
Abstract
There are only a few published studies that demonstrate associations between life expectancy, severe comorbidities, and their complications in patients with hereditary hemorrhagic telangiectasia (HHT). Relatives of 73 deceased patients with suspected HHT completed a questionnaire about causes of death, and symptoms and comorbidities that the patients had developed. We compared the data for 55 cases where HHT had been clinically confirmed with the general population. Patients suffering from HHT lost, on average, 19 years (SD 11 years) of potential life compared to the general population. Among the deceased HHT patients, 35% (95% CI: 23–48%) died from sepsis, 26% (95% CI: 16–38%) from cardiac failure, 20% (95% CI: 9–28%) from a severe bleeding episode, and 13% (95% CI: 6–24%) from terminal cancer. Congestive heart failure (69%, 95% CI: 56–80%) and pulmonary hypertension (23%, 95% CI: 14–36%) were the main non-fatal comorbidities in patients with HHT. Patients with HHT appear to have a lower life expectancy than the general population. Sepsis and cardiac failure were the main causes of death. Optimized and targeted screening programs for the most frequent comorbidities followed by improved management of infectious complications may increase life expectancy.
Keywords
Introduction
Hereditary hemorrhagic telangiectasia (HHT), also known as Rendu-Osler-Weber syndrome, is characterized by recurrent epistaxis, mucocutaneous telangiectases and visceral arteriovenous malformations. The estimated disease prevalence is between 1 in 5000 and 1 in 8000 individuals.1,2 It is an inherited genetic disorder and the first symptoms usually occur before adolescence when patients typically suffer from epistaxis.1–3
Organ manifestations of arteriovenous malformations range from small telangiectatic lesions in the oral or nasal mucosa, leading to bleeding and larger lesions affecting the lungs, liver and brain.3,4 Up to 10% of patients with HHT have cerebral vascular malformations 5 and 15–45% suffer from pulmonary vascular malformations. 6 Between 30% and 80% are diagnosed with hepatic vascular malformations. 7 In the liver, these shunts can lead to a high cardiac output state. Pulmonary vascular malformations can cause paradoxical embolism of septic material or thrombi. 8 An association between HHT and comorbidities such as heart failure, arterial aneurysms, anemia, juvenile polyposis syndrome, primary pulmonary hypertension and infectious diseases has been reported.9–12 Only a few studies describe the association between life expectancy in patients with HHT and comorbidities.13–15
The aim of this study was to evaluate causes of death and comorbidities in patients with HHT.
Methods
The senior author (UG), consulting physician for the German patient advocacy group, developed a questionnaire to gather information about deceased members of this group in 1997. From 1997 to 2016, relatives of 73 deceased patients with potential HHT completed the questionnaire about symptoms and comorbidities that the patients had developed, their age at death and cause of death. This study includes patients who died between the early 1980s and 2016. Once the patient advocacy group for HHT was informed about a patient’s death, a letter was sent to the patient’s relatives explaining the questionnaire and the study. The relatives were asked whether the cause of death could be a consequence of the disease or other circumstances. The patients’ medical reports were used to complement the data from the questionnaire. In 55 of the 73 cases, the diagnosis of HHT was found in their medical records, or was confirmed by the treating physician, or the patients met at least three of the four Curaçao criteria (see Supplementary Appendix A). Two authors independently checked the files of the cases. The analyses included these 55 patients with confirmed HHT. The study was approved by the Ethics Committee of the University Duisburg-Essen (16-7007-BO) and data were provided voluntarily by relatives of the deceased patients.
We estimated the overall life expectancy and potential years of life or the strata-specific life expectancy by age (1 year), sex, and calendar year of death. Life tables were provided by the German Federal Statistical Office. To compare the distribution of causes of death in the general population with that of the HHT patients, we used the German cause of death statistics for the year 2015.16,17 We assessed the data concerning the cause of death and sought agreement between the medical charts (yes, likely, possible, unclassifiable, unlikely, no) and the report by the relatives (yes, no, unknown). For this agreement analysis, we regrouped the answer categories ‘yes, likely and possible’ as ‘yes’ and the answer categories ‘unclassifiable, unlikely and no’ as ‘no’. We excluded deaths where the relatives did not know the cause of death. Besides observed agreement, we calculated chance-corrected agreement (kappa) with 95% confidence intervals (CIs). We estimated odds ratios (ORs) and exact 95% confidence intervals.
Statistical analyses were performed with IBM SPSS Statistics, version 23 (IBM Corp., Armonk, NY, USA).
Results
Clinical presentation and life expectancy
The study contained 25 men and 30 women with ages at death ranging from 30 to 88 years. All patients suffered from epistaxis and a majority (90%) had typical mucocutaneous telangiectases and arteriovenous malformations in their livers (Table 1). In our cohort, the relative frequencies of cerebral or pulmonary vascular malformations were similar among women and men (cerebral vascular malformation: n=24, men = 8% vs women = 8%, 95% CI: 2–26; pulmonary vascular malformation: n=23, men = 17%, 95% CI: 7–37 vs women = 30%, 95% CI: 16–51).
Manifestations of HHT among 55 deceased patients.
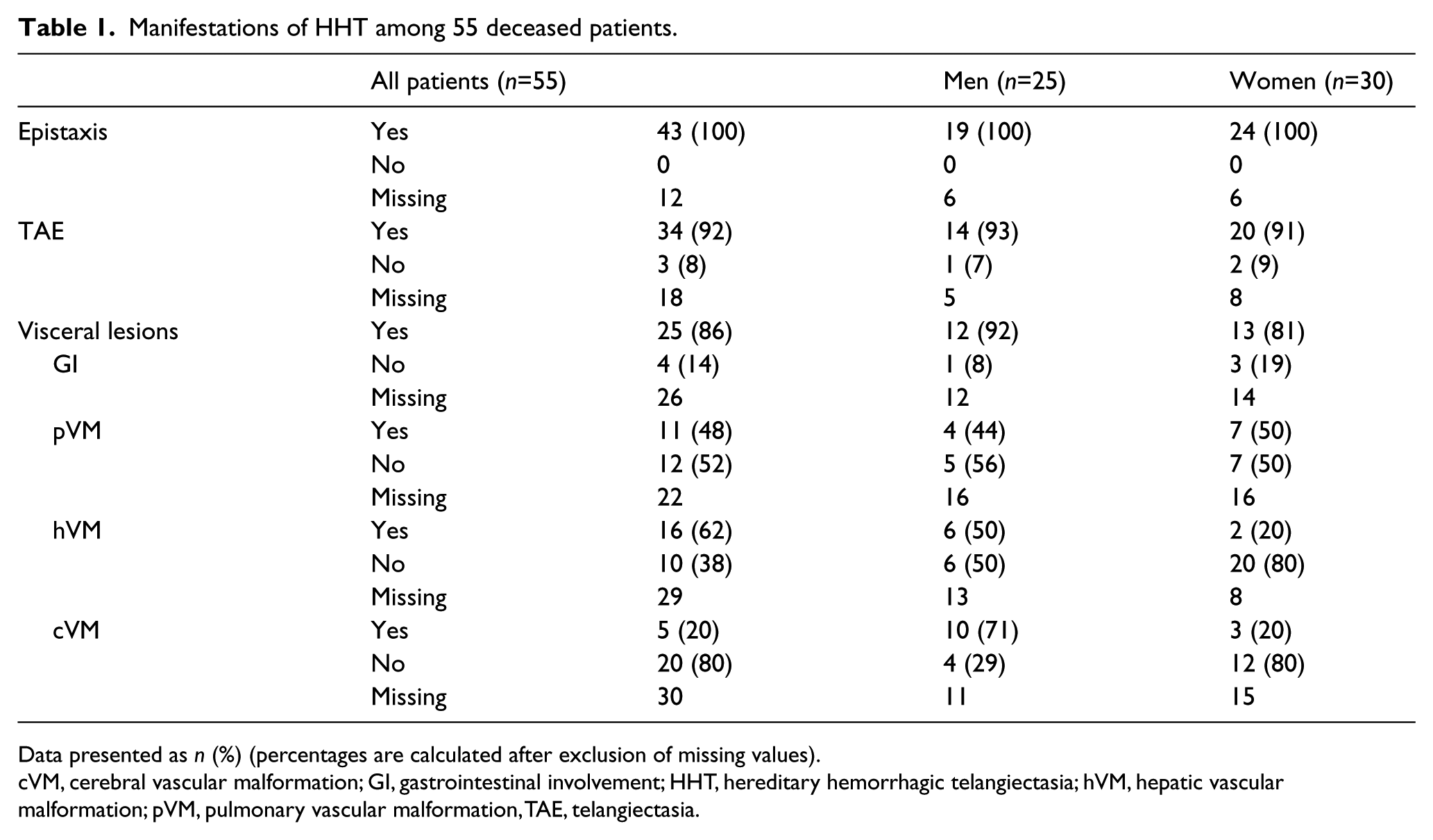
Data presented as n (%) (percentages are calculated after exclusion of missing values).
cVM, cerebral vascular malformation; GI, gastrointestinal involvement; HHT, hereditary hemorrhagic telangiectasia; hVM, hepatic vascular malformation; pVM, pulmonary vascular malformation, TAE, telangiectasia.
Women had a higher frequency of being diagnosed with hepatic vascular malformations (n=26; men = 23%, 95% CI: 11–42 vs women = 38%, 95% CI: 22–57).
In our study, the mean age at death was 66 years (SD 13 years; median: 67 years). Female patients with HHT died earlier than male patients (women: 64 years, SD 15 years; men: 68 years, SD 10 years; general population: women, 83 years; men, 78 years) (Table 2).
Mean age at death in a population of patients with HHT and the general population.
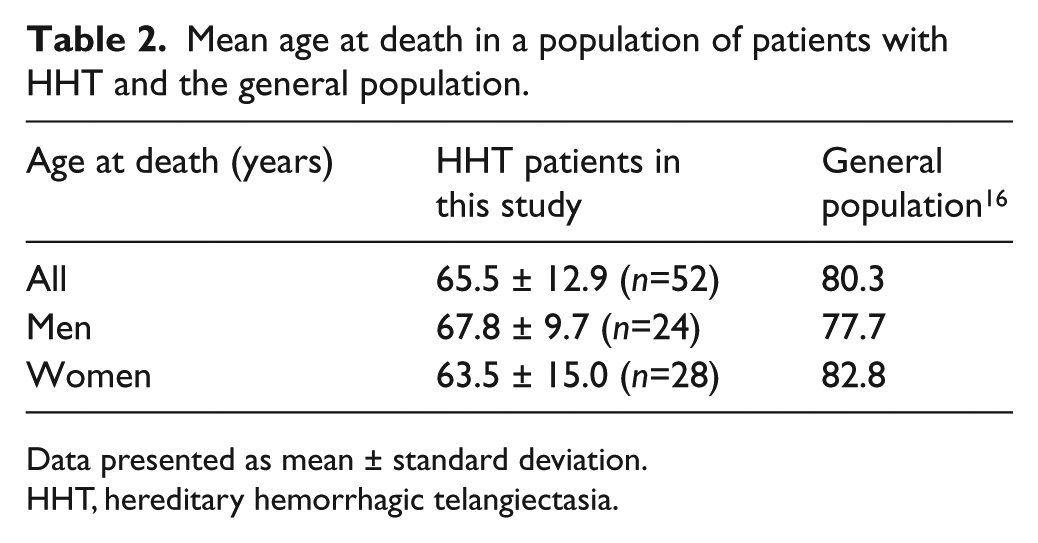
Data presented as mean ± standard deviation.
HHT, hereditary hemorrhagic telangiectasia.
Patients suffering from HHT on average lost 19 years (SD 11 years) of potential life (women: 24 years, SD 15 years, n=29; men: 15 years, SD 7 years, n=23) according to the corresponding life tables (Appendix A). 16
Causes of death
Figure 1 shows the recorded causes of death in patients with HHT: 26% (12/46) had a lethal cardiac failure; 35% (16/46) died from an infectious disease leading to sepsis; 13% (6/46) died from a carcinoma; and 20% (9/46) had a major bleeding episode leading to death.
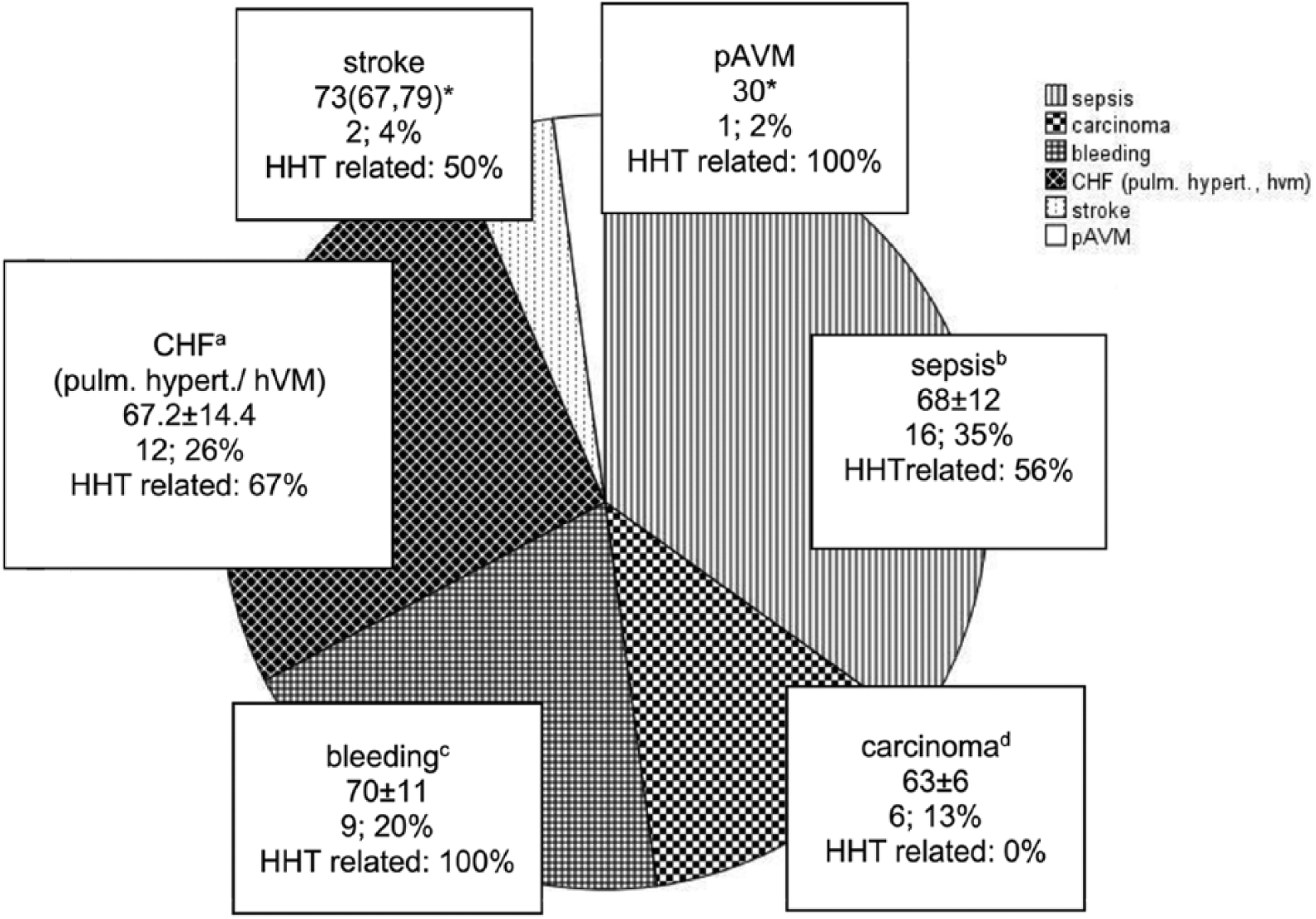
Recorded causes of death in patients with HHT.
We were able to contact 24 out of 55 relatives about the perceived relationship between cause of death and HHT. In 83% (20/24) of the cases relatives stated that HHT was the probable cause of death. In 92% of the deaths (22/24), the relatives reported that the patient’s physician associated the patient’s death with HHT. According to the authors’ assessment, in 28 out of 55 patients with HHT (51%) the cause of death was at least probably or possibly HHT-related, whereas in 13 cases (24%) the patients died from another disease (Appendix A). The observed agreement on HHT between the medical chart review and reports from relatives regarding cause of death was 91% (20/22). The chance-corrected agreement as measured by kappa was 62% (95% CI: 16–100).
In all patients who died from a major bleeding (n=9) or from a pulmonary vascular malformation (n=1), their cause of death was assessed to be HHT-related (Figure 1).
Comorbidities
Regarding comorbidities, 23% (9/39) suffered from pulmonary hypertension and six patients (6/39, 15%) had cancer. Approximately 10% (4/39) were diagnosed with diabetes, 15% (6/39) with a neurological disease and 69% (27/39) had a congestive heart failure (CHF) (Figure 2). Two patients who suffered from pulmonary vascular malformations developed brain abscesses later.
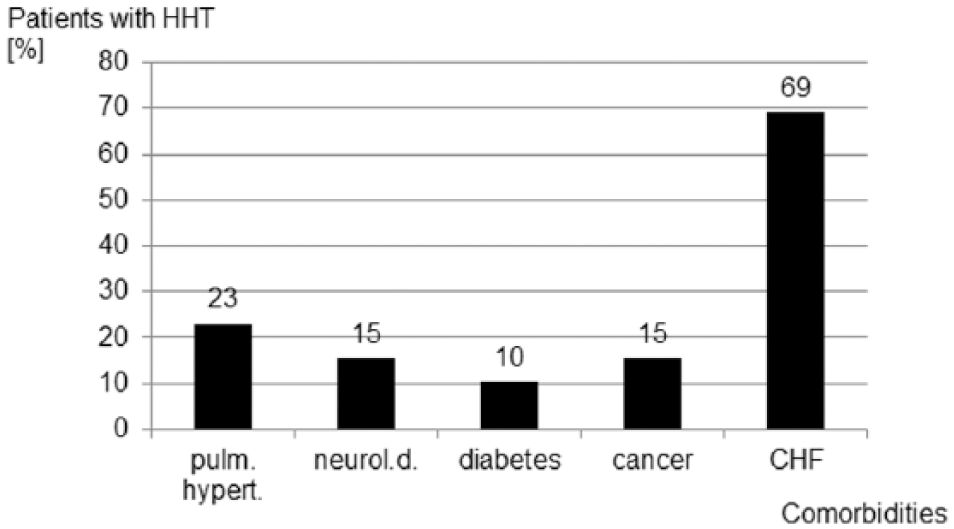
Comorbidities in deceased patients with HHT (n = 39).
Specific risk factors
Patients with pulmonary vascular malformations had a higher chance of death by sepsis than patients without pulmonary vascular malformations (4/10 vs 2/12, respectively, OR=3.3, 95% CI: 0.3–45.1). Patients with pulmonary vascular malformations had a higher chance of stroke, brain abscess and transient ischemic attack (TIA) than patients without (3/11 vs 1/12, respectively, OR=4.1, 95% CI: 0.3–47.3). Patients with hepatic vascular malformations had a similar chance of heart failure as those without hepatic vascular malformations (9/16 vs 6/10, respectively, OR=0.9, 95% CI: 0.1–5.5).
Discussion
In clinical practice, life expectancy and the assessment of comorbidities may optimize screening programs. They are important tools in evaluating potential benefits and the adverse effects of treatments. Articles on the mortality rate and comorbidities in patients with HHT are sparse and their results have been contradictory.13–15
Life expectancy
In accordance with other studies,1,13–15 our data suggest that patients with HHT have a lower life expectancy (66 years) compared to the general German population (80.3 years). 16 Other studies assessing life expectancy used familial medical histories (sample size: n=40, 13 n=57, 14 n=113 15 ) or patient registries analyzing 675 patients with HHT. 13 These patients were either compared to the general regional population1,13 or affected partners with their non-affected partners.14,15 Our data about life expectancy in patients with HHT are congruent with literature.13–15
Screening for cerebral and pulmonary vascular malformations in patients with HHT has been frequently recommended over the last years. This enables identification and prompt treatment of high-risk patients, thus preventing comorbidities and increasing the life expectancy of those patients.18–21 As this study contains data from patients whose death occurred from the early 1980s to 2016, there might be a difference in the quality and quantity of screening examinations.
Our study demonstrated that, in contrast to the general population, women with HHT died earlier than men. The risk of developing hepatic vascular malformations was higher in women than in men. Buscarini and colleagues 22 also showed that women suffer more often from hepatic vascular malformations than men and therefore might experience a more severe disease course and a higher rate of clinically relevant complications.23–26
Causes of death
Every fifth patient with HHT died from a major bleeding episode such as major epistaxis or gastrointestinal bleeding, or ruptured splenic artery aneurysm (other studies described ruptured splenic aneurysm as a rare comorbidity of HHT).27–29 Sepsis and cardiac diseases were stated more often than major bleedings as causes of death. A total of 26% of patients with HHT died from cardiac failure, which is less frequent than in the general German population (39%). 17 Our study could not establish a link between HHT patients with hepatic vascular malformations and cardiac failure as a cause of death. However, other research suggests that patients with hepatic vascular malformations have a higher risk of heart failure. 14
While there seems to be a lower life expectancy as well as a higher risk for cardiac, pulmonary or neurological comorbidities,13–15 patients with HHT may have a lower risk of developing certain carcinomas. This finding is, however, inconclusive.30–32 In our study, 13% of the patients with HHT died from carcinomas, while approximately one in four cases of death in the general German population was related to cancer in 2015 (26%). 17 However, this comparison cannot be made without standardizing to age. The number of patients with cancer in our sample was too small (n=6) to make any significant statement about HHT and the prevalence and mortality rate of specific cancer rates. Further studies could investigate the relationship between HHT and cancer, and associated risk factors might be a relevant next step.
A third of our cohort (35%) unexpectedly died from sepsis compared with just 2% in the general German population. 17 The reasons for this disparity are unclear. Several mechanisms have been documented on how HHT might influence the immune system.33–37 Owing to recurrent epistaxis and its treatment (e.g. nasal packing, coagulation, laser treatment) in patients with HHT, nasal bacteria may persist and proliferate. 33 Patients with pulmonary vascular malformations may suffer from septic or sterile thrombiproducing brain infarcts, allowing bacteria to flourish. 8 In our cohort, 15% of the patients suffered from a neurological disorder (brain abscess, stroke, cerebral bleeding, Parkinson’s disease). Two patients had a history of brain abscess several years before death. However, both patients were diagnosed with cerebral and pulmonary vascular malformations. Brain abscess is known to occur in 1% of patients with HHT but has a 40% mortality rate. 38 HHT patients should therefore be considered to be at high risk of recurrent cerebral 35 and severe extracerebral11,39 complications involving infections. However, pulmonary vascular malformations on their own do not explain the elevated mortality rate caused by sepsis in all patients, suggesting the role played by changed immune systems in patients with HHT.
We acknowledge that there may be a difference between the relatives’ subjective perception of the patients’ cause of death being associated with HHT and the actual medical records. This variance is likely because relatives are acutely aware of the daily challenges faced by patients with HHT.40–42 Relatives may overestimate the influence HHT had on the patients’ cause of death.
Comorbidities and specific risk factors
Our results show that more than half of the patients with HHT were diagnosed with a congestive heart failure. This may be explained by the high rate of hepatic malformations in these patients. 7 However, this association could not be proven statistically.
Every fourth patient from our cohort suffered from pulmonary hypertension. Hepatic vascular malformations may lead to pulmonary hypertension.43,44 HHT-related gene mutations (ALK-1) are associated with this disease. 12 To our knowledge, the precise prevalence of pulmonary hypertension in patients with HHT is unknown. Other studies estimated that the prevalence of pulmonary hypertension in patients with HHT to be up to 21%.45,46 Unfortunately, pressure estimations and gradients calculated with the transthoracic echocardiography may be inaccurate. 47 Right heart catheterization might be necessary to confirm pulmonary hypertension. 48 Consequently, Chizinga et al. 49 claimed that a quite high proportion of HHT patients may have pulmonary hypertension and this result correlates with our study. There were associations between pulmonary hypertension and patients with hepatic vascular malformations. Currently, no screening for pulmonary hypertension is recommended in patients with HHT. This raises the question of whether early detection and treatment of hepatic vascular malformations and pulmonary hypertension might have had reduced mortality in patients with HHT.
A subset of the patients in our cohort typically developed neurologic diseases (e.g. stroke, brain abscess, TIA). Pulmonary vascular malformations can lead to neurologic complications such as embolic stroke13,25 or cerebral abscesses, 35 and cerebral vascular malformations can result in seizures or hemorrhagic strokes.
Study limitations
As in most other studies on this topic (see discussion on life expectancy), the number of patients included in the research is small. It is likely that a high number of patients with HHT remained undiagnosed. 50 We reached patients mainly via the German patient advocacy group, whose members grew from just 50 to 600 during the course of our study. We had to rely on external data for the diagnosis. Spouses or siblings of elderly patients at the same age might not have been able to answer the questionnaire sufficiently. Therefore, we might have received data largely from patients who died at a relatively young age. The majority of the patients in our study showed typical multiple telangiectases and suffered from epistaxis. Like previous studies, 7 patients in our cohort were diagnosed with hepatic vascular malformations. A total of 20% of patients had cerebral and 48% had pulmonary vascular malformations. In other studies,5,6 fewer patients were diagnosed with cerebral and pulmonary vascular malformations. As all deceased patients were members of the German advocacy group, we may have inadvertently collected data from patients with potentially severe disease progression. Patients with milder forms of the disease may have a natural history more similar to that of the general public. Therefore, our data may not be representative of the total HHT population. Life expectancy may also be influenced by different lifestyles, socio-economic conditions and other environmental factors which we did not evaluate in this study. Since all deceased patients were members of the German patient association, regularly receiving information about HHT, the consequent general interest in and acceptance of the disease among relatives may have caused another bias.
Conclusion
HHT is a chronic and incurable disease, which reduced the life expectancy of our patient cohort. The most frequent causes of death were sepsis and heart failure. Only 20% of the patients with HHT died from a major bleeding. The rate of pulmonary hypertension, which may be associated with cardiac failure, was unexpectedly high. The mechanisms behind our findings are not completely clear. Were further studies to indicate a major role of pulmonary hypertension and immunological changes in HHT-related deaths, the introduction of targeted screening programs for these manifestations could increase life expectancy.
Supplemental Material
VMJ767761_Supplementary_material – Supplemental material for Life expectancy and comorbidities in patients with hereditary hemorrhagic telangiectasia
Supplemental material, VMJ767761_Supplementary_material for Life expectancy and comorbidities in patients with hereditary hemorrhagic telangiectasia by Freya Droege, Kruthika Thangavelu, Boris A Stuck, Andreas Stang, Stephan Lang and Urban Geisthoff in Vascular Medicine
Footnotes
Acknowledgements
The authors are grateful both to the relatives of the deceased patients for answering the questionnaire and also to the German advocacy group who assisted with the distribution of the questionnaire. In addition, the authors thank Michael Denniss who, as a native English speaker, edited the manuscript. Informed consent was obtained from all relatives of the deceased patients included in the study.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Supplementary material
The supplementary material is available online with the article.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.