweek dialysis session, and serum galectin-3 concentration was measured with an enzyme-linked immunosorbent assay (Human Galectin-3 Quantikine ELISA Kit; R&D Systems Inc., Minneapolis, MN, USA). The association between galectin-3 and arterial stiffness was reported elsewhere. 7
Aortic calcification assessment was offered to a subset of the study group who agreed to participate in this sub-project (n = 105, male = 61%, median age = 62 years, median dialysis duration = 79 months). We used a plain lateral lumbar radiograph to assess AAC. Calcific densities in the aorta at the level of the first through fourth lumbar vertebrae were graded on a 0 to 3 scale at each lumbar vertebra. The severity of AAC was categorized into tertiles based on the total aortic calcification score: no or mild (< 5 points), moderate (5–15 points), and severe (> 15 points).8,9
We found that as high as 74% of patients had moderate or severe AAC (moderate = 49, severe = 29). Serum galectin-3 concentration was significantly higher in those who had moderate or severe AAC (33.64 ± 11.41 vs 27.53 ± 9.74 ng/mL, p = 0.021). The optimal cut-off value of galectin-3 for the classification of AAC was 35.08 ng/mL, which was obtained based on the maximization of the Youden index. On the receiver operating characteristic (ROC) curve analysis, the area under the ROC curve was 0.654. Univariable logistic regression showed that a high galectin-3 level, increasing age, longer time since start of dialysis, and increased pulse pressure were associated with a high prevalence of moderate or severe AAC. These results were in line with prior studies.10,11 After adjusting for demographics and clinically relevant factors, including age, years on dialysis, pulse pressure, spKt/V for urea, C-reactive protein, and phosphorus, multivariable logistic regression showed the galectin-3 concentration (1 ng/mL increase) was independently associated with a 7% increased risk of moderate or severe AAC (odds ratio = 1.07, 95% CI: 1.007–1.138, p = 0.03) (Table 1).
Correlations between serum galectin-3 and moderate or severe abdominal aortic calcification in a multivariable logistic regression model.
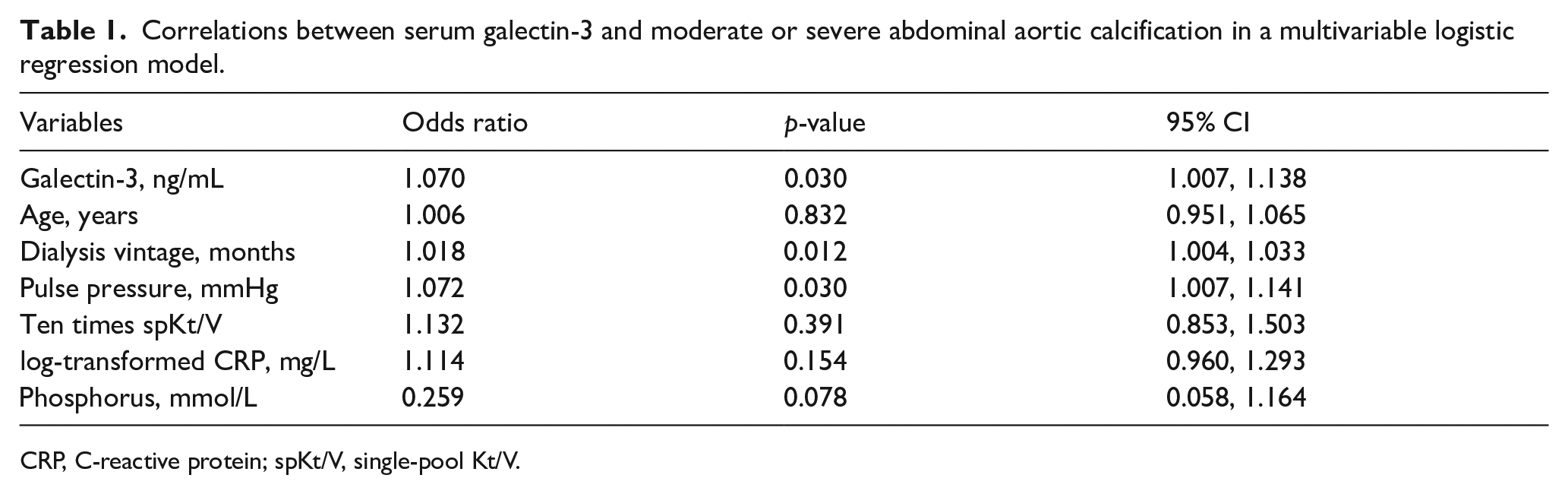
CRP, C-reactive protein; spKt/V, single-pool Kt/V.
The diagnostic and prognostic utilities of galectin-3 have been demonstrated in various cardiovascular diseases but remain controversial in the setting of advanced chronic kidney disease or renal failure. 12 Our study demonstrates that galectin-3 has a weak but independent association with AAC in patients on hemodialysis. These findings may be explained by the important role galectin-3 plays in the phenotype transformation of human vascular smooth muscle cells, contributing to vascular wall calcification. 13 Galectin-3 is also actively involved in atherosclerosis development and progression, which may indirectly cause arterial calcification. 14 This study suggests that galectin-3 may be a new biomarker of predicting AAC in patients undergoing hemodialysis. Given the relatively weak association, combining galectin-3 with other biomarkers, such as OPG and OPN, could be a more promising strategy to predict AAC. Besides, further studies are needed to evaluate the utility of galectin-3 in predicting the long-term risk of developing cardiovascular events in hemodialysis patients.
Footnotes
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: this work was partly supported by the Science & Technology Innovation Fund (No. CK2019010) of Shanghai Ninth People’s Hospital, Shanghai Jiaotong University School of Medicine.