
Abstract
Abnormal vasculature is a key feature of hereditary hemorrhagic telangiectasia (HHT) and can also present in the nail fold capillary beds. However, the exact prevalence and the clinical diagnostic value in HHT are still largely unknown. The nail fold can be easily and noninvasively inspected with a capillary microscope. We therefore retrospectively assessed the prevalence and diagnostic value of abnormal nail fold capillaries in all patients who were screened between January 2000 and July 2017 for the presence of HHT and underwent capillary microscopy in St Antonius Hospital, The Netherlands. Capillary microscopy results and clinical characteristics were extracted from medical files and the prevalence of abnormal nail fold capillaries was calculated and the diagnostic value of the Curaçao criteria with and without capillary microscopy results was assessed. Of the 1761 individuals screened, 923 (52%) were diagnosed with a clinical and/or genetic HHT diagnosis. In these patients, capillary microscopy was normal in 23% (n = 218), enlarged loops were seen in 11% (n = 99), and giant loops in 66% (n = 606). The sensitivity and specificity of the Curaçao criteria for the diagnosis of HHT without capillary microscopy results were 96% and 90%, respectively. The addition of the presence of giant loops to the Curaçao criteria led to a small increase in sensitivity to 97% without affecting the specificity. In conclusion, the prevalence of nail fold abnormalities in patients with HHT is high. Capillary microscopy can be a useful, easy, and noninvasive diagnostic tool in HHT.
Keywords
Background
Hereditary hemorrhagic telangiectasia (HHT), also known as Rendu–Osler–Weber syndrome, is a rare autosomal dominant-inherited disease affecting approximately 1 in 5000 persons. 1 There are mainly two types of HHT with disease-causing mutations in the genes encoding for ENG (endoglin) and for ACVRL1 that cause HHT type 1 and HHT type 2, respectively.2,3 In a minority of the patients, mutations in the SMAD4 gene lead to the juvenile polyposis/HHT overlap syndrome. 4 However, families still exist with clinically confirmed HHT where a specific gene cannot be identified despite extensive genetic testing.5,6 The aforementioned genes are expressed in endothelial cells of blood vessels and regulate signaling of the transforming growth factor β pathway. Disruption of this pathway will result in remodeling of vascular structures and eventually in the formation of telangiectases and arteriovenous malformations (AVMs). 7
The microvasculature of the nail folds can be inspected with a capillary microscope, which is a safe and noninvasive technique. 8 The normal capillary bed of the fingernail shows a regular, homogenous pattern of hair-pin shaped capillary loops along the nailbed in a ‘comb-like’ distribution with nine to 14 capillaries per millimeter. 9 In autoimmune rheumatic diseases like scleroderma, systemic sclerosis and dermatomyositis, or more common diseases such as diabetes mellitus, the nail fold can show abnormal patterns of capillaries with architectural disorganization and enlargement (so-called mega or giant capillaries).10–12 In autoimmune diseases, these vascular abnormalities seem to appear in an early stage of the disease and have proven to be a valuable characteristic in the diagnostic process.9,13
Limited data are available of capillary microscopy results in patients with HHT. However, in accordance with autoimmune rheumatic diseases, abnormal capillaries have been observed in patients with HHT. The prevalence is estimated to be between 7% and 87% of patients.14–17 However, the number of patients in these published studies is relatively small, with the sample sizes ranging from 54 to 195 patients and the range of capillary abnormality prevalence is wide. The aims of this study were: (1) to further assess the prevalence of nail fold abnormalities in a large cohort of patients with (suspected) HHT; and (2) to evaluate the additional diagnostic value of capillary microscopy in the clinical diagnosis of HHT. In HHT, it is possible that, similar to rheumatologic diseases, microvascular abnormalities are present as an early sign and could precede the macroscopic mucocutaneous telangiectases. Especially in patients with a possible clinical diagnosis (e.g. two positive criteria) without any other visible mucocutaneous telangiectases, capillary microscopy could be of additional value.
Methods
Study design and patients
This retrospective cohort study involved all patients who were referred to the pulmonology outpatient clinic of St Antonius Hospital, Nieuwegein, The Netherlands, with the suspicion of HHT between January 2000 and July 2017. All patients were examined with a structured diagnostic protocol assessing signs and symptoms of HHT. The clinical diagnosis of HHT is made based on the presence of the four Curaçao criteria. 18 The Curaçao criteria included the presence of spontaneous epistaxis; multiple mucocutaneous telangiectases at characteristic sites; visceral AVMs; and a first-degree relative with HHT. HHT is ‘unlikely’ with less than two criteria present; ‘possible or suspected’ with two criteria present; and ‘definite’ with three or more positive criteria. Genetic testing was offered to adult patients. The nail fold capillary microscopy results were not used in the Curaçao criteria except in the sensitivity and specificity analyses.
Nail fold capillary microscopy
Capillary microscopy has been incorporated in the diagnostic protocol of patients referred to our hospital with the suspicion of HHT since our first publication concerning capillary microscopy in 2000. 14 Nail fold capillary microscopy was performed by one of the two experienced pulmonologists involved in the HHT center of excellence at St Antonius Hospital using a stereo zoom microscope (Leica MZ6 and Leica M60; Leica Microsystems, Heerbrugg, Switzerland). A magnification of 16× to 40× was used to inspect the nail fold capillaries. A circular lamp embedded in the microscope elicited the light source. Immersion oil was used to increase the resolving power of the microscope. We examined all fingers from both hands with the exception of the thumbs because the skin at the nail fold of the thumb may be too thick for adequate inspection. We distinguished ‘normal capillaries’, ‘capillaries with enlarged afferent or efferent loops’, and ‘giant loops’ – also referred to as ‘mega capillaries’. Enlarged loops were defined as non-substantial enlargement of the capillary compared to the adjacent capillaries or only an enlargement of either the afferent or efferent part of the capillary. Giant loops were defined as enlargement of both the afferent and efferent part with a substantial difference in size as compared to the adjacent capillaries. If nail fold abnormalities that can be seen in rheumatic diseases such as micro-hemorrhages, loss of capillaries, disorganization of the capillary architecture, or absent capillaries were also observed, together with giant or enlarged loops, we did not regard this as giant loops associated with HHT. Example photographs for this article were made with both the stereo microscope and a Dino-Lite Edge CapillaryScope with a magnification of approximately 20× to 180× (see Figure 1).
Statistical analysis
Data are presented as mean and SD, and parametric testing is used. Quantitative data were presented as absolute frequencies or percentage. We used the independent sample’s t-test to compare continuous variables and we used the chi-squared test to compare categorical variables. In case of missing data, complete case analysis was performed. Statistical analysis was performed with SPSS version 23.0 for Windows (IBM Corp., Armonk, NY, USA). The sensitivity and specificity of the Curaçao criteria were calculated without and with capillary microscopy results. In the sensitivity and specificity analysis 1, capillary microscopy results were not used. In analysis 2, in patients without mucocutaneous telangiectases but with giant loops in the nail fold, the criterion ‘mucocutaneous telangiectases’ shifted from ‘negative’ to ‘positive’. In analysis 3, in patients without mucocutaneous telangiectases but with both giant and/or enlarged loops in the nail fold, the criterion ‘mucocutaneous telangiectases’ changed to ‘positive’. For the sensitivity and specificity analysis 1, individuals with two Curaçao criteria were excluded from this analysis since their clinical diagnosis is ‘possible’ but not definite. For the sensitivity and specificity analyses 2 and 3, the individuals with two Curaçao criteria after the addition of the capillary microscopy results, were excluded. DNA testing was regarded as the gold standard: patients without a DNA test were excluded. In addition, patients without a known genetic family mutation were excluded from the sensitivity and specificity analyses. This was done to ensure that patients with a negative mutation do not in fact have HHT, rather than belonging to the group of HHT families without a known mutation.
Ethics
Exemption for a full review from the Local Research Ethics Committee (Medical research Ethics Committees United (MEC-U)) was obtained (Z12.070). Reporting of this study is done in accordance with the Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) statement 19 and the Declaration of Helsinki.
Results
Patient characteristics
In total, 1761 individuals were screened between January 2000 and July 2017 in St Antonius Hospital for the presence of HHT features and underwent capillary microscopy. In this study, 56% (982 patients) were female. The mean age was 34 years with a SD of 20 years. HHT was diagnosed according to clinical Curaçao criteria in 814 (46%) of the individuals. A genetic mutation was found in 654 patients (37%), with mutations in the ENG, ACVRL1, and SMAD4 gene in 334, 296, and 24 individuals, respectively. A clinical and/or genetic HHT diagnosis was made in 923 individuals (52%). The baseline characteristics are described in Table 1.
Baseline characteristics.
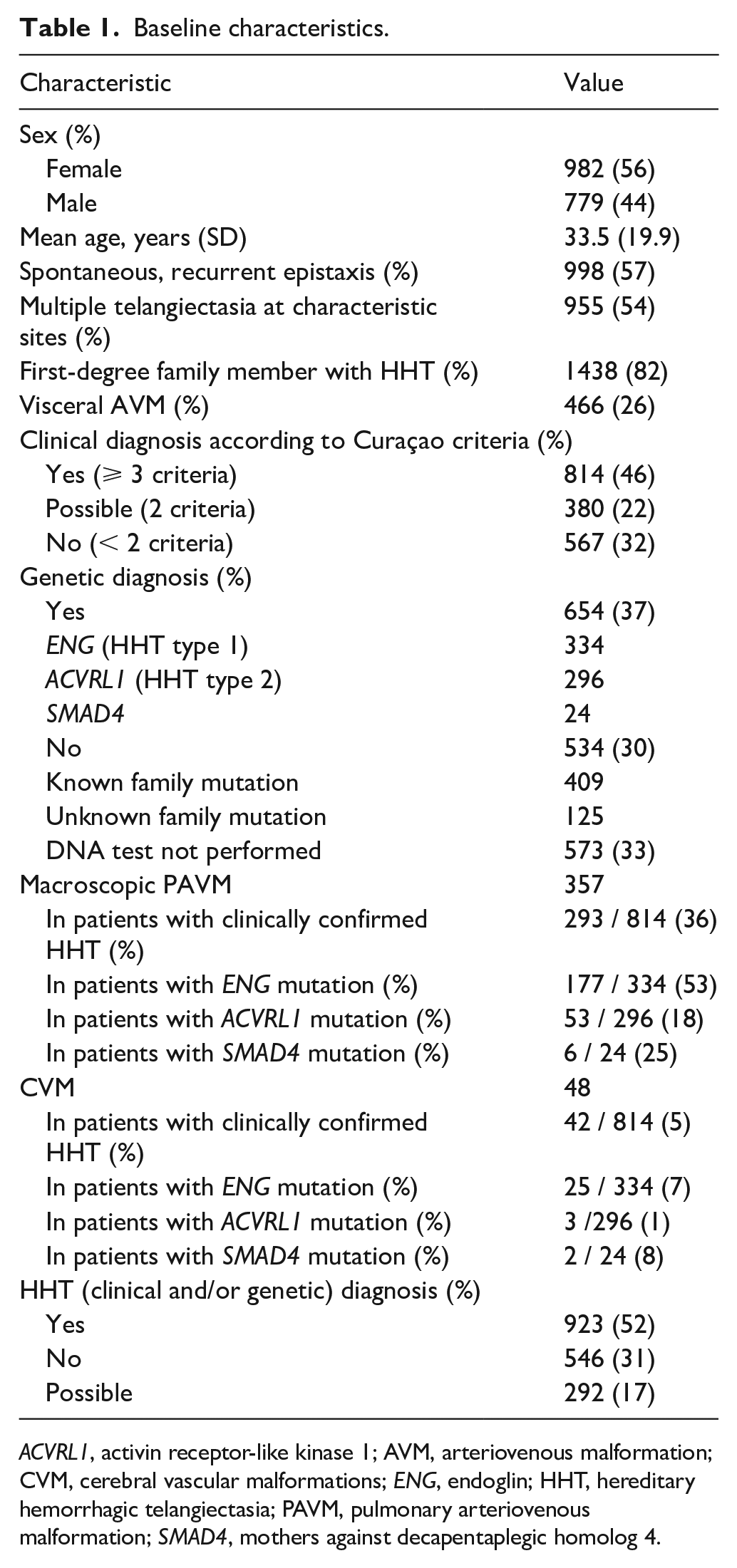
ACVRL1, activin receptor-like kinase 1; AVM, arteriovenous malformation; CVM, cerebral vascular malformations; ENG, endoglin; HHT, hereditary hemorrhagic telangiectasia; PAVM, pulmonary arteriovenous malformation; SMAD4, mothers against decapentaplegic homolog 4.
Prevalence of abnormal capillary microscopy results
In Figure 1, examples of normal nail folds and nail folds with both enlarged and giant loops are depicted. Capillary microscopy was normal in 852 individuals (48%) and in 909 individuals (52%) either enlarged loops (n = 246) or giant loops (n = 663) were observed. In patients with clinically and/or genetically confirmed HHT (n = 923), capillary microscopy was normal in 23% (n = 218), in the other 705 individuals (77%) abnormal nail fold capillaries were observed: enlarged loops were seen in 11% (n = 99) and giant loops in 66% (n = 606). In patients with HHT ruled out based on DNA testing (e.g. a known family mutation, the individual did not inhere the specific mutation), normal nail folds were observed in n = 326 (80%), enlarged loops in n = 72 (17%), and giant loops in n = 11 (3%). Table 2 shows the characteristics of the included patients.
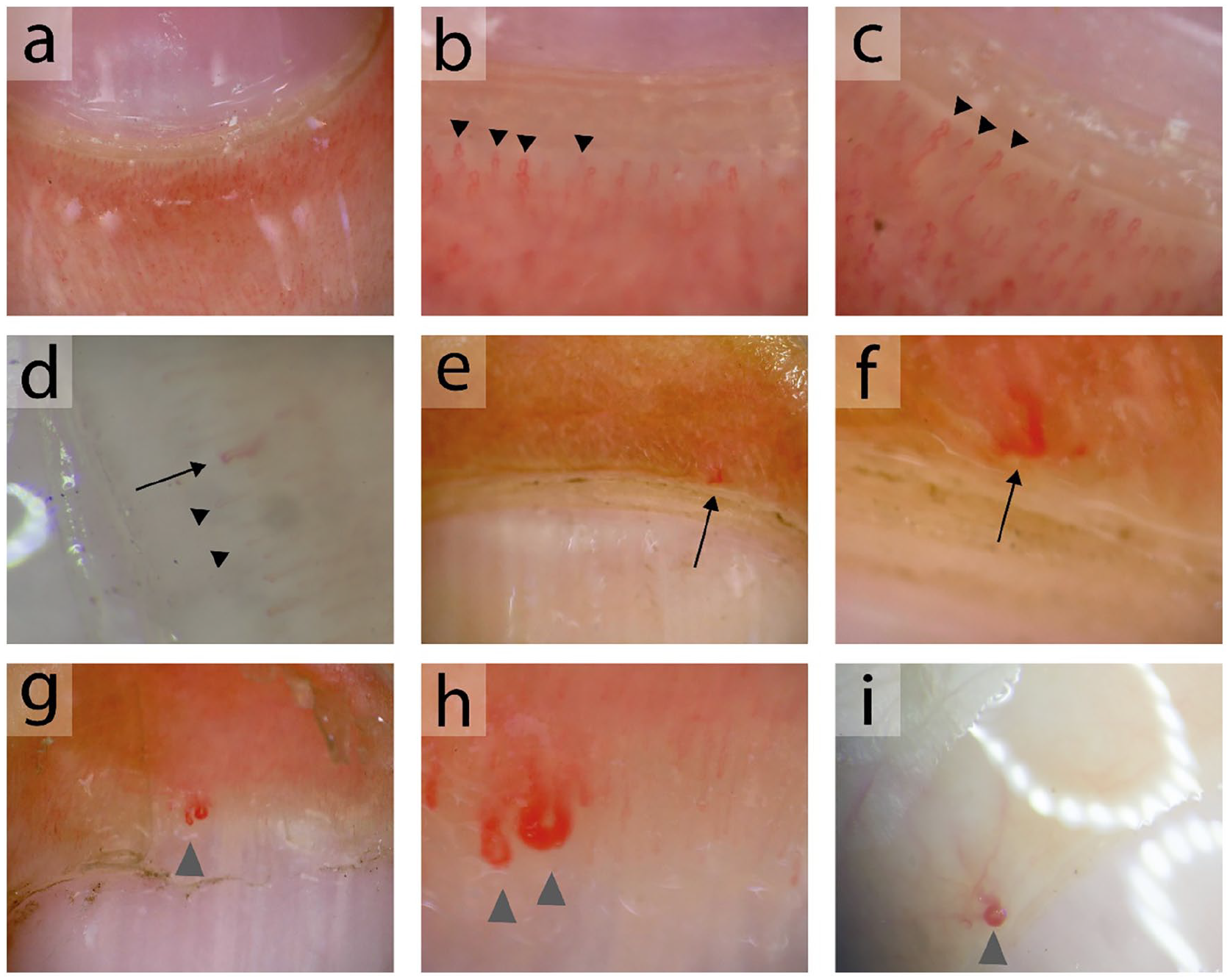
Examples of capillary nail microscopy.
Characteristics for individuals with normal nail fold capillaries, with enlarged and with giant loops.
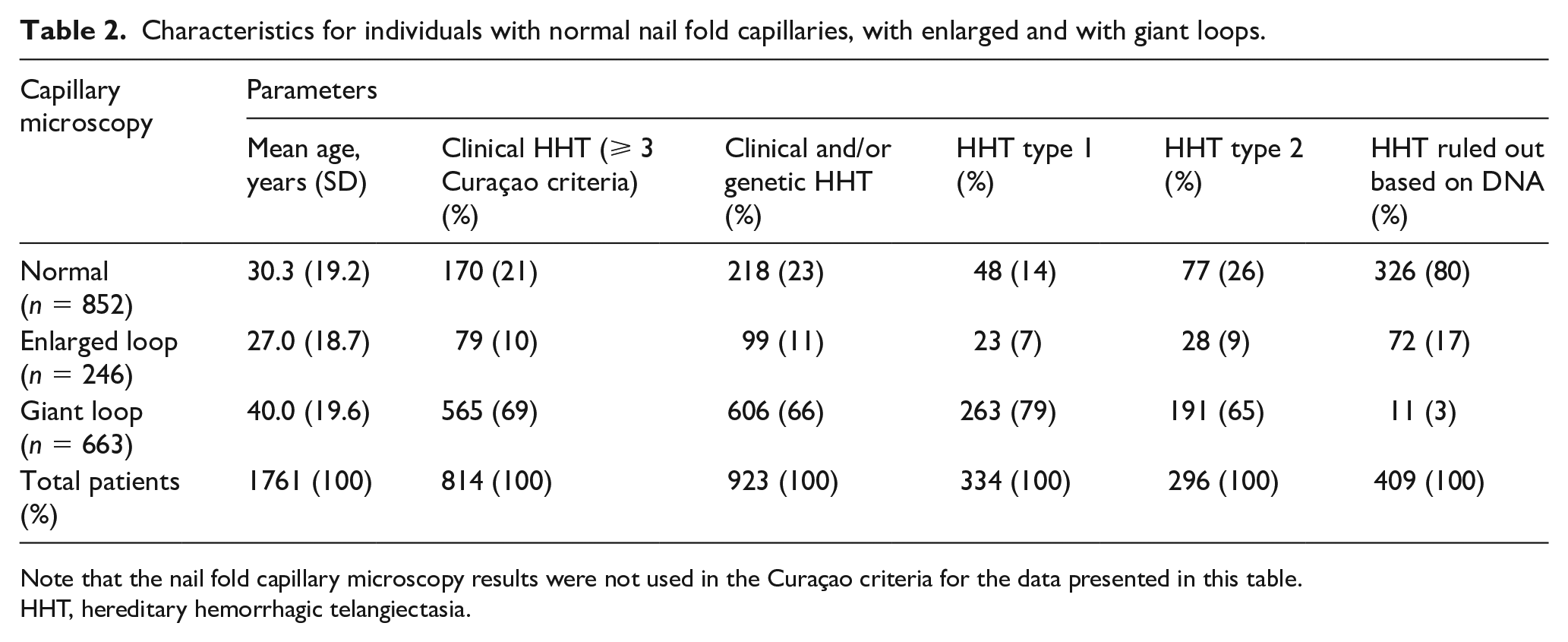
Note that the nail fold capillary microscopy results were not used in the Curaçao criteria for the data presented in this table.
HHT, hereditary hemorrhagic telangiectasia.
Additional diagnostic value of capillary microscopy in HHT
For establishing the additional diagnostic value of capillary microscopy, patients without genetic testing or without a known family mutation were excluded. The sensitivity and specificity analyses of the Curaçao criteria are shown in Table 3A–C. The sensitivity and specificity of the Curaçao criteria without capillary microscopy were 96% and 90%, respectively (Table 3A). When ‘giant loops’ were added as a positive criterion for mucocutaneous telangiectasia the sensitivity increased to 97% and specificity remained similar (Table 3B). When both giant and enlarged loops were regarded as a positive criterion, the sensitivity increased to 98% and the specificity decreased to 85% (Table 3C).
Sensitivity and specificity analyses.
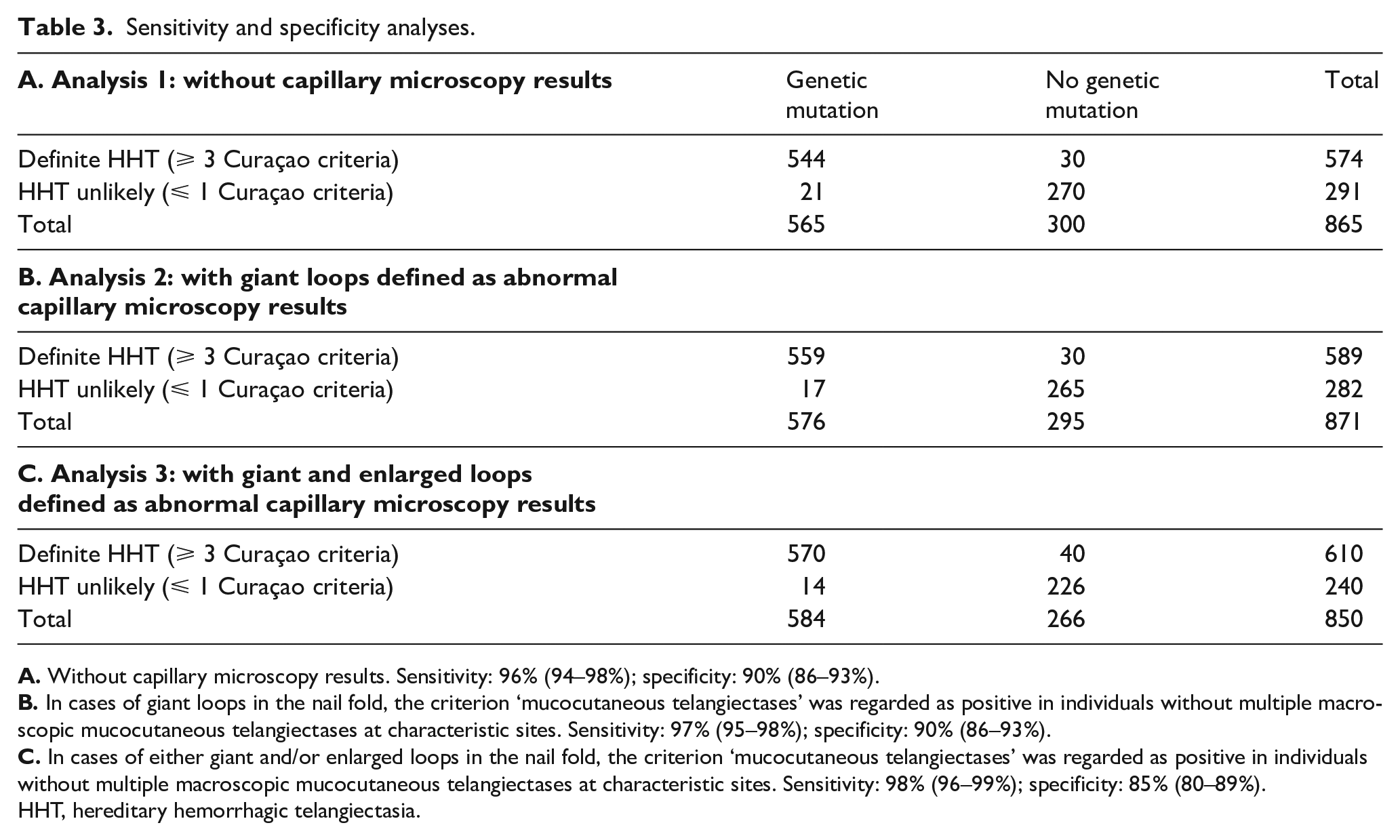
HHT, hereditary hemorrhagic telangiectasia.
In patients with a ‘possible’ HHT diagnosis (two Curaçao criteria) without any visible mucocutaneous telangiectases, capillary microscopy could be most useful because the presence of abnormal nail fold capillaries could make the clinical diagnosis ‘definite’ (three criteria). The flowchart of these patients (n = 380) is shown in Figure 2. Patients that did not have a genetic test (n = 132) or without a known family mutation (n = 47) were excluded. In total, 201 patients were included, of whom 113 (56%) did not meet the criterion ‘mucocutaneous telangiectases’. Of these 113 patients, 15 (13%) had giant loops, 21 (19%) had enlarged loops, and 77 (68%) had normal nail fold capillaries. HHT was confirmed with DNA testing in all 15 individuals (100%) with giant loops. The mean age in this group was 26 (± SD 16) years. This was significantly lower compared to the mean age of all the individuals with giant loops (40 years) (p = 0.005). In the group of patients with enlarged loops (n = 21), HHT was genetically diagnosed in 11 patients (52%), and in 10 patients (48%) HHT was ruled out based on the DNA results. In the patients with normal capillaries, HHT was genetically diagnosed in 23 patients (30%) and excluded in 54 patients (70%). The mean age for the patients with enlarged loops and with normal nail folds were 28 (± SD 18) and 27 (± SD 18) years, respectively. The mean age of both normal nail folds and enlarged loops were not significantly different compared to their entire group (for normal nail folds: 30 years; for enlarged loops: 27 years).
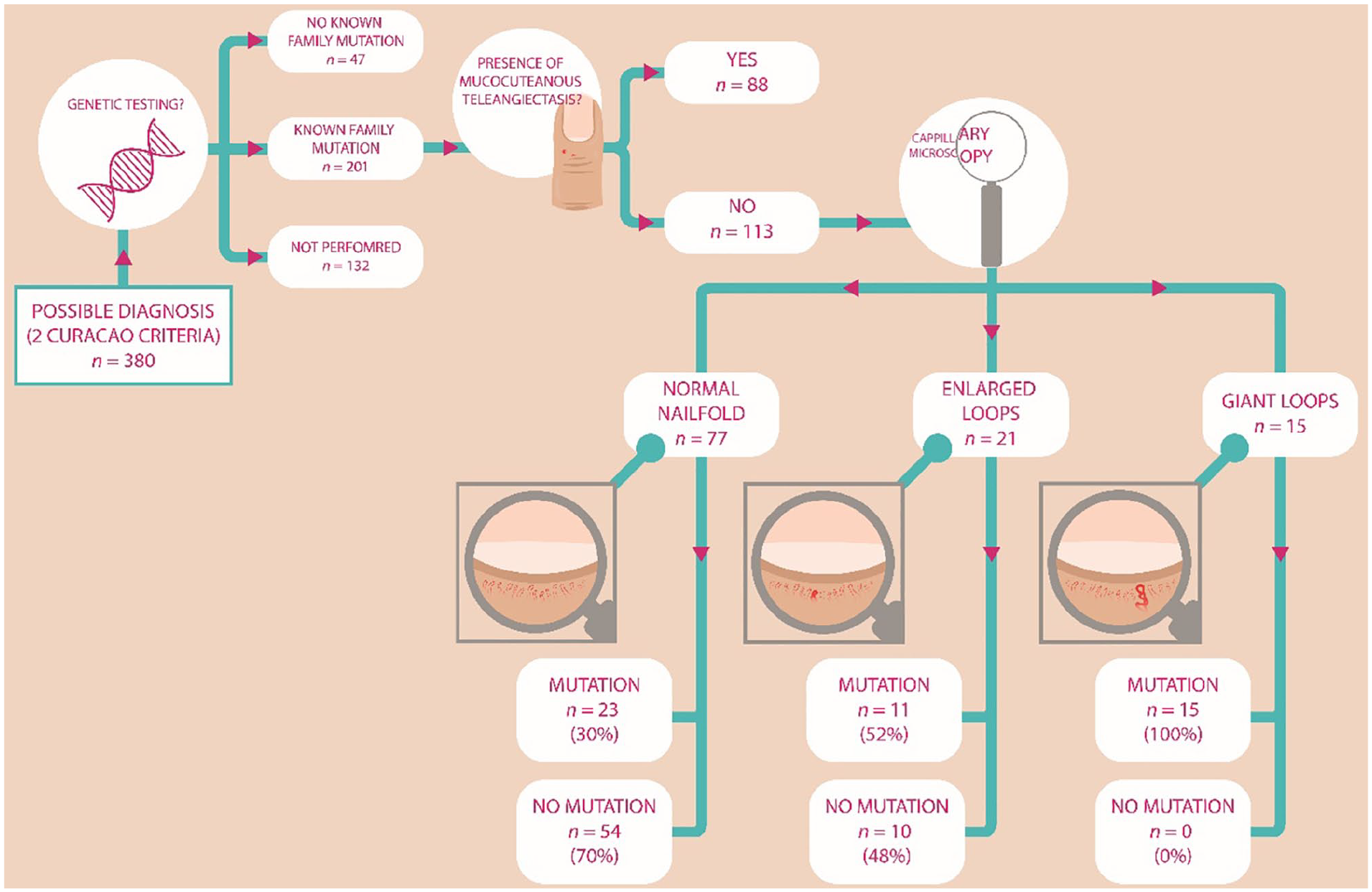
Flow chart of capillary microscopy and subsequent genetic diagnosis of patients with a ‘possible’ HHT who underwent genetic testing and do and do not meet the criterion ‘mucocutaneous telangiectases’.
Nail fold abnormalities in relation to several clinical characteristics
Patients with genetically confirmed HHT and giant loops (n = 459) had significantly lower hemoglobin levels and used iron supplementation (34% vs 13%, p < 0.001) and blood transfusions (9% vs 3%, p = 0.004) more frequently compared to genetically confirmed HHT patients with normal nail folds or enlarged loops (n = 195). Furthermore, pulmonary arteriovenous malformations (PAVMs) were more frequently observed in patients with giant loops (41% vs 25%, p < 0.001). Table 4 describes all the characteristics.
Characteristics associated with abnormal capillary microscopy.
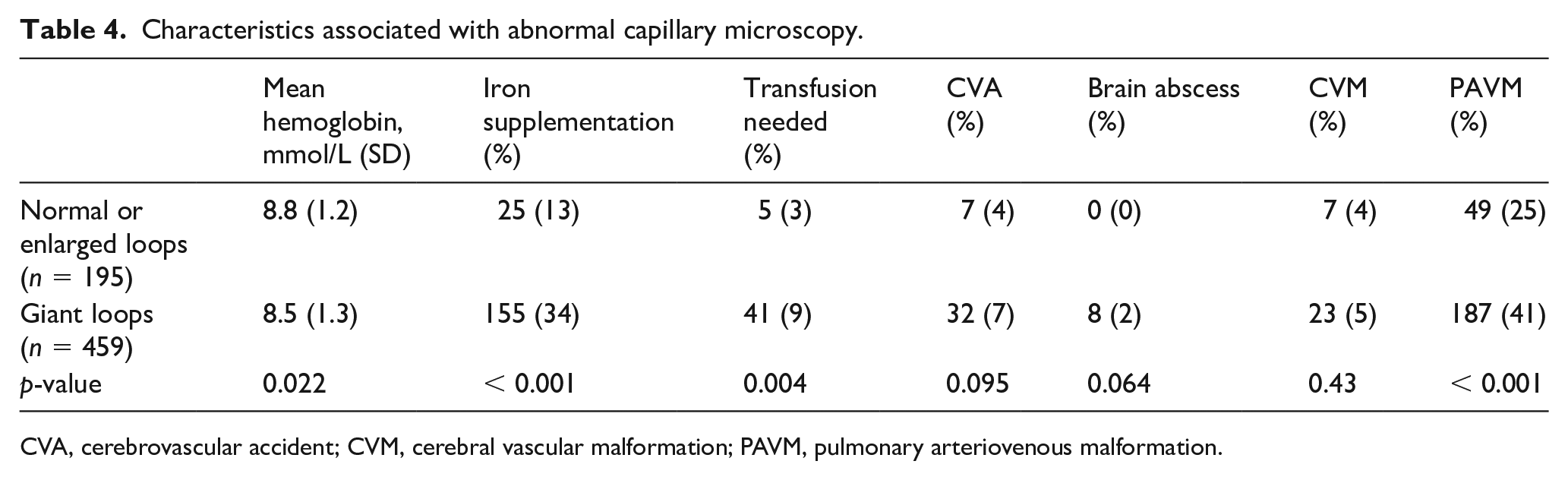
CVA, cerebrovascular accident; CVM, cerebral vascular malformation; PAVM, pulmonary arteriovenous malformation.
Discussion
In this study we assessed the prevalence and diagnostic value of capillary microscopy in patients suspected with HHT. The Curaçao criteria are internationally used for the clinical HHT diagnosis and thus evaluating and improving these criteria are important. We observed giant loops in 66% and enlarged loops in 11% of more than 900 patients with clinically and/or genetically confirmed HHT. The prevalence of abnormal nail fold capillaries in HHT in the literature ranges from 7% to 87%. Our finding is in line with a previous study of our group. Earlier, we found either enlarged or giant loops in 87% of 54 patients with HHT. 14 In a prospective study with 44 patients with HHT, abnormal nail fold capillaries were observed in 70.5%. 17 A lower prevalence was found in another study, where abnormal nail fold capillaries were discovered in 53.8% of the patients with HHT. 16 However, only the third and fourth finger of the right hand were inspected in this study. This might explain the lower prevalence rate. In the same study, they also observed an association of abnormal nail folds and PAVMs, similar to our findings. This finding can be explained by the fact that giant loops were more frequently seen in HHT type 1 than HHT type 2 (79% vs 65%) and by the higher mean age of the group with giant loops compared to the other groups and the age-related penetrance of HHT. 20 In another study, both the skin of the dorsal hand and the nail fold were inspected. They observed abnormal microscopic telangiectases on the dorsum skin of the hands in 91%, but only in 7% were pseudo-mega capillaries and mega capillaries seen. 15 They investigated the capillaries with a magnification up to 16×, in contrast to our and the other studies where magnifications up to 40× to 200× were used. This might partly explain the difference in prevalence because small abnormalities could have been missed. Interestingly, we observed, in individuals without HHT, enlarged loops (17%) and giant loops (3%). These abnormalities could have been caused by, for example, rheumatologic diseases or by more common disorders such as diabetes mellitus.8,12 Unfortunately, we did not examine comorbidities of the included patients. Thus, the cause and explanation of the nail fold abnormalities in non-HHT subjects remains unclear.
In the aforementioned study assessing the diagnostic value of capillary microscopy, the sensitivity, positive predictive value and accuracy of the criteria with epistaxis, telangiectasia, and a positive family history increased when microvascular abnormalities (both microscopic telangiectases on the dorsum and/or abnormal nail fold capillaries) was added as an additional criterion. 15 Unfortunately, they did not report a value for the specificity or absolute data to calculate the value. We did not regard capillary microscopy results as a separate criterion but as part of the criterion ‘mucocutaneous telangiectases’ of the Curaçao criteria. Regarding the presence of giant loops as a positive criterion for ‘mucocutaneous telangiectases’ increased the sensitivity of the Curaçao criteria to 97% without affecting the specificity (90%). When either giant loops or enlarged loops were regarded as a positive criterion, the sensitivity of the Curaçao criteria increased even further; however, the specificity decreased substantially to 85%. Although the change in sensitivity was small, we still believe capillary microscopy is of additional diagnostic value, especially in patients with a ‘possible’ diagnosis. In our study, in patients with a ‘possible’ clinical HHT diagnosis without mucocutaneous telangiectases but with giant loops, the genetic diagnosis was confirmed in all patients (n = 15). The mean age of these 15 individuals was lower than the mean age of the entire study cohort (26 vs 34 years) and lower than the total group with giant loops (26 vs 40 years). This would be compatible with the microscopic abnormalities preceding the (macroscopic) mucocutaneous telangiectases in patients with HHT.
Strengths and limitations
The major strength of this study is the large sample size of 1761 individuals, of whom 923 (52%) were either clinically and/or genetically diagnosed with HHT. To date, this is the largest study assessing capillary microscopy in individuals suspected with HHT. In addition, the subjects that underwent capillary microscopy were all at risk of having HHT instead of using healthy subjects as controls. This reduces the chance of a spectrum bias, which can lead to changes in estimates of diagnostic accuracy.21,22
However, this study also has several limitations. First, capillary microscopy was performed by one clinician and (digital) photographs were not routinely taken. This may result in inter-observer differences that might cloud the results. This is especially true for the enlarged loops, but probably not so much for the giant loops because they are very distinct from normal capillaries and can be easily recognized. Second, the clinicians who performed the microscopy were not blinded for the clinical data of the patients, which can introduce outcome assessment bias. However, we believe this was limited by the fact that visceral HHT involvement and genetic testing were usually not available at the time of screening and capillary microscopy. Third, this study is of a retrospective design. This design enables a large number of individuals to be assessed, but may introduce selection bias. We tried to minimize the selection bias affecting the data by using a standardized diagnostic protocol. This protocol was established after the first publication of capillary microscopy by our group. 14 We tried to minimize selection bias further by including all the patients who underwent capillary microscopy and had suspected HHT. Moreover, St Antonius Hospital is the only HHT center of excellence in The Netherlands. We believe, therefore, that the included participants are an adequate sample of the HHT population.
Conclusions
The prevalence of abnormal findings with capillary microscopy in patients with HHT is high. Although the addition of the presence of giant loops to the Curaçao criteria only led to a small increase in sensitivity without affecting the specificity, we still recommend using capillary microscopy in certain situations. Especially in patients with a possible diagnosis without any other mucocutaneous signs of HHT, capillary microscopy has proven to be not only an easy but also a valuable tool to make a definite clinical diagnosis.
Footnotes
Acknowledgements
We thank Dr A Herman from the rheumatology department of St Antonius Hospital, for his help with and expertise in making the capillary microscopy photographs.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: the study was funded by a TopZorg subsidy from ZonMw and by the Dutch scientific research organization for hereditary hemorrhagic telangiectasia: Stichting Wetenschappelijk Onderzoek Rendu Osler (SWORO).