
Abstract

Keywords
The clinical significance and management of subsegmental pulmonary embolism (SSPE) remains controversial, with questionable benefit of anticoagulation in these patients.1,2 Some studies have suggested overtreatment and possible treatment-related harm. 3 Lack of consensus is due to paucity of data regarding clinical presentation, underlying associated comorbidities and lack of long-term follow-up.
We conducted a retrospective study at a tertiary care, academic center to understand clinical characteristics, management, and outcomes in SSPE patients. The study protocol was approved by our institution’s human subjects protection committee and the institutional review Board. Imaging and medical records were reviewed to identify patients with SSPE diagnosed using multi-detector computed tomography angiography (CTA) from January 1, 2013 to June 30, 2017, with 73% of CT scans done per pulmonary embolism (PE) protocol. Patients with proximal PE or concomitant deep vein thrombosis (DVT) at time of SSPE diagnosis or without follow-up information were excluded.
We identified 189 patients with isolated SSPE. A majority of patients were symptomatic (78.3%) at time of diagnosis (Table 1) and the rest (21.7%) were diagnosed incidentally (SSPE found on chest CT ordered for a reason other than suspected PE). Most patients (74.6%) had at least one underlying risk factor for venothromboembolism (VTE) (71.2% symptomatic group; 86% asymptomatic group). Diagnostic settings were as follows: inpatient (43.4%), emergency department (ED) (33.9%), and clinic (22.8%). There were significant differences in hospitalization rates after diagnosis based on the clinical setting: 94.6% of those who presented to the ED were admitted, while only 19.2% from the clinic.
Findings in patients with isolated SSPE.
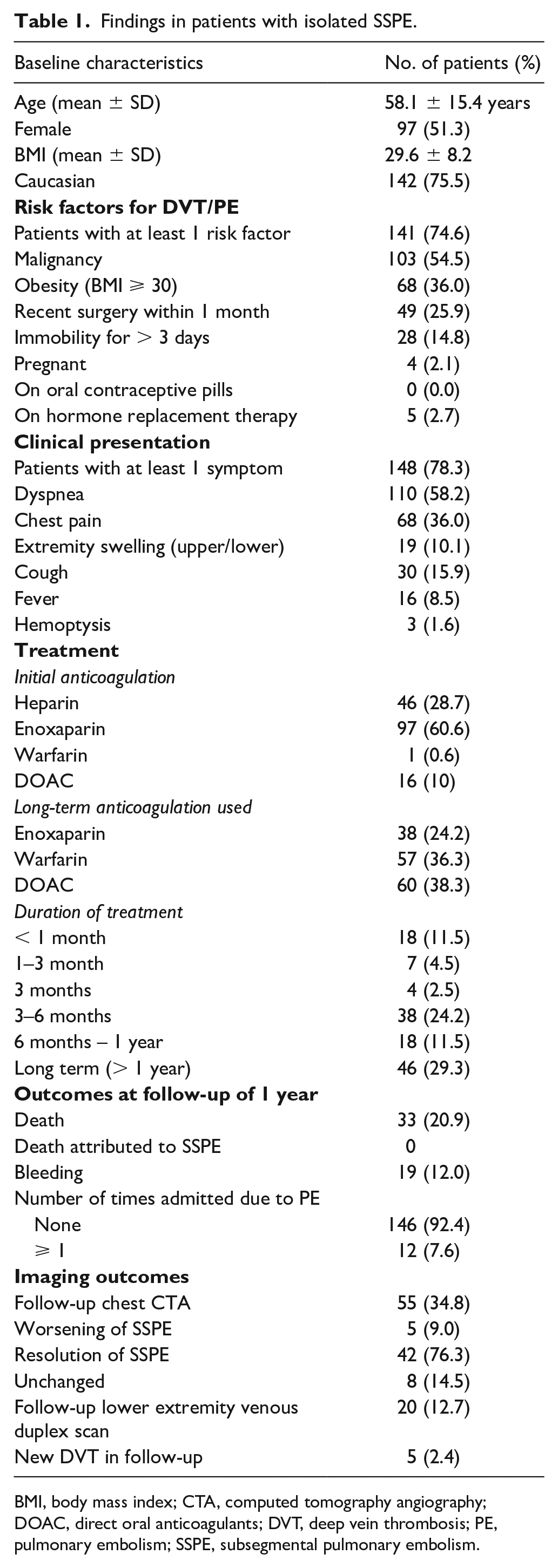
BMI, body mass index; CTA, computed tomography angiography; DOAC, direct oral anticoagulants; DVT, deep vein thrombosis; PE, pulmonary embolism; SSPE, subsegmental pulmonary embolism.
Most patients (84.7%) received anticoagulation (AC) irrespective of VTE risk factors and symptoms. Enoxaparin was the most frequent initial agent (60.6%) used, whereas for long-term anticoagulation, direct oral anticoagulants (DOACs) were used in 38.3% and warfarin in 36.3%. Duration of AC was variable, with 67.5% of patients treated for ⩾ 3 months (Table 1).
One-year follow-up was available for 69% of the cohort. One-year all-cause mortality was 20.9% (none attributable to VTE). The 1-year recurrence rate for VTE was 15.4% in non-anticoagulated versus 3.0% in anticoagulated patients (p = 0.009). Nineteen patients (12%) experienced bleeding during the follow-up period (anticoagulated patients (n = 18; 13.6%); non-anticoagulated (n = 1; 3.8%), p = ns).
Several reviews and commentaries have been published in the past few years that have suggested that SSPE is most often a benign entity that may not need anticoagulation.1,4–6 These opinions are based mostly on small retrospective studies. A recent Cochrane review was unable to reach any conclusions due to absence of enough evidence. 7 This lack of a strong evidence base is reflected in current CHEST guidelines that recommend surveillance in most patients with isolated SSPE and anticoagulating those considered at higher risk (level of recommendation is weak at 2C). 8 Further, a recent systemic review of 14 studies identified just 693 (the largest study had 116) patients, with no randomized study. 1 This review found a low mortality (2.1% vs 3.0%) and a low 3-month VTE recurrence (5.3% vs 3.9%) in AC and non-AC patients, respectively. These findings are discrepant from our study, where we found SSPE to be associated with a higher risk of VTE recurrence and all-cause mortality, but due to the small number of patients in our study, firm conclusions cannot be drawn. This may be because our patient population in a large tertiary care academic center had a high prevalence of underlying VTE risk factors (malignancy in 55%) and symptoms. As opposed to several prior studies, where either symptomatic status was not reported or low, and if reported, the number of asymptomatic patients was significantly higher. Our findings are more in line with the study by Den Exter et al., who compared isolated SSPE patients (n = 116) to those with proximal PE and those in whom SSPE had been ruled out. 9 They found that SSPE patients had similar VTE risk profiles, symptoms, and 3-month outcomes to the proximal PE patients and a higher risk profile than those with no SSPE/PE.
The observed high 1-year all-cause mortality (20.9%) likely suggests that presence of SSPE may be a harbinger of poor prognosis and may represent a sicker patient pool. In fact, 88% of those who died in follow-up had an underlying malignancy. Since most patients were anticoagulated, we are unable to draw firm conclusions about the benefits of anticoagulation, though the higher VTE recurrence rate in non-AC patients is concerning. The optimal duration of anticoagulation is also difficult to conclude, though 40.8% of patients in our study were anticoagulated for ⩾ 6 months. The high 1-year bleeding risk of 12% is concerning, but comparable to that of prior studies in patients with SSPE or PE.3,10
A major limitation of our study is that the results may not apply to healthier patients diagnosed in a primary care or less acute setting and in those where the diagnosis is mostly incidental.
In conclusion, our study results show that in a tertiary care setting most patients with isolated SSPE are either symptomatic or have underlying VTE risks and most of them receive AC appropriately per current guidelines.
Footnotes
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.